
Abstract
Background:
Historically, microfracture has been used to treat small talar osteochondral lesions with good results, whereas osteochondral autologous transplantation (OAT) has proven effective for the treatment of larger lesions. It is not clear which method is more effective for medium-sized lesions around the critical size of 150 mm2, above which microfracture outcomes tend to be poor. The purpose of this study was to determine the potential advantages of OAT augmented with a combination of extracellular matrix and bone marrow aspirate concentrate (ECM-BMAC) compared to debridement with ECM-BMAC (DEB) in the treatment of medium-sized osteochondral lesions of the talus (OLTs).
Methods:
Clinical and radiographic data were collected retrospectively for patients treated by a single fellowship-trained foot and ankle surgeon. Magnetic resonance images (MRIs) were scored using the Magnetic Resonance Observation of Cartilage Tissue (MOCART) system and were evaluated for the presence of cysts and edema. Fifty-two patients met inclusion criteria, with 25 who received an OAT procedure. Age, body mass index, lesion size, lesion location, and follow-up time were similar between groups. Average MRI follow-up times were 16.7 months for the OAT group and 20.3 months for the DEB group (P = .38).
Results:
Patients treated with OAT had significantly higher average total MOCART scores (69 vs 55, P = .04) and significantly lower rates of cyst (14% vs 55%, P < .01), edema (59% vs 90%, P = .04), revision surgery (0% vs 19%, P = .05), and therapeutic injection for pain (4% vs 30%, P = .02) compared to patients treated with DEB. No significant differences were detected in patient-reported outcome scores between groups.
Conclusion:
The native hyaline cartilage introduced by OAT appears to result in higher-quality repair tissue when compared to DEB, as evidenced by OAT patients’ higher MOCART scores and lower rates of cyst and edema. There was no difference in clinical outcome scores, though OAT patients did not require revision surgery or therapeutic injection for pain as frequently as DEB patients.
Level of Evidence:
Level III, retrospective comparative study.
Keywords
Introduction
Several operative approaches have been described to repair osteochondral lesions of the talus (OLTs). Microfracture has been considered the gold standard treatment for smaller, symptomatic OLTs because it is a simple, single-stage procedure that can be performed arthroscopically with low morbidity. 10 The microfracture procedure involves penetrating the subchondral bone to promote the migration of mesenchymal stem cells to the area of cartilage injury. Although microfracture and arthroscopic bone marrow stimulation procedures have been shown to produce good to excellent results in approximately 80% to 85% of patients, outcomes seem to deteriorate over time.4,7,23 This may be due to the fact that the resulting tissue is composed of fibrocartilage, which has been shown to be biomechanically inferior to native hyaline cartilage. One recent study found that during second-look arthroscopy at a mean of 3.6 years after microfracture, more than one-third of lesions had not completely healed and demonstrated inferior tissue quality. 22 The fibrocartilage that results from microfracture is structurally lacking compared with native cartilage.
In addition to this shortcoming of fibrocartilage formation, microfracture has also been shown to be a less successful treatment for larger OLTs. Lesion size has been found to be a predictive factor for success in operative treatment of OLTs. 5 Several authors have reported that patients treated for OLTs larger than a critical size of 150 mm² had poorer outcomes than those treated for smaller lesions.5,6,10 Thus, although microfracture has generally been found to improve clinical outcomes for smaller lesions, other operative interventions are needed to treat larger lesions effectively. 10
The existing literature suggests that procedures such as osteochondral allograft or autograft transplantation are effective in treating larger lesions.2,5,6,11,12,19,20 Osteochondral autologous transplantation (OAT) involves retrieving a plug of native cartilage from the femoral condyle and inserting it into the talar defect. Though OAT has the potential for donor site morbidity and requires a malleolar osteotomy, the use of transplanted autograft bone and native hyaline cartilage may be advantageous when compared to microfracture, as native cartilage is biomechanically superior to the fibrocartilage that forms following microfracture.
Although microfracture remains the standard procedure for smaller lesions, and OAT or other similar procedures are preferred for larger lesions, the optimal procedure for medium-sized lesions around or slightly smaller than the critical size of 150 mm² remains unclear. The aim of this study was to retrospectively compare clinical and radiographic outcomes following the treatment of medium-sized OLTs (80-165 mm²) with an arthroscopic debridement procedure or OAT. Both of the procedures assessed in this study were augmented with a combination of extracellular matrix and bone marrow aspirate concentrate (ECM-BMAC). We hypothesized that patients treated with OAT would demonstrate better postoperative outcomes compared with those treated arthroscopically with debridement plus ECM-BMAC (DEB) because of the introduction of native hyaline cartilage into the site of the OLT.
Methods
Study Population and Design
After obtaining approval from our institution’s institutional review board (IRB) and IRB-approved steering committee, which oversees the institution’s foot and ankle registry, patients were identified using relevant Current Procedural Terminology codes for DEB or for OAT with knee autograft. In each case, treatment type was based on surgeon preference. OAT was generally used for revision cases, as well as cases involving deeper lesions or those with a cystic component. Patients treated for an OLT between 2015 and 2018 by a single surgeon fellowship-trained in sports medicine and foot and ankle surgery were screened.
Retrospective chart review was performed to determine operative treatment, concurrent injuries, and demographic information. Patients undergoing DEB or OAT with lesion size between 80 and 165 mm² and minimum follow-up of 12 months were eligible for inclusion. Based on operative notes, it was confirmed that all operative repairs were augmented with an adjuvant mixture of ECM-BMAC. Lesion size (in square millimeters) and location (medial, lateral, or central talus) were also noted based on operative notes or assessment of preoperative magnetic resonance images (MRIs). Clinical outcomes, including failure or postoperative therapeutic injection, were also noted during chart review. Failure was defined as a patient either undergoing revision or being recommended for revision because of persistent pain.
Patient-reported functional outcomes were collected through our institution’s prospective registry database. Patients treated prior to March 2016 were administered preoperative Foot and Ankle Outcome Score (FAOS) questionnaires. Patients treated after this date were administered preoperative Physical Function, Pain Interference, Pain Intensity, Global Physical Health, Global Mental Health, and Depression Patient-Reported Outcomes Measurement Information System (PROMIS) domains. Both FAOS and PROMIS were administered postoperatively.
Fifty-two patients were identified who fit inclusion criteria. Twenty-seven of these patients received DEB, and 25 patients received OAT with ECM-BMAC. Thirty patients were female and 22 were male. There was no significant difference between groups in age, body mass index (BMI), average lesion size, or lesion location (Table 1). In total, 10 patients were treated for concurrent pathologies at the time of the index procedure. In the OAT group, 6 patients presented with ankle instability requiring stabilization. Four of these received a Brostrom-Gould stabilization and 2 received lateral ligament reconstruction with hamstring autograft. In the DEB group, 2 patients received a Brostrom-Gould stabilization, 1 received open reduction and internal fixation of the syndesmosis, and 1 received debridement and tenolysis of the flexor hallucis longus. Three of 27 DEB cases were revision cartilage treatments, compared to 17 of 25 OAT cases. Of the 3 DEB revision cases, 1 had previously received microfracture at an outside hospital, 1 had a DeNovo cartilage allograft procedure with the senior author, and 1 had open cartilage restoration at an outside hospital. Prior procedures before OAT included 10 microfractures, 2 DEBs, 2 debridements, 1 retrograde drilling, 1 osteochondral fixation, and 1 allograft OAT. All but 3 of these prior procedures were done at outside hospitals.
