
Abstract
Background:
Total ankle arthroplasty (TAA) can result in excellent outcomes in patients with end-stage arthritis, but most patients with end-stage hemophilic ankle arthropathy (ESHAA) still undergo ankle arthrodesis (AA). The purpose of this study was to analyze clinical and radiological results of TAA and AA for ESHAA.
Methods:
A total of 29 cases (16 TAAs and 13 AAs) of painful ESHAA were included. For clinical outcome evaluation, visual analog scale (VAS) for pain, Foot Function Index (FFI), and range of motion (ROM) were analyzed. Postoperative clinical and radiological complications were also analyzed. The mean duration of follow-up was 6.8 ± 3.0 years. The mean age was 44.1 ± 9.9 years.
Results:
The VAS for pain was significantly improved from 5.5 ± 2.3 to 0.9 ± 1.2 (P < .001). The FFI scale was significantly improved from 61.6% ± 15.5% to 16.6% ± 15.4% (P < .001). In FFI disability and activity subscales, the TAA group exhibited meaningful outcomes relative to those of the AA group (P = .012 and .036, respectively). The total ROM in the TAA group changed from 30.8 ± 12.6 degrees to 37.3 ± 12.8 degrees at final follow-up (P = .090). Three cases of osteolysis and 1 case of heterotopic ossification were noted in the TAA group. No cases of nonunion were noted in the AA group. Progressive arthrosis of adjacent joints after AA was observed in 1 case.
Conclusion:
Both TAA and AA in ESHAA exhibited significant improvement in pain based on VAS and FFI scales. Compared to AA, TAA resulted in superior outcomes in FFI disability and activity subscales, suggesting that TAA may be considered as a surgical option alongside AA for ESHAA.
Level of Evidence:
Level III, retrospective comparative study.
Keywords
Ankle arthrodesis (AA) and total ankle arthroplasty (TAA) are widely used as treatment methods for end-stage ankle arthritis accompanied by severe pain and activity limitations. 11 AA is well established but has the disadvantages of loss of joint function, long periods of immobilization postoperation, incidence of pseudoarthrosis, and load on adjacent joints. TAA, which is based on successful results from hip and knee joints, has gained interest since the demonstration of its effectiveness for functional joint reconstruction. Furthermore, the current literature of foot and ankle reconstructive surgery suggests that TAA can be superior to AA in patients with end-stage ankle arthritis.9,22
The ankle joint is the third most common site of hemophilic arthropathy, after the knee and elbow joints. 18 Consideration should be given to characteristics that are affected at a younger age. The ankle may become a target joint by repeated intra-articular bleeding, eventually worsening to end-stage arthrosis at a relatively young age. 17 The traditional treatment for symptomatic end-stage hemophilic ankle arthropathy is AA. AA is a reliable and proven treatment that relieves pain, reduces intra-articular bleeding, and corrects deformities. 13 In nonhemophilic arthropathy, arthrosis of adjacent joints may occur during long-term follow-up after AA, 12 which may require additional adjacent joint arthrodesis. 30 There is a paucity of literature on how these characteristics affect hemophilic arthropathy.4,7,33 As the joint replacement in hemophiliacs has been beneficial in hip and knee joints,21,32 some affirmative studies on TAA for end-stage hemophilic ankle arthropathy (ESHAA) have been reported,5,16,25,34 but the evidence remains insufficient. To address this gap in the literature, we retrospectively analyzed the clinical and radiological results of TAA and AA cases. We hypothesized that both TAA and AA could obtain adequate clinical and radiological results for ESHAA.
Methods
Patients
A total of 29 patients with painful ESHAA who underwent TAA or AA between January 2008 and July 2017 were included. Of the 29 cases, TAA was performed in 16 cases and AA in 13 cases. Since there were no specific guidelines in proceeding with either TAA or AA, the decision was made on the individual patient basis after obtaining consent. In this process, unmanageable malalignment and contralateral ankle fusion status were considered along with the patient preference. Most patients in this study were being treated with coagulation factors from the National Hemophilia Foundation clinics as they visited the hospital only with uncontrolled symptoms. The indications for operation included a lack of improvement with conservative management such as use of medications and immobilization, hemarthrosis, swelling, arthralgia, and decreased ankle range of motion (ROM). All patients showed stage 4 arthropathy based on Kellgren-Lawrence classification. Exclusion criteria were active infection, extensive talar necrosis, unmanageable instability, severe malalignment, documented allergy or intolerance to metals, and/or neuropathic arthropathy. All study participants provided informed consent, and the study design was approved by the appropriate ethics review board.
