
Abstract
Background:
Both the percutaneous technique with arthroscopic assistance, also known as arthroscopic Broström (AB), and the arthroscopic all-inside ligament repair (AI) are widely used to treat chronic lateral ankle instability. The aim of this study was to compare the clinical outcomes of these 2 arthroscopic stabilizing techniques.
Methods:
Thirty-nine consecutive patients were arthroscopically treated for chronic ankle instability by 2 different surgeons. The AB group comprised 20 patients with a mean age of 30.2 (range, 18-42) years and a mean follow-up of 19.6 (range, 12-28) months. The AI group comprised 19 patients with a mean age of 30.9 (range, 18-46) years and mean follow-up of 20.7 (range, 13-32) months. Functional outcomes using the American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot score and visual analog pain scale (VAS) were assessed pre- and postoperatively. Range of motion (ROM) and complications were recorded.
Results:
In both groups the AOFAS and VAS scores significantly improved compared with preoperative values (P < .001) with no difference (P > .1) between groups. In the AB group the mean AOFAS score improved from 67 (range, 44-87) to 92 (range, 76-100) and the mean VAS score from 6.4 (range, 3-10) to 1.2 (range, 0-3). In the AI group the mean AOFAS score changed from 60 (range, 32-87) to 93 (range, 76-100) and the mean VAS score from 6.1 (range, 4-10) to 0.8 (range, 0-3). At the final follow-up 8 complications (40%) were recorded in the AB group. In the AI group 1 complication (5.3%) was observed (P < .05).
Conclusion:
Both the AB and AI techniques are suitable surgical options to treat chronic ankle instability providing excellent clinical results. However, the AB had a higher overall complication rate than the AI group, particularly involving a painful restriction of ankle plantarflexion and neuritis of the superficial peroneal nerve.
Level of Evidence:
Level III, retrospective comparative study.
Keywords
Introduction
Ankle sprains are one of the most common orthopedic injuries, with the lateral ligament complex being involved in 85% of cases.14,16 Ankle sprains can lead to instability in 10% to 40% of patients, and some of them will require surgical intervention to restore ankle stability. 6,13
In the past, anatomical open lateral ligament repair as originally described by Broström was considered the gold standard procedure to surgically treat ankle stability. 5 However, the potential for addressing both the instability and any intra-articular associated pathology arthroscopically has deemed ankle arthroscopy as better positioned to be the technique of choice when treating ankle instability.
Hawkins 19 described the first arthroscopic ankle stabilization technique in 1987, although subsequent complaints arose due to the prominent staple used in that technique. Since then, the technical aspects of ankle arthroscopy and instruments have significantly evolved, providing much better results in the treatment of ankle instability.
As has been the case in open surgery, a number of arthroscopic techniques have been proposed to restore ankle stability. These can be broadly classified into arthroscopic-assisted and all-arthroscopic techniques. Arthroscopic-assisted techniques combine arthroscopic procedures with a percutaneous 1 or mini-open approach, 19 whereas the all-arthroscopic techniques 32 involve a fully arthroscopic procedure. All-arthroscopic techniques can be further subdivided into ligament repair and ligament reconstruction or ligamentoplasty. The emergence of publications reporting excellent clinical results has helped to popularize both arthroscopic-assisted and all-arthroscopic ligament repairs.8,23,25,32
The percutaneous technique with arthroscopic assistance has also been termed arthroscopic Broström (AB). The procedure entails arthroscopic insertion of anchors into the fibula and a percutaneous step to stitch the lateral ligament and the inferior extensor retinaculum (IER). The technique yields excellent clinical results despite a high rate of reported complications (5.3%-29%) due to neurological entrapment or prominent implants.8,18,22 The all-arthroscopic ligament repair technique, popularized as the arthroscopic all-inside ligament repair (AI), is an anatomical repair of the lateral ligaments under direct arthroscopic visualization with the use of anchors.32,33 Excellent clinical results have been reported with a low rate of complications, mostly minor ones.17,27,32
The purpose of this study was to compare the clinical outcomes of 2 arthroscopic stabilizing techniques used for chronic lateral ankle instability: the percutaneous technique with arthroscopic assistance and the all-arthroscopic ligament repair.
Methods
From February 2016 to June 2018, 39 consecutive patients were arthroscopically treated for chronic ankle instability, after being assessed due to limitations in their daily activities. Surgeries were performed by 2 surgeons trained in foot and ankle arthroscopy, each with more than 3 years of experience and more than 30 cases performed of the described techniques.
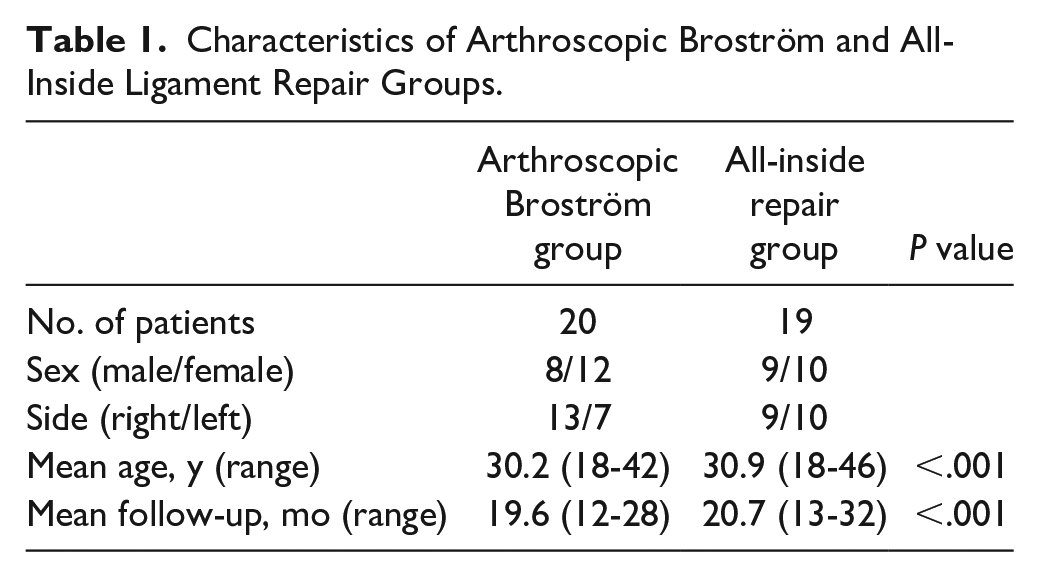
Patients were included in 2 groups: the first one underwent the percutaneous technique with arthroscopic assistance (AB), and the second the arthroscopic all-inside ligament repair (AI). Each technique was always performed by the same surgeon, without crossing over. The AB group comprised 20 patients (8 males and 12 females) with a mean age of 30.2 (range, 18-42) years. The right ankle was affected in 13 cases. The mean follow-up was 19.6 (range, 12-28) months. The AI group comprised 19 patients (9 males and 10 females) with a mean age of 30.9 (range, 18-46) years. The right ankle was affected in 9 cases. The mean follow-up was 20.7 (range, 13-32) months.
Inclusion criteria included chronic ankle instability with a minimum duration of symptoms of 6 months. Clinical findings consisted of anterolateral pain, recurrent ankle sprains, or a feeling of the ankle giving way along with a positive anterior drawer test. All patients underwent a 3- to 6-month course of nonoperative treatment (anti-inflammatory therapy, rest, and physiotherapy) without improving.
Patients with previous foot and ankle surgery, malalignment, or end-stage tibiotalar joint osteoarthritis were excluded. Exclusion criteria consisted of the presence of a talar osteochondral lesion, peroneal tendon pathology, or deltoid ligament tear. Cases of generalized ligamentous laxity and neuromuscular diseases were also discarded from the study. The observation of a calcaneofibular ligament (CFL) tear in addition to the anterior talofibular ligament (ATFL) tear was not an exclusion criterion.
Full weightbearing radiographs and magnetic resonance imaging (MRI) were obtained in all cases to obtain a complete imaging study. No stress radiographs were requested.
Functional outcomes using the American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot score and visual analog pain scale (VAS) were assessed preoperatively and at the latest follow-up (minimum of 1 year after the procedure) by a third surgeon not involved in the surgeries. Preoperative and latest follow-up ankle anterior drawer test scores, range of motion (ROM), and complications were recorded. At the latest follow-up, the anterior drawer test score and ROM were compared with the healthy contralateral side. Ankle ROM was measured by a goniometer and a postoperative deficit >10 degrees with discomfort or pain was classified as a minor complication.
The study was approved by the ethics committee of our institution.
Surgical Technique
The instruments required for the arthroscopic procedure included a 4.0-mm 30-degree scope, 3.5-mm arthroscopic motorized shaver, and burr plus standard arthroscopic instruments. Patients were positioned supine under spinal anesthesia with a thigh tourniquet. Cutaneous landmarks over the anterior aspect of the ankle were highlighted.
An ankle dorsiflexion arthroscopic and no-distraction technique was performed that allowed access to the lateral gutter.9,11 Standard anteromedial and anterolateral portals were established. The anteromedial portal was mainly used as a visualization portal for the arthroscope, whereas instruments were introduced through the anterolateral portal. A full arthroscopic examination was performed, and when present, scar tissue or synovitis was debrided before proceeding to the stabilizing technique.
Percutaneous Technique With Arthroscopic Assistance
The footprint of the remaining ligament on the fibula was debrided with an arthroscopic shaver to create a rough area that would promote healing.
Two bone anchors (3.5 × 10–mm CorkScrew; Arthrex, Naples, FL) were introduced through the anterolateral portal and placed 1 and 1.5 cm proximal to the tip of the fibula (Figures 1 and 2). 31 Sutures were pulled out from the anterolateral portal. Next, with the ankle in neutral position, sutures coming from the distal anchor were passed inside out with the use of a suture passer (SutureLasso; Arthrex). The suture passer loaded with one of the sutures was directed first proximally to the peroneal tendons, at about 1.5 cm distal to the apex of the fibula; then a second suture was passed 1 cm proximal to the first suture. Next, sutures from the second anchor were passed with the suture passer at about 1 cm medial to the last suture, and the same with the other suture at 1 cm medial from it (Figure 3). Sutures were intended to penetrate the IER while avoiding the superficial peroneal nerve. Two small incisions were made between sutures in order to subcutaneously retrieve them. Next, with the ankle in neutral dorsiflexion and slight eversion, a sliding knot was made with the sutures in every anchor. The stitch was aimed to grasp the ligament structures, the capsule joint, and the IER. Finally, sutures were cut and the incisions closed. A removable walking booth was applied.
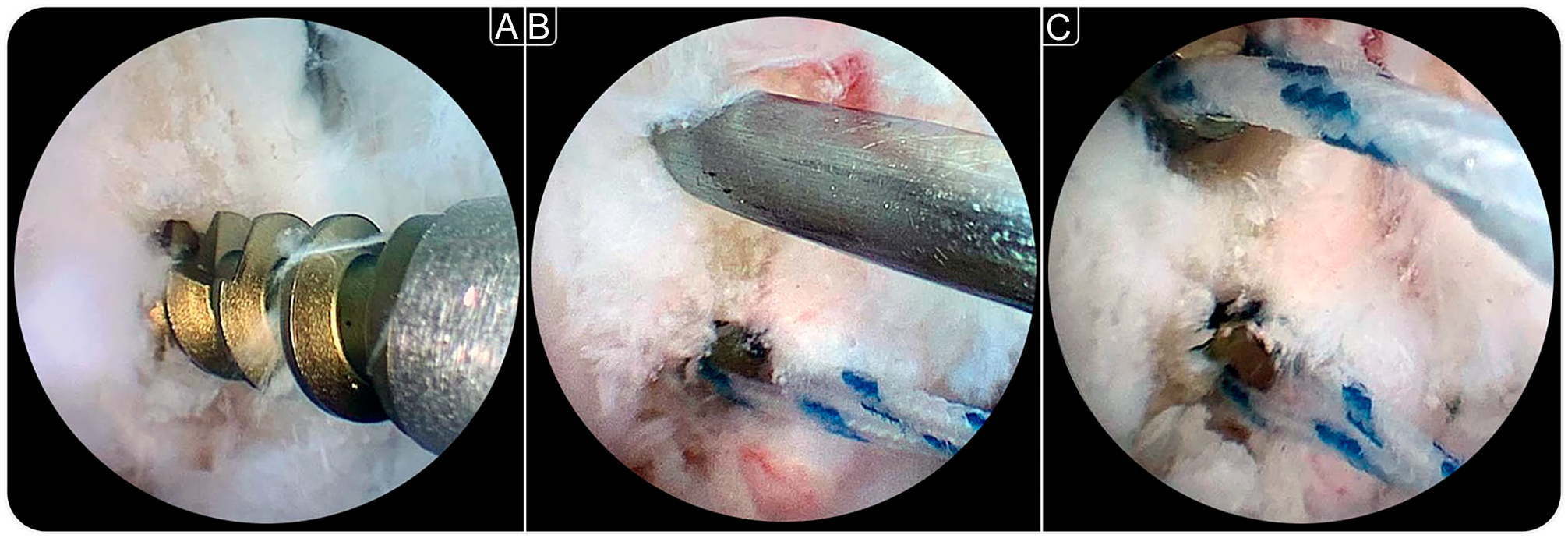
Arthroscopic-assisted placement of 2 suture anchors in the lateral malleolus during arthroscopic Broström. Anchors are placed at approximately 0.5 cm from each other.
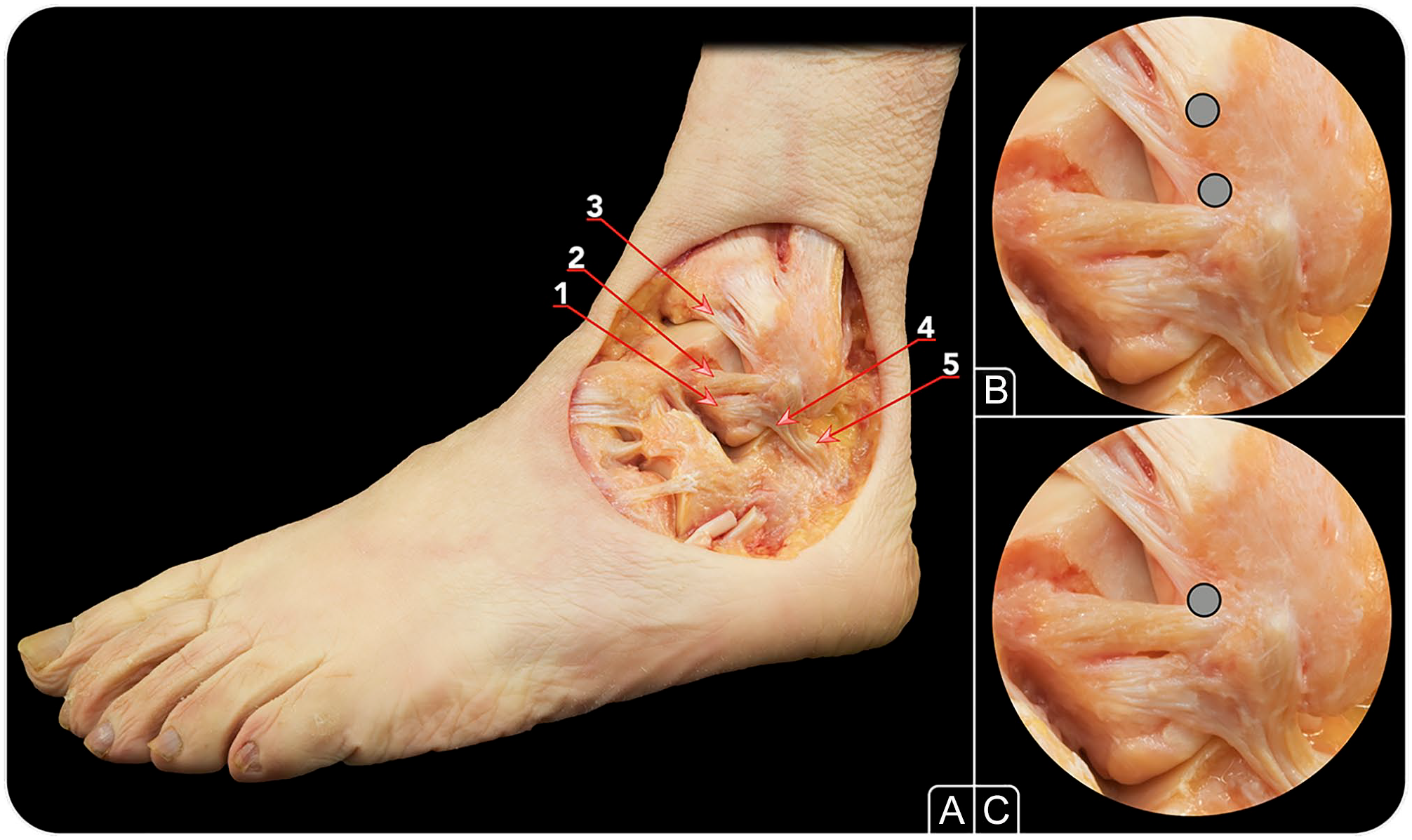
Anterolateral view of an anatomical dissection depicting the (A) anatomy of the lateral ankle ligaments and the position of the anchors for the (B) arthroscopic Broström and (C) all-inside technique. 1, anterior talofibular ligament’s (ATFL’s) inferior fascicle; 2, ATFL’s superior fascicle; 3, distal fascicle of anterior tibiofibular ligament; 4, fibers of the lateral fibulotalocalcaneal ligament complex; 5, calcaneofibular ligament.
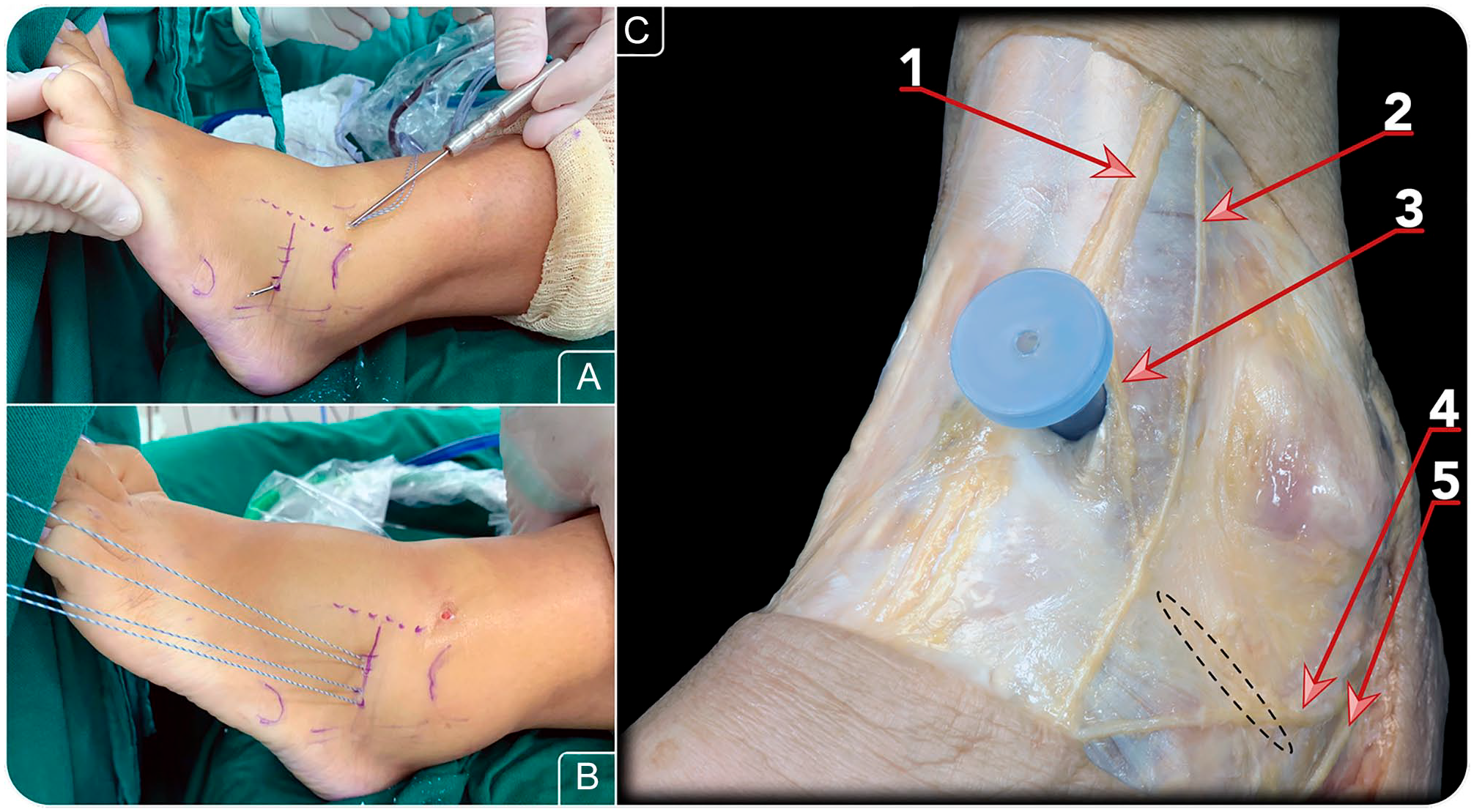
(A,B) Percutaneous suture passing and (C) anatomy of relevant nerves in the arthroscopic Broström. (C) A cannula has been inserted through the anterolateral portal. 1, medial dorsal cutaneous nerve (branch of superficial peroneal nerve); 2, intermediate dorsal cutaneous nerve (branch of superficial peroneal nerve); 3, communicating branch; 4, communicating branch; 5, sural nerve. The dotted area represents the location of the suture.
Arthroscopic All-Inside Ligament Repair
In addition to the standard portals, an accessory anterolateral portal was located about 1 to 1.5 cm proximal to the fibular tip and just anterior to it. The fibular ligament footprint was debrided with an arthroscopic shaver to facilitate the ligament healing. A suture passer (Microsuture lasso 70 degrees curved; Arthrex) was introduced through the anterolateral portal to grasp the ATFL remnant from lateral to medial. Next, the nitinol loop was inserted into the ankle joint and pulled out through the accessory portal. The nitinol was then replaced by a doubled high-resistance suture (Fiberwire No. 0; Arthrex). The limbs of the suture located in the accessory portal were passed through the anterolateral portal. Next, one limb of the sutures was passed through the loop suture, creating a lasso loop. By pulling both suture limbs, the lasso loop was introduced into the joint and the ATFL remnant was grasped. To reattach the ATFL onto its native insertion, a bone tunnel for the knotless anchor was drilled just distal to the fibular attachment of the anterior tibiofibular ligament distal fascicle (Figure 2C). Next, the knotless anchor (Pushlock 2.9 × 15.5 mm; Arthrex) was loaded with sutures and introduced into the fibular tunnel by impaction while the ankle was held in dorsiflexion and eversion (Figure 4). Finally, sutures were cut with arthroscopic scissors and the incisions were closed. A removable walking boot was applied.
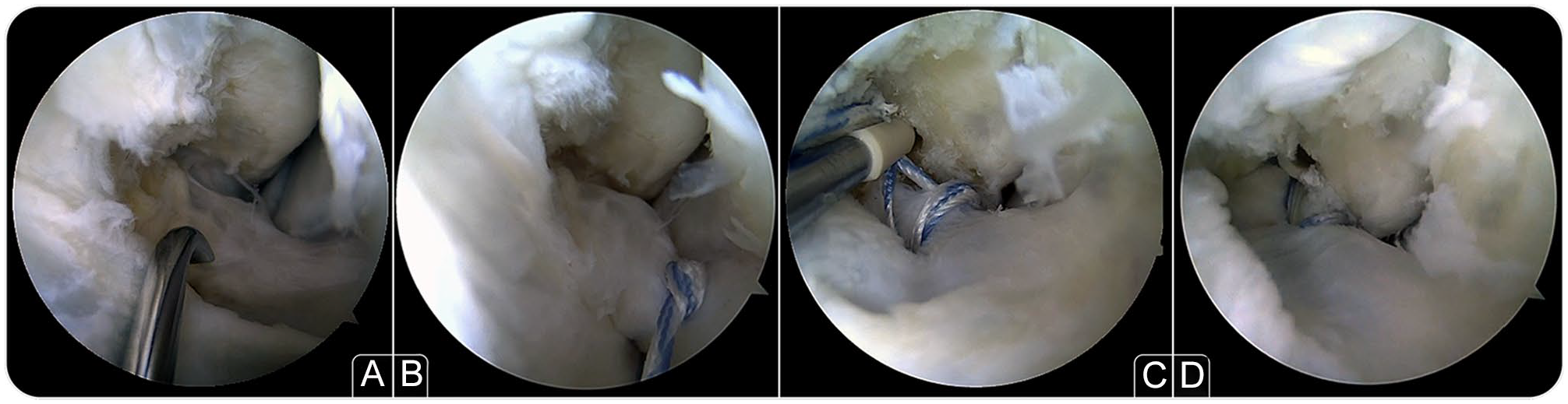
Arthroscopic all-inside anterior talofibular ligament (ATFL) repair. With the help of a (A) suture passer the ATFL is grasped with a (B) high-resistance suture. With a (C) knotless anchor the ligament is reattached onto its (D) native footprint.
Postoperative Protocol
The same postoperative protocol was utilized in both groups. The removable walking boot was kept on at all times for the first 3 to 4 weeks. Partial weightbearing as tolerated with the aid of crutches was recommended from the day following surgery. Formal physiotherapy was initiated after the walking boot was removed. Progressive strengthening and exercises to increase ROM of the ankle were advised. Return to noncontact sports (eg, swimming and cycling) was allowed 2 months postoperatively, and return to any sports without restrictions was allowed 3 months postoperatively depending on muscle conditioning.
Statistical Analysis
Statistical analysis was performed using SPSS 23 (IBM Corp, Armonk, NY). Descriptive results were presented as median, mean, and range. Several tests were used to evaluate the difference between both surgical techniques. For qualitative variables, Pearson’s chi-square and Fisher statistical test were used with continuity correction when necessary. For quantitative variables, the Mann-Whitney U test for independent samples was used, since the null hypothesis of data normality by the Kolmogorov-Smirnov test was rejected. Pre- and postoperative VAS and AOFAS results were also evaluated with the Wilcoxon signed-rank tests. P values <.05 were considered statistically significant.
Results
The 2 groups were homogenous, and no significant difference was noted in mean age and follow-up (Table 1).
Characteristics of Arthroscopic Broström and All-Inside Ligament Repair Groups.
In both groups the AOFAS and VAS scores significantly improved compared with preoperative values (P < .001) (Table 2): in the AB group the mean AOFAS score improved from 67 (range, 44-87) to 92 (range, 76-100) and the mean VAS score from 6.4 (range, 3-10) to 1.2 (range, 0-3); in the AI group the mean AOFAS score changed from 60 (range, 32-87) to 93 (range, 76-100) and the mean VAS score from 6.1 (range, 4-10) to 0.8 (range, 0-3). With regard to the AOFAS and VAS improvement, there was no difference (P > .1) between groups.
Clinical Outcomes of Arthroscopic Broström and All-Inside Ligament Repair Groups.
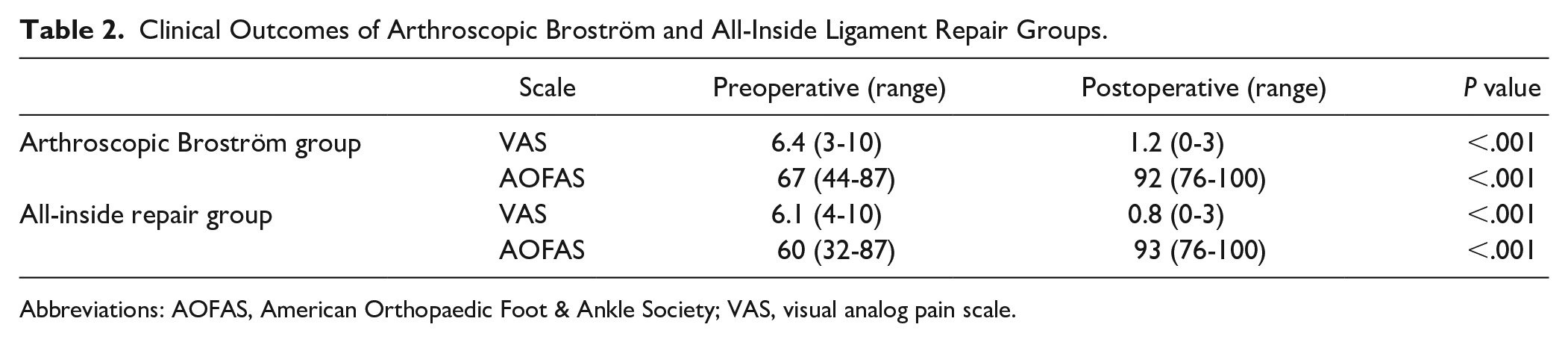
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; VAS, visual analog pain scale.
At the final follow-up, 8 complications (40%) were recorded in the AB group (Table 3). Four patients (20%) presented a deficit in ankle plantarflexion >10 degrees compared with the contralateral side, complaining of mild discomfort or pain when plantarflexing the ankle, and it was considered a minor complication. A transient neuritis of the superficial peroneal nerve was experienced in 3 patients (15%). In 1 case (5%) the prominent suture knots required anchor removal 4 months after surgery. Regarding the AI group, only 1 complication (5.3%) involving painful ankle plantarflexion deficit >10 degrees was observed and was considered a minor complication. No cases of neuritis, anchor prominence, or other complications were noted. The differences in complication rates between groups were statistically significant (P < .05).
Complications of Arthroscopic Broström and All-Inside Ligament Repair Groups.
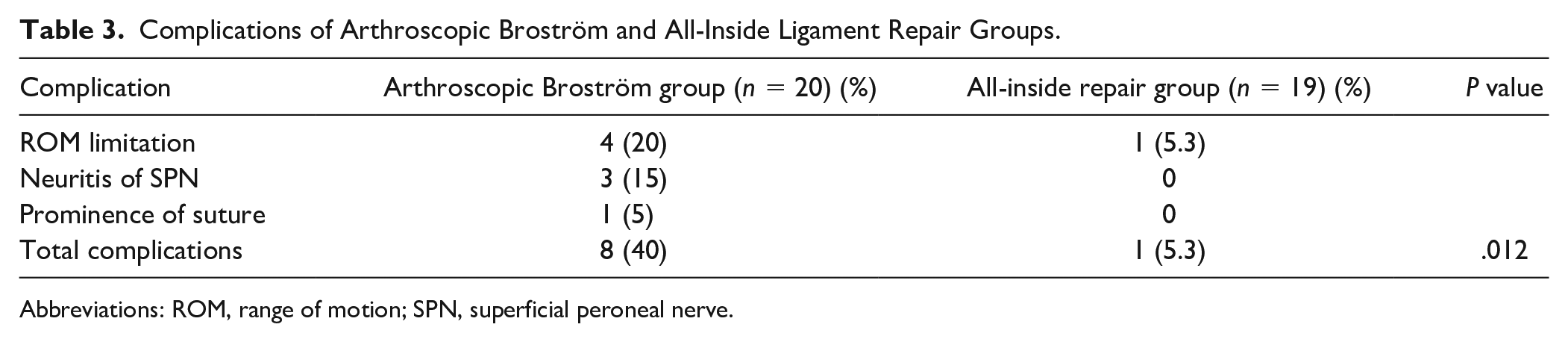
Abbreviations: ROM, range of motion; SPN, superficial peroneal nerve.
At the latest follow-up, all patients reported subjective improvement in their ankle stability. On clinical examination, the anterior drawer test and the talar tilt test were negative in all patients. To date, no patients required ligament revision surgery. All patients returned to daily and recreational activities without limitations. One patient in the AB group had an ankle sprain after returning to sport activities that was treated conservatively.
Discussion
The most important contribution of this study is that both AB and AI demonstrated similarly excellent clinical results according to AOFAS and VAS scores. However, AB had a higher potential risk of complications.
Arthroscopic techniques to treat ankle instability have significantly evolved in the recent years. While attracting interest from foot and ankle surgeons both the AB and the AI have gained further popularity. They present with the advantage of a minimally invasive approach and the added benefit to arthroscopically treat any concomitant intra-articular pathology besides that of ankle instability. Intra-articular pathology is frequently observed in association with ankle instability, and its treatment at the time of surgery is essential for an optimal result.3,20,21,29 We believe the potential for addressing both the instability and any associated pathology places ankle arthroscopy as the technique of choice in the presence of ankle instability.3,7,15,20,21
Previous studies on AB and AI demonstrated excellent clinical results and a low rate of recurrence of instability of the ankle.2,8,18,25,27,32 These findings were confirmed in the current study with a statistically significant improvement in clinical scores (AOFAS and VAS) (P < .001). When the 2 techniques were compared, no differences were observed in clinical results (P > .1). At the latest follow-up, no recurrence of instability was reported in any group.
The main difference observed in the literature between both techniques is in complication rates. Higher complication rates have been reported in the AB technique (5.3%-29%). 18 The 2 most frequently reported complications are neuritis of the superficial peroneal nerve and pain or discomfort due to a prominent anchor or suture knot. 18 This reported higher rate of complications in the AB technique was also confirmed in the current study (40%). Efforts were made to describe a “risk-free” zone for the AB technique, 2 although it is our opinion that nerve complications can be explained due to the percutaneous passage of the suture along the anterolateral aspect of the ankle. In addition, the affected superficial peroneal nerve is known to have multiple anatomical variants plus a mobile path that varies depending on ankle dorsiflexion.12,28 Anatomical variations in the nerve distribution pose higher risk of injury by the subcutaneous suture passing. 28 Moreover, the nerve moves approximately 2.4 mm laterally when the ankle is dorsiflexed when compared with a plantarflexed and inverted position. 23 In contrast to the AB, the AI is a fully arthroscopic procedure in which the ligament is grasped intra-articularly under direct arthroscopic vision, obviating any risk of subcutaneous nerve entrapment. 17
As for the postoperative stiffness, it is accepted that a mild deficit in ROM is expected as a consequence of the surgery itself that tightens the stabilizing structures. However, a ROM deficit >10 degrees may compromise the functional outcome and participation in sports activities. 30 In the current study, 4 of 20 (20%) patients from the AB group reported a painful ROM deficit >10 degrees, while in the AI group it was observed in only 1 of 19 (5%) patients. This difference could be explained due to the anatomical elements and tissues grasped with each technique. During the AI procedure, the ATFL and occasionally the CFL remnant are addressed in what is considered an anatomical repair of the ligaments. 34 In contrast, the AB is not strictly an anatomic ligament repair, as the sutures grasp the ligament, the capsule, the IER, and/or the sural fascia while tightening these up. In the authors’ opinion, by holding these anatomical structures a secondary effect may ensue, creating ROM deficit and possibly scarring in some patients.
The fact that AB is designed to include the IER to the ligament repair is a matter of controversy known from its open Broström counterpart.4,10 The augmentation using the IER requires the presence of the superolateral IER band, only present in 25% of cases. 10 In addition, an anatomical study observed that the superolateral IER band is a thin and fragile band that may not add significant mechanical contribution to the ligament repair. 10 This could explain why incorporation of the IER in the traditional Broström procedure showed any mechanical advantage when compared with just a ligament repair without the IER. 4 It is likely that during the percutaneous AB step what is actually tightened is not only the IER but also subcutaneous fatty tissue that brings no real stability to the construct.
In the present study both surgeons had more than 3 years of experience and had performed more than 30 cases of the techniques described. However, it is worth mentioning after the publication of a recent study demonstrating the reproducibility of AI 17 that it is still a demanding technique that requires a higher level of expertise in arthroscopy than the AB. The arthroscopic step in the AB is minimal and only aimed at placing anchors onto the fibula. However, the AI procedure is fully performed under direct arthroscopic control. As such, AI is not ideally suitable for the novice ankle arthroscopist. The progress through the learning curve of the surgeon can have implications in the results of the AI technique.
The present study was limited by the fact that a small number of patients were included in each group with no randomization process. Data were collected from 2 different patient cohorts and operating surgeons performing 1 technique each. This may incur a risk of design bias, as may the retrospective nature of the study. However, patients were included consecutively in both cohorts, and surgical indications were the same between the groups. A larger case series with a prospective randomized allocation in groups would certainly improve the validity of the study. Despite the fact that goniometry is commonly used in the clinical setting to measure ankle ROM, the literature suggests that it may not be an accurate measuring method; thus, its use could be considered a limitation. 24 Nevertheless, the same method was used for both groups and the deficit of ankle plantarflexion was also a complaint of the patient. The use of an inclinometer or an automatic device for measurement of ankle ROM could improve the reliability of the measurement and the validity of the study. 35
Another limitation is that the AOFAS score used is not a validated outcome scale to evaluate ankle instability, 26 and consequently, some clinical aspects may have been overlooked. A specific clinical score to assess ankle instability would have increased the validity of the study.
Conclusion
In conclusion, both the AB and the AI techniques were suitable surgical options to treat chronic ankle instability providing excellent clinical results. However, a higher rate of overall complications was observed in the AB group, particularly involving a painful restriction of ankle plantarflexion and neuritis of the superficial peroneal nerve.
Supplemental Material
FAI938672_disclosures – Supplemental material for Arthroscopic-Assisted Versus All-Arthroscopic Ankle Stabilization Technique
Supplemental material, FAI938672_disclosures for Arthroscopic-Assisted Versus All-Arthroscopic Ankle Stabilization Technique by Matteo Guelfi, Gustavo Araujo Nunes, Francesc Malagelada, Guillaume Cordier, Miki Dalmau-Pastor and Jordi Vega in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.