Comparison of Demographic Variables Between Groups.
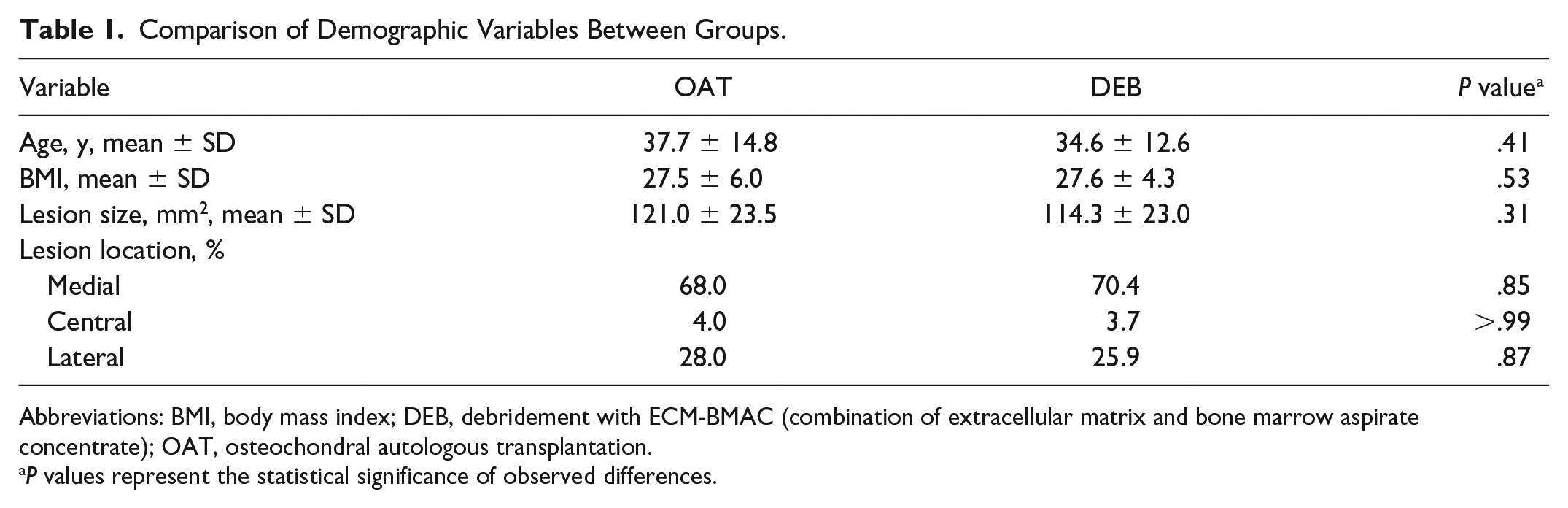
Abbreviations: BMI, body mass index; DEB, debridement with ECM-BMAC (combination of extracellular matrix and bone marrow aspirate concentrate); OAT, osteochondral autologous transplantation.
P values represent the statistical significance of observed differences.
MRI Assessment
Patients who had not already received a postoperative MRI at the time of study were contacted to return to the hospital for MRI studies, which were billed to a departmental research fund. All magnetic resonance (MR) images were reviewed by a radiologist fellowship-trained in musculoskeletal radiology. MRIs were evaluated using the modified Magnetic Resonance Observation of Cartilage Tissue (MOCART) score, which has been utilized in the literature to evaluate MRIs. 14 MOCART scoring uses 9 parameters to evaluate the morphology and signal intensity of the repair tissue. It has been shown to be a reliable measure to evaluate cartilage repair radiographically. 14 Because MOCART is designed to assess cartilage repair tissue, only postoperative studies were scored. All MRIs were performed at our institution using a standardized protocol and 1.5-tesla scanner.
Operative Techniques: Debridement Plus ECM-BMAC (DEB)
A modified version of a standard operative technique for microfracture was used. 7 First, a thigh tourniquet was applied and standard anteromedial and anterolateral arthroscopic portals were established. Once identified, the lesion was inspected and palpated with a probe. It was then debrided until it was bordered by normal, healthy cartilage. This included debridement of any necrotic bone or cystic tissue surrounding the lesion. The area around the lesion was also debrided using a mechanical shaver in order to remove any scar tissue, osteophytes, or loose fragments that were present. No iatrogenic perforation of the subchondral plate was performed.
In order to prepare the ECM-BMAC, roughly 60 mL of bone marrow was withdrawn from the anterior superior iliac crest and concentrated using the Magellan Autologous Platelet Separator (Anteriocyte Medical Systems, Cleveland, OH) in order to produce about 3 mL of BMAC. For cases that include a significant bone defect, necrotic bone, or a void resulting from a subchondral cyst that was 1 cm or greater in depth, bone graft was used to fill the base of the lesion. When necessary, bone graft was harvested at this time from the calcaneus or iliac crest, depending on the defect’s size. All fluid was then removed from the ankle joint using vacuum suction. An epidural spinal needle was placed into the joint posteriorly, from just lateral to the Achilles tendon, in order to prevent moisture buildup that would have reduced visibility during the dry portion of the arthroscopy. At this point, the ECM was mixed with the BMAC from the iliac crest. If needed, the bone graft was placed into the defect using an arthroscopic cannula and was packed down with a Freer elevator to form a stable bed at the base of the lesion. The defect was then filled with ECM-BMAC using an arthroscopic cannula. It either rested on the subchondral bone or on top of the bone graft, if one was used. A Freer elevator was used to spread ECM-BMAC over the entire defect until adequate coverage was achieved (Figure 1). The ECM-BMAC was also covered with a layer of Evicel (Johnson & Johnson, Somerville, NJ) to keep the graft in position. The leg was kept in traction while the fibrin glue set, which typically took 10 minutes.