Hematological Care
Hematological screening tests, including a complete blood count, partial thromboplastin time, prothrombin time, serum levels of coagulation factors, and assessment of coagulation inhibitors to confirm the absence of coagulation inhibitors, were performed. Based on the department protocol, all patients received factor replacement therapy. Patients with coagulation problems or perioperative bleeding events were managed by an interdisciplinary team of hematologists. Antihemophilic factor VIII (FVIII) and antihemophilic factor IX (FIX) were administered at doses of 50 U/kg and 65 U/kg body weight, respectively, to restore factor levels to 100% preoperatively. Serum levels were maintained at 100% for 2 days postoperatively, at 80% until day 5, at 60% until day 8, and at 40% until the second week postoperatively. FVIII (half-life of 8 hours) was administered thrice a day, whereas FIX (half-life of 12 hours) was administered twice a day. No other antithrombotic prophylaxis was used. In the case of prolonged exudation or bleeding at the surgical site or through the drainage tube, an additional coagulation factor was administered to target 100% of the coagulation factor.
Demographics
Parametric tests were performed for each variable. The data were not normally distributed. Of the 29 cases, 16 were TAA and 13 were AA. All patients were male. The mean age of all patients was 44.1 ± 9.9 (range, 21.3-57.7) years. No difference between the mean ages of 2 groups could be detected (P = .232). The mean follow-up for all patients was 6.8 ± 3.0 (range, 2.0-11.6) years. Cases comprised 15 right ankles and 14 left ankles. The mean body mass index of all patients was 25.1 ± 3.8 (range, 18.9-35.2) kg/m2. Of the 29 cases, hemophilia type A comprised 27 cases and type B comprised 2 cases. No cases of factor VII deficiency were noted. There were 19 cases of hepatitis C and no cases of hepatitis A or B. All patients showed stage 4 