
Abstract
Background:
This study was aimed at assessing clinical and radiographic outcomes of the Minimally Invasive Intramedullary Nail Device (MIIND) to correct moderate to severe hallux valgus (HV) and the long-term persistence of its effects.
Methods:
This case series study involved 100 patients, 84 women and 16 men (mean age, 59 years), who underwent the MIIND procedure with a mean follow-up of 97 months. Assessment was performed preoperatively, postoperatively, at 6 and 12 months, and at last follow-up. Clinical outcomes were evaluated with American Orthopaedic Foot & Ankle Society (AOFAS) scores, visual analog scale (VAS), and patient satisfaction. Intermetatarsal angle (IMA), metatarsophalangeal hallux valgus angle (HVA), distal metatarsal articular angle (DMAA), and tibial sesamoid position were assessed. Statistical analysis was performed.
Results:
The mean AOFAS score improved from 57.9 to 90.5 points, VAS scale was 1.5 ± 2.0, and patients’ satisfaction was 8.7 ± 1.4. The mean correction of the HVA and IMA showed a significant correction; however, the effect of time was not statistically significant on DMAA. Sex (P = .047), severity (P = .050), associated procedures (P = .000), and preoperative angle (P = .000) showed significant association with HVA correction and its persistence over time. Age was not statistically significant. Complications were 9 cases of superficial wound infection and 6 recurrences.
Conclusions:
The MIIND technique proved a viable procedure to correct moderate to severe HV with a low rate of complications and recurrence, producing significant correction of most radiographic parameters assessed and their persistence, even at long term.
Level of Evidence:
Level IV, case series study.
Keywords
Hallux valgus (HV) surgery is one of the most frequently performed orthopedic interventions of the forefoot. 53 Nevertheless, its ideal operative treatment, in relation to the severity of deformity, is still debated among foot and ankle surgeons.51,66 Operative correction is the standard treatment of symptomatic HV, as it is more effective compared to nonoperative methods. 22 For this reason, many different open, minimally invasive (MI) and percutaneous operative procedures have been proposed,6,40,49 but their choice seems to depend in most cases on the surgeon’s experience and preferences or patients’ demands rather than a proper radiographic preoperative assessment and consequent protocol of care.23,50,62
To standardize the treatment according to HV severity, distal first metatarsal (I-MTT) osteotomies are generally indicated for mild or moderate deformities.23,40,64 However, because it is mostly the site of the osteotomy that determines the potential of angular correction, this remains limited in cases of distal procedures. 28 Hence, to correct moderate to severe HV, proximal I-MTT osteotomies are preferred for their higher corrective potential.54,70,72 Nevertheless, an associated Akin osteotomy is often suggested for these procedures. 67
Recently, MI procedures have become popular for their decreased recovery times, smaller scars, and a greater range of early postoperative motion.6,32,44,47,49,61 Among these, a Minimally Invasive Intramedullary Nail Device (MIIND), produced under the name of Endolog (by Medical Due), has been proposed for mild to severe HV correction, and it has shown encouraging results at medium-term follow-up.4,5,21 Our initial experience with this device showed the most evident functional improvements for moderate to severe HV, 5 while for mild HV, purely percutaneous procedures are preferred at our institution. 6
The MIIND consists of a curvilinear cylindrical titanium body with a diameter of 4.5 mm and a blade inclined by 4 degrees with respect to the axis of the nail. It is available in 3 sizes (44, 45, and 46) with 3 different degrees of curvature (40, 42, and 32 degrees, respectively) and 3 different lengths (26 mm, 31 mm, and 33 mm). Using a 3.66-mm titanium angular stable screw, available in 2 different lengths (15 mm and 20 mm), it is fixed to the first metatarsal head (I-MTTH), stabilizing the osteotomy site (Figure 1). This device produces progressive lateral displacement of the I-MTTH, up to 100% with respect to the metatarsal neck (MTTN), and its contemporary derotation, allowing multiplanar correction of the HV and the anatomic reduction of the sesamoids without performing lateral release (LR). Furthermore, it does not require routine removal.
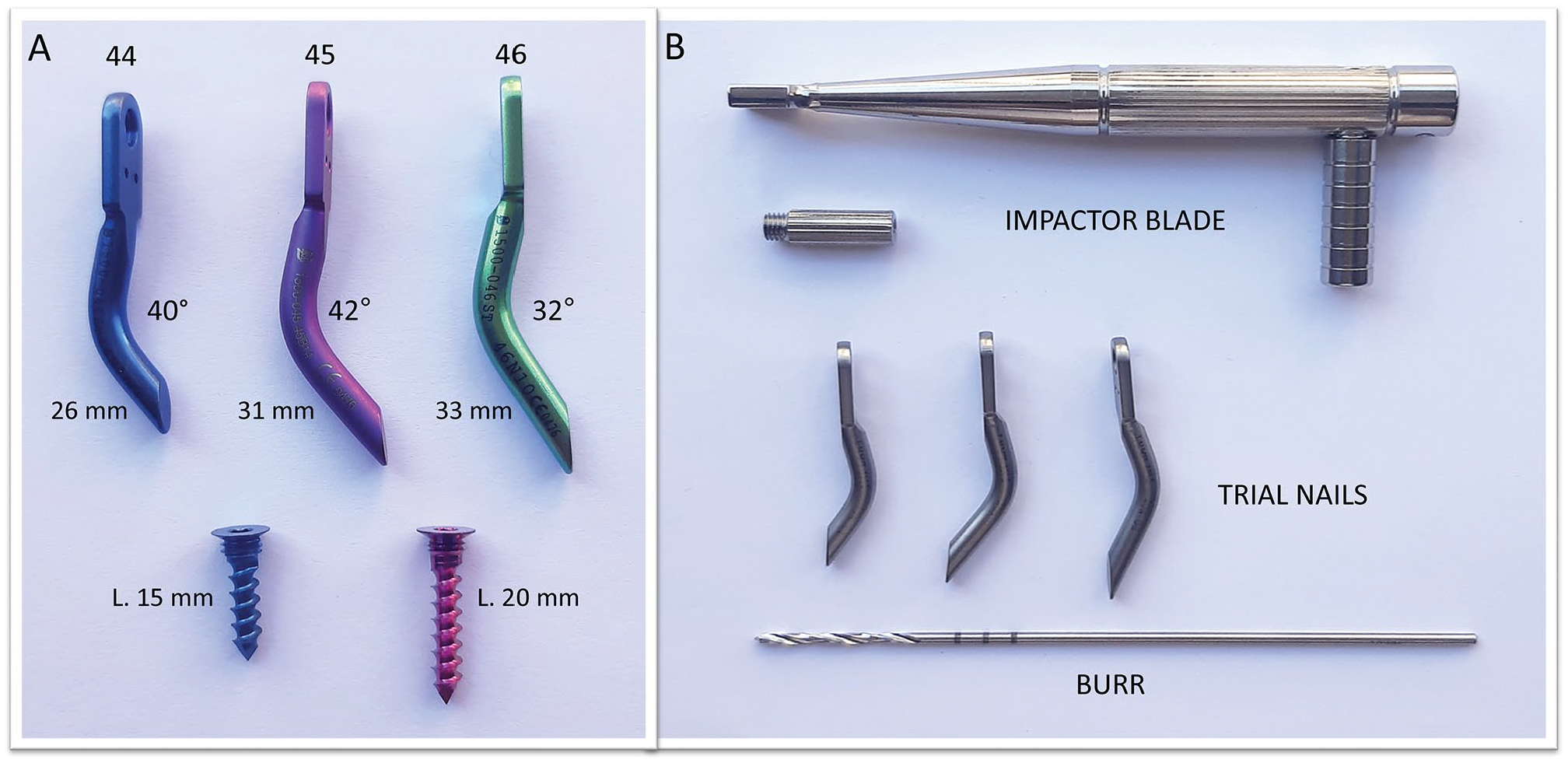
(A) Image of the 3 different sizes of the Minimally Invasive Intramedullary Nail Device (44, 45, and 46), each with different degrees of curvature (40, 42, and 32 degrees, respectively) and lengths (26 mm, 31 mm, and 33 mm); two 3.66-mm titanium angular stable screws (15 mm and 20 mm) are available for its fixation. (B) The complete kit of the device, including impactor blade for its application, trial nails for test during surgery, and burr to make the screw hole.