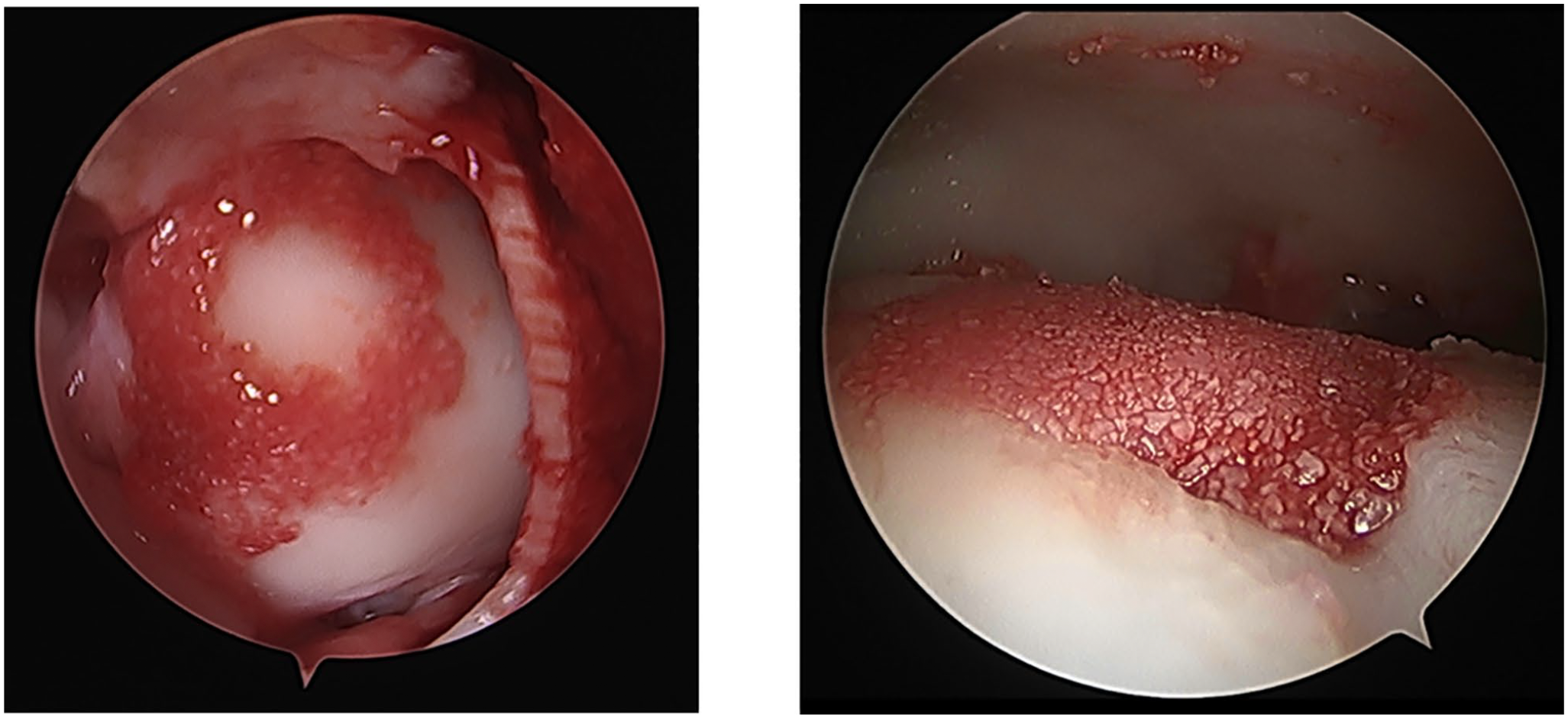
(Left) Example of OAT plug surrounded by ECM-BMAC. (Right) DEB. Lesion filled with ECM-BMAC arthroscopically after debridement. DEB, debridement with ECM-BMAC (combination of extracellular matrix and bone marrow aspirate concentrate); OAT, osteochondral autologous transplantation.
Operative Techniques: OAT With ECM-BMAC
OAT is also a commonly used procedure and has been supported by multiple studies and a position statement by the American Orthopaedic Foot & Ankle Society. 3 The use of ECM-BMAC to augment OAT is considered experimental at this time. First, BMAC was harvested in similar fashion as above. A thigh tourniquet was routinely used, and standard anteromedial and anterolateral portals were established for diagnostic arthroscopy. Standard arthroscopic debridement was performed. A 5- to 6-cm curvilinear incision was made over the medial malleolus, and sharp dissection was performed through the skin and subcutaneous tissue. The first step was to identify and protect the posterior tibial tendon, as it passes just posterior to the medial malleolus. A K-wire was passed from proximal to distal, typically from the flare of the tibia to the shoulder to replicate the direction of the osteotomy (Figure 2). Next, a chevron-type osteotomy was performed, and the osteochondral lesion was visualized. The lesion was inspected to determine the number of osteochondral grafts to be harvested, which are typically 10 mm in diameter. Once a guide wire was placed at the center of the lesion, it was reamed to a depth of 12 to 14 mm. Any existing cysts were curetted and if any necrotic bone or degenerative cartilage remained, it was also removed.
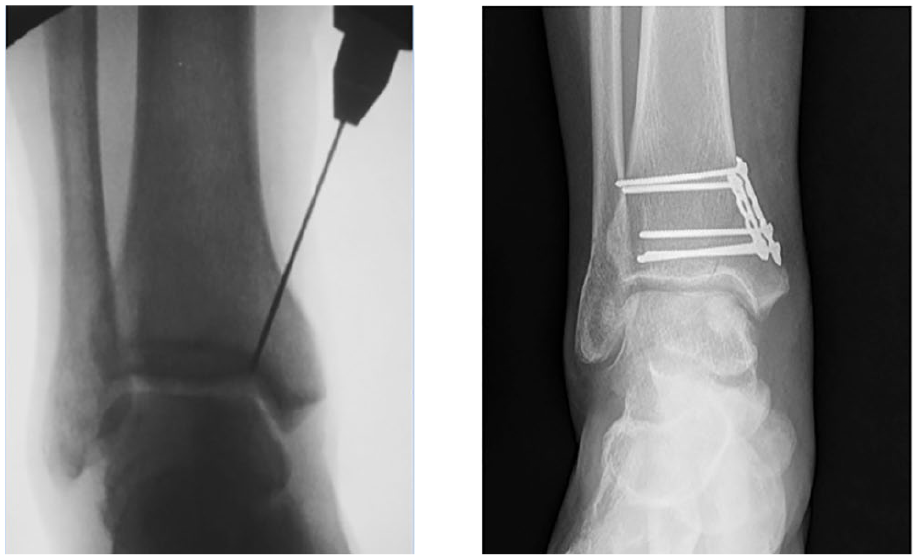
(Right) K-wire passed prior to osteotomy. (Left) The osteotomy is repaired using 2 plates.
In order to procure the autografts from the patient’s ipsilateral knee, a 3 to 4 cm incision was made over the lateral aspect of the patella. The lateral retinaculum was incised in line with its fibers. One or 2 grafts that were 13 to 15 mm deep and 10 mm in diameter were then taken from the lateral aspect of the trochlea. These plugs were shaped to fit the lesion and soaked in BMAC. It was important to ensure that the depth of the grafts matched the depth of the lesion to reduce any areas of proud or sunken graft compared to the surrounding talus. The area from which the autograft was procured in the trochlea was filled with a JFR allograft plug (Arthrex Inc, Naples, FL).
