
Abstract
Background:
Tranexamic acid (TXA) is a medication that has been shown to decrease blood loss and risk of blood transfusion in total knee and total hip arthroplasty. The purpose of this study was to evaluate the use of TXA in patients undergoing total ankle arthroplasty (TAA). We hypothesized there would be less blood loss and wound complications in patients receiving TXA.
Methods:
A retrospective review of 2 patient cohorts operated on by 2 surgeons was performed from 2010 to 2018. We compared a group of TAA patients that did not receive TXA vs a subsequent group that received TXA. Patients received 1g intravenous TXA before the tourniquet was inflated followed by another 1 g after release of the tourniquet. Intraoperative blood loss was recorded and preoperative hemoglobin and hematocrit levels were compared to postoperative levels. Intraoperative and postoperative complications were compared between the 2 groups. A total of 119 patients were included in the study, of whom 55 received TXA. No significant difference existed between the 2 groups in gender, age, body mass index, or Charlson comorbidity index.
Results:
There was no difference in estimated blood loss, postoperative hemoglobin/hematocrit values or preoperative to postoperative change in hemoglobin/hematocrit values. Additionally, there was no difference in wound complications or overall complication rate between the groups.
Conclusion:
TXA has been shown to be effective in total knee and total hip arthroplasty in decreasing blood loss and transfusion risk. We did not find it to be effective in reducing intraoperative blood loss, perioperative blood loss, or wound complications in TAA.
Level of Evidence:
Level III, comparative study.
Introduction
Total ankle arthroplasty (TAA) is a procedure that is continuing to increase in popularity among orthopedic surgeons. According to Singh et al, 16 from 1998 to 2010, there was a 6-fold increase in the number of total ankle arthroplasty procedures performed in the United States. Pugely et al 15 sampled the Medicare database and showed that total ankle arthroplasty volume increased from 72 procedures in 1991 to 888 in 2010. As with any operative procedures, total ankle arthroplasty is not without potential complications. Studies have shown some complications of TAA including implant failure, fracture, infection, need for blood transfusion, death, pneumonia, deep vein thrombosis, pulmonary embolism, cerebrovascular accident, myocardial infarction, hematoma, infection, and wound complication.2,9,11,14,17 The rate of perioperative blood loss, transfusion rate, and hematoma formation following total ankle arthroplasty has been shown to be relatively low. 6
Tranexamic acid (TXA) is a medication that has been studied extensively over the past 2 decades in the total hip arthroplasty and total knee arthroplasty literature. It has been shown to reduce perioperative blood loss and transfusion rates with both total hip and total knee arthroplasty.4,7,8,18,20,22 There has been a paucity of literature investigating TXA use in foot and ankle surgery. In a recent article, Nodzo et al 13 showed, in a retrospective study, that TXA use in total ankle arthroplasty resulted in decreased perioperative blood loss, hemarthrosis, and wound complications when compared with patients who did not receive TXA. In another study evaluating surgery about the foot and ankle, Xie et al 21 showed that TXA reduced the postoperative blood loss wound complication rate with no reported complications.
The purpose of this study was to retrospectively review patients who underwent total ankle arthroplasty and received TXA preoperatively and compare this group of patients to a control group who underwent total ankle arthroplasty without TXA use. The primary outcomes included intraoperative blood loss, postoperative blood loss, and postoperative wound complications. Given the results of previous studies, our hypothesis of this study was that the use of TXA intraoperatively would reduce perioperative blood loss and wound complications.
Methods
Institutional review board approval was obtained for this retrospective multicenter study. Inclusion criteria included all patients older than 18 years undergoing a primary total ankle arthroplasty for end-stage ankle osteoarthritis at 2 institutions by 2 foot and ankle fellowship-trained senior surgeons. Patients were excluded if they were undergoing a revision total ankle arthroplasty, had a contraindication to TXA use or had known coagulopathies. In all patients, an anterior approach to the ankle was used. Tourniquets were used in all patients and no drains were used in any patients; the tourniquets were deflated after components were implanted and hemostasis was obtained before layered wound closure. Both surgeons used the same total ankle implants (Wright Medical Infinity, Wright Medical, Memphis, TN), which was used in a non cemented fashion in most patients unless the patients had osteoporotic bone. It should be noted that with this system, the company does recommend cement use in the United States. Postoperative anticoagulation included aspirin, unless the patient was at high risk for a deep vein thrombosis or was on an anticoagulant prior to surgery. Postoperative immobilization and weightbearing protocols were similar between the 2 surgeons.