Despite the extensive literature on the operative treatment of this deformity, very few studies, mostly retrospective, have been conducted on a longer term follow-up on the different osteotomies proposed for bunion surgery and none regarding the MIIND.23,62 A recent review on HV recommended that research should be directed toward assessing outcomes at long-term follow-up postoperatively. 39 Hence, the aim of this case series study was to assess clinical and radiographic results of the MIIND technique for the correction of moderate to severe HV in a subsequent, wide series of patients, at different follow-up points, with a final one at long term. Our study hypothesis was that this mini-incision procedure with direct view of the I-MTT can achieve and maintain satisfactory functional and radiographic outcomes over time with an acceptable complication rate after moderate to severe HV treatment.
Methods
Patients
In this single-center, case series study, clinical and radiological data were prospectively collected and retrospectively analyzed. Local ethics committee approval was obtained.
All patients with a diagnosis of moderate to severe HV, having failed conservative management and fulfilling the following inclusion criteria, were enrolled consecutively from September 2009 to September 2012 before evaluating their outcomes. Inclusion criteria were age between 20 and 80 years (according to the indications of our institutional forefoot operative protocol), moderate to severe HV with persistent pain in the area of the I-MTTH, and having particular discomfort while wearing shoes. According to the presence of one of these Mann and Coughlin parameters,
18
moderate HV was defined as an intermetatarsal angle (IMA)
We used these strict selection criteria to avoid possible confounding factors, having hypothesized for some of them a probable impact on the generalizability of our results. Specifically, we excluded some conditions, such as generalized joint laxity or hypermobility, 8 which, while having a specific correlation with HV, are usually treated in a different way.29,38
At our institution during the 3-year enrolled period, a consecutive series of 100 patients (45 right and 55 left feet), including 84 women and 16 men (male/female = 1:5.3) with a mean age of 59.0 ± 12.1 years (range, 20-80 years), underwent the MIIND technique for moderate (grade 2: 69) and severe (grade 3: 31) symptomatic HV.
Operative Technique
In this case series, the preoperative protocol, postoperative management, and the 1-day hospital stay detailed operative procedure for MIIND implantation were executed only by the senior author, as previously described. 5 Anesthesia consisted of conscious sedation in association with a regional ankle block. The patient was in a supine position and a tourniquet was applied at the level of the ankle. The operative procedure started with a 3-cm dorsal-medial longitudinal incision centered on the I-MTT. Then, the capsular incision was performed along the line of the skin incision. A very minimal, oblique bunionectomy removed the prominent medial eminence. This allowed the support of the impactor’s blade upon which the device was assembled (Figure 2A). Perfect coplanarity and maximum adherence of the pallet support to the flat surface previously created on the I-MTTH were essential for a correct position of the MIIND (Figure 2B). The oblique bunionectomy was carried out with a thickness no more than 2 to 4 mm from the distal part of the medial eminence, close to the articular surface, to zero at the level of the MTTN, allowing lateral translation and at the same time derotation of the I-MTTH, which were pushed and maintained by the nail after its application. For this purpose, two 1.6-mm Kirschner wires, acting as joysticks, were inserted to allow the derotation of the metatarsal head during its lateral translation. A linear osteotomy was then performed at the proximal level of the MTTN. The trial nail device was assembled on the impactor and then gently introduced into the medullary cavity with progressive lateral displacement of the MTTH and its concomitant derotation, correcting the distal metatarsal articular angle (DMAA) and sesamoid subluxation. Before the right size of MIIND was applied, the correction obtained was checked clinically and under fluoroscopy (Figure 2C). The MTTH was fixed to the implant with a screw long enough to provide angular stability (Figure 2D). It was necessary to regulate the medial angle of the MTTN using the micro-saw to prevent conflict of the bone with the soft tissues and skin before closing the capsule and suturing the wound.
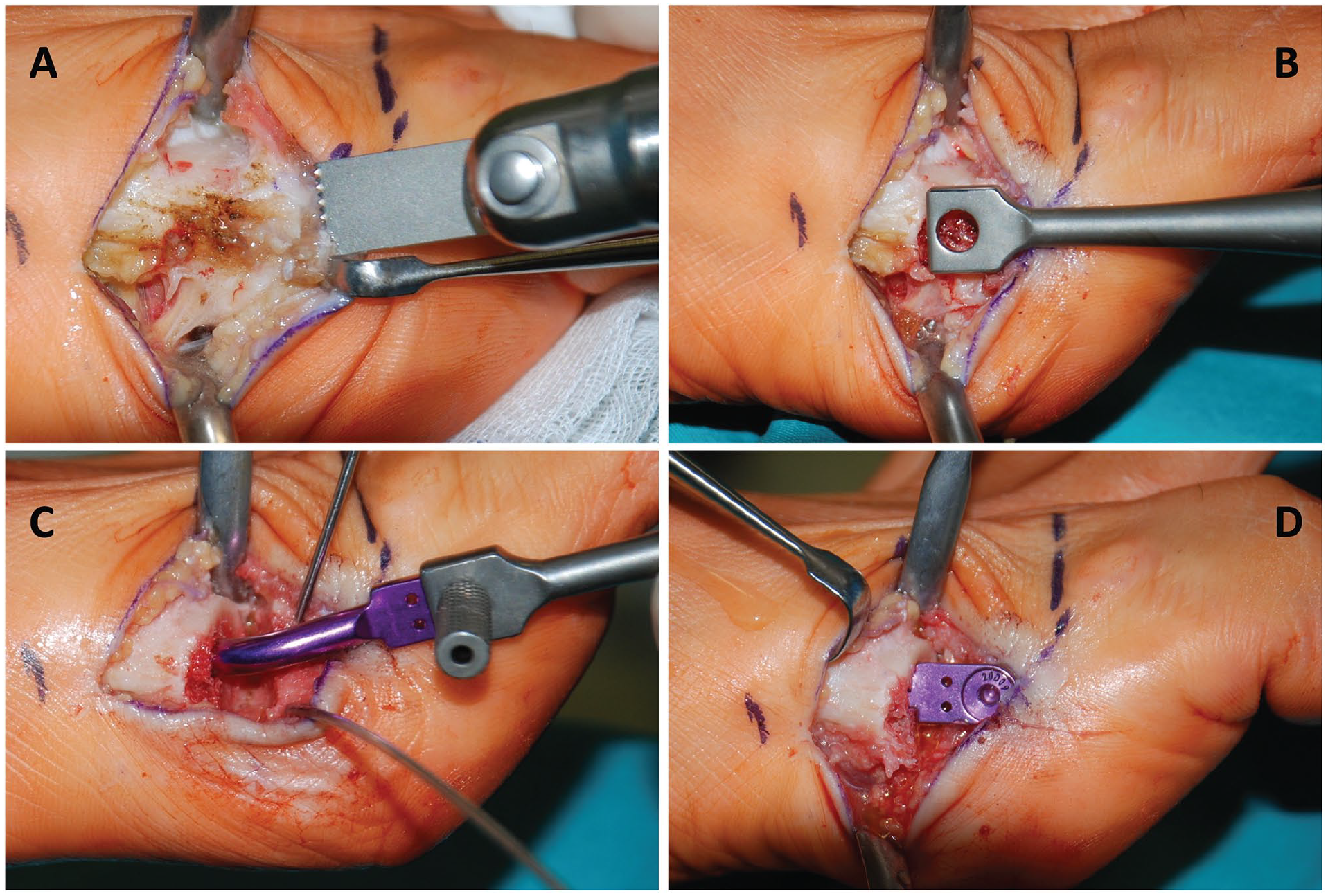
(A) Intraoperative images showing the main steps of the Minimally Invasive Intramedullary Nail Device (MIIND) technique: bunionectomy is performed to remove the medial eminence by a standard oscillating micro-saw in a distal to proximal direction. (B) A flat surface on the first metatarsal head (I-MTTH) is made to support the impactor’s blade and ensure maximum adherence with the blade pallet support. (C) The MIIND-45 is applied definitively to maintain the correction by progressively lateral displacement and concomitant derotation of the I-MTTH. Previously, a linear osteotomy was performed at the proximal level of the neck and the trial nail was introduced into the medullary cavity to verify adequate alignment of the first ray. (D) Finally, the I-MTTH is fixed to the MIIND implant with a 20-mm screw, providing angular stability.