As with arthroscopic DEB, bone graft was first be placed in the base of the lesion if required. The plug was then placed in the lesion so that it sat perfectly level with the talar dome. ECM and BMAC were combined and this mixture was placed around the autograft (Figure 1). A Freer elevator was used to fill any surrounding areas of damaged cartilage and to ensure that the borders between the plug and talus were adequately filled. A layer of Evicel was placed over the repair and was allowed to dry for 10 minutes. Finally, the medial malleolar osteotomy was repaired per the surgeon’s preference and often with 2 plates (Figure 2). The ankle and knee incisions were repaired prior to placing the patients in a nonweightbearing splint for 2 weeks. At that point, each group started range of motion and physical therapy exercises. Partial weightbearing was initiated 6 weeks after surgery for both OAT and DEB patients.
Statistical Analysis
Analyses were performed for clinical outcomes, FAOS and PROMIS patient-reported scores, and radiographic outcomes, MOCART scores and presence of cysts and edema. All analyses were run with a significance level of .05. Demographic variables such as age, BMI, lesion size, and lesion location were also analyzed. Student paired and 2-group t tests were used to evaluate pre- to-postoperative changes in scores and differences between procedure groups. Categorical variables such as lesion location, revision rate, injection rate, and rate of cyst or edema were compared using the Fisher exact test or chi-square test, depending on the available sample size.
Results
Radiographic Outcomes
Twenty MRIs were collected for the group treated with DEB, and 22 were collected for the group treated with OAT. Average follow-up time to MRI was 20.3 months (SD ± 14.1 months; range 5-51 months) for DEB and 16.7 months (SD ± 11.9 months; range 4-47 months) for OAT. Difference in follow-up time to MRI was not statistically significant (P = .38). Minimum radiographic follow-up was 4 months. The average total MOCART score of 68.9 for the OAT group was significantly better than the average of 55.3 for the DEB group (P = .04) (Table 2).
Comparison of Postoperative Radiographic Outcomes.
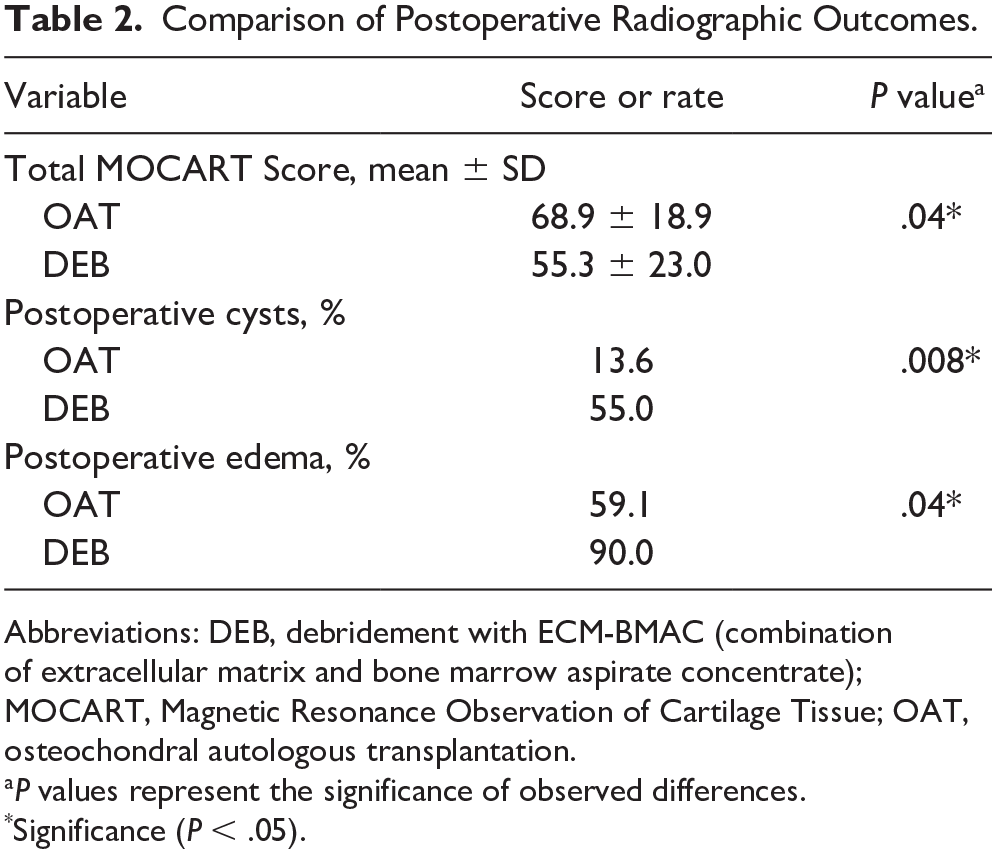
Abbreviations: DEB, debridement with ECM-BMAC (combination of extracellular matrix and bone marrow aspirate concentrate); MOCART, Magnetic Resonance Observation of Cartilage Tissue; OAT, osteochondral autologous transplantation.
P values represent the significance of observed differences.
Significance (P < .05).
The group treated with OAT experienced significantly lower rates of postoperative cysts (P < .01) and edema (P = .04) as determined by a board-certified, musculoskeletal fellowship–trained radiologist’s evaluation of postoperative MRIs (Table 2). 13.6% of MRIs for OAT patients showed postoperative cysts compared to 55.0% for the group treated with DEB. Overall, 59.1% of MRIs for OAT patients had postoperative edema compared to 90.0% for DEB patients (Table 2).
When comparing individual MOCART categories, the OAT group had significantly better scores than the DEB group for both subchondral lamina (P < .01) and subchondral bone (P < .01). No significant differences were observed for the other MOCART categories, but the average scores for OAT patients were higher in all but 2 categories, Adhesions and Infill (Supplemental Table S1).
Functional Outcomes
In 2016, our foot and ankle department began administering PROMIS surveys instead of FAOS surveys, meaning that the number of patients with complete FAOS data was small. For patients with postoperative FAOS, average follow-up time was 22.2 months (SD ± 7.1) for patients treated with DEB and 28.8 months (SD ± 11.6) for OAT patients. This difference was not statistically significant (P = .07). In the OAT group, 6 patients completed FAOS both pre- and postoperatively, and significant improvement in scores was detected for the Pain, Sports Activities, and Quality of Life categories, as well as for total FAOS (Supplemental Table S2). Seven of the patients treated with DEB completed both pre- and postoperative FAOS surveys, but no significant improvements were observed for this group (Supplemental Table S3). Between treatment groups, no significant differences were observed in either mean postoperative FAOS or mean pre to postoperative change for individual FAOS categories or for total FAOS (Table 3).
Comparison of FAOS for OAT and DEB Treatment.