We retrospectively reviewed the charts of 119 patients who underwent total ankle arthroplasty from January 1, 2006, to December 31, 2018, and divided the patient into 2 cohorts: those that received TXA and those that did not receive TXA. In the patients that received TXA, 1 g of intravenous TXA was administered before inflating the tourniquet and 1 g was administered after release of the tourniquet. Patients received TXA based on the attending surgeons’ preference. TXA was primarily used by one surgeon (V.R.) in this study who initially did not use TXA, but began using TXA for total ankle arthroplasty based on the literature for total hip and knee arthroplasty.
The primary outcomes for this study included intraoperative blood loss and postoperative wound complications. Intraoperative blood loss was estimated by the operating surgeon based on the weight of the operative sponges and volume of blood within the suction canisters. Postoperatively, patients’ wounds were monitored for drainage, hematoma formation, necrosis, dehiscence, and delayed healing. Other data included were preoperative hemoglobin values, postoperative day 1 hemoglobin values, intraoperative complications, need for postoperative transfusion, postoperative deep vein thrombosis, pulmonary embolism, cerebrovascular event, cardiovascular event, and limb ischemia. To assess intergroup homogeneity, demographic data included age, sex, ethnicity, body mass index, reason for TAA, preoperative aspirin use, and Charlson comorbidity score.
Statistical Analysis
Differences between the group of patients who received TXA and the group who did not receive TXA were analyzed. Means were compared between groups using a 2-sample t test. Medians were compared between groups using a Wilcoxon rank sum test for skewed distributions. Proportions were compared between groups using a chi-square test unless the expected frequency counts were small (at least 20% with expected value less than 5), in which case, the Fisher exact test was used. A 2-sided 0.05 alpha level was used to define statistical significance.
Based on the clinical trial results of TXA use among patients with calcaneal fractures reported by Xie et al, 21 we estimate that the standardized effect size for mean postoperative blood loss at 24 hours postsurgery would be 0.75 (mean ± SD for TXA 110 ± 160 mL vs 320 ± 360 mL for control). 5 With a standardized effect size of 0.75, assuming a 2-sided 0.05 alpha level, a total sample size of 64 (24 TXA and 40 control participants) would be required to detect the stated difference with 80% power. If we assumed that 20% of the variability in the clinical use of TXA could be explained by confounding factors, addressing selection bias, the minimum total sample size would be increased to 71 (27 TXA and 44 control participants).5,10
Results
Of the 119 patients included in this study, 55 received TXA and 64 did not. Demographics for our sample of patients are shown in Table 1. Table 2 shows the primary outcomes for our study. When comparing the TXA group and the non-TXA group, there was no difference in regard to preoperative to postoperative day 1 change in hemoglobin or hematocrit values. Additionally, there was no difference in the preoperative or postoperative hemoglobin and hematocrit values between the 2 groups. In the non-TXA group, 54 patients had postoperative hemoglobin and hematocrit values, and in the TXA group, 32 patients had postoperative hemoglobin and hematocrit values available. There was no difference in the estimated intraoperative blood loss between the 2 groups. Only 1 blood transfusion was needed postoperatively and was in the TXA group.
Patient Demographics.