Although preoperative planning was useful for choosing which size of the implant could guarantee adequate translation of the head according to the severity of the HV (ie, MIIND-45, presenting the greatest curvature, allows the greatest translation) and width of the I-MTT bone medullary cavity (Figure 3A), it was not possible to standardize the exact lateral translation of the I-MTTH. Hence, trial nails in the different sizes were used intraoperatively.
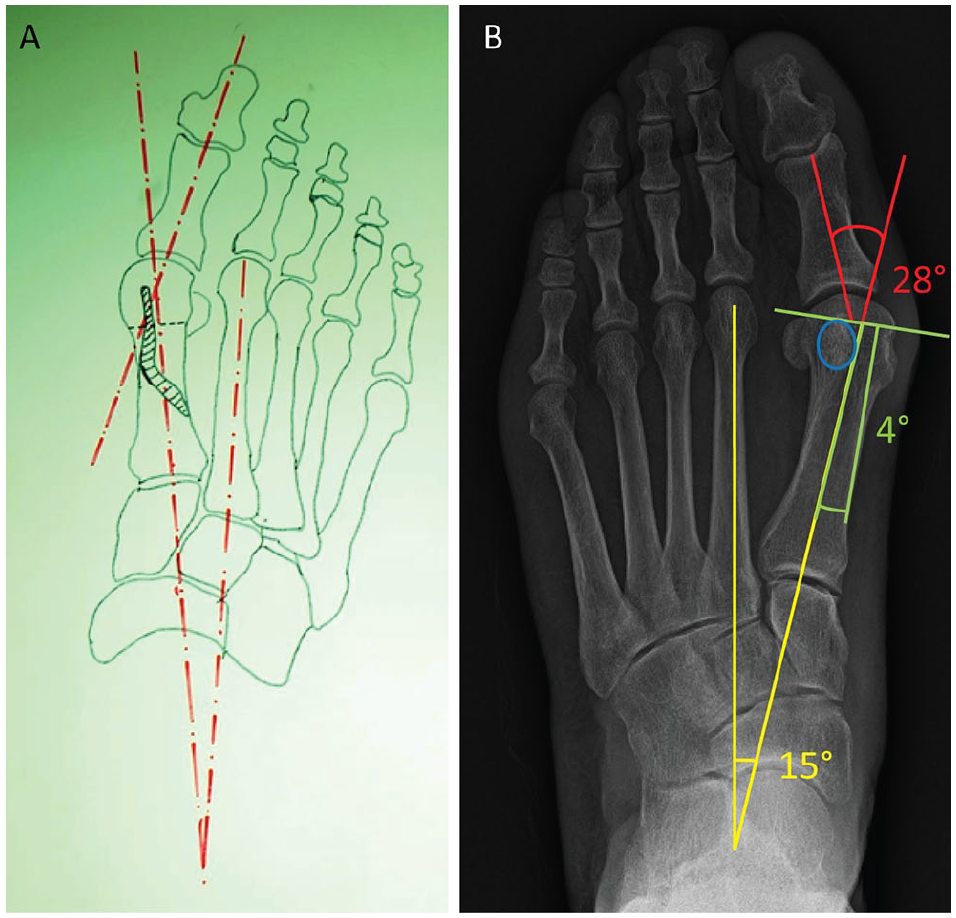
(A) Image of preoperative planning before surgery to choose the right size of the implant, to ensure adequate translation of the head according to the hallux valgus severity and width of the first metatarsal bone medullary cavity. (B) Example of electronically computer-assisted measurements (MedStation program) from weightbearing anteroposterior radiographs of the following angles and tibial sesamoid position (TSP) to define the deformity according to Mann and Coughlin parameters 15 : intermetatarsal angle (15 degrees), hallux valgus angle (28 degrees), distal metatarsal articular angle (4 degrees), and TSP (circle).
According to the preoperative degree of valgus (grade 3) or in cases of concomitant hallux valgus interphalangeus (HVI) greater than 10 degrees or an HVA persisting more than 10 degrees after MIIND application, a percutaneous Akin osteotomy was performed. For the other common pathologies of the forefoot, the following adjunctive operative procedures were carried out: distal metatarsal metaphyseal osteotomy (DMMO) for metatarsalgia,5,30 and/or percutaneous osteotomy of the proximal phalanx for fixed deformities of the lesser toe, and/or percutaneous tenotomy of the flexor and extensor tendons in cases of flexible or fixed lesser toe deformities. 7
As the MIIND technique provides a linear extra-articular osteotomy to the proximal level of the neck, the release of the soft tissues on the lateral side of the first metatarsophalangeal joint (I-MTPJ) was not performed, nor was lateral capsulotomy of the joint carried out for repositioning of the sesamoids.
Postoperative Protocol
Anteroposterior and lateral x-rays of feet were taken before the patients were discharged and at 1-month follow-up (the first were not included for the radiographic evaluation because they were nonweightbearing). The patients were allowed to walk as much as they could tolerate the same evening after surgery at discharge using a rigid flat-soled orthopedic shoe for the following 30-day period, according to the indications of our institutional forefoot postoperative protocol also used for other MI techniques. 6
A prophylactic antibiotic was administered only before surgery, and thromboembolic prophylaxis with nadroparin calcium was prescribed the same evening for a 10-day period. We recommended an antiedemigen therapy (Leucoselect, Lymphaselect, and Bromelain [Laborest]: 1 tablet/d) for 30 days, starting from the day of the surgery, and an analgesic therapy for 2 weeks with Etoricoxib (90 mg, 1 cp/d) in the morning, also to prevent heterotopic ossification. All patients were seen once every 2 weeks for a month in our outpatient clinic, where functional taping was replaced at the first appointment.