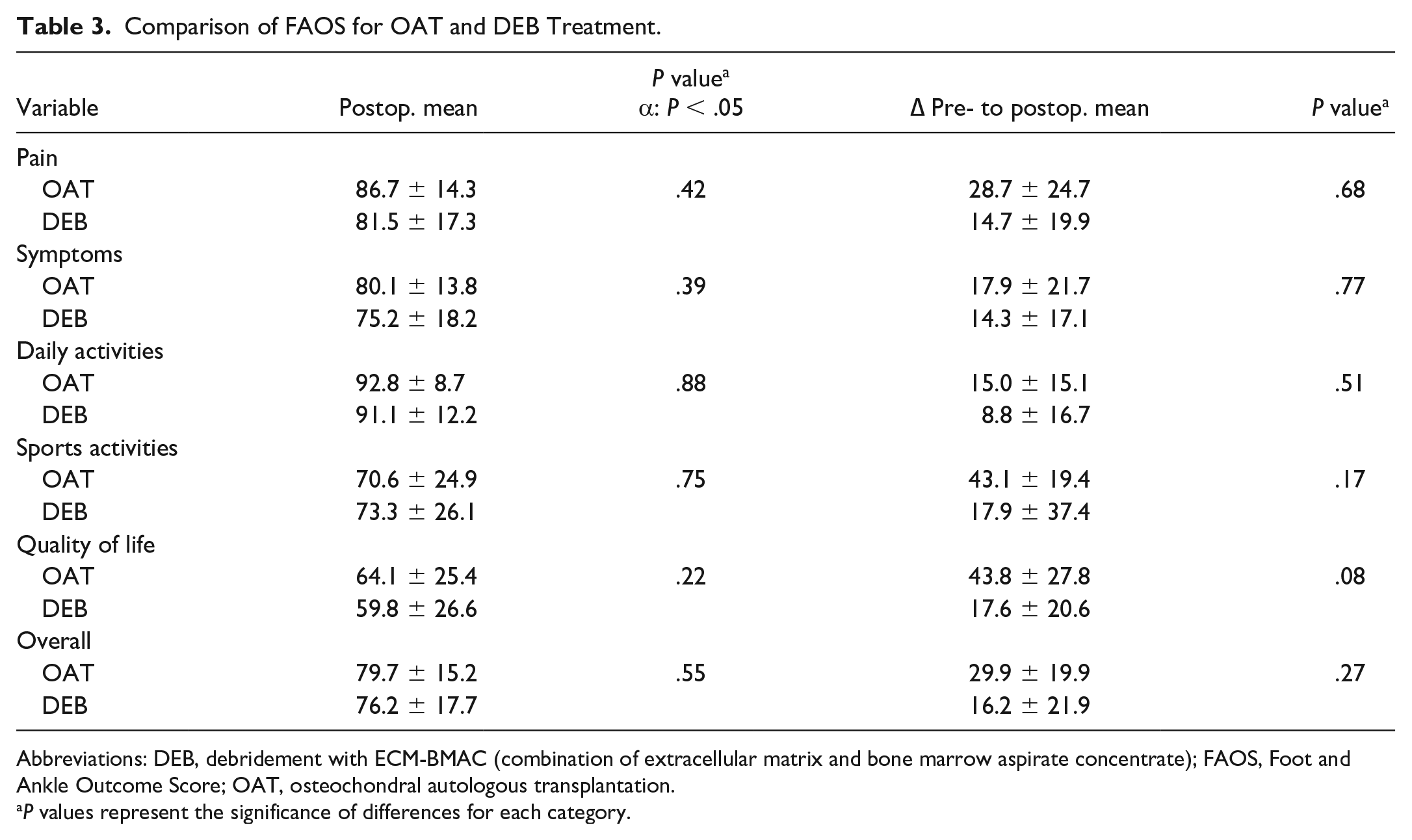
Abbreviations: DEB, debridement with ECM-BMAC (combination of extracellular matrix and bone marrow aspirate concentrate); FAOS, Foot and Ankle Outcome Score; OAT, osteochondral autologous transplantation.
P values represent the significance of differences for each category.
Average follow-up time to postoperative PROMIS survey was 24.4 months (SD ± 10.8) for OAT patients and 24.8 months (SD ± 11.9) for DEB patients. This difference was not statistically significant (P = .92). Eleven of the patients who received OAT treatment completed both pre- and postoperative surveys, and significant improvements were observed in the Physical Function, Pain Interference, Global Physical Health, and Pain Intensity domains (Supplemental Table S4). Significant pre to postoperative improvement was observed in these same categories for the 14 DEB patients who completed both pre- and postoperative surveys (Table 6). On average, neither group demonstrated significant improvement in Global Mental Health or Depression between pre- and postoperative surveys. Between treatment groups, no significant differences were observed in either postoperative means or the average pre- to postoperative change for any of the PROMIS domains (Table 4).
Comparison of PROMIS Scores for OAT and DEB.
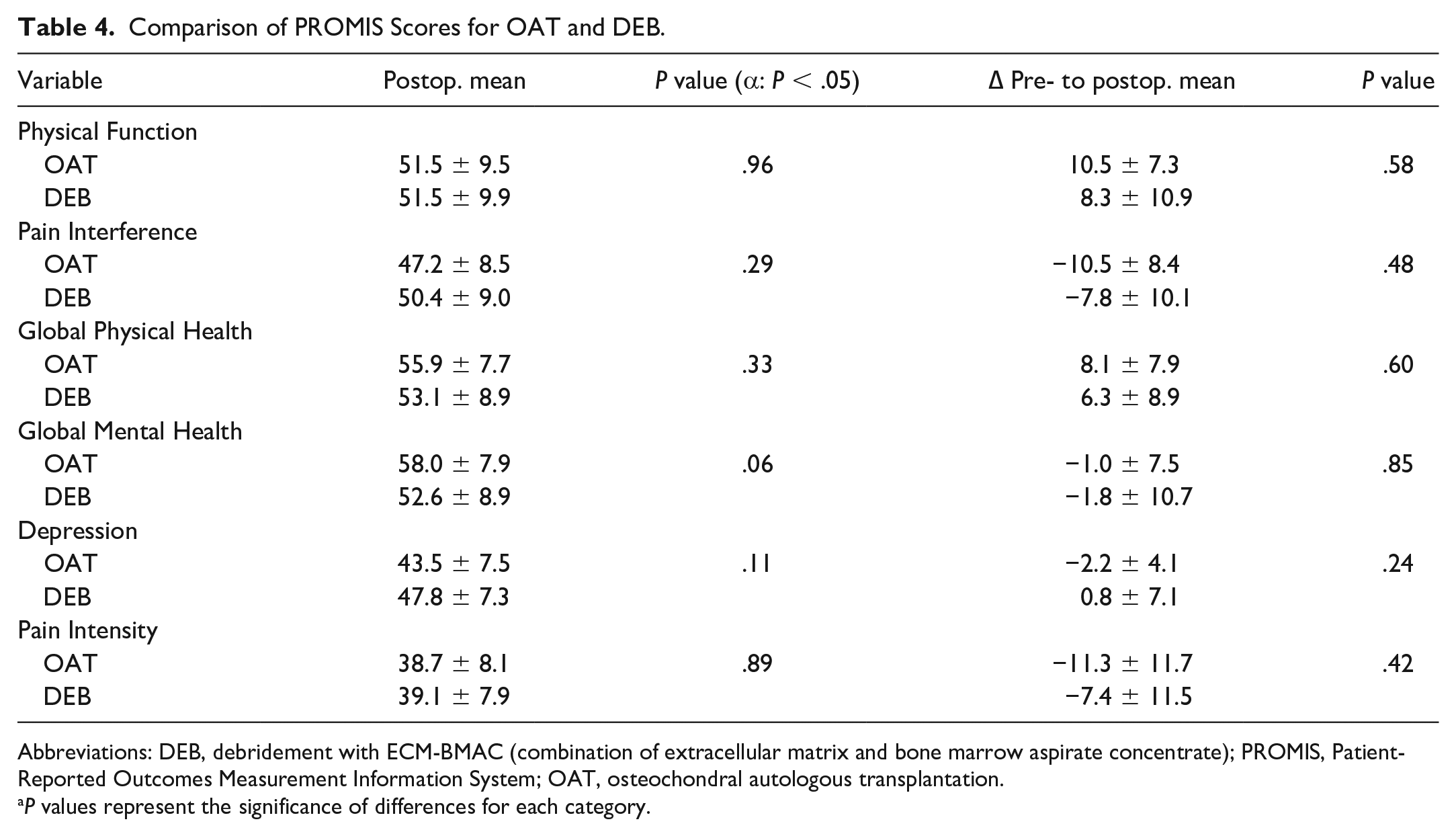
Abbreviations: DEB, debridement with ECM-BMAC (combination of extracellular matrix and bone marrow aspirate concentrate); PROMIS, Patient-Reported Outcomes Measurement Information System; OAT, osteochondral autologous transplantation.