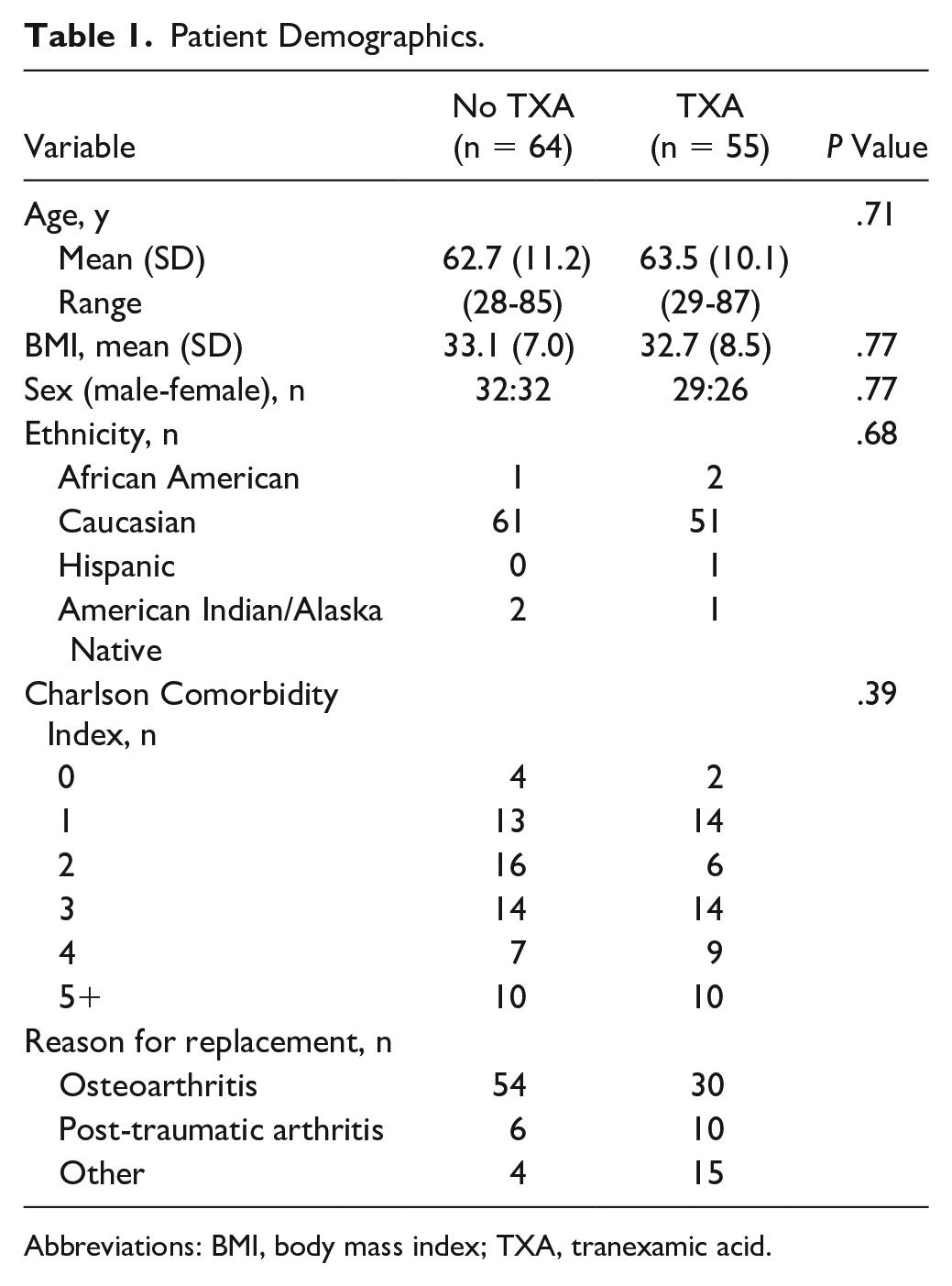
Abbreviations: BMI, body mass index; TXA, tranexamic acid.
