
Abstract
Background:
Quantifying first ray mobility is crucial to understand aberrant foot biomechanics. A novel device (MAP1st) that can perform measurements of first ray mobility in different weightbearing conditions, foot alignments, and normalization was tested. The reliability of these measurement techniques was assessed in comparison to a handheld ruler considered representative of the common clinical examination.
Methods:
The study included 25 participants (50 feet). Two independent raters performed baseline, test-retest, and remove-replace measurements of first ray mobility with MAP1st and the handheld device. The effects of non-, partial, and full weightbearing in subtalar joint neutral and the resting calcaneal stance position were assessed. Measurement normalization relative to foot size was also investigated. Intra- and interclass correlation coefficients (ICCs) were calculated for each device between the 2 raters. In addition, Bland-Altman plots were constructed to determine if fixed biases or substantial outliers were present.
Results:
Similar intrarater ICC values were found for both devices (≥0.85). However, interrater ICC values were substantially improved by MAP1st compared with the handheld device (0.58 vs 0.06). Bland-Altman plots demonstrated biases of 1.27 mm for the handheld ruler, and 2.88 to 0.05 mm and −1.16 to 0.00 for linear and normalized MAP1st measurements, respectively. Improved reliability was achieved with MAP1st for normalized assessments of first ray mobility while the foot was placed in partial- and full-weightbearing resting calcaneal stance positions.
Conclusion:
MAP1st provided reliable assessments of partial- and full-weightbearing first ray mobility. It should help investigators to explore the potential relationships between first ray function and aberrant foot biomechanics in future research.
Level of Evidence:
Level II, prospective cohort study.
Introduction
First ray mobility is the collective motion between the navicular, medial cuneiform, and first metatarsal. Superior translation of this structure under load is typically used to quantify first ray mobility.4,11,37 Several investigators have hypothesized that first ray hypermobility, which refers to abnormal first ray mobility while the forefoot is bearing weight,8,30 plays a role in various pathologies of the foot.3,4,13,20,27,38 Definitions of first ray hypermobility 24 can vary from 7 to 10 mm based on differences in case definitions and methods of assessment.5,11,20,23,25,33,36 It has been proposed that superior translation ≥8 mm is abnormal.6,21 While numerous clinical methods are used to assess the mobility of different joints, none are performed in structures below the knee. The lack of a standardized and reliable technique for measuring first ray mobility has hindered research into aberrant foot biomechanics imposed by first ray hypermobility.
Clinical examination of first ray mobility is performed by grasping the first metatarsal head between the thumb and forefinger, translating the first ray superiorly and inferiorly. Voellmicke and Deland advocated use of the thumb’s interphalangeal joints as visual reference lines from the plantar aspect of the foot. 37 Glasoe et al 6 found that such manual examinations were unreliable, demonstrating wide variations among experienced clinical staff. Over the past 40 years, a variety of handheld rulers6,19,25,38 and mechanically driven devices have been developed to objectively quantify first ray mobility. Rodgers and Cavanagh 29 built the first-of-its-kind prototype, which was prone to include fat pad compression in the measurement, yielding overestimates of the actual first ray mobility. Klaue et al 21 constructed an ankle-foot orthosis with an integrated calliper to measure first ray translation. Their device was found to be reliable; however, it required a manual force that potentially added variability to the result. Finally, Glasoe et al 7 produced a device that was reliable but bulky and not made commercially available.
To address the limitations of previous methods, a novel electromechanical device named MAP1st was developed to measure first ray mobility. The device applies a controlled load at the plantar surface of the first metatarsal head to measure superior first ray translation. The subject’s foot is unconstrained to enable assessments in user-defined alignments of the foot-ankle complex. In addition, measurements of first ray mobility can be performed in either partial- or full-weightbearing conditions normalized to foot length. The study’s aim was to test the intra- and interrater reliability of MAP1st compared with a commercially available handheld ruler. The handheld device was selected to re-create the clinical examination reported by Voellmicke and Deland 37 with the addition of a ruler to quantify first ray displacement.
Description of MAP1st
MAP1st was implemented as a pair (left and right) (Figure 1). The base was configured from 2 upper and lower aluminum base plates and 4 polycarbonate side panels that housed the electronic components and circuitry. The upper base plate acts as a platform for the foot. The head of the first metatarsal is placed against an aluminum block with a delve for repeatable positioning. A heel cup is used to accommodate the rearfoot, which is adjustable for foot length in the anterior/posterior directions. Located at the medial border of the foot is a ruler used to quantify truncated foot length (TFL). TFL is a measure of foot length taken from the first metatarsal head to heel. This measurement enables normalization of first ray mobility relative to the size of the subject’s foot. The heel is not constrained, allowing user-defined positioning of the foot. At the anterior border of the device is an auto-adjustable toggle clamp (Bessey STC-HH; Bessey Tools, Bietigheim-Bissingen, Germany) to mechanically ground the second metatarsal head. The clamping force is set to 110 N. The toggle clamp includes a quick-release handle, enabling the subject to remove his or her foot at any time during examination. The toggle clamp base is screwed to an aluminum block with a dovetail joint, allowing for medial-lateral translation to accommodate different foot widths.