P values represent the significance of differences for each category.
Revision Surgery and Therapeutic Injection
There were 5 failures out of 27 patients in the DEB group. Three patients underwent revision to OAT and 2 more were recommended for revision but did not schedule surgery. These 3 OAT revision patients were not included in the OAT cohort because of inadequate follow-up at the time of this study. These revision patients lacked complete follow-up surveys, as they were not collected before their revision procedure. By comparison, none of the 25 patients in the OAT group experienced failure, a statistically significant difference (P = .05; Table 5). Eight of 27 patients treated with DEB were recommended for an injection due to persistent pain, whereas 1 of 25 OAT patients were recommended for injection. This difference was also statistically significant (P = .02). Two of these DEB patients who received injection did not experience lasting relief and went on to revision to OAT. MRIs of those cases requiring revision surgery showed persistent edema surrounding the repair site.
Comparison of Revision and Injection Rates.
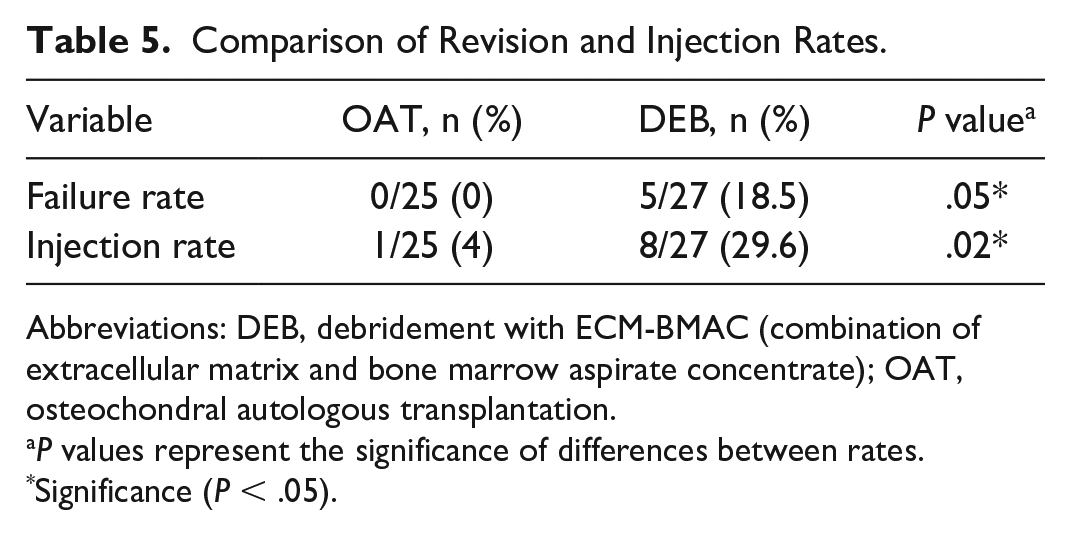
Abbreviations: DEB, debridement with ECM-BMAC (combination of extracellular matrix and bone marrow aspirate concentrate); OAT, osteochondral autologous transplantation.
P values represent the significance of differences between rates.
Significance (P < .05).
PROMIS Scores for the DEB Patient Group.
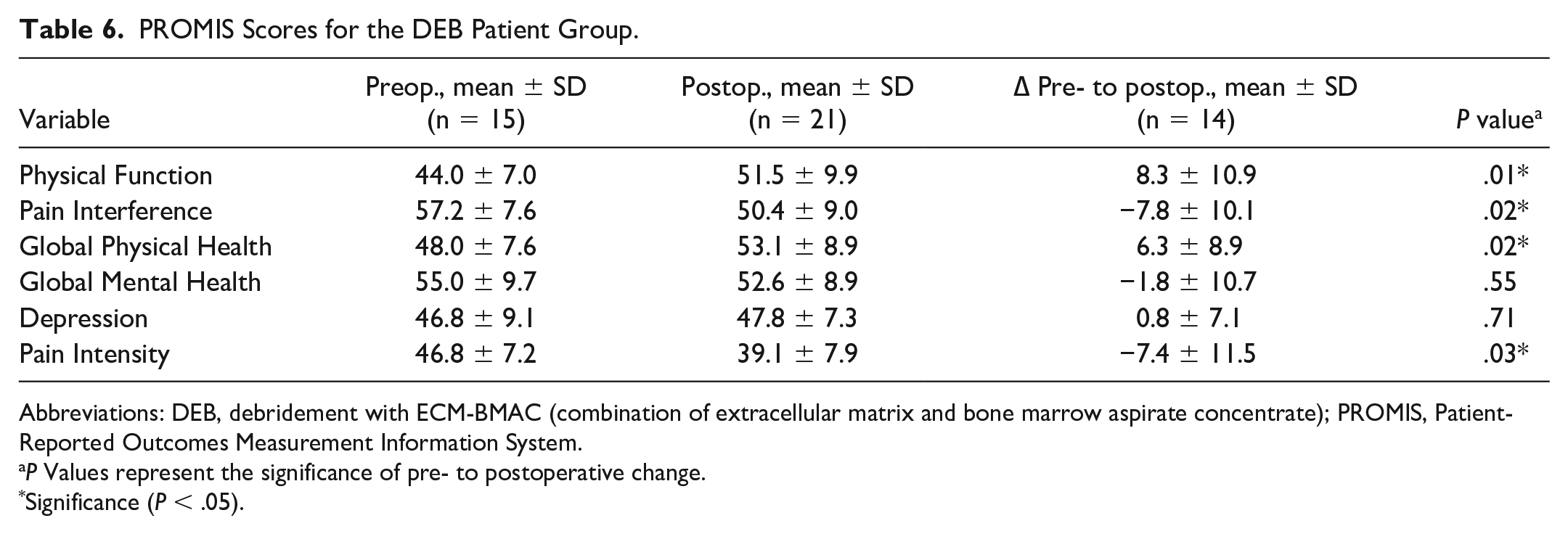
Abbreviations: DEB, debridement with ECM-BMAC (combination of extracellular matrix and bone marrow aspirate concentrate); PROMIS, Patient-Reported Outcomes Measurement Information System.