Blood Loss and Complications. a
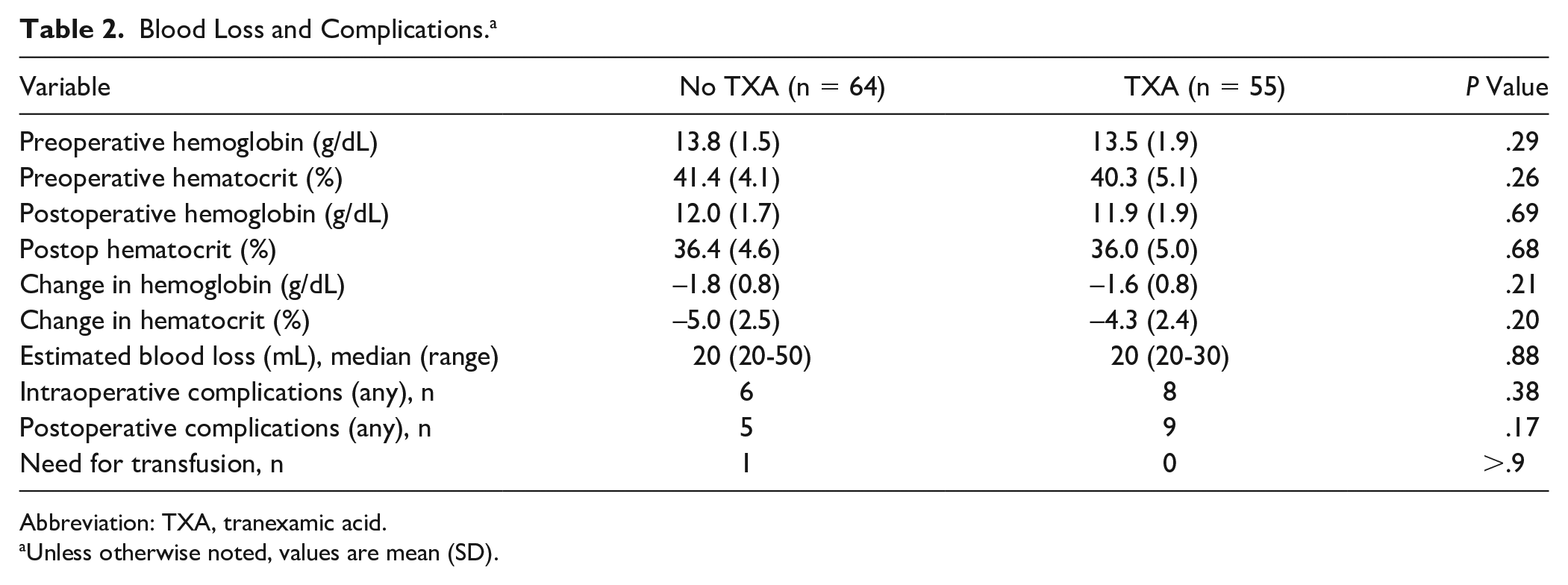
Abbreviation: TXA, tranexamic acid.
Unless otherwise noted, values are mean (SD).
There were no differences in the intraoperative or postoperative complications between the 2 groups. The postoperative complications are shown in Table 3. Surprisingly, the TXA group had a higher number of early postoperative wound complications (<3 months), but it did not achieve statistical significance (P = .09). There was one pulmonary embolism which was in a patient that did not receive TXA.
Complications Following Total Ankle Arthroplasty.
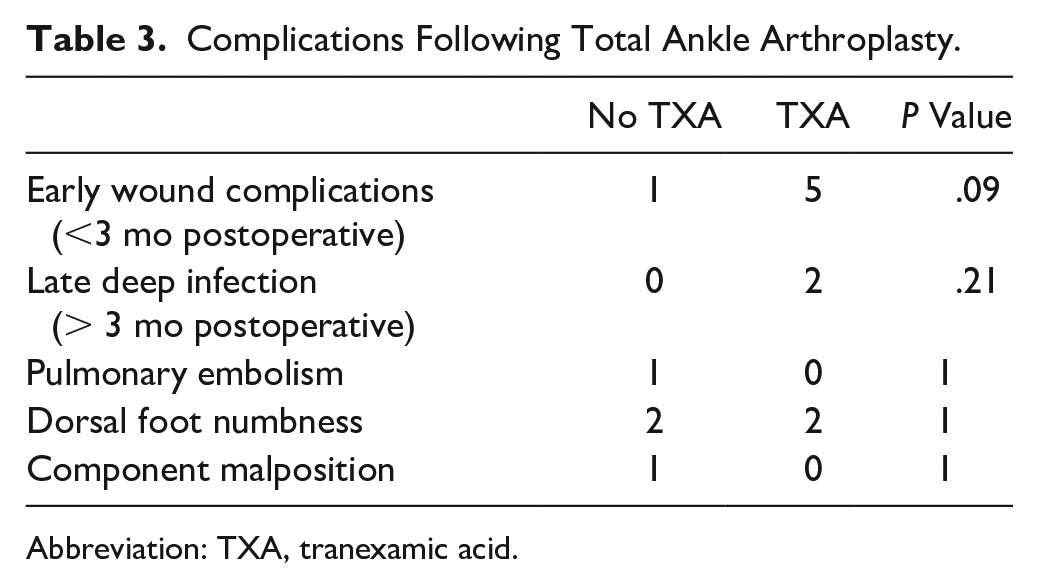
Abbreviation: TXA, tranexamic acid.