arthropathy based on Kellgren-Lawrence classification. Of the 16 TAA cases, 13 received Hintegra (Newdeal), 2 received Mobility (DePuy), and 1 received Salto (Tornier). Of the 13 AA cases, screw fixation was performed in 9, anterior plate fixation in 2, and S-pin fixation and plaster immobilization in 2 (Table 1).
Baseline Characteristics of All Ankles.
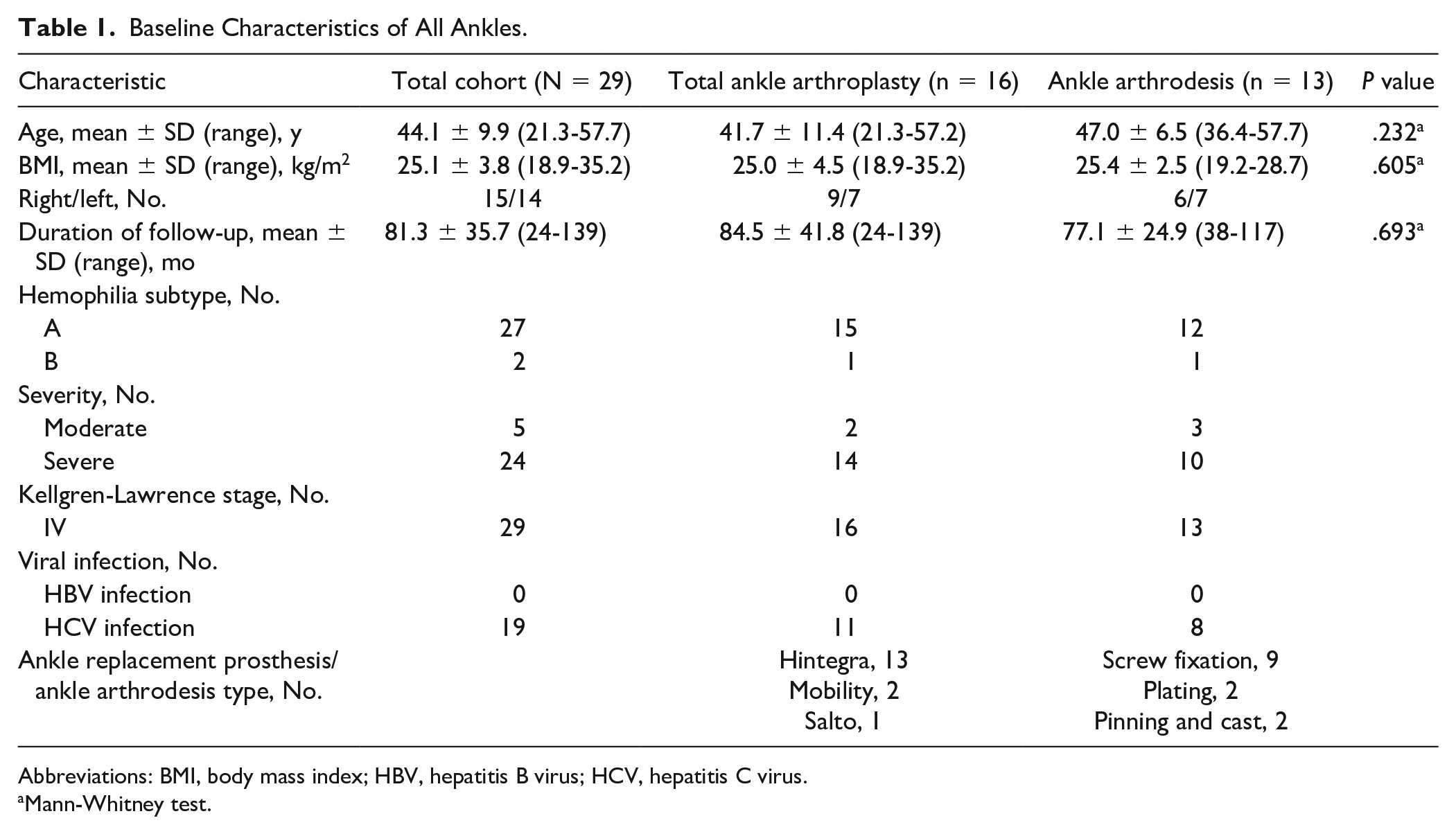
Abbreviations: BMI, body mass index; HBV, hepatitis B virus; HCV, hepatitis C virus.
Mann-Whitney test.
Operative Procedures
For TAA, the conventional procedure with cementless fixation was performed with third-generation implants, including Hintegra (Newdeal), Salto (Tornier), and Mobility (DePuy).
Depending on each case, AA was performed via the anterior approach or lateral transfibular approach. The ankle was fixed with 2 to 3 screws that penetrated the distal tibia and talus, or a precontoured plate was fixed in an appropriate position in front of the ankle. When the lateral transfibular approach was applied, the distal part of the fibula was osteotomized and ankle joint exposed. If necessary, autologous bone was harvested from the fibula. The alignment position was set to a neutral or slightly externally rotated position.
Once the wound condition was dry and stable, patients in the TAA group were mobilized for 6 weeks with their feet placed in a short leg walking cast or cam walker. Active and passive motion of the ankle joint was performed to support soft tissue recovery during the first 6 weeks. In the AA group, a short-leg nonweightbearing cast was applied for 6 weeks after wound stabilization. Additional immobilization with a cast was determined according to the signs of radiographic healing and presence of pain. If signs of delayed healing were observed or the patient was still in pain, additional casting was further applied for up to 12 weeks. After 12 weeks, all patients were allowed to perform weightbearing as tolerated.