P Values represent the significance of pre- to postoperative change.
Significance (P < .05).
Five OAT patients reported persistent pain at the knee where the OAT plugs were taken. Three of these patients received a therapeutic injection at the knee joint. One of the patients who required injection began to feel pain only after sustaining an acute twisting injury to the knee. The likelihood of developing knee pain was significantly correlated with BMI greater than 30. The incidence of knee pain in those patients with a BMI >30 was 44%, compared with 6% in patients with a BMI <30 (P = .04). Five of 25 OAT patients underwent hardware removal. No patient required an additional procedure on their knee.
Discussion
This retrospective study aimed to compare OAT with ECM-BMAC and DEB as operative treatments for medium-sized talar lesions by analyzing radiographic and clinical outcome data (Figure 3). OAT was found to result in a higher total MOCART score and a lower rate of cyst, edema, revision, and therapeutic injection compared to DEB. No discernible differences were observed in survey scores between groups, and both groups demonstrated substantial improvement between pre- and postoperative surveys.
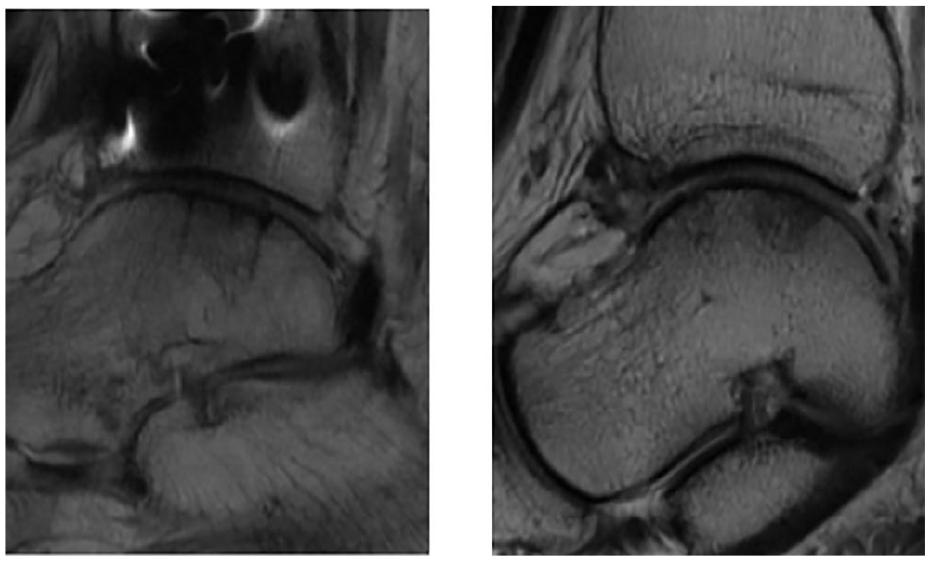
(Right) T1-weighted MRI showing an OAT graft 3 years after surgery. (Left) T1-weighted MRI showing a lesion treated with DEB 3 years after surgery. DEB, debridement with ECM-BMAC (combination of extracellular matrix and bone marrow aspirate concentrate); MRI, magnetic resonance image; OAT, osteochondral autologous transplantation.
The ECM product (BioCartilage; Arthrex Inc) consists of particulated allograft cartilage and acts as scaffolding for the mesenchymal stem cells and growth factors naturally occurring in BMAC. The stem cells and growth factors found in BMAC are thought to improve cartilage repair tissue, though clinical evidence is still in its early stages. 8 ECM-BMAC may improve outcomes when used for the treatment of small talar lesions, and promising results have been published on ECM, though with a lack of control group. 1 In an animal model study, ECM and platelet-rich plasma resulted in improved cartilage repair compared to microfracture alone. 9 A similar matrix plus BMAC technique, known as MAST, has also demonstrated promising outcomes in treating medium to large lesions, but without radiographic data or a control group. 15 There is also a lack of existing literature on the use of ECM-BMAC alongside OAT, though supplementing OAT with BMAC alone seems to lower the rate of postoperative cysts. 20 ECM and BMAC in combination may further improve the results of OAT by providing a structural scaffold, stem cells, and growth factors to encourage thorough cartilage repair around the OAT plug.
Although OAT has previously proven effective for the treatment of larger lesions,11,19,20 prior studies have not determined whether it is more effective than arthroscopic procedures such as microfracture or DEB for medium-sized lesions. The patients included in this study presented with an average lesion size of 117.5 mm2, smaller than the 150 mm2 cutoff above which microfracture tends to result in poor outcomes. 5 Though microfracture has proven fairly effective for smaller lesions,5,6 the relative benefits of OAT seen in this study suggest that OAT may outperform DEB by many metrics in lesions around or slightly smaller than the proposed 150-mm2 cutoff.
Evaluation of postoperative MRI using total MOCART scores indicated that patients who received OAT had significantly better repair quality compared with those treated with DEB. Analysis of individual MOCART categories revealed that OAT MRIs scored significantly higher than DEB MRIs in the Subchondral Lamina and Subchondral Bone MOCART categories. This suggests that the subchondral bone and lamina were found to be intact significantly more often for OAT repairs compared with DEB. OAT patients also had significantly lower rates of postoperative cysts and edema as noted during MRI evaluation. The relatively low prevalence rate of postoperative cysts in OAT patients is of particular interest given that cysts are thought to be one of the most common comorbidities associated with OAT procedures.18,21 Two past studies reported rates of postoperative cysts around 65%, much higher than the rate of 14% observed among OAT patients in the present study.18,21 In our cohort, the low rate of cysts among OAT patients may reflect the use of ECM-BMAC as adjuvant therapy. Used as a mortar to surround the OAT graft, ECM-BMAC may prevent fluid buildup between the graft and surrounding tissue, thus preventing cyst formation. On the whole, the radiographic data indicates that the reparative tissue resulting from OAT treatment was superior to that following DEB, as highlighted by a significantly greater total MOCART score and decreased rates of cyst and edema.