Clinical and Radiological Outcome Measures
The clinical and radiological analyses were carried out by 2 independent investigators, senior orthopedic residents and junior authors, who were not directly involved in the patients’ operative treatment. The resident who performed clinical assessment was blinded to the type of procedure used. After a period of training in HV measurement techniques by the senior author, the resident who performed radiographic evaluation used a digital workstation and software (MedStation program) to minimize bias during the measurements. 16
Clinical evaluations were performed pre- and postoperatively at 6 months, 12 months, and last follow-up. The hallux-metatarsophalangeal scale by the American Orthopaedic Foot & Ankle Society (AOFAS) was used. A VAS for rating pain was evaluated at last follow-up. The patients were asked whether they were satisfied with the overall result of the procedure or not, using the VAS for patient satisfaction, ranging from 0 to 10 points (with 0 indicating no satisfaction and 10 denoting complete satisfaction for the performed procedure).
All patients underwent radiographic assessment before surgery and postoperatively at 1 month, as well as at 6 months, 12 months, and the final follow-up. Radiological outcomes were evaluated using the MedStation program, which allows the retrieval of electronically computer-assisted measurements from weightbearing radiographs of the following angles (Figure 3B): IMA (normal value
The relationship between the IMA values, HVA values, and tibial sesamoid displacement was used to classify the deformities into 2 groups, moderate HV or severe HV, as explained above. Any complications were recorded, including HV recurrence (defined as HVA
Statistical Analysis
Statistical analysis was performed by an independent statistician from another university, blinded to the type of treatment. Before any data processing, statistical figures were visually inspected for capturing potential outliers (ie, those values more than 1.5 times the interquartile range below the first or above the third quartile). Normality of data distribution was verified performing the D’Agostino-Pearson omnibus test. Continuous parameters were expressed as mean ± standard deviation, together with median and range, whereas categorical variables were computed as percentages where appropriate. A generalized linear model for repeated measures (before operative intervention, after operative intervention at 1 month, 6 months, 12 months, and last follow-up) was used. The homogeneity of covariance matrices and the independence assumptions were checked. The sphericity assumption was verified carrying out Mauchly’s W test. In case of sphericity violation (when the F test was significant) and with epsilon values (ε, quantitatively measuring the extent of departure from sphericity) less than 0.75, the Greenhouse-Geisser correction was adopted to properly adjust for the degrees of freedom of the interaction effect between different time points and the sample group. Otherwise (in case of ε greater than 0.75), the Huynh-Feldt correction was carried out. Effect size was estimated by computing the partial eta squared (
Results
Patient Characteristics
Descriptive characteristics of the studied population, associated procedures performed, and preoperative and postoperative radiographic parameters of the enrolled patients are reported in Table 1. As described, other operative corrections were performed in 42% of the cases. The mean long-term follow-up was 97 (range, 84-120) months, and none of the patients were lost during the different follow-ups, including the final one (Figure 4).
Descriptive Statistics of the Studied Population.
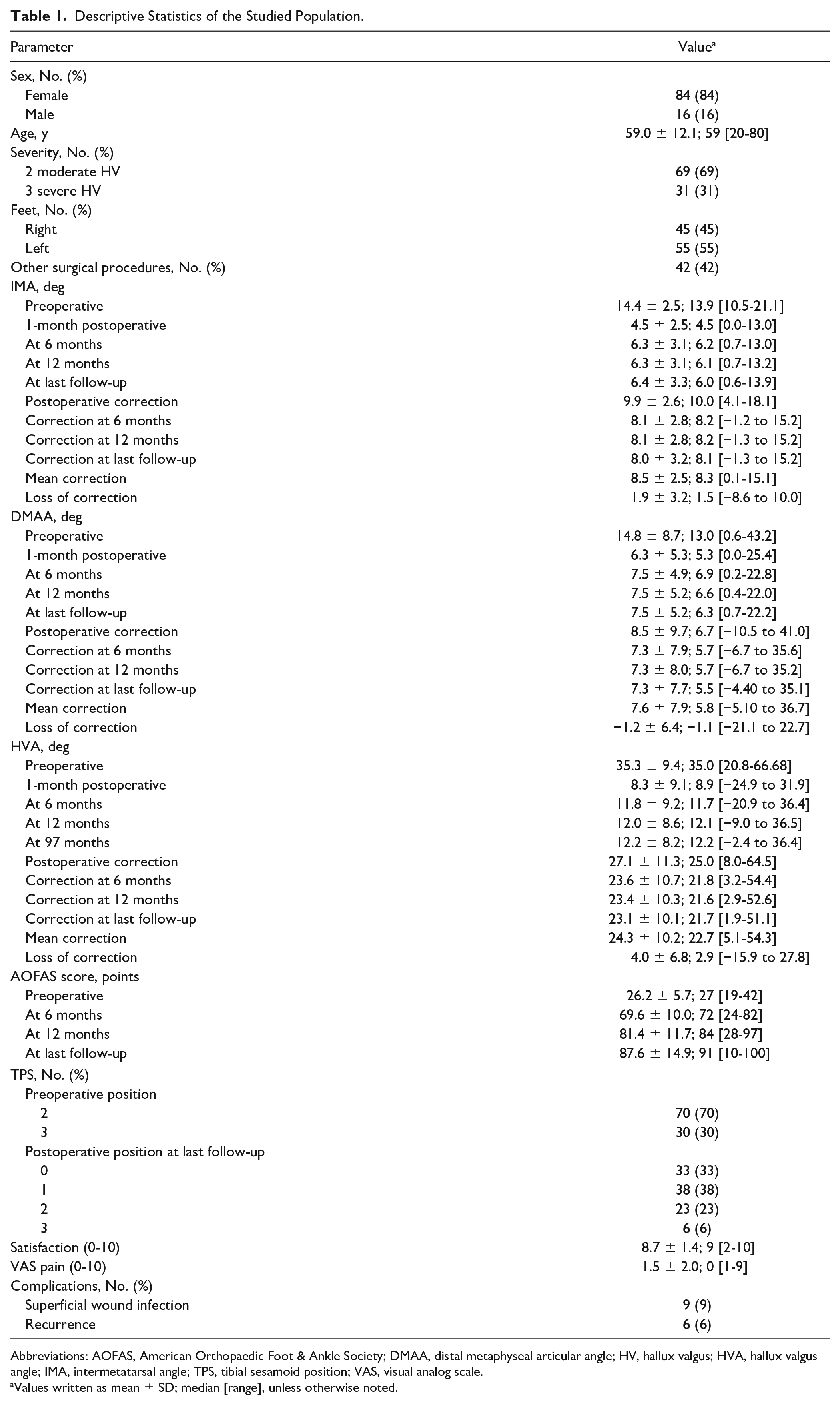
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; DMAA, distal metaphyseal articular angle; HV, hallux valgus; HVA, hallux valgus angle; IMA, intermetatarsal angle; TPS, tibial sesamoid position; VAS, visual analog scale.
Values written as mean ± SD; median [range], unless otherwise noted.

Case 1: A 68-year-old woman having undergone the Minimally Invasive Intramedullary Nail Device technique in addition to Akin percutaneous osteotomies for severe hallux valgus correction of her left foot. Weightbearing radiographic images of (1) anteroposterior and (2) sesamoids axial views at (A) preoperative period, (B) 1-month follow-up, (C) 6-month follow-up, (D) 12-month follow-up, and (E) last follow-up of 101 months after surgery, showing bone callus consolidation and its remodeling, maintaining the correction of the different radiographic parameters analyzed. FU, follow-up.