Clinical Assessment
For clinical assessment, visual analog scale (VAS), Foot Function Index (FFI), and ROM of the ankle joint before and after operation were measured. ROM in the AA group was not measured after the operation. Patients’ pain levels were rated from 0 (no pain) to 10 (maximum pain) using the VAS. For functional evaluation, the FFI, which comprised 23 divided questionnaires, including a pain subscale (9 elements), a disability subscale (9 elements), and an activity limitation subscale (5 elements), was assessed before and after the operation, as well as during the follow-up period.1,8 When measuring ROM, the angle between the axis of the calf and lateral edge of the foot in the knee flexion position was measured using a goniometer. Major complications were identified perioperatively and during the follow-up period. Osteolysis or loosening around the implant, osteosynthesis, changes in arthritis in adjacent joints, and hardware failure were examined.
Statistical Analysis
The Kolmogorov-Smirnov test was performed on the measured values of each variable for a normality test. To verify the significance of changes in each variable, a Wilcoxon signed placement test and Mann-Whitney U test were performed to compare the results of TAA and AA. SPSS Windows version 20.0 (SPSS, Inc) was used for all statistical analyses. The level of statistical significance was set at 5% (P ≤ .05). For each comparison, the effect size was calculated (Cohen’s d) to evaluate the clinical relevance of the magnitude of the differences (0.2, small; 0.5, medium; 0.8, large) in pain VAS and FFI between groups and not only the statistical significance. 10
where mTAA and mAA are the mean for the TAA group and AA group, respectively, and σ AA is the standard deviation for the AA group.
Results
The mean pain VAS of all cases improved significantly from 5.5 ± 2.3 (range, 2-10) preoperatively to 0.9 ± 1.2 (range, 0-5) at final follow-up (P < .001). Mean pain VAS of the TAA group improved from 6.2 ± 2.3 (range, 3-10) preoperatively to 0.8 ± 1.3 (range, 0-5) at the final follow-up; that of the AA group improved from 4.5 ± 2.2 (range, 2-10) to 0.7 ± 0.9 (range, 0-3) (P = .002 and .005, respectively). Preoperatively and at final follow-up, no difference could be detected in mean pain VAS of the 2 groups (P = .088 and .927, respectively) (Table 2). Effect size d value was 0.16, which means a small effect.
Clinical Outcomes and Radiographic Complications.
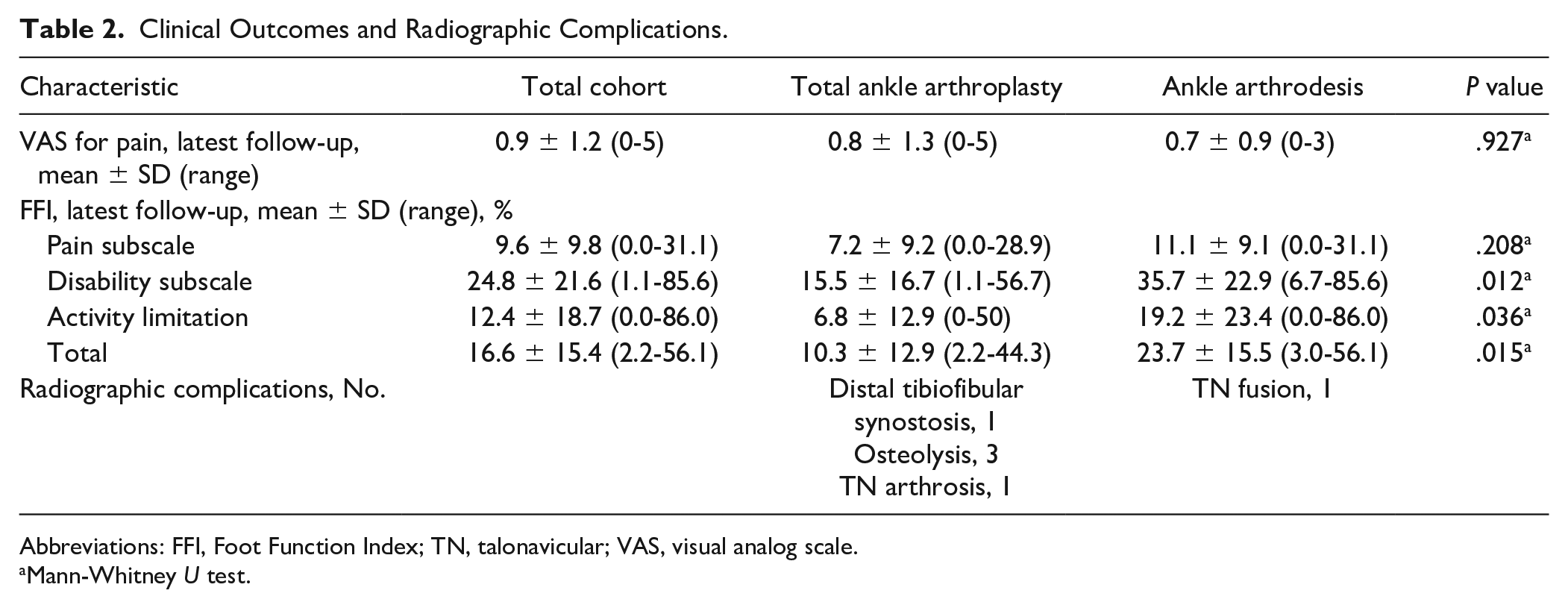
Abbreviations: FFI, Foot Function Index; TN, talonavicular; VAS, visual analog scale.
Mann-Whitney U test.