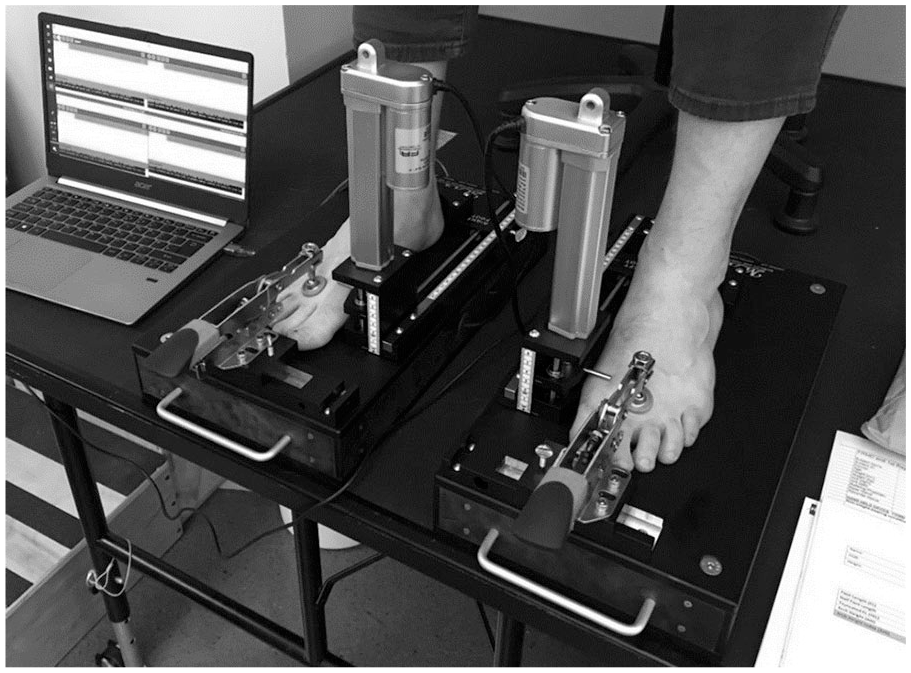
MAP1st (left and right) prepared for testing, with each of the subject’s feet positioned and clamped in the device. The Arduino microcontrollers of each device are plugged into a laptop to interface the custom-written code for upload and testing.
Measurements of first ray mobility are driven by a linear actuator (Premium Linear Actuator; Firgelli Automations, Ferndale, WA). The top of the linear actuator stroke is connected to a load cell beneath the first metatarsal head. This platform, which acts as a plunger, is attached to 2 cylindrical pillars fitted with linear bearings for frictionless superior-inferior translation. The force is controlled by a negative feedback servo using a compression load cell and amplifier (FC22 Compression Load Cell; TE Connectivity, Schaffhausen, Switzerland). An Arduino Uno microcontroller (Arduino Uno; Arduino, Somerville, MA), powered by 12 V DC, implements the force servo required for measurement of first ray mobility. Recharging is enabled by an AC-DC converter. Powering the circuitry and recharging are mutually exclusive by use of a double pole–double throw switch.
Methods
Subject Recruitment
The study included 25 subjects (N = 50 feet). The project research coordinator ensured that each participant gave consent. Potential subjects were recruited from any willing individual who met the study inclusion/exclusion criteria in Table 1. Participant characteristics are shown in Table 2. All procedures were approved by the Hospital for Special Surgery (HSS) Institutional Review Board. Testing was performed at the Leon Root, MD, Motion Analysis Laboratory at HSS, where each subject gave consent before testing.
