
Abstract
Background:
The purpose of this study was to evaluate the clinical and radiological outcomes following a polyvinyl alcohol hydrogel implant in the treatment of hallux rigidus.
Methods:
A retrospective cohort study investigating patients treated with a polyvinyl alcohol hydrogel implant for hallux rigidus was performed. Clinical outcomes were evaluated with the Foot and Ankle Outcomes Score (FAOS) and visual analog scale (VAS) score at the final follow-up. Plain radiographs were assessed postoperatively. Eleven patients (11 feet) with a mean follow-up of 20.9 months (range, 14-27 months) were included. The mean age was 60.3 years.
Results:
All FAOS subscales showed pre- to postoperative improvements, but there was no statistical significance in all subscales. The mean VAS score showed improvement from 4.1 to 3.0 (P = .012). On postoperative plain radiographs, implant subsidence was observed 60% (6/10) at 4 weeks after surgery and 90% (9/10) at the final follow-up. Fifty percent (5/10) showed radiologic lucency around the implant. Forty percent (4/10) had erosion of the proximal phalanx of the great toe. Four patients (36%) reported no improvement following surgery at the final follow-up, which were considered as failures. Three patients required additional surgery related to the implants. An additional patient is waiting to revise the implant.
Conclusion:
Our current cohort study demonstrated a high failure rate with the polyvinyl alcohol hydrogel implant in patients with hallux rigidus. Significant radiologic subsidence with lysis around the implant, erosion of the proximal phalanx countersurface, and implant wear are harbingers for concern in the long term.
Level of Evidence:
Level IV, case series.
Introduction
Hallux rigidus is a common problem that affects 1 in 40 people over the age of 50 years and leads to pain and activity limitation. 6 In advanced-stage arthritis, the current surgical options are limited to a partial or total joint arthroplasty, or first metatarsophalangeal (MTP) arthrodesis. First MTP arthroplasty has been associated with a high complication rate from bone loss, wear debris, implant fragmentation and loosening, and transfer metatarsalgia. 5 Following first MTP arthroplasty implant failure, a salvage of the problem by conversion to a first MTP arthrodesis has been shown to have more complications and even poorer functional results than the index procedure alone. 7 Based on these challenges, primary first MTP arthrodesis is considered the most reliable surgical option for advanced arthritis of the first MTP joint.
A polyvinyl alcohol hydrogel implant (Cartiva Synthetic Cartilage Implant; Cartiva Inc, Alpharetta, GA) has been developed. This synthetic material has a water content comparable to healthy cartilage and a compressive modulus and tensile strength similar to human articular cartilage.2,8 These biomechanical features have been thought to be an ideal material for use in hemiarthroplasty of the first MTP joint. The efficacy and safety of the polyvinyl alcohol hydrogel implant in comparison with first MTP arthrodesis were evaluated in a prospective, randomized clinical trial conducted at 12 centers in Canada and the United Kingdom. The implant hemiarthroplasty demonstrated equivalent pain relief and functional outcomes to a first MTP arthrodesis, with no cases of implant fragmentation, wear, or bone loss. 3
In the United States, this implant was recently approved by the Food and Drug Administration for use in July 2016. Since then, however, there are conflicting reports regarding the success of this implant.1,4,9 The purpose of the current study was to evaluate the clinical, functional, and radiological outcomes following a polyvinyl alcohol hydrogel implant in the treatment of hallux rigidus in a single-surgeon (J.G.K.) case series.
Methods
Patients
All study protocols were approved by the institutional review board of the authors’ institution. A retrospective cohort study investigating patients treated with polyvinyl alcohol hydrogel implant for hallux rigidus was performed. All patients who underwent polyvinyl alcohol hydrogel implantation for the treatment of hallux rigidus between 2016 and 2019 were evaluated. Patients who had grade 2, 3, or 4 hallux rigidus based on Coughlin classification and failed nonoperative treatment for at least 3 months were indicated for the polyvinyl alcohol hydrogel implant procedure. Exclusion criteria included hallux valgus angle >20 degrees; concomitant bunion surgery; inflammatory disease; smokers; peripheral neuropathy; or history of infection of the joint. Patients who had a history of cheilectomy resulting in inadequate bone stock were excluded. Cases performed for a diagnosis other than hallux rigidus were also excluded.
Surgical Technique
The operative technique was consistent with the manufacturer’s technique except for minor adjustments, as follows. 3 A straight mid-medial approach to the first MTP joint was used. The dorsal, medial, and lateral osteophytes were removed, preserving the cortical rim of the metatarsal head. Flexion of the proximal phalanx was performed to allow for visualization of the metatarsal head. A central guide wire was placed in the metatarsal head and extended into the shaft. An 8- or 10-mm implant was selected based on the sizing guide, and the step drill was placed over the guide wire and the metatarsal head was drilled. The appropriately sized polyvinyl alcohol hydrogel implant (Cartiva Synthetic Cartilage Implant) was placed with the implant delivery tube and seated to allow for 1 to 2 mm of the implant to extend beyond the adjacent native cartilage of the metatarsal head. Layered closure of the capsule and subsequently the skin was performed. Sutures were removed at 2 weeks postoperatively. The patients were placed in a postoperative shoe and were allowed weightbearing as tolerated at 2 weeks and transitioned to a regular shoe as swelling and pain permitted.
Data Collection
Data on patient characteristics and clinical information were collected, including sex, age at the time of surgery, and history of previous surgery. Clinical outcomes were evaluated using the Foot and Ankle Outcomes Score (FAOS) and visual analog scale (VAS) score preoperatively and at the final follow-up. A 5-point Likert scale regarding patients’ satisfaction with their foot following surgery was also evaluated at the final follow-up. Failures of the procedure and complications were assessed.
A total of 15 consecutive patients (15 feet) who underwent the polyvinyl alcohol hydrogel implant were identified. Eleven patients (11 feet) who met the inclusion/exclusion criteria were included in this study; 1 patient was lost to follow-up and 3 patients had a history of a cheilectomy procedure. There were 6 males and 5 females. The mean age was 60.3 ± 9.3 years (range, 50-70 years), and the mean body mass index (BMI) was 25.4 ± 2.9 kg/m2 (range, 20.6-29.5 kg/m2). The mean follow-up time was 20.9 ± 4.6 months (range, 14-27 months). Three patients with previous cheilectomy with adequate bone stock were analyzed separately. Patient demographic data are shown in Table 1.
Patient Demographic Data and Outcomes.
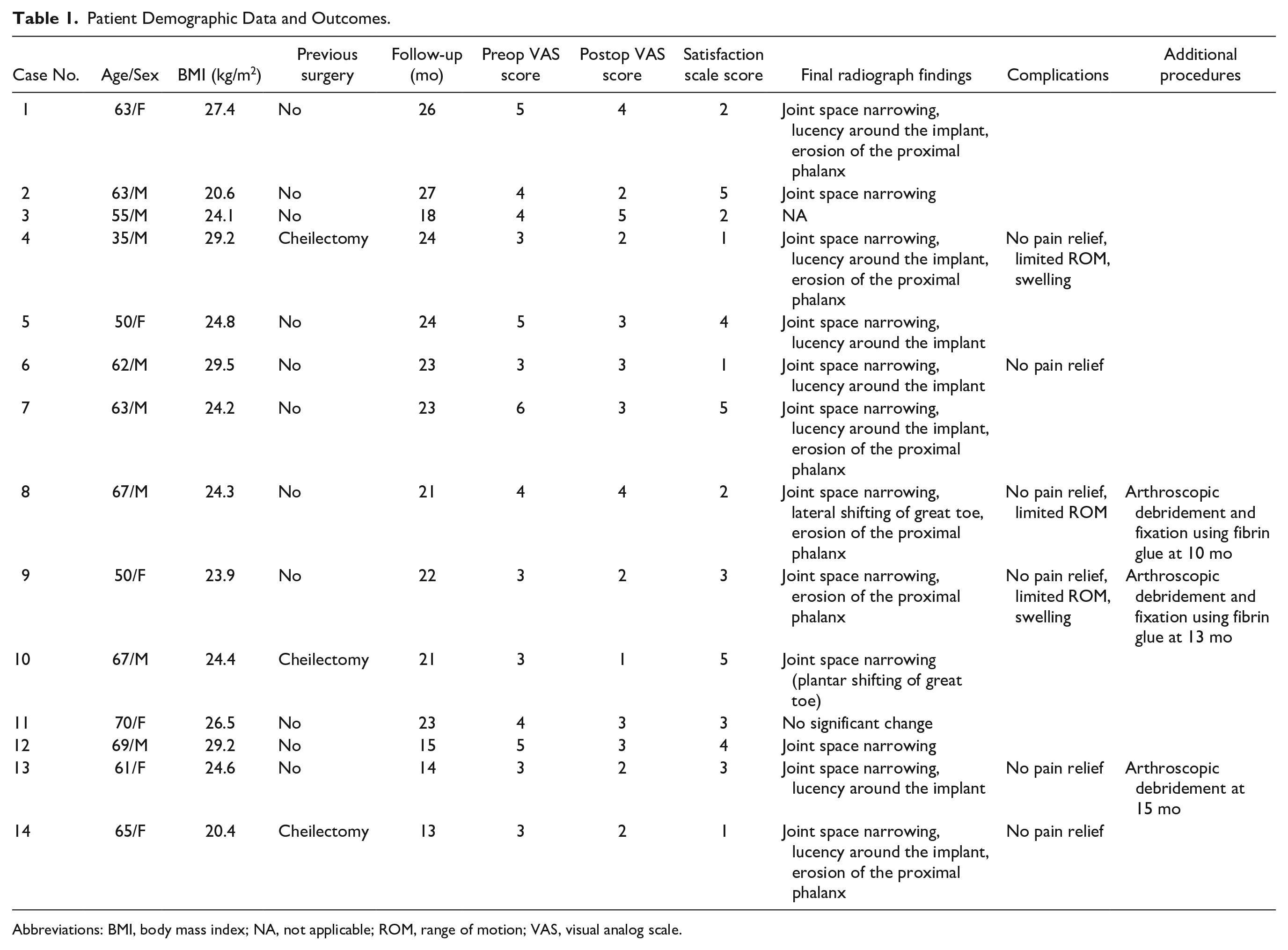
Abbreviations: BMI, body mass index; NA, not applicable; ROM, range of motion; VAS, visual analog scale.
Weightbearing anteroposterior and lateral radiographs were assessed for implant position, cyst formation, radiolucency, bony reactions, and heterotopic ossification, postoperatively at 2, 4, and 8 weeks and at the final follow-up. The progression of arthritis between the 2-week and final postoperative radiographs was also evaluated. The arthritis was characterized as having progressed if any of the following were found on subsequent radiographs: joint space narrowing, subchondral bone sclerosis on the proximal phalanx or metatarsal head side of the joint, osteophytes, or subchondral cysts.
We further selected patients who had postoperative magnetic resonance imaging (MRI) of the foot, which was indicated due to persistent pain or dysfunction of the first MTP joint. Each MRI was assessed for the dimensions of the polyvinyl alcohol hydrogel implant on axial, coronal, and sagittal T2-weighted sequences as previously described. 1 The diameter was averaged from measurements at the base, midsection, and 1 mm below the implant surface. The height was averaged from measurements at one-third and two-thirds of the implant width to avoid the rounded edges of the implant surface. The presence of peri-implant fluid and edema of the proximal phalanx and metatarsal head were also evaluated on T2-weighted sequences.
Statistical Analysis
Descriptive statistics consist of the mean and standard deviation for continuous variables and frequency and percentage for categorical variables. The Wilcoxon signed-rank test was performed to compare preoperative and postoperative outcome scores. A comparison of percentage of decrease between the implant diameter and height was performed using the Mann-Whitney U test. A value of P < .05 was considered statistically significant. All statistical analyses were performed with IBM SPSS Statistics for Windows version 22 (IBM Corp, Armonk, NY).
Results
Clinical Outcomes
The mean FAOS-reported symptoms, pain, daily activities, sports activities, and quality of life trended to improve, from 62.2, 66.7, 81.1, 60.8, and 42.9 preoperatively to 64.8. 68.7, 86.1, 62.5, and 45.5 at the final follow-up, respectively, but there were no significant differences in all subscales (P = .577, .723, .390, .857, and .813, respectively). Then mean VAS score significantly decreased from 4.1 ± 1.0 (range, 3-6) to 3.0 ± 0.9 (range, 2-5) at the final follow-up (P = .012). On a 5-point Likert scale, the mean satisfaction rating was 2.8 ±1.4 (range, 1-5). Two patients (18.2%) were very satisfied, 2 patients (18.2%) were satisfied, 3 patients (27.3%) were neutral, 3 patients (27.3%) were unsatisfied, and 1 patient (9.1%) was very unsatisfied with their outcome (Table 1).
Radiological Outcomes
Of the 10 patients who had taken adequate postoperative plain radiographs, implant subsidence was observed in 6 patients (60%) at 4 weeks after surgery and 9 patients (90%) at the final follow-up (Figure 1). Four patients (40%) had erosion of the articulating surface of the proximal phalanx of the great toe at the final follow-up. Five patients (50%) showed enlargement of a lucency around the implant at the final follow-up, suggesting osteolysis (Table 1). Two patients had computed tomography (CT) scans due to abnormal bone findings on the radiographs with persistent pain. All CT scans revealed erosion of the proximal phalanx and osteolysis around the implant (Figure 2).
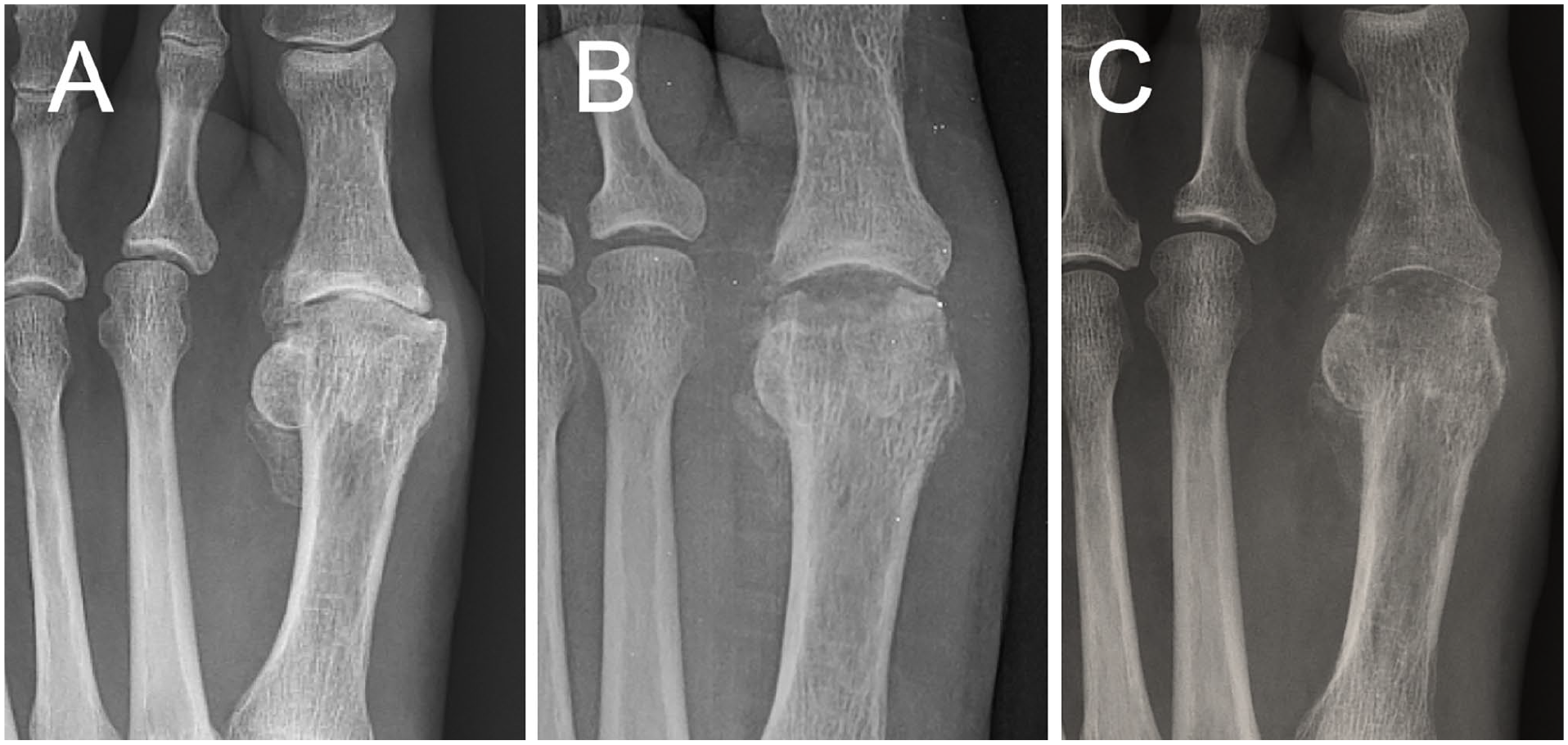
Joint space narrowing during the postoperative course, (A) preoperatively, (B) at 2 weeks, and (C) at 3 months after surgery.
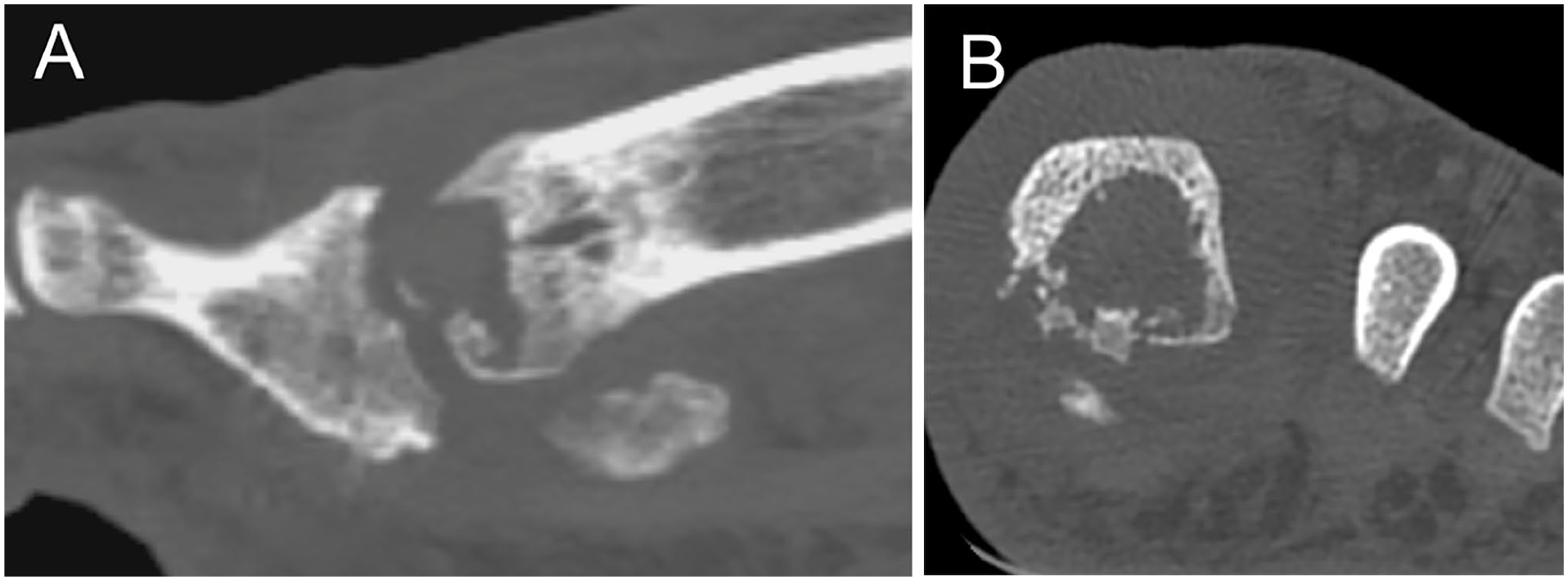
(A) Erosion of the proximal phalanx of the great toe. (B) Osteolysis of the first metatarsal head around the implant.
Of this cohort, 5 patients had MRI due to persistent symptoms postoperatively. The mean time between surgery and MRI was 10.5 ± 6.3 months (range, 5-21 months). Review of 5 MRI studies included three 10-mm implants and two 8-mm implants. In the 10-mm implants, the dimensions for the postoperative implant diameter (mm) × height (mm) were 9.9 × 9.3, 9.8 × 9.7, and 9.6 × 9.0. In the 8-mm implants, the dimensions for the postoperative implant diameter (mm) × height (mm) were 7.5 × 7.1 and 7.3 × 6.8. All implants were reduced in size. The mean percent decreases were 3.8% in diameter and 9.2% in height. The decrease in height was significantly greater than the decrease in diameter (P = .029). The irregular surface of the implant was evident in 2 patients. Qualitatively, 3 of 5 patients had evidence of peri-implant fluid, and all patients had peri-implant edema in the proximal phalanx and metatarsal. The MRI outcomes are shown in Table 2.
MRI Outcomes.
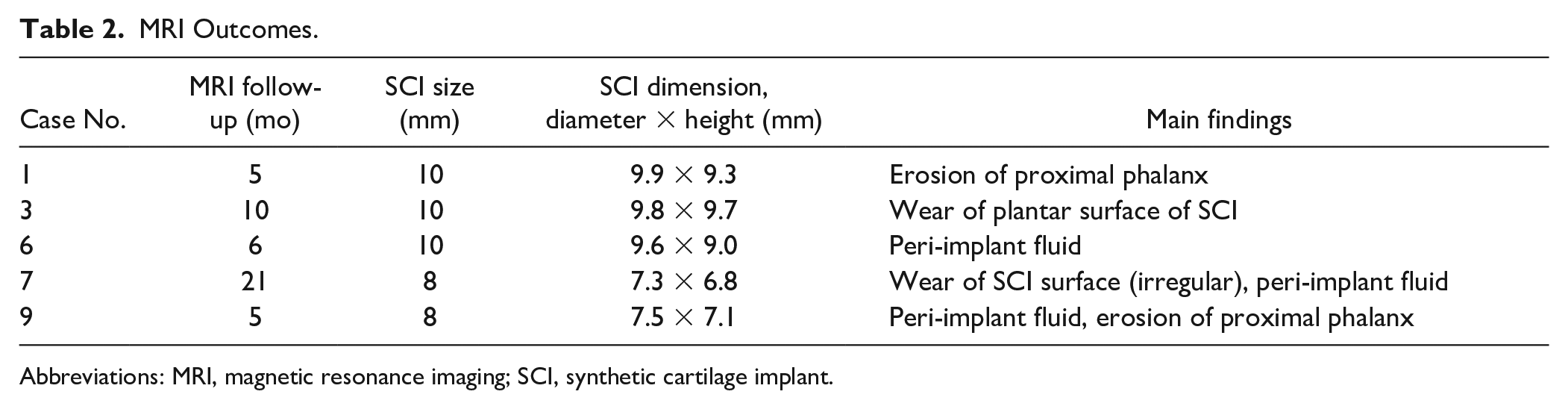
Abbreviations: MRI, magnetic resonance imaging; SCI, synthetic cartilage implant.
Complications
We considered the treatment for 4 patients (2 male and 2 females; 36.4%) as a failure due to persistent pain with no symptomatic improvement. Of those, 3 patients have undergone additional surgery, including debridement and fixation of the implant using fibrin glue for loosening. During the additional surgery, all patients had implant loosening and 2 patients had wear of the articular surface of the implant. An additional patient is currently awaiting surgery.
There were 3 patients who were excluded in this study due to a history of previous cheilectomy. Of those, only 1 patient was satisfied with the result, and 2 patients are awaiting revision surgery.
Discussion
The most important finding in this study was that there was a high failure rate of the polyvinyl alcohol hydrogel implant in this small cohort. Our study showed postoperative abnormal radiographic findings, including osteolysis around the implant, erosion of the proximal phalanx, and articular surface wear or volume loss of implant. The biggest limitation of our study was a small cohort and short-term follow-up, but we felt that the results were significantly different from those of previous original studies, and therefore it is worth highlighting these outcomes as well as the high failure rates even in this small cohort at short-term follow-up.
Originally, Baumhauer et al 3 performed a randomized controlled trial of 202 patients assessing the safety and efficacy of the polyvinyl alcohol hydrogel implant for the first MTP joint, with arthrodesis as a control. They demonstrated equivalence in the pain and functional outcome score improvement between the 2 cohorts, and the polyvinyl alcohol hydrogel implant allowed for improvement of first MTP range of motion. They also found a similar rate of revision surgery between the 2 cohorts, although this was more than 10% with both procedures. Additionally, they did not encounter implant fragmentation, wear, or bone loss.
A recently published study by Cassinelli et al 4 sought to evaluate patient experience with the synthetic cartilage implant in the United States. This single-center, single-surgeon study identified a cohort of 60 patients (52 females and 8 males) who had received a total of 64 synthetic cartilage implants. The outcomes of this study were less impressive than the original level I prospective clinical trial, with only 42% (27/64) of patients being satisfied or very satisfied. Similarly, while our study found some improvement in clinical outcomes, the treatment of 43% of patients was considered a clinical failure, with no symptom improvement, with only 36% of patients being satisfied or very satisfied. However, the potential advantages of joint preservation should be noted as patient’s highly value first MTP range of motion. In Baumhauer et al’s 3 clinical trial, they found that almost a quarter of patient’s dropped out of the arthrodesis group after randomization, highlighting this importance.
The most concerning finding from our study was the abnormal radiographic findings, including osteolysis around the implant, erosion of the proximal phalanx, and articular surface wear of the implant. Although it may be difficult to distinguish osteolysis from postsurgical osteopenia at early time points after surgery, the sufficient follow-up time of radiographs in our study can eliminate this concern. Similarly, An et al 1 performed radiographic imaging and MRI analysis of 16 patients who received a polyvinyl alcohol hydrogel MTP implant. They showed a size mismatch between the implant and the bony channel. Additionally, all patients had evidence of edema in the surrounding bone and soft tissue, with 14 patients having peri-implant fluid. They also found a 37.5% revision rate, with all patients having radiographic evidence of joint degeneration. In another retrospective radiographic case series, Shi et al 9 also reported a joint space area decrease within 1 month after polyvinyl alcohol hydrogel surgery. These radiological outcomes were similar to those of our study. All cases had evidence of bone marrow edema, and 3 of 5 cases had peri-implant fluid in our study. Peri-implant fluid may suggest loosening of the implant. The presence of peri-implant edema may be due to a short follow-up period, but the reactions of polyvinyl alcohol hydrogel implant with bone are poorly understood.
We assessed the implant dimensions using previously described methods by An et al. 1 Interestingly, our MRI analysis showed a size reduction of all implants, which was especially evident in the height. This may be due to surface wear and/or dehydration of the implant, and may be the cause of joint space narrowing on plain radiographs. We also found the erosion of the articulating countersurface of the proximal phalanx in nearly half of the patients. The implant was seated 1 to 2 mm more prominently than surrounding articular cartilage, as described in the initial study. 3 However, it may not be appropriate in some cases, leading to a tight first MTP joint. Further studies on proper implant position are warranted, as there is no consensus on this yet.
Based on our radiographic findings, we believe that revising the polyvinyl alcohol hydrogel implant to an arthrodesis would be technically challenging due to the bony reaction surrounding the implant and bone loss not only in metatarsal but also in proximal phalanx. By comparison, Baumhauer et al 3 noted that conversion to arthrodesis was not technically challenging despite the large bone defect once the implant was removed.
The biggest limitation of our study was the small cohort and short-term follow-up, but we felt that the results were significantly different from those of previous original studies, and it was worth highlighting the outcomes and high failure rates even in this small cohort and even at this short-term follow-up. The retrospective design of the study is another limitation. Additionally, the MRI studies were standard forefoot protocols and not arranged to evaluate the implant specifically; however, we used previously described methods for the implant dimension measurements. 1 We excluded 3 patients with a history of previous cheilectomy from this study, although those patients had a small amount of bone resected from their previous surgery—less than 20% of the metatarsal head and less than 10% of the base of the proximal phalanx. However, the treatment of 2 patients with prior cheilectomy was considered a failure, but in contrast, 1 patient was very satisfied with the result, warranting further investigations as to proper indication of the implant for hallux rigidus. Our current results have prompted us to reexamine our use of the polyvinyl alcohol hydrogel implant, and for now, we have stopped its use for hallux rigidus. Based on growing evidence in the recent literature, meticulous care should be taken in patient selection for using the cartilage implant in the treatment of hallux rigidus. Additional studies are necessary to determine which patients can safely receive this procedure.
Conclusion
Our current small cohort study revealed a high failure rate with the polyvinyl alcohol hydrogel implant in patients with hallux rigidus. Significant radiologic subsidence with lysis around the implant, erosion of the proximal phalanx surface, and implant wear are harbingers for concern in the long term.
Supplemental Material
FAI962482_disclosures – Supplemental material for Early Failures of Polyvinyl Alcohol Hydrogel Implant for the Treatment of Hallux Rigidus
Supplemental material, FAI962482_disclosures for Early Failures of Polyvinyl Alcohol Hydrogel Implant for the Treatment of Hallux Rigidus by Yoshiharu Shimozono, Eoghan T. Hurley and John G. Kennedy in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.