In the TAA group, the FFI scale improved from 59.6% ± 15.8% (range, 27.4%-87.4%) preoperatively to 10.3% ± 12.9% (range, 2.2%-44.3%) at the final follow-up (P = .001). The AA group improved from 61.5% ± 15.0% (range, 39.6%-82.6%) to 23.7% ± 15.5% (range, 3.0%-56.1%) (P = .007). No significant difference in the FFI scale between groups preoperatively could be detected with the numbers available (P = .927), but a significant difference was observed at the final follow-up (P = .015). Effect size d value of FFI scale was −0.87, which means a large size of effect. The FFI subscales (pain, disability, and activity limitation) of all cases improved significantly from 61.7% ± 18.7% (range, 26.7%-91.1%), 71.9% ± 16.5% (range, 32.2%-96.7%), and 48.7% ± 25.5% (range, 0.0%-96.0%) to 9.6% ± 9.8% (range, 0.0%-31.1%), 24.8% ± 21.6% (range, 1.1%-85.6%), and 12.4% ± 18.7% (range, 0.0%-86.0%), respectively (P < .001, P < .001, and P < .001, respectively). Among the FFI subscale results, no difference in pain subscale between the 2 groups could be detected with the numbers available (P = .208), but the TAA group demonstrated better results on the disability and activity limitation subscales (P = .012 and .036, respectively) (Table 2). Effect size d values of FFI disability and activity limitation subscales were −0.88 and −0.537, which means large and medium size of effect, respectively.
The mean preoperative total ROM was 25.8 ± 13.2 (range, 0-55) degrees, and no significant difference between the 2 groups could be detected with the numbers available (30.8 ± 12.6 [range, 10-55] degrees and 20.6 ± 11.9 [range, 0-35] degrees), respectively (P = .243). The mean preoperative dorsiflexion range of the ankle exhibited a difference between the TAA group and AA group (2.8 ± 5.3 degrees vs −6.1 ± 10.7 degrees, P = .043) with the numbers available.
After TAA, ROM changed from 30.8 ± 12.6 (range, 10-55) degrees to 37.3 ± 12.8 (range, 20-60) degrees, but this did not reach statistical significance. However, the plantarflexion range of the ankle improved significantly from 28.0 ± 12.5 (range, 10-50) degrees to 38.5 ± 9.7 (range, 20-55) degrees (P = .046).
Two patients with TAA developed an intra-articular hematoma during the perioperative period. With coagulation factor supplementation and appropriate wound management, this improved without additional complications. In 1 case of TAA, heterotopic ossification around the distal tibiofibular area was observed. In 3 cases after TAA, a small amount of osteolysis was observed on routine follow-up around the posterior part of the tibial component. The demographic data and clinical results of these 3 cases are summarized in Table 3. However, no significant differences in any variable relative to those of the 13 cases without osteolysis could be detected with the numbers available. One patient with osteolysis (case 2) presented with osteophytes in the talonavicular joint at 2 years and 4 months after the operation. There was some tenderness and pain in the area, but this gradually improved without further operation. No cases of implant loosening or component revision were noted.