Clinical Outcomes
The AOFAS score improved significantly after operative intervention, remaining higher over time (F = 38.82,
Impact of the Variables Under Study on the IMA, DMAA, HVA, AOFAS Score, and Their Persistence Over Time.
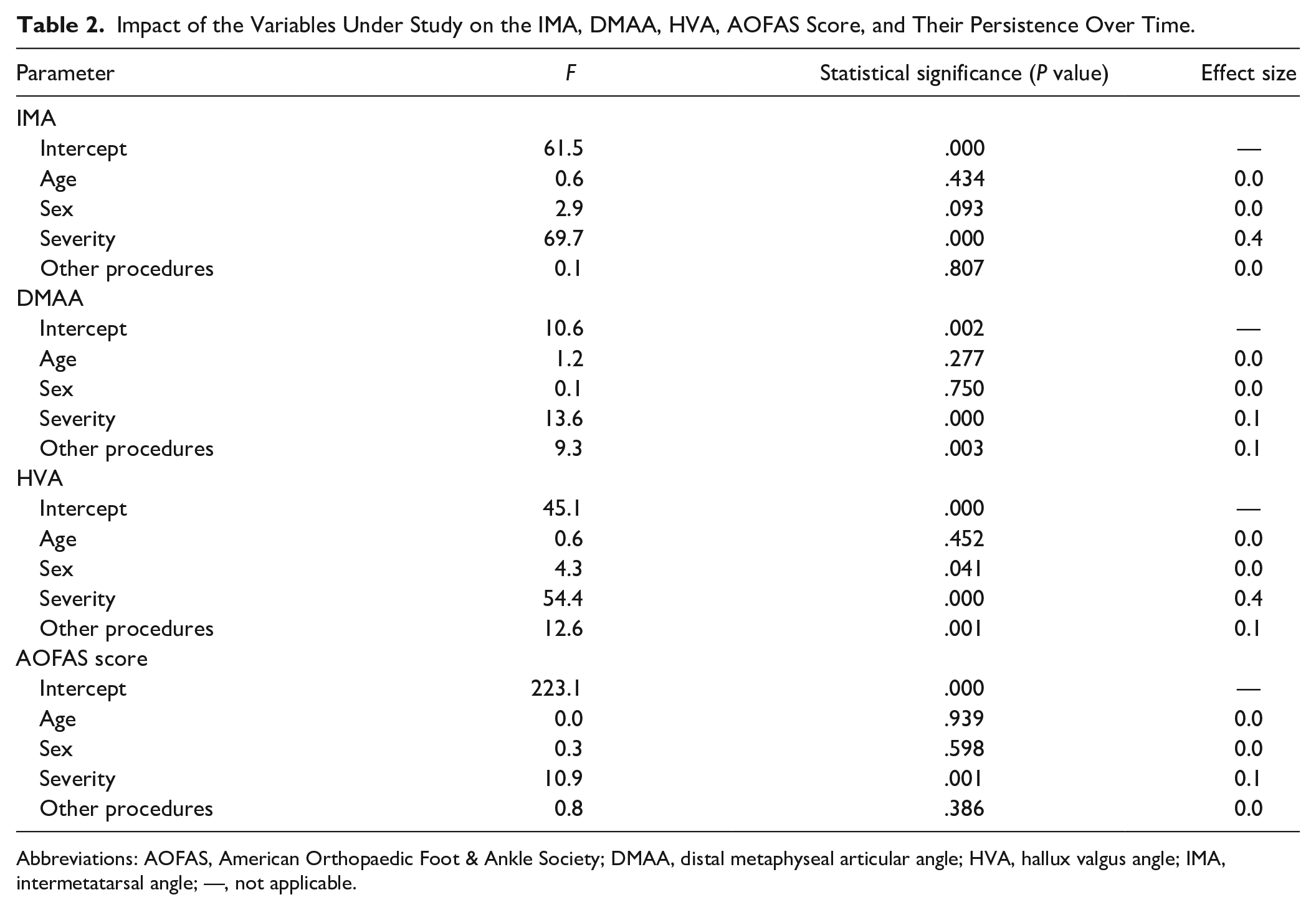
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; DMAA, distal metaphyseal articular angle; HVA, hallux valgus angle; IMA, intermetatarsal angle; —, not applicable.
Determinants of the Improvement in the IMA, DMAA, HVA, AOFAS Score, and Their Persistence Over Time.
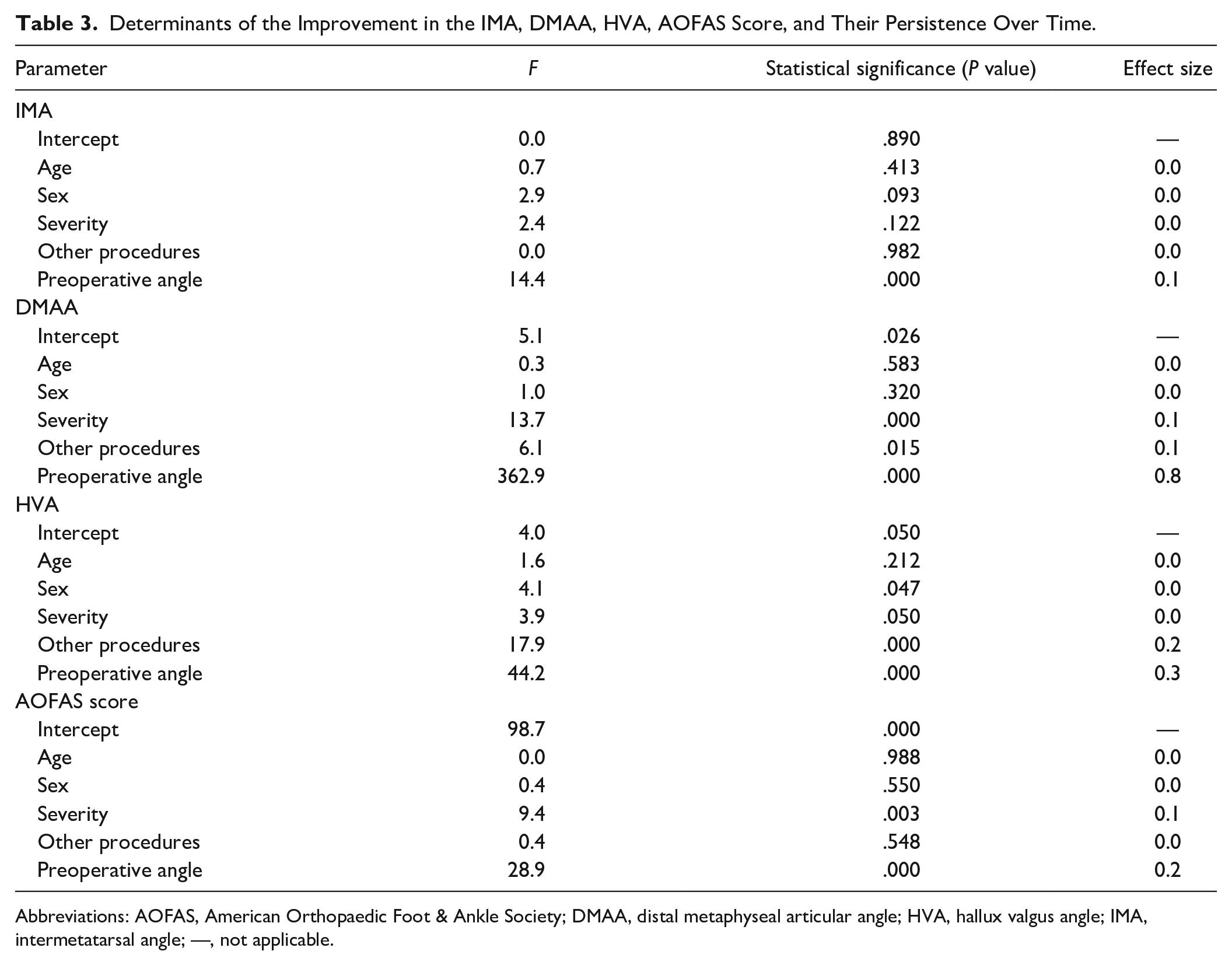
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; DMAA, distal metaphyseal articular angle; HVA, hallux valgus angle; IMA, intermetatarsal angle; —, not applicable.