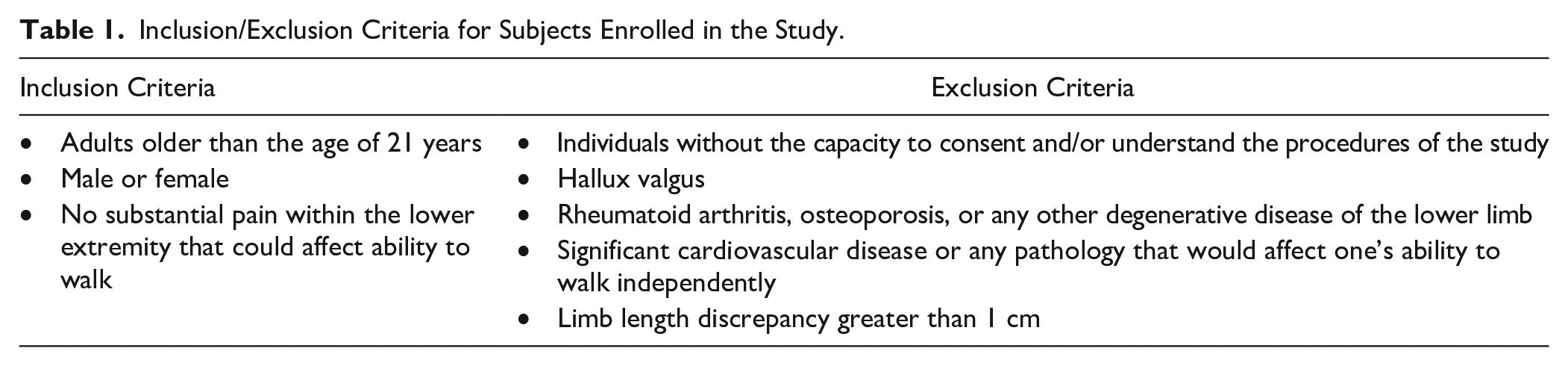
Inclusion/Exclusion Criteria for Subjects Enrolled in the Study.
Participant Characteristics.
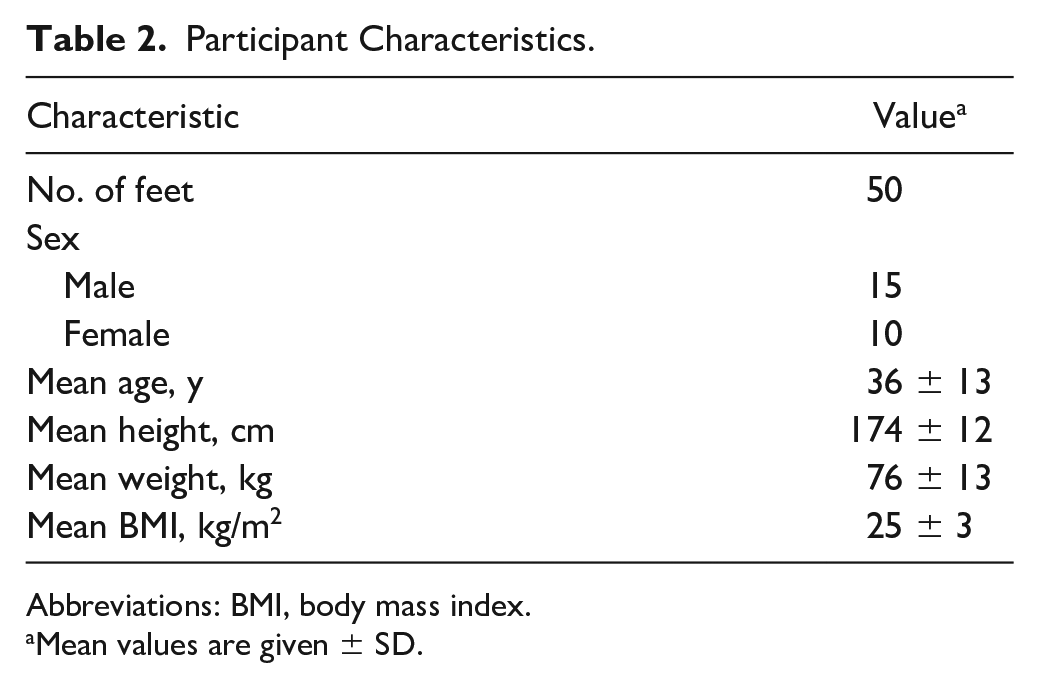
Abbreviations: BMI, body mass index.
Mean values are given ± SD.
Measures of First Ray Mobility
Prior to first ray mobility measurements with MAP1st, 10 successive 25-N loading cycles were used to control the soft tissue recent strain history. 39 The procedure for recent strain history control spanned approximately 60 seconds. First ray mobility measurements were taken from the dorsal aspect of the first metatarsal head. To quantify first ray mobility, a vertical steel rod was positioned at the dorsal aspect of the first metatarsal head (Figure 1). The measurement of first ray mobility was defined as the linear displacement of the first metatarsal head, on a graticule (Figure 2A), after a 50-N load. Glasoe et al 12 previously found that 50 N may fully translate the first metatarsal without causing discomfort to the test subject. Furthermore, they found that mobility measurements were only valid compared with radiograph-based measurements when the load applied to the first ray, using the Glasoe device, did not exceed 55 N. Two methods of measurement were performed with MAP1st: (1) linear displacement of the first ray (FRM; given in mm) and (2) linear displacement normalized by TFL to provide a first ray mobility index (FRMI) for measurements relative to foot size, using the following equation:

First ray mobility, using MAP1st, was measured while the subjects were seated (ie, lower extremity positioned in 90 degrees of hip and knee flexion) and standing (ie, hip-knee-ankle in 0-degree alignment) (Figure 