Demographic Data of 3 Patients Undergoing Total Ankle Arthroplasty for End-Stage Hemophilic Ankle Arthropathy With Osteolytic Lesions in the Posterior Tibial Area at Final Follow-up.
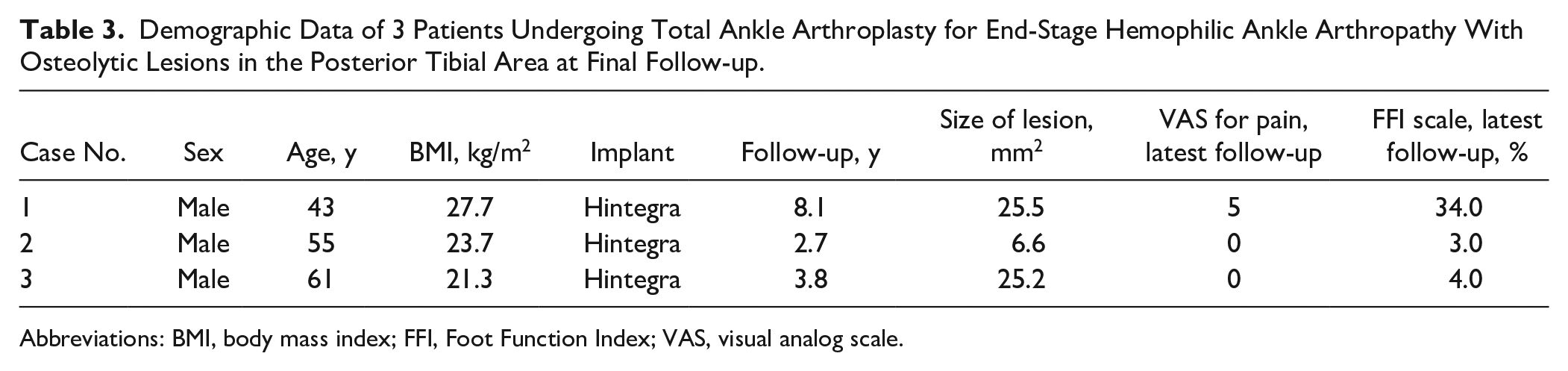
Abbreviations: BMI, body mass index; FFI, Foot Function Index; VAS, visual analog scale.
Good bone union was obtained in all AA cases. There were no cases of nonunion. Six of the 13 cases presented with concomitant arthrosis of adjacent segments, but simultaneous operations for adjacent segments were not performed at the time of AA. In 1 of 6 cases, arthrosis of the adjacent segment had progressed. In the 44-year-old man with arthrosis in the talonavicular joint, spontaneous union was observed 2 years and 2 months after AA. The pain VAS improved from 3 to 1, and FFI scale improved from 39.6% to 27.0%. A case of AA with anterior plate fixation achieved good bone union. Two years later, however, a broken plate was observed in the bridged area to the next segment, which was removed. No other major radiological complications were observed.
Discussion
In this study, both TAA and AA were performed on painful ESHAA, and significant improvements in the pain VAS and FFI scales were identified. The TAA group showed better results on the FFI disability and activity limitation subscales than those of the AA group. After TAA, no significant improvement in ROM was detected with the numbers available. No major complications such as nonunion or component revision were observed.