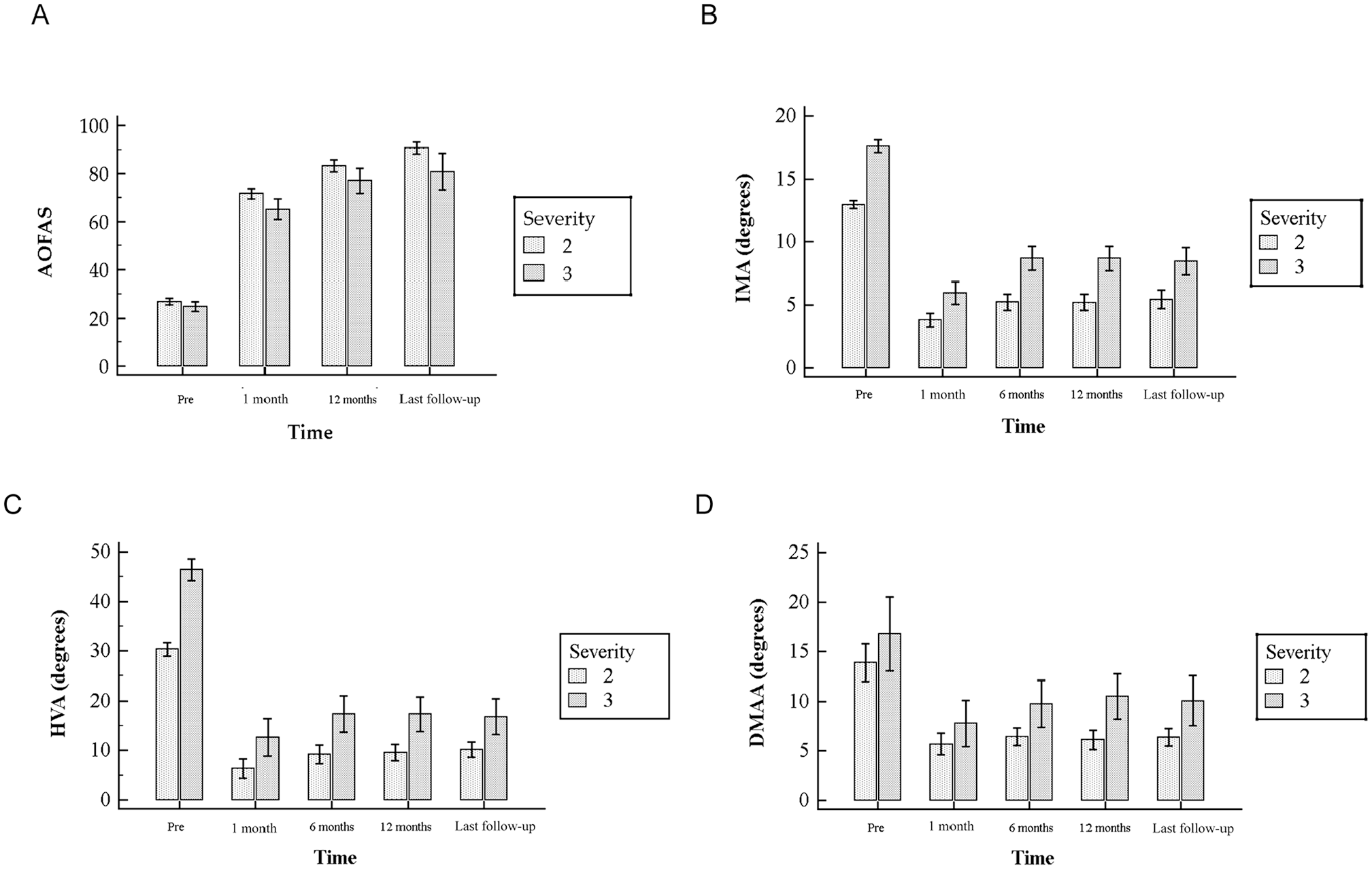
The impact of hallux valgus severity (2: moderate hallux valgus; 3: severe hallux valgus) on (A) AOFAS score, (B) IMA, (C) HVA, and (D) DMAA over time. AOFAS, American Orthopaedic Foot & Ankle Society; DMAA, distal metatarsal articular angle; HVA, hallux valgus angle; IMA, intermetatarsal angle.
At the last follow-up, mean satisfaction of the operative intervention was 8.7 ± 1.4, and perceived pain for the VAS scale was 1.5 ± 2.0. The former parameter did not differ between patients undergoing or not undergoing additional procedures (8.6 ± 1.3 vs 8.7 ± 1.5, respectively, P = .432), whereas the 2 groups of patients differed in terms of HV severity, resulting in higher satisfaction in less severe cases (8.9 ± 1.2 vs 8.2 ± 1.7, P = .041). VAS for rating pain did not differ in terms of additional surgical procedures (1.7 ± 2.0 vs 1.3 ± 2.1, P = .168) and HV severity (1.3 ± 1.9 vs 2.1 ± 2.3, P = .090) between the 2 groups of patients.
Radiological Outcomes
IMA significantly decreased after operative intervention, remaining lower over time (F = 20.54,
The effect of time was not statistically significant on the DMAA (F = 0.61,
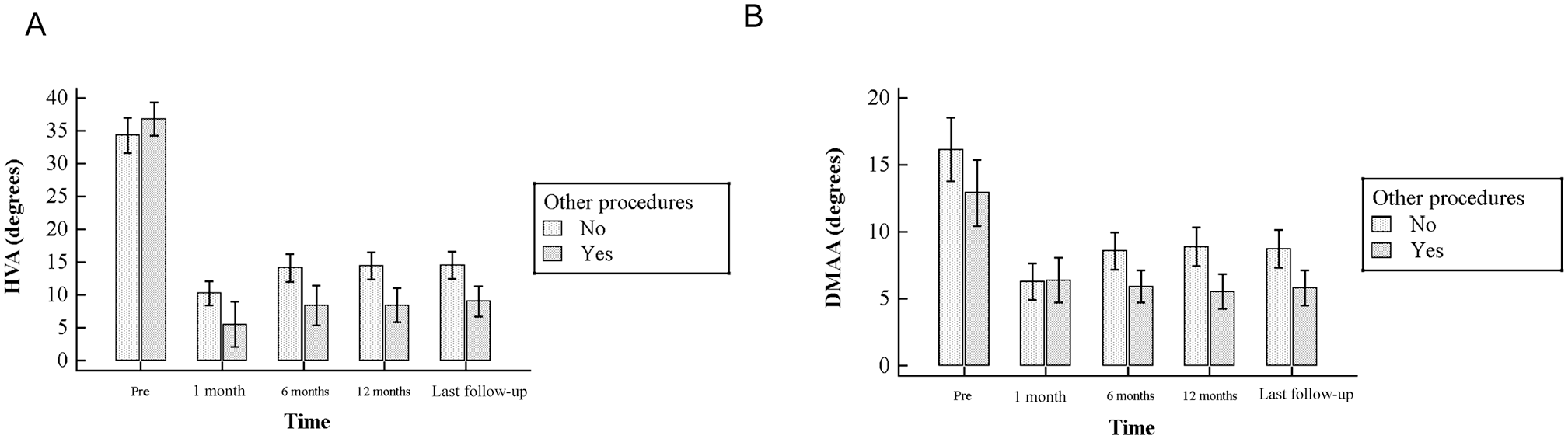
The impact of undergoing other procedures on (A) HVA and (B) DMAA. DMAA, distal metaphyseal articular angle; HVA, hallux valgus angle.