A comparison of rates of failure and recommendation for injection demonstrated that OAT patients experienced failure and underwent postoperative therapeutic injections at a significantly lower rate than DEB patients. No OAT patient underwent or was recommended for subsequent revision, compared with 5 of 27 DEB patients. This difference could in part be due to the fact that a DEB procedure can be revised to OAT if results are not satisfactory, whereas revision procedures for OAT, including revision OAT, osteochondral allograft, ankle fusion, and total ankle replacement are less straightforward. However, the OAT group’s lower rate of injection for pain suggests that fewer OAT patients experienced persistent pain after surgery compared with DEB patients. This was not reflected in clinical outcome scores but may help to explain the OAT group’s lower revision rate. This notion is supported by results from past studies that have demonstrated positive outcomes of OAT, even without the addition of ECM-BMAC.11,19
Analysis of clinical data revealed that both groups demonstrated significant improvement in all PROMIS categories except Global Mental Health and Depression, indicating that all patients tended to experience better physical function and health and less pain after surgery. No significant differences were detected in survey scores between groups. However, some trends in the data were observed. Compared with patients treated with DEB, those treated with OAT improved to a greater degree in the Physical Function, Pain Interference, Global Physical Health, and Pain Intensity PROMIS domains. Similarly, OAT patients reported higher, though not significantly higher, pre- to postoperative change in FAOS scores for Pain, Symptoms, Activities of Daily Living, Sports Activities, and Quality of Life domains. The lack of detectable differences in survey averages could be due to small sample sizes, especially for FAOS surveys. The limited number of complete pre- and postoperative surveys in both groups was the result of a departmental switch in standard preoperative surveys in 2016.
Notably, of the 5 DEB patients who required revision, only 1 had complete FAOS surveys and only 1 had complete PROMIS surveys. This was in part due to the fact that surveys could not be administered retrospectively to these patients once they had undergone revision to OAT, as such scores would not reflect the outcome of the DEB procedure. However, the lack of surveys from this subgroup points to a potential reason for the lack of detectable difference in patient-reported outcome scores between groups. As evidenced by radiographic data, revision rate, and injection rate, OAT patients seemed to experience improved outcomes compared with DEB patients. Along with small sample sizes, the lack of survey data from these patients who failed treatment with DEB and required revision may explain the similar averages observed between groups, as their survey responses could reasonably be expected to be substandard.
The potential for donor site morbidity at the knee is a concern with OAT procedures. At 20%, the rate of knee pain observed in this study falls within the ranges reported in the past, though the current evidence shows substantial variability. At the low end, one study reported a similar rate of 15% symptomatic knees, 16 whereas a smaller study found that as many as 50% of OAT patients experienced knee pain at the harvest site. 21 Historically, several studies have found increased BMI to be associated with knee comorbidities for OAT patients, and the pattern observed in our study corroborates this finding.13,17 Four of 5 patients who experienced knee pain in our study had a BMI >30, and statistical analysis revealed that BMI >30 was significantly correlated with an increased rate of knee pain. Consistent with previously reported results, this suggests that BMI may be an important factor to consider when choosing a treatment method for OLTs. Ultimately, OAT does carry a risk of complications at the knee, an issue that must be balanced alongside the advantages that OAT seems to hold over arthroscopic treatments like DEB as described in this study. Importantly, no patient in the present study required an operative revision procedure to address persistent knee symptoms.
This study includes several limitations, several related to its retrospective nature. Appropriate treatment was decided by a single surgeon, which introduces the potential for selection bias between the 2 groups that would not be present in a prospective, randomized study. Patients receiving OAT had either failed a previous treatment or presented with a deeper or cystic lesion. This means the 2 groups may not have had the same baseline characteristics, although their lesions were all within the defined size range and preoperative survey scores did not reveal any functional differences between groups on average. This limitation should not take away from the observed advantages offered by OAT and may in fact strengthen the case for OAT, as OAT patients presented with more challenging lesions.
Another primary limitation of this study is the small sample size for complete survey data. Because FAOS surveys were administered preoperatively before 2016 and PROMIS was administered after 2016, patient survey data was divided between FAOS and PROMIS. As a result, the lack of significant differences in survey scores may be due to lack of power. We declined to perform a retrospective power analysis as we did not think this would be meaningful. The MRI findings of the study also face limitations. MRIs were collected retrospectively for many patients, rather than at a given time point, leading to large variance in MRI follow-up times. This means that many MRIs were performed less than 2 years after surgery, whereas the MOCART score was initially developed for 2-year follow-up in the knee. 14 Further, there is no established minimal clinically important difference for MOCART scores, so although the groups demonstrated statistically significant differences in these scores, the clinical relevance of these differences is not clear. Finally, longer follow-up times for both survey and radiographic data may be needed to more definitively determine the relative advantages of OAT and DEB.
Conclusion
This study compared OAT augmented with ECM-BMAC and debridement with ECM-BMAC (DEB) as operative interventions to address medium-sized osteochondral lesions of the talus. Greater total MOCART scores indicate higher-quality repair tissue in OAT patients, suggesting that the hyaline knee cartilage introduced with OAT may be structurally superior to the fibrocartilage tissue that forms following DEB. Further, OAT patients experienced significantly lower rates of postoperative cysts and edema. They also had significantly lower failure rates and were less likely to need a therapeutic injection for pain. These results suggest that by introducing native hyaline cartilage, OAT may offer benefits over arthroscopic treatments such as DEB that outweigh the relative cost and risk of comorbidity at the knee when treating medium-sized OLTs.
Supplemental Material
sj-docx-2-fai-10.1177_1071100720980020 – Supplemental material for Comparison of Clinical and Radiographic Outcomes Following Arthroscopic Debridement With Extracellular Matrix Augmentation and Osteochondral Autograft Transplantation for Medium-Size Osteochondral Lesions of the Talus
Supplemental material, sj-docx-2-fai-10.1177_1071100720980020 for Comparison of Clinical and Radiographic Outcomes Following Arthroscopic Debridement With Extracellular Matrix Augmentation and Osteochondral Autograft Transplantation for Medium-Size Osteochondral Lesions of the Talus by Oliver B. Hansen, Stephanie K. Eble, Karan Patel, Taylor N. Cabe, Carolyn Sofka, Jonathan T. Deland and Mark C. Drakos in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_1071100720980020 – Supplemental material for Comparison of Clinical and Radiographic Outcomes Following Arthroscopic Debridement With Extracellular Matrix Augmentation and Osteochondral Autograft Transplantation for Medium-Size Osteochondral Lesions of the Talus
Supplemental material, sj-pdf-1-fai-10.1177_1071100720980020 for Comparison of Clinical and Radiographic Outcomes Following Arthroscopic Debridement With Extracellular Matrix Augmentation and Osteochondral Autograft Transplantation for Medium-Size Osteochondral Lesions of the Talus by Oliver B. Hansen, Stephanie K. Eble, Karan Patel, Taylor N. Cabe, Carolyn Sofka, Jonathan T. Deland and Mark C. Drakos in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jonathan T. Deland, MD, reports personal fees from Arthrex, outside the submitted work. One or more of the authors has received or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.