Discussion
Total ankle arthroplasty for symptomatic ankle osteoarthritis is a procedure that continues to gain popularity among orthopedic surgeons as implant survival and clinical outcomes continue to improve. 19 When compared to total hip and total knee arthroplasty, total ankle arthroplasty has been shown to have a significantly lower rate of perioperative blood loss and blood transfusion.1,12 The rate of blood transfusion following total ankle arthroplasty has been shown to be 1.1% to 1.3%.6,11 Although the rate of blood transfusion is low following total ankle arthroplasty, it has been shown to significantly increase in-hospital complications and hospital cost. 6
TXA has been extensively studied in both total knee and total hip arthroplasty and has been shown to reduce intraoperative blood loss and transfusion rates in the perioperative period.4,7,8,18,20,22 Oral, intravenous, and topical administration of TXA have all been shown to be effective in total knee and total hip arthroplasty.4,7,8,18,20,22 Despite the extensive literature investigating TXA use in total knee and total hip arthroplasty, there is a paucity of literature involving the use of TXA in TAA. In a recent study, Nodzo et al 13 retrospectively evaluated the use of TXA in total ankle arthroplasty. They found that TXA use decreased perioperative blood loss, hemarthrosis, and wound complications compared with patients who did not receive TXA. These findings are contradictory to our findings in which we found no difference in intraoperative blood loss and postoperative change in hemoglobin or wound complications. Additionally, there was no difference in the blood transfusion rate. Worth mentioning is that despite tourniquet use in our study, both senior surgeons deflated the tourniquet after implantation, and hemostasis was performed before layered operative anatomical closure of the anterior ankle wound. Although the thin soft tissue envelope of the anterior ankle poses significant risk for wound breakdown in cases of hematoma formation after TAA, meticulous attention to hemostasis might have contributed to the aforementioned findings and lack of difference between groups in our study. Based on the findings from our study, we believe that TXA use in total ankle arthroplasty may not be as beneficial in the perioperative period as it is in total hip and total knee arthroplasty. One potential complication of TXA use is thrombosis, which could lead to pulmonary embolus or stroke, however, in our study the only patient with a pulmonary embolus was a patient who did not receive TXA.
Our study does have several limitations that need to be pointed out. It is retrospective in nature, which allows for potential selection bias. Another limitation is that the intraoperative blood loss may have been underestimated as the system used for estimating intraoperative blood loss may not have accounted for the exact amount of total blood loss. 3 Additionally, as noted above, not all patients had postoperative day 1 hemoglobin values, which could have affected the results. The postoperative hemoglobin values that were obtained could have been affected by the perioperative intravenous fluid that the patients received. Our sample size was relatively small and was underpowered to address rare outcomes, and thus further studies with larger sample sizes would be beneficial to detect clinical differences.
Conclusion
Tranexamic acid has been shown to be effective in reducing perioperative blood loss and transfusion rate in total knee arthroplasty and total hip arthroplasty. Based on our findings, we believe it may not be effective in reducing intraoperative blood loss, perioperative blood loss, transfusion rate, or wound complications in total ankle arthroplasty.
Supplemental Material
FAI934889disclosure – Supplemental material for Effect of Tranexamic Acid on Wound Complications and Blood Loss in Total Ankle Arthroplasty
Supplemental material, FAI934889disclosure for Effect of Tranexamic Acid on Wound Complications and Blood Loss in Total Ankle Arthroplasty by R. Garrett Steinmetz, Laura Luick, Shaun Tkach, Spencer Falcon, Julie Stoner, Kimberly Hollabaugh, Vytautas Ringus and Amgad M. Haleem in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.