Severity (F = 13.68,
HVA significantly decreased after operative intervention over time (F = 10.65,
Operative intervention had a statistically significant impact on TSP (median position 2 before intervention and median position 1 at last follow-up [mean, 97 months] after intervention, Hodges-Lehmann median difference −1.5 [95% CI, −1.5 to −1], P < .001).
In the between subjects effects test (Table 2), the estimated marginal mean for male patients was higher compared to females (20.2 ± 1.5 vs 16.8 ± 0.7, mean difference 3.5 ± 1.7 [95% CI, 0.15-0.6.78], F = 4.29,
Finally, to verify the real effectiveness of MIIND in HV correction regardless of Akin osteotomy, a sensitivity analysis was performed, excluding those patients having undergone additional Akin osteotomy (20%). This analysis confirmed the effectiveness of the minimally invasive nature of MIIND in HVA correction (F = 360.49, P < .001) in both groups of patients (undergoing or not undergoing Akin), in whom no statistically significant impact on DMAA could be found in either group (P > .05).
Complications
There were superficial wound infections in 9 patients that were treated successfully with antibiotic therapy. No cases of osteomyelitis or postoperative lesser transfer metatarsalgia were recorded. Six cases of recurrence were observed at the last follow-up, while no cases of hallux varus due to overcorrection, malunion, delayed union, or nonunion were found. Only 6 of the 100 implants were removed 4 years after surgery because of occasional pain or irritation from the device. None of the patients experienced postoperative avascular necrosis of the I-MTTH.
Discussion
In accordance with the recommendations given in the literature23,62 for correction of mild to moderate HV, several distal MTT osteotomies have been reported to yield good clinical results. 67 However, only a relatively small amount of correction of this deformity is possible, and some shortening of the I-MTT results in consequent risk of avascular necrosis of the I-MTTH and transfer metatarsalgia. To our knowledge, only a few short- to medium-term retrospective studies have reported the outcomes involving the MIIND technique.4,5,20,21 Hence, this study was designed to evaluate its potential on the basis of clinical and radiographic data, even at long-term follow-up, in the correction of moderate to severe HV by a single surgeon and a large series of patients prospectively enrolled.
The main expectations of the patients before HV surgery are pain relief and improvement in wearing footwear and walking ability.15,63,68,69 In this case series, the MIIND technique, sometimes performed in association with Akin osteotomy and/or other lateral procedures (42%), resulted in good to excellent clinical and radiographic outcomes. Most of our patients’ expectations were satisfied, maintaining the results at last follow-up: mean VAS of 1.5 ± 2.0 and satisfaction rate of 8.7 ± 1.4. The mean AOFAS score improved from 26.2 to 69.6 points 6 months after surgery and remained high over time, with 81.4 points at the 12-month follow-up and 87.6 at the last follow-up of 97 months. The severity of the deformities (P = .003) and the preoperative AOFAS scores (P < .001) were associated with improvement in the HVA after surgery and its persistence over time. As expected regarding the different grades of deformity, postoperative mean AOFAS scores among patients with severe HV were significantly lower with respect to those with moderate HV (P = .001), even if the loss of correction over time trended toward significance (P = .051).
Our clinical results not only compare favorably to earlier reports,4,20,21 in which the postoperative AOFAS score had ranged from 82.2 to 93, but also show that good outcomes can be maintained in the long term. In a systematic review, 44 5 distinct groups of a total of 25 studies regarding current MI operative techniques were compared: Bosch and modifications (11 studies), chevron and Akin (5), Reverdin-Isham (4), MIIND (3), and distal soft tissue release [DSTR] and fixation (Akin or arthroscopically assisted DSTR and M1-M2 screw fixation; 2 studies). Although no MI techniques have shown superiority over others, the MIIND group showed excellent results in all of the studies assessed,5,20,21 giving a mean improvement in AOFAS score of 62.7 points vs 36.9 points achieved by the remaining 4 groups of studies analyzed and vs 61.4 points reported by the present study at longer follow-up of 97 months, which demonstrates the long-lasting effectiveness of the MIIND system. This evident improvement of the AOFAS score in the MIIND group could be attributed to the lesser severity of preoperative clinical aspects of the HVs included in the groups of the other MI techniques (AOFAS mean values: 55.8 points). In the MIIND group, more symptomatic HVs were treated (AOFAS mean values: 27.7 points). Furthermore, Malagelada et al 49 believe that these excellent results would be due to the hybrid nature of the MIIND procedure, completely different from traditional open distal osteotomy techniques, combining open surgery (direct view of the metatarsal) with those of percutaneous procedures (minimal skin incision and relying on fluoroscopic control), allowing proper correction of both moderate and severe forms of HV.
A recent randomized controlled trial pointed out no statistically significant differences between MIIND and Reverdin-Isham percutaneous osteotomy in the treatment of mild to moderate HV, providing both good to excellent outcomes. 21 However, distal metatarsal osteotomies,10,19,47-49 particularly the intra-articular ones, such as Reverdin-Isham,3,6 can lead to a greater risk of I-MTPJ stiffness, probably due to the need to perform LR. On the contrary, the MIIND, applied after an extra-articular osteotomy and without LR, reduces this risk.5,21
Data from the present study suggest that the multiplanarity of the correction (IMA), the large lateral displacement of the I-MTTH and its derotation (DMAA), 59 the clinical correction of valgus (HVA), 56 and the anatomic reduction of the tibial sesamoid (TSP) 55 had an important role for preventing the recurrence of valgus in almost all of our cases over time. Hence, this successful angular correction in this large series fully supports prior studies in which the MIIND was shown to be an effective method to correct moderate and severe angular values at short to medium follow-ups.4,5,20,21 In 4 previous studies4,5,20,21 ranging in size from 20 to 194 patients, the average correction of the HVA varied from 13.9 to 20.1 degrees, while the IMA was corrected by 5.95 to 9.9 degrees. In the current analysis, the long-term mean correction of the IMA, HVA, and TSP was 7.8, 20 degrees, and position 1, respectively, which was significantly different compared to the preoperative values (P < .001). However, regarding the persistence of DMAA correction over time, statistical significance was not achieved (P = .653), probably because of the presence of a high incidence of abnormal DMAA in our case series, rather than a real lack of decrease of its values. The severity of the deformity correlates significantly with the correction of DMAA (P < .001). In the MIIND technique, the DMAA correction is due to triplane movement of the I-MTTH after osteotomy exerted by the device during its gradual application. It is maintained by the angular stable screw fixation in the desired position between the nail and the I-MTTH until bone consolidation. Failure to achieve proper fixation may result in a higher incidence of complications, including delayed union and malunion, which lead to first ray dorsiflexion and recurrence. Technically, an excessively oblique placement of a fixation screw may lead to penetration of the I-MTPJ, causing progressive degenerative arthritis of this joint.