Arthropathy is one of the most important causes of morbidity in hemophilia, and up to 90% of severely affected patients have this complication. 18 Arthrosis develops into the stages of acute intra-articular bleeding, chronic synovitis, and degenerative arthritis. Intra-articular bleeding occurs in the frequency order of knee, elbow, ankle, shoulder, hip, and wrist joint. 2 Repeated bleeding of the ankle joint begins at 2 to 5 years of age, when gait begins and activity increases. 7 Repeated intra-articular bleeding can cause irreversible damage over time and lead to hemophilic arthropathy. The quality of life of the severe hemophiliacs examined appears to have been affected. 3 In patients with severe hemophilic arthropathy, painful complaints have been reported in the order of ankle joint (45.1%), knee joint (39.4%), and elbow joint (7.0%). 37 As such, the incidence of hemophiliac ankle arthropathy is relatively high, 18 occurs at a relatively young age, and is likely to become a target joint by repeated intra-articular bleeding. Furthermore, the severe pain affects the patient’s quality of life, and this condition can easily progress to end-stage arthrosis. 17
AA and TAA are the main treatment options for end-stage nonhemophilic ankle arthritis, and numerous studies have been reported.15,28 AA can provide pain relief and proper ankle alignment but alters the normal function of the hindfoot and adds strain to adjacent segments, which leads to degenerative changes in adjacent joints. 23 Although TAA had a high probability of failure and poor results with early generation implants, a survival rate of 89% was reported with newly developed implants in a 10-year follow-up study. 41 In a recent meta-analysis, 15 the 2 methods performed equally well based on the American Orthopaedic Foot & Ankle Society (AOFAS) Ankle-Hindfoot score, 36-item Short-Form Health Survey (SF-36) 38 physical component summary subscale and mental component subscale, pain VAS, and patient satisfaction. The implementation of TAA has gradually increased due to improved implant design, advances in surgical techniques, positive literature reports, and increased patient needs. 26
In hemophilic ankle arthropathy, arthroscopic and/or open synovectomy, osteophyte resection, or corrective osteotomy may be considered depending on initial symptoms.24,40 However, in recalcitrant ESHAA, more invasive surgery such as distractive arthroplasty, AA, or TAA may be required.4,5,7,33-35 To date, the standard treatment is AA, 3 but the scientific evidence for this is poor compared to that for nonhemophilic ankle arthritis. Luck and Kasper 16 first performed TAA in 1978 for hemophilic ankle arthropathy but failed to follow up and did not report adequate results. Since then, case reports, including 3 cases by van der Heide et al, 34 6 short-term follow-up cases by Min and Zhang, 19 and reports from Berdel et al 6 have been presented. Barg et al 5 prospectively followed 10 cases of TAA for a mean of 5.6 years and suggested that TAA was an effective alternative to AA based on pain relief and improvement of the SF-36 scale. 38 Strauss et al 31 reported 2 cases of deep infection in 10 patients with a mean follow-up duration of 3 years and reported good clinical results without infection. Preis et al 25 presented the possibility of various treatment methods through a report of 14 cases of retrospective results, including the conversion to TAA after AA.
Precise criteria have yet to be suggested regarding the indication for AA and TAA in ESHAA. Nevertheless, if the morphological and epidemiologic features of hemophilic arthropathy are carefully applied, it would be reasonable to apply the indications for nonhemophilic ankle arthropathy. The appropriate indication criteria related to the patient’s age are not clear in either hemophilic or nonhemophilic arthropathy. Several comparative studies of AA and TAA in nonhemophilic arthritis demonstrated that most TAAs were performed at a mean age of 70 years. 15 However, Rodrigues-Pinto et al 27 suggested that since 80% of ankle arthritis causes are traumatic, it should be considered that patients tend to be relatively young with high demands for physical activity; thus, the aspects of hip and knee joints that led to high satisfaction in young patients should also be adapted to the ankle joint. Vora and Kelikian 36 have claimed that physical activity demands, expectations, demands of the patients, and functional age rather than chronological age should be considered when establishing end-stage arthritis treatment strategy. In a health-related quality-of-life study of patients with moderate to severe hemophilia, Miners et al 20 reported that physical function and roles were decreased compared to that of healthy adults of the same age group based on the SF-36 scale. As such, TAA may be considered a cautious treatment option for ESHAA patients with relatively low physical activity compared to that of the same age group. The mean age of the TAA group in this study was 41.7 years, and previous TAA reports on hemophilic ankle arthropathy performed in the 40s may be interpreted in a similar manner.5,25,31
No significant improvement in joint ROM was detected before and after TAA in this study based on the numbers available, which is similar to previous studies. 5 Therefore, the consideration of TAA for joint ROM improvement requires careful evaluation. The TAA group presented with superior outcomes in the FFI disability and activity limitation subscales compared to those of the AA group, likely due to the relatively young patients’ expectations and demands. Future studies should confirm this. In this study, the FFI scale was used before and after the operation for clinical evaluation. This is an evaluation tool based on a VAS with 10 stages comprising 3 subscales.1,8 The reliability and validity of this test in patients with ankle and foot disease have been demonstrated, and a significant correlation with SF-36 has been reported. 29 Previous studies on TAA for hemophilic arthropathy have adapted the AOFAS score for clinical evaluation, which has not been fully validated. 14 Therefore, an additional discussion of the scale that most objectively reflects the status of ESHAA before and after the operation is needed. Further discussion regarding the nature and progression of adjacent arthrosis after operation is also necessary.
The clinical results of total joint replacement for hemophilic arthropathy of the hip and knee joint have been reported. Strauss et al 32 reported clinical improvement in ROM, Harris hip score, and VAS for pain at a mean 11.4-year follow-up period of total hip arthroplasty in 49 cases of severe hemophilic arthropathy. In a study by Yoo et al, 39 osteolysis of the acetabular side was shown in 3 of 27 cases, while osteolysis of the femoral side was shown in 3 of 27 cases with cementless THA. Revision was performed in 1 case of oteolysis of the acetabular side. A meta-analysis of total knee arthroplasty studies showed improved ROM and knee scores, but the complication rate was 31.5%. 21 Infection and bleeding were the main source of complications, while complications due to osteolysis have not been reported. Previous reports of TAA on ESHAA did not provide sufficient analytic information on osteolysis. Three of the 16 TAA cases had osteolysis, and thus it appears to be relatively common. However, all were found by chance during the routine follow-up. Moreover, no significant differences in any variable relative to those of the 13 cases without osteolysis could be detected with the numbers available. There were no associated symptoms and no size deterioration on the follow-up.
This study has some limitations. First, it is a retrospective analysis and therefore has methodological limitations. Second, each treatment was carried out individually for the situation of each patient at that time, which is somewhat heterogeneous, including implant designs, approaches, and fixation techniques. Third, longer-term follow-up is needed to understand the longevity of the TAA in ESHAA. Fourth, sample size was not enough in this study. To compensate for this problem, the effect size was measured. Because the effect size, which represents both the actual difference and relevance between 2 groups, is not affected by the sample size, it can be used to appropriately substitute methods that use the P value. Cohen 10 arbitrarily classified and assigned each effect size with a value—small (0.2), medium (0.5), or large (0.8)—in an effort to help researchers intuitively understand. To that end, the actual mean differences found in each of FFI disability and activity subscales in the TAA group were measured as large and medium, respectively. This indicated that there were statistically meaningful differences regardless of the number of samples. However, the values suggested by Cohen are still relative and may vary depending on the characteristics of the population and the variables involved. Therefore, while the effect size can be used as a helpful reference, it should not be accepted as an absolute indicator. Nevertheless, this is the first study to compare and analyze the results of 2 treatment options using clinically validated scales with more cases than that in previous studies.
In conclusion, both TAA and AA in ESHAA resulted in significant improvement in pain VAS and FFI scales. Moreover, TAA resulted in better clinical outcomes in FFI disability and activity subscales than those of AA. These results suggest that TAA may be considered a surgical option alongside AA for ESHAA.
Supplemental Material
FAI929002_disclosures – Supplemental material for Comparison of Total Ankle Arthroplasty and Ankle Arthrodesis in End-Stage Hemophilic Arthropathy
Supplemental material, FAI929002_disclosures for Comparison of Total Ankle Arthroplasty and Ankle Arthrodesis in End-Stage Hemophilic Arthropathy by Jungtae Ahn, Myung Chul Yoo, Jeunghwan Seo, Moonsu Park and Bi O Jeong in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.