
Abstract
Background:
A lack of access to care is predictably associated with negative outcomes in foot and ankle surgery. Despite recent advances in telecommunication technologies, the field of orthopedics has been slow to adopt these resources in offsetting barriers to care. The COVID-19 pandemic has forced departments to change their clinical approach, lending unprecedented opportunity to better understand how telehealth may bridge this care gap in foot and ankle practices. The purpose of this study was to assess patient-reported outcomes of telemedicine encounters, including comfort and patient satisfaction. Our hypothesis was that patients would be significantly less satisfied with telemedicine when compared with in-office appointments for all nonemergency visit types.
Methods:
Telemedicine satisfaction was assessed via phone survey with a modified 1 to 5 Likert scale. Patients who had completed a telemedicine visit between April 13, 2020, and June 19, 2020, were eligible to participate. Patient demographics were recorded, and data were analyzed using paired and independent t tests for parametric continuous data and Fisher’s exact and chi-square tests for noncontinuous data. A total of 216 patients completed the telemedicine questionnaire.
Results:
The overall mean satisfaction for telemedicine visits (4.7) was significantly lower than that for in-office visits (4.9) (P < .001). However, the majority (90.3%) of patients reported they would use telemedicine again in the future. When compared, patients seeking fracture care had significantly higher telemedicine satisfaction (4.9, n = 38) than those receiving nonfracture care (4.6, n = 178) (P = .001), and those greater than 50 miles from the clinic had higher satisfaction (5.0, n = 14) than patients living within 50 miles of the clinic (4.7, n = 202) (P < .001).
Conclusion:
Patients were more satisfied with their in-office clinic visit than telemedicine, although the vast majority of patients endorsed a willingness to utilize telemedicine in the future. Patients with trauma and greater barriers to foot and ankle care were more satisfied with their telemedicine visits.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
The field of orthopedics has been on the forefront of medical technological advances. However, in the case of virtual healthcare delivery, we, along with the rest of the medical community, have been slow to adopt its use. The COVID-19 pandemic has forced changes in medicine to better allocate resources. A significant change seen by orthopedic surgeons was the rapid adoption of telemedicine to be able to continue to efficiently deliver musculoskeletal care while limiting patient-provider interactions. However, with this rapid utilization, much is still unknown regarding the safety and efficacy of this healthcare delivery method.
Given the relative ubiquity of smartphone, tablet, and/or laptop ownership in the United States, nearly all patients are candidates for telemedicine services (2016 Census, https://www.census.gov/content/dam/Census/library/publications/2018/acs/ACS-39.pdf). However, the potential of such services has long been underutilized.2,4,18 Current orthopedic literature on telemedicine is limited; most studies have involved adult reconstruction or shoulder and elbow clinical visits.14,21,27 However, these studies have primarily been limited to postoperative follow-ups without variety or stratification of visit type. Regarding foot and ankle–specific practices, the literature on the use of telemedicine is even more sparse. A single study from Brogan et al 5 found that telemedicine was a safe and cost-effective means of follow-up treatment for fifth metatarsal fractures treated in the emergency department. Furthermore, some studies have broadly studied the implementation of telemedicine in orthopedics and have included patients with foot and ankle–related pathologies. Still, none solely focused on foot and ankle care.7,15,23 These studies demonstrated significantly reduced wait times and optimization of travel times and expenditures.7,15,23 To our knowledge, no study has assessed the feasibility of widespread telemedicine implementation across any single orthopedic subspecialty.
The extraordinary circumstances of the 2020 coronavirus pandemic have resulted in an unprecedented spike in the use of telemedicine to engage in safety precautions to minimize in-person contact. 1 This allows for a wealth of opportunity to explore its role in orthopedic outcomes, patient satisfaction, and clinical workflow. Though novel, recent global studies on the rapid rollout of expansive telemedicine have shown it to be safe, cost-effective, and satisfying on both the patient and provider ends.3,11,20 More consistent use of telemedicine demonstrates the potential to improve foot and ankle care through decluttered clinical volumes and the opportunity to provide care for patients burdened by distance or socioeconomic barriers. This study aimed to explore outcomes related to telemedicine encounters, such as patient satisfaction, comfort, and time burden. We hypothesized that patients would be significantly less satisfied with telemedicine relative to in-office appointments for all nonemergency visit types.
Methods
Study Design
This was an Institutional Review Board–approved retrospective analysis of the Emory University orthopedic foot and ankle department telemedicine visits from April 13, 2020, to June 19, 2020, secondary to the COVID-19 pandemic. All patients were seen by a single surgeon (J.T.B.) in the foot and ankle department during the stated time period. Following their telemedicine visit, patients were contacted by one of the study authors via telephone and asked to complete a telemedicine questionnaire. During the study period, the surgeon’s clinic was not open for patients to choose between a telemedicine and in-office visit. Only patients needing to be seen for emergency trauma or complication were allowed to visit the office per institution COVID-19 guidelines.
Inclusion and Exclusion Criteria
Inclusion criteria for this study were all patients over 18 years of age who experienced a telemedicine visit from April 13, 2020, to June 19, 2020, via tablet, computer, and/or smartphone. All 338 eligible patients were contacted and, 216 (63.9%) completed the questionnaire. Included patients may or may not have undergone prior operative intervention. Patients who were seen solely in the office for a medically necessary visit during the pandemic were excluded. Additionally, we excluded patients who declined the survey or were unable to be successfully contacted after 2 phone call attempts. Lastly, nonnative English speakers were excluded due to limited access to interpreter services.
Demographics
Over 5 weeks, 216 patients completed a telemedicine visit within the foot and ankle department and responded to the telemedicine questionnaire. The average patient age of our cohort was 50.6 years (range, 19-84 years), including 57 male (26.4%) and 159 female (73.6%) patients. The remaining patient demographic data can be found in Table 1. The most common chief complaints of patients seen via telemedicine were associated with disease of the ankle and hindfoot (55.1%), followed by forefoot (33.3%). Counts of broad disease processes can be found in Table 2.
Patient Demographics.
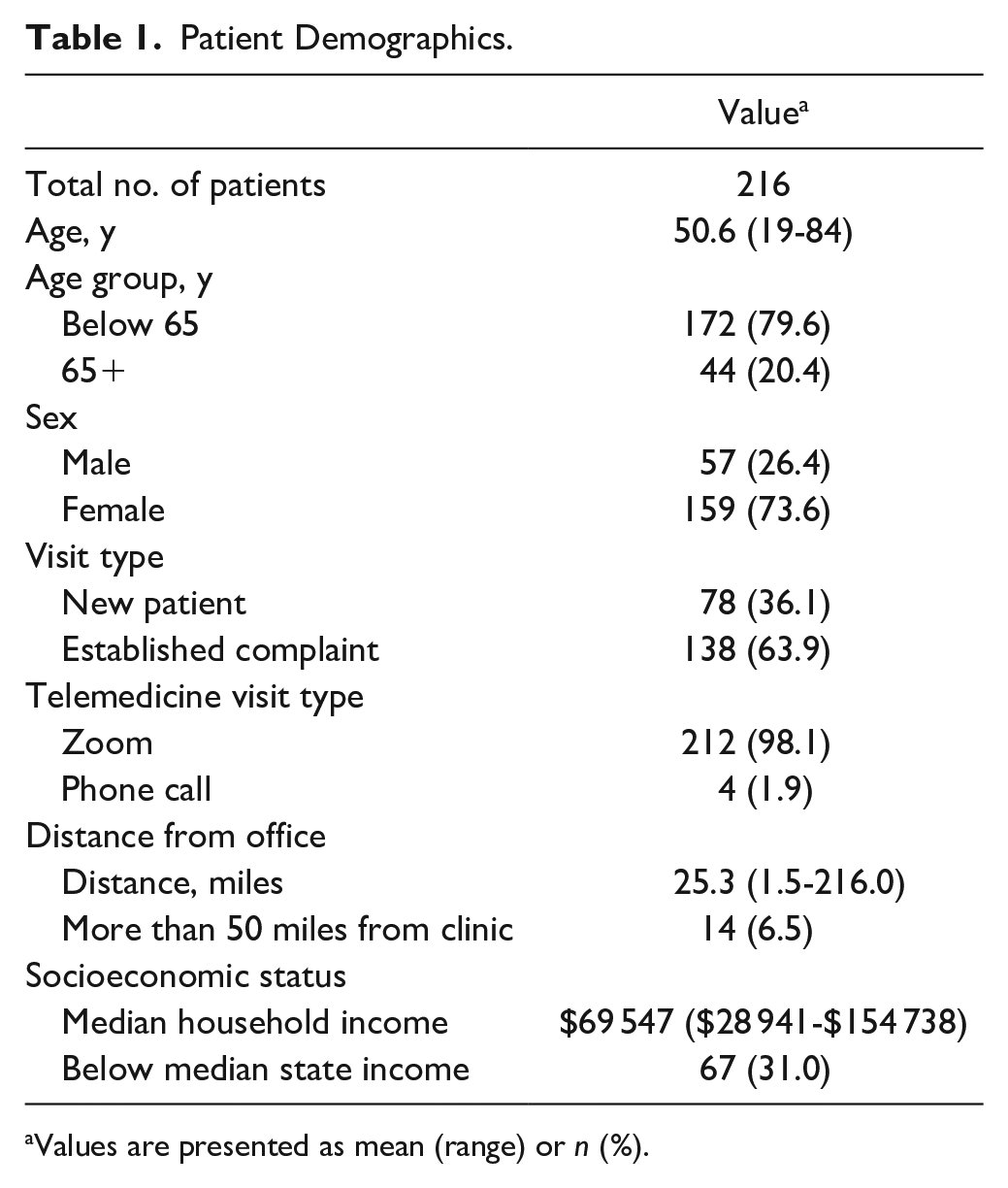
Values are presented as mean (range) or n (%).
Characterization of the Specific Anatomy and Disease Processes for Patients. a
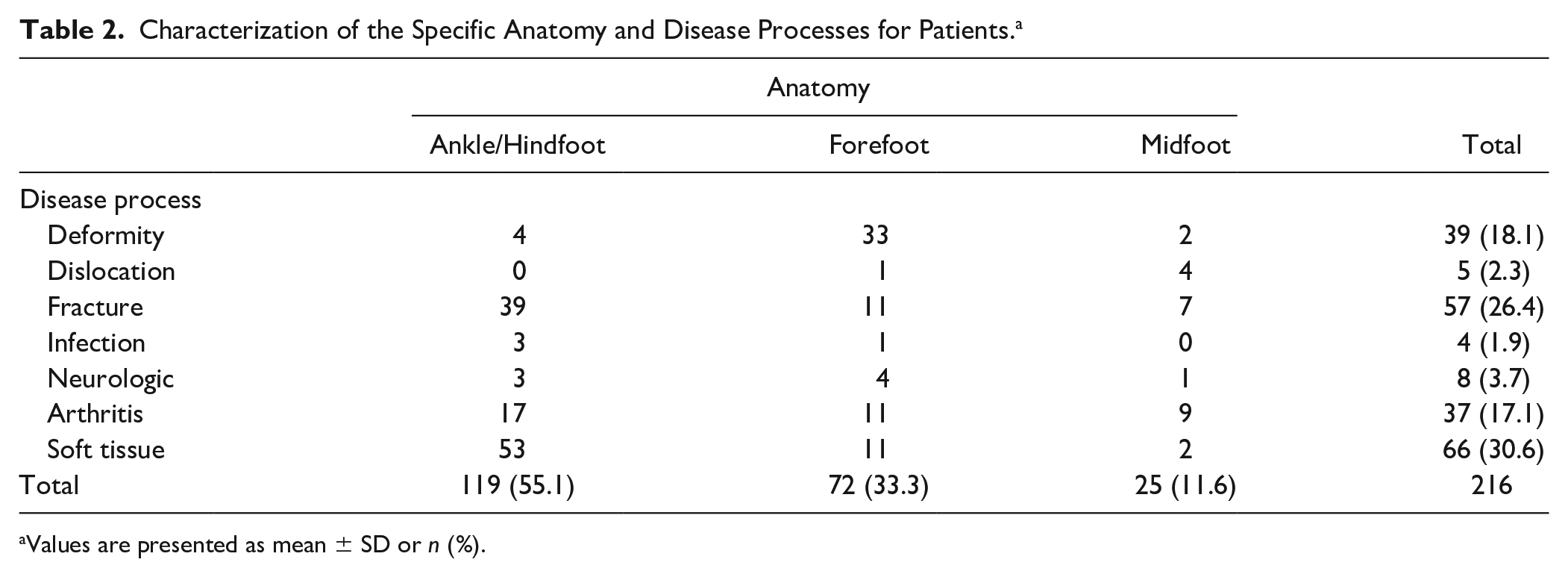
Values are presented as mean ± SD or n (%).
Telemedicine Questionnaire
The telemedicine questionnaire was the product of a quality improvement initiative to quantify patient satisfaction with the telemedicine visit. Satisfaction was gauged with a Likert scale from 1 to 5, with 1 being extremely dissatisfied and 5 being extremely satisfied (Appendix). 14 The questionnaire was administered by a member of the research team. Patients were contacted via phone call from our institution’s clinic office using their last provided telephone number in the electronic medical record. Those who did not answer after 2 call attempts were excluded from the study.
Patients were denoted as either “new” or “established” based on whether they had an in-office clinic visit within the past year. The “established” label includes patients seen for regular postoperative follow-up, those who had previously seen the physician but then presented with a new complaint, and those presenting for nonoperative follow-up. Those denoted as “established” were asked to rate their satisfaction with both their most recent in-office clinic visit and their telemedicine visit with the same, single surgeon. Anatomy and disease processes were determined from review of the chief complaint and billing code within the telemedicine visit note. All in-office clinic visits were conducted at a single site, and distance to the clinic was determined based on the patient’s previously reported address. Median household income was estimated based on the patient-provided zip code and publicly available U.S. Census American Community Survey income data. Socioeconomic stratification was based on the median household income for the state of Georgia ($55 679 per U.S. Census).
Statistics
Statistical analyses were conducted with the following assumptions: β = 0.8 and α < .05. A paired sample t test was used to compare normally distributed continuous data for in-office versus telemedicine visits; additional comparisons of telemedicine data utilized independent sample t tests for normally distributed continuous data. Fisher’s exact and chi-square analyses were used for categorical data. Descriptive statistics were used to relay patient demographic information. A post hoc power analysis was performed on the first 100 patients enrolled in the study for in-office versus telemedicine satisfaction, indicating a need for 212 subjects to achieve adequate power.
All analyses were conducted with SPSS software version 26.0 (IBM Corp, Armonk, NY).
Results
Of all patients surveyed, 39.4% reported they would have preferred to have their visit conducted via telemedicine if done again, regardless of COVID-19. The majority of patients (90.3%) also reported they would use telemedicine again if offered in the future. Further characterization of all-telemedicine patient visit perception can be found in Table 3.
Grouped Visit Data.
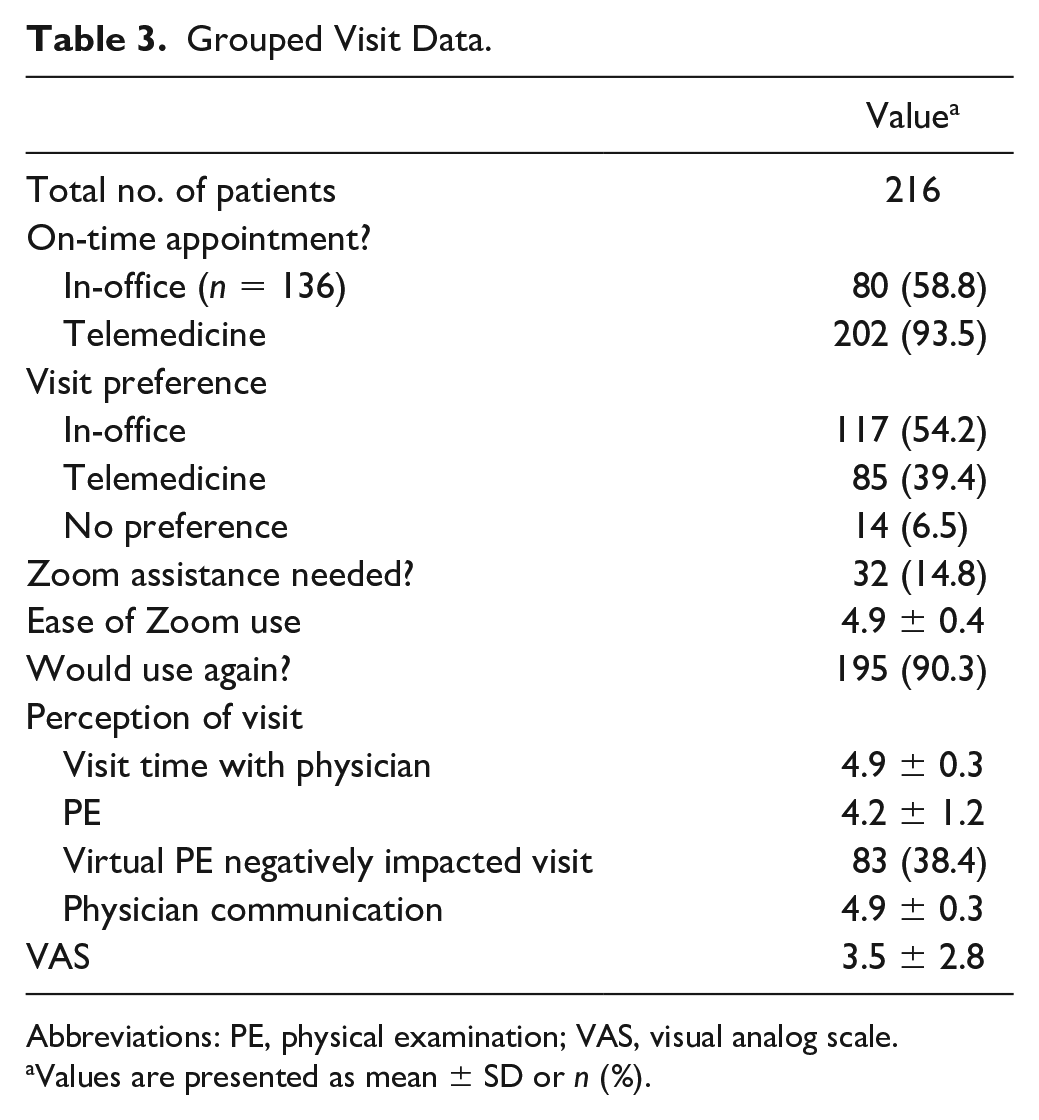
Abbreviations: PE, physical examination; VAS, visual analog scale.
Values are presented as mean ± SD or n (%).
The overall mean satisfaction of telemedicine visits was 4.7 versus 4.9 for in-office visits (P < .0001) (Table 3 and Figure 1). Patients establishing care with the provider for the first time via telemedicine had a mean visit satisfaction of 4.84, while previously established patients had a mean visit satisfaction of 4.7 (P < .0001) (Figure 2). Telemedicine satisfaction was significantly greater in patients traveling more than 50 miles to the clinic (P < .0001) and those patients seeking care for a fracture (P = .001) (Figures 3 and 4). No significant differences in overall telemedicine satisfaction were found in patients grouped by age above or below 65 years, and those from a region with a median household income more or less than $55 679 (Figures 5 and 6).
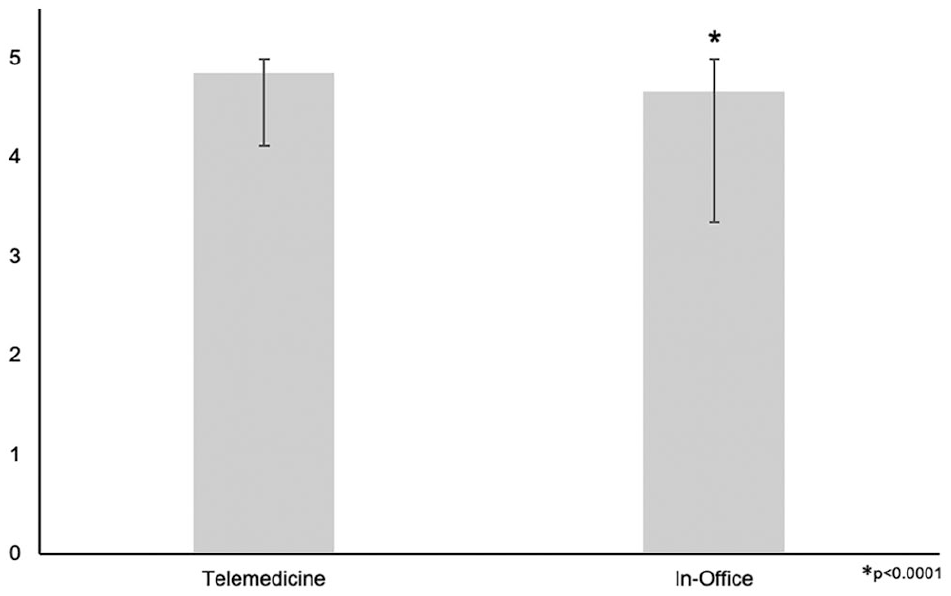
In office versus telemedicine visit satisfaction. The mean satisfaction for in-office visits (4.9 ± 0.4) was significantly greater than that for telemedicine visits (4.7 ± 0.7).
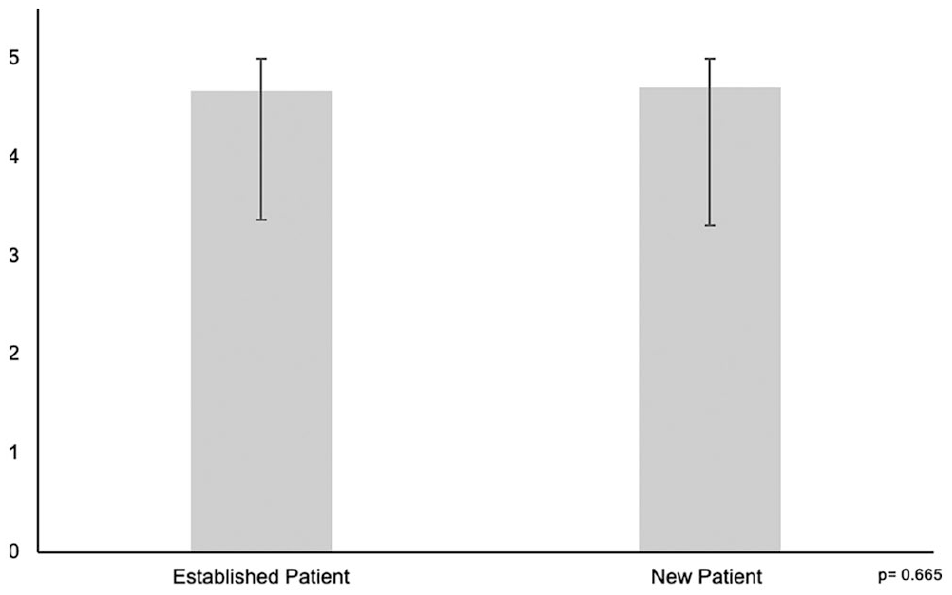
Telemedicine satisfaction and newly established patients. No significant difference in satisfaction was observed between new patient (4.7 ± 0.7) and previously established patient visits (4.7 ± 0.7).
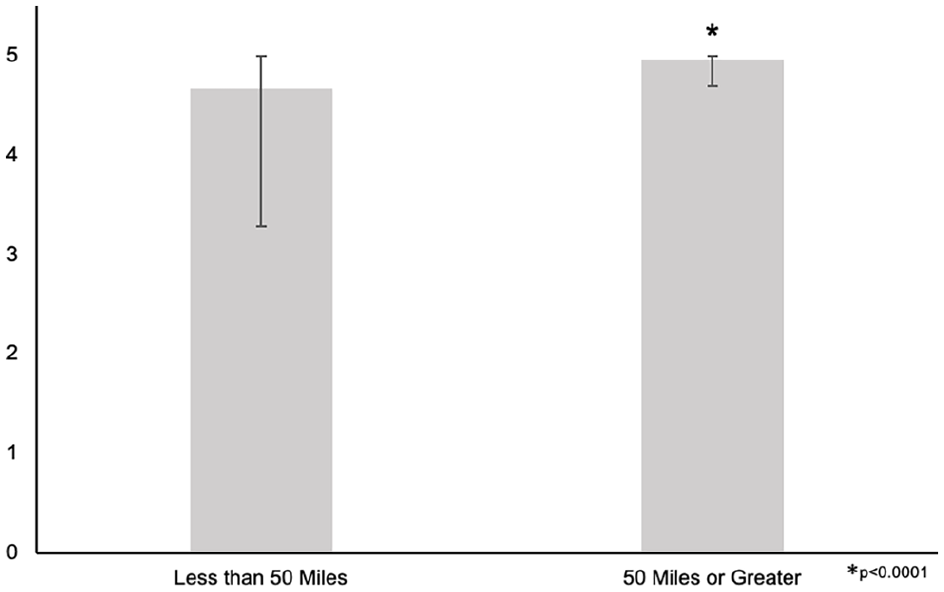
Telemedicine satisfaction and distance. The mean satisfaction for patients normally traveling greater than 50 miles to the clinic (5.0 ± 0.1 miles) was significantly greater than those traveling less than 50 miles (4.7 ± 0.7 miles). The mean distance for those greater than 50 miles from the clinic was 106.7 ± 50.4 miles, and for those closer than 50 miles it was 19.6 ± 12.4 miles (P < .0001).
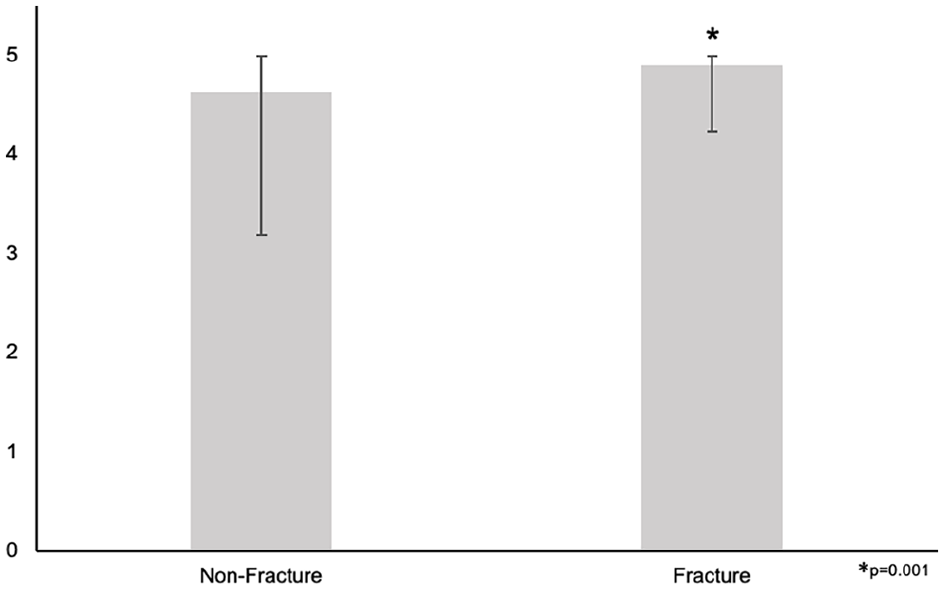
Telemedicine satisfaction and fractures. The mean satisfaction for telemedicine patients with a fracture (4.9 ± 0.3) was significantly higher than that for all other ankle pathologies (4.6 ± 0.7).
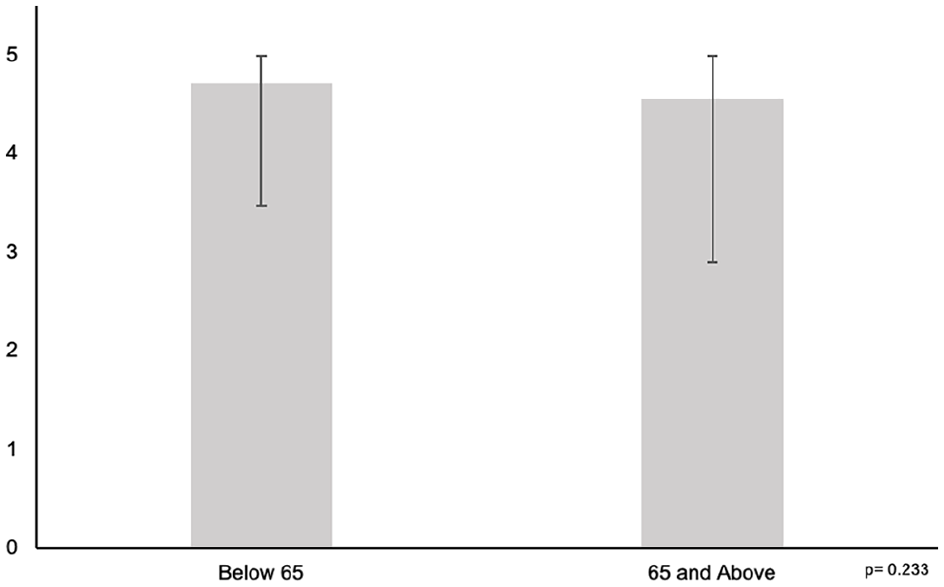
Telemedicine and age. No significant difference in satisfaction was observed between patients aged 65 years and older (4.6 ± 0.8 years) and those younger than 65 years (4.7 ± 0.7 years).
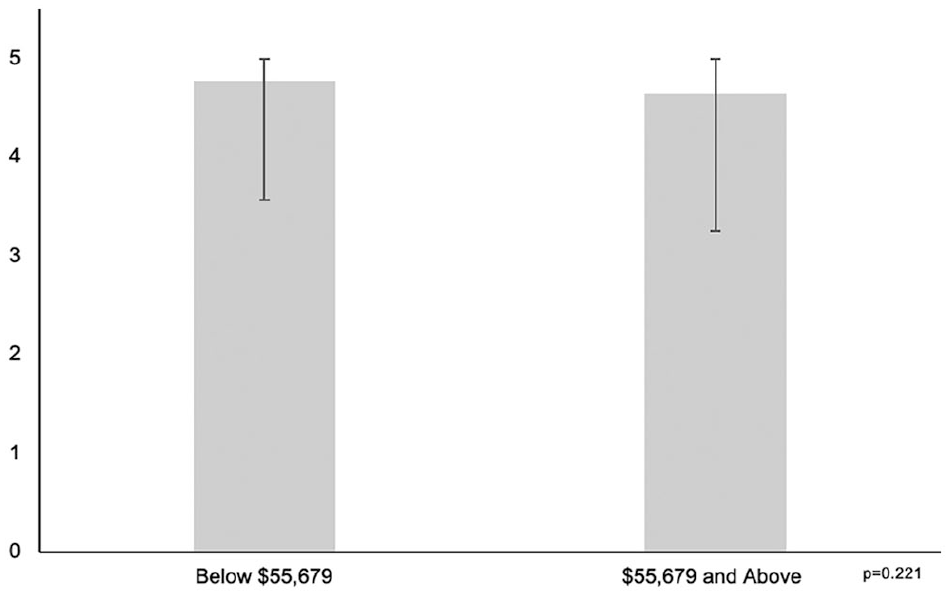
Telemedicine satisfaction and income. No significant difference in satisfaction was observed between patients with a median household income of $55 679 or more ($4.7 ± $0.7) and those with a median income less than $55 679 ($4.8 ± $0.6). The mean median household income for those below the Georgia median was $46 930 ± $6408, and it was $79 566 ± $1286 for those above the state median (P < .0001).
Subgroup analysis of telemedicine visit perception when stratified by age showed that a significantly lower percentage of patients 65 years and older would use telemedicine in the future (79.5% vs 93.0%). Patient satisfaction with the virtual physical examination was also significantly lower for those in the 65 years and older as compared with the younger cohort (P = .007). No other differences in visit perception were observed between age groups; those data are shown in Table 4.
Subanalysis of Age on Visit Perception. a
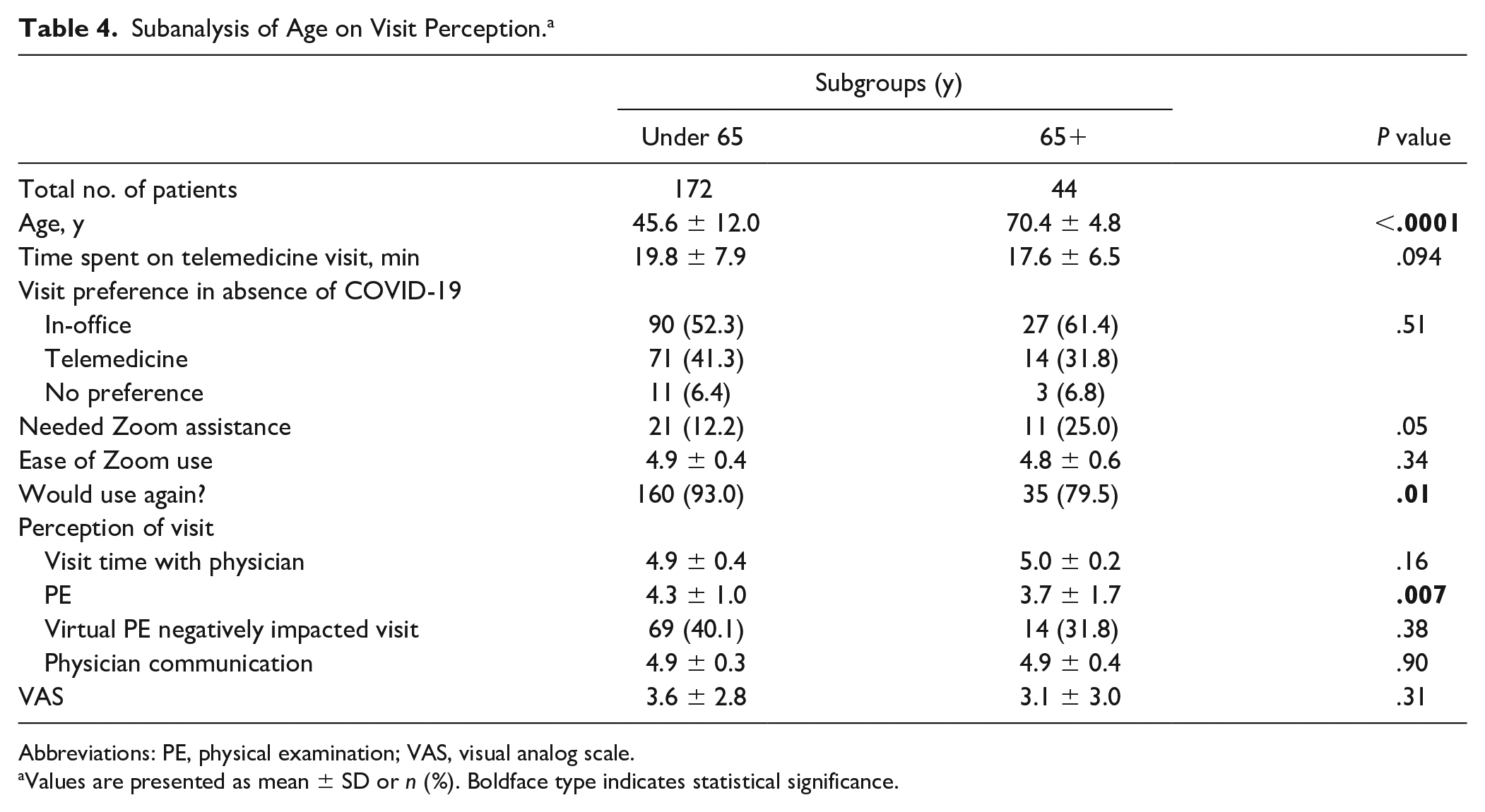
Abbreviations: PE, physical examination; VAS, visual analog scale.
Values are presented as mean ± SD or n (%). Boldface type indicates statistical significance.
Discussion
During the current COVID-19 pandemic, Loeb et al 17 and others20,29 have shown that telemedicine platforms are invaluable for providing consistent orthopedic care while maintaining social distance. Widely used across other medical specialties for nonemergency cases, telemedicine models have made their way into orthopedics as a means to decrease both patient and physician burden.14,27 While traditionally reserved for routine, specific operative follow-up, a large percentage of academic orthopedic institutions have transitioned to department-wide telemedicine models to increase coverage and maintain clinic volume during this pandemic.16,26 However, it remains unclear whether metrics of visit quality are maintained in orthopedic telemedicine outside of the current scope of literature. This study sought to assess the short-term transition to telemedicine in a foot and ankle–specific practice and quantify the patient experience during the rapid implementation of a telemedicine platform. The primary finding was that patients were slightly less satisfied with telemedicine visits for foot and ankle consultations than they were with conventional in-office visits but would be willing to utilize the platform again. This study had 2 secondary findings: 1) patients who were seeking care for a fracture and those living beyond 50 miles of the clinic office both reported increased satisfaction with their telemedicine visits, and 2) patients 65 years and older had no overall difference in telemedicine satisfaction compared with younger patients.
Though we found a slight decrease in overall satisfaction with telemedicine visits relative to in-office visits, a nonsignificant trend toward increased satisfaction was seen between patients establishing care for the first time via telemedicine and those who had established care before COVID restrictions. Patients rated their experience with different aspects of the telemedicine visit highly across patient types and agreed they would use a telemedicine service in the future if offered. The virtual physical examination was the lowest-rated aspect of the visit for all patients. Still, most patients agreed that the lack of an in-office physical did not detract from the overall quality of their visit (Table 3). None of the patients triaged to a telemedicine visit experienced an adverse clinical event, but given the acute nature of the COVID crisis and recent implementation of our telemedicine program, additional study is needed to assess the long-term safety and efficacy of this initiative.
To our knowledge, this is the first study showing successful implementation of a new telemedicine model across a foot and ankle orthopedic division. This is essential when there is such a paucity of studies regarding telemedicine efforts across all orthopedic departments. 21 Like others, we have seen that telemedicine is associated with positive outcomes in the routine postoperative care following orthopedic surgeries.6,14,19,21,24,27 In contrast to both Kane et al 14 and Sharareh et al, 27 who found no difference in patient satisfaction in those utilizing telemedicine, our study revealed a significant decrease in satisfaction between telemedicine and in-office visits. However, we believe it unlikely that this is a clinically significant difference, as evidenced by the vast majority of patients endorsing they would use telemedicine again in the future. This small difference may be attributed to several factors: mandated use of telemedicine for all nonemergency patients, unfamiliarity with virtual medicine on the part of patients and physicians, and the inclusion of postoperative patients with nonroutine recovery courses desiring face-to-face visits. Our study increases the generalizability of previously drawn conclusions by analyzing additional visit types and disease processes. Patients who were seen for evaluation or treatment of a fracture were significantly more satisfied with their telemedicine visits than all other disease processes (Figure 4). This difference is likely due to a multitude of factors, including decreased time to initial office visits following an injury at a time of limited access to care. Fractures of the foot and ankle are particularly debilitating in terms of patient mobility, many times requiring a patient to arrange for travel to be seen in clinic. Our results would appear to support notions from Sathiyakumar et al 25 that telemedicine may be more useful for patients with limited mobility secondary to closed fractures.
The results of our study also indicate that telemedicine may be a viable tool for offsetting disparities that exist in the management of foot and ankle pathology. It is well reported across medical specialties that distance from the clinic office and income are correlated with follow-up retention rates.12,22,28,33 In patients with distal radius fractures, Tejwani et al 30 reported a significant increase in the proportion of patients lost to follow-up with median incomes less than $50 000, and those whose highest education level was a high school diploma. Additionally, Whiting et al 32 reported significantly greater rates of noncompliance and loss to follow-up in patients with surgical trauma living greater than 100 miles from the office, and a slight, though nonsignificant, increase in risk for those living 50 to 99 miles from the clinic. Using the data from both Whiting and Tejwani, we stratified patients a priori on the basis of distance more or less than 50 miles from the clinic, and those with a median household income above or below the Georgia state median ($55 697). An analysis of patients living greater than 100 miles from the clinic was not conducted as only 2 patients fell into this category. We observed significantly increased telemedicine satisfaction for those living 50 miles or more from the clinic office, and a trend toward increased satisfaction for those with a median household income below the Georgia state median income.
Lastly, we are unaware of any orthopedic study that has addressed variations in patient satisfaction with telemedicine in relation to their age. It is well documented that younger patients prefer telemedicine visits in other specialties.9,13 Additionally, prior literature has shown that even when randomized, subjects consenting to participate in telemedicine programs were typically younger or admitted to being more comfortable with technology.9,13 Despite data showing a more favorable relationship with younger patients and telemedicine, our findings during this pandemic have been contrary to this trend. We have seen similar satisfaction and ease of use across ages, with the elderly requiring more assistance. While a significantly higher proportion of elderly patients stated they would not utilize telemedicine again in the future relative to younger patients, nearly 80% reported that they would use the telemedicine platform again. Given the current need for social distancing, these results are novel in that elderly patients seen during this time had no other means of obtaining an appointment with their surgeon. Sharareh et al 27 had previously noted the issue of selection bias in elderly populations agreeing to telemedicine utilization as those who were most comfortable with technology. While our study does suggest an increased, though nonsignificant, level of discomfort with telemedicine in older populations, we hope that our study’s lack of difference in patient satisfaction in subgroup analysis stratified by age counters the assumption that telemedicine is best suited for younger patients.
As we adapt and improve in response to this crisis, it is essential to look forward to how telemedicine platforms can improve foot and ankle practices in the future. Multiple studies have shown telemedicine to be a safe alternative to in-office follow-up across medical specialties. A recent Cochrane review of level I telemedicine studies conducted before 2013 found that telemedicine had produced an equal quality of care in treating heart failure patients and better performance in controlling blood sugar in patients with diabetes. 8 Telemedicine has recently been shown to be a safe and cost-effective alternative for treatment of fifth metatarsal fractures following standardized implementation in the emergency department. 5 Vuolio et al 31 revealed no difference in conservative and operative management of knee osteoarthritis at 1 year following the use of telemedicine visits relative to in-office visits. Additionally, in the routine postoperative follow-up of total hip and knee arthroplasty, Sharareh et al 27 demonstrated no differences in clinical outcome with the use of telemedicine. Coupled with our findings of high patient satisfaction for all nonurgent complaints and the well-documented time-saving benefits, the void that telemedicine may be able to fill has become clearer.10,14,27 Already, changes in the way we implement orthopedic telehealth are taking place to optimize these services for the future, including the standardization of basic video physical examination techniques. 29
We recognize the variety of limitations present in this study. Given that all of our patient-reported responses were collected retrospectively via phone call, recall bias is inherently present. Additionally, as our in-office control data were derived from patient-reported experiences within the last year, we recognize that a secondary element of recall bias is present. We experienced a 36% patient loss, with 216 of 338 eligible patients completing the study. While the vast majority of these patients were excluded because they could not be reached by phone, a small minority declined to compete the study and may have been more dissatisfied with their visits than those who completed the survey. Those patients without access to a computer or other technology capable of supporting a video telemedicine platform were unable to participate; however, in our experience, this was a minority of patients. We acknowledge that the patients included in this study were seen by a single physician and their staff, limiting the generalizability of our results and conclusions, but it does show that successful implementation is possible. We also acknowledge the relatively small sample size of our study cohort and the challenge this presents in drawing definitive conclusions from our subgroup analyses. While the COVID-19 pandemic has offered an opportunity to study telehealth platforms, the ability to access care that would otherwise be inaccessible may falsely elevate patient-reported telemedicine satisfaction. Our data showed a nonsignificant difference in satisfaction between age groups, but it is reasonable to think that some patients with nonurgent orthopedic concerns would wait to be seen in person if they were less familiar or uncomfortable with telehealth technologies.
Conclusion
Our study gives strong, preliminary data that a foot and ankle orthopedic practice can rapidly and successfully implement a telemedicine program with minimal loss of patient satisfaction. New and previously established patients agreed that they received high-quality telehealthcare with their desired provider when such visits would be otherwise impossible due to the COVID-19 pandemic. Debulking both the patient and physician time burden will be essential when social distance restrictions are lifted, and telemedicine may provide a viable forum to offset some of this load. However, further study on larger patient populations is needed to illuminate the specific manner in which telemedicine can best complement foot and ankle–specific practices and offset barriers to foot and ankle care, and to assess the safety of such interventions.
Supplemental Material
FAI963059_disclosures – Supplemental material for Feasibility of Rapid Development and Deployment of a Telemedicine Program in a Foot and Ankle Orthopedic Practice
Supplemental material, FAI963059_disclosures for Feasibility of Rapid Development and Deployment of a Telemedicine Program in a Foot and Ankle Orthopedic Practice by Wesley J. Manz, Rahul Goel, Omolola P. Fakunle, Sameh A. Labib and Jason T. Bariteau in Foot & Ankle International
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.