It has been shown that there is a significant relationship between reduction of sesamoids and recurrent deformities.11,55,65 In the present study, a significant improvement of TSP was achieved because the device permitted the derotation and relocation of the I-MTTH during lateral translation above the sesamoids without performing the LR of the sesamoid complex. During the MIIND technique, surgeons should be meticulous in the correction of IMA and HVA by proper bunionectomy, linear osteotomy, and adequate I-MTTH lateral translation to achieve the optimal balancing of the sesamoid complex. Our previous 5 and present findings, in line with those of other reports,14,41,45 suggest that LR is not necessary when a distal extra-articular osteotomy is performed. Associating LR, whether open or MI, to an extra-articular distal osteotomy could involve an overcorrection and consequent hallux varus,9,13,28 increase the risk of postoperative stiffness of the I-MTPJ, 42 and cause neurovascular injuries. 33 In particular, a correlation between avascular necrosis and open LR has been found during traditional distal osteotomy techniques,33,71 while a high risk of neuritis has been found after LR in the MI procedure.1,46
A high rate of simultaneous additional procedures was recorded (42%), including 20 Akin osteotomies, which positively influenced HVA values and significantly correlated with the severity of deformity. Hence, further procedures were required because of the severity of forefoot deformities. However, the sensitivity analysis, performed after exclusion of patients who underwent additional Akin procedures (20%), confirmed the effectiveness of MIIND in HVA correction (F = 360.49, P < .001).
Female sex was observed to be associated with effective correction of the HVA after surgery31,58 and its persistence over time (P = .047). However, in line with the recent literature, 12 the male patient group achieved greater correction of HVA than the female patient group (P = .041). Age did not have any impact on the radiological parameters assessed; hence, the MIIND technique can be used in adults within a wide age range (20-80 years).
Complications
A common complication after distal I-MTT osteotomy is HV recurrence, mainly due to undercorrection,28,37 with rates reported to be as high as 16%. 43 Often, the recurrences have been described in connection with different operative methods, independent from the implementation of an Akin osteotomy.35,36 This loss of correction has been shown to correlate with the preoperative HVA, IMA, DMAA, TSP, and I-MTPJ congruency.59,60
Among the current MI techniques, the complication rates varied widely even within the same groups. 49 The Bosch technique was reported to have 0% complication rates by some authors 26 and 22% by others. 14 The Reverdin-Isham technique varied from a 5% 3 to 73% 27 rate of complications. This last high complication rate was due to the exclusive evaluation of children younger than 16 years, showing high rates of recurrence. In the chevron Akin group, complications were between 0% and 40%.34,49 However, if the early stages subgroups from the analysis are excluded, the overall complication rate becomes 13%. 49 In the other studies published regarding the MIIND,4,5,20,21 the incidence of complications ranged from 0% to 5%. In 1 study, the recurrence of deformity or undercorrection was reported to be 2%. 4 In our study, 6 of 100 patients (6%) complained of HV recurrence. None of these patients underwent operative revision because all patients had good functional outcomes at last follow-up with an AOFAS score >70 and a VAS for satisfaction rated as “good” in 5 cases and “fair” in 1 case.
In our series, there were no sequelae associated with metallic fixation, such as loosening or breakage of the implant; no cases of malposition of the device or the I-MTTH with consequent delayed or nonunion were recorded. As the MIIND provides completely internal fixation, the risk of infection is reduced with respect to other techniques that use percutaneous K-wires. 52 No deep infection of soft tissues or osteomyelitis was found among our patients. However, there have been a few cases of hardware intolerance with occasional pain or irritation. Thus, 6 implants were removed 4 years after surgery with resolution of symptoms. This was probably due to the technical characteristics of the MIIND, which is completely endomedullary except for the blade (8 mm long × 2.3 mm wide × 14 mm high) fixed on the lateral part of the head, which could have been the cause of soft tissue irritation in these cases.
Although implant removal is associated with increased costs and further surgery, we found this small nail to be easy to remove without risk of I-MTT bone fractures. Avascular necrosis of the I-MTTH, the most serious complication of HV operative correction by distal osteotomy, was not observed in this case series or in our previous one or other similar experiences with the MIIND.4,5,20,21
Strengths and Weaknesses
The strengths of our study include (1) the prospective data collection of this case series, whose size was calculated a priori, with the same fixed follow-ups until the long-term one; (2) the large consecutive patient inclusion (100 implants); (3) the standardization of patient operations and aftercare; (4) the analysis of the clinical and radiographic outcomes, carried out separately by independent investigators (the one who performed clinical assessment was blinded to the type of procedure used); and (5) the multivariable statistical analysis, performed by an independent statistician, also blinded to the type of operative treatment. We are also aware of its weaknesses: (1) single-center, case series study and single surgeon for all operations, aspects that could have affected the generalizability of the operative procedure; (2) the retrospective analysis of prospectively collected data and the lack of a control group, which prevented us from comparing results; and (3) the use of the AOFAS score for the outcome measure, which, although it was the most widespread health measurement in foot and ankle clinical practice when the data collection began, was only partly validated 17 and may have overlooked some clinical aspects, such as psychological ones. This physician-based score does not have items directly related to psychological health and does not adequately consider the patient’s point of view. 17 For these reasons, VAS for patients’ satisfaction was used in this study. For future studies, other scores are now available (eg, the Foot and Ankle Outcome Score, which has been shown to be a valid score for assessing patients with HV). 73
Conclusion
Being aware that a single ideal procedure adequate to cover all deformities of HV has not been described, our data showed that the MIIND technique was a viable procedure for correction of moderate to severe HV at long-term follow-up, with a low rate of complications and recurrence. In our series of adult patients with a wide age range, the device allowed improvement of variable preoperative clinical and radiographic cases, resulting in a significant reduction of most radiographic parameters and a significant improvement of clinical scores, maintaining these results over time. Furthermore, in cases of concomitant forefoot disorders, additional percutaneous osteotomies, such as Akin and DMMO, can be associated successfully.
Supplemental Material
sj-pdf-1-fai-10.1177_1071100720969676 – Supplemental material for Functional and Radiographic Outcomes of Minimally Invasive Intramedullary Nail Device (MIIND) for Moderate to Severe Hallux Valgus
Supplemental material, sj-pdf-1-fai-10.1177_1071100720969676 for Functional and Radiographic Outcomes of Minimally Invasive Intramedullary Nail Device (MIIND) for Moderate to Severe Hallux Valgus by Carlo Biz, Alberto Crimì, Ilaria Fantoni, Jacopo Tagliapietra and Pietro Ruggieri in Foot & Ankle International
Footnotes
Acknowledgements
We thank Nicola Luigi Bragazzi, MD, PhD, for assistance provided in clinical and radiological statistical analysis of the data and Elisa Belluzzi, PhD, for her preliminary general analysis.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data and Materials
The data set supporting the conclusions of this article is available at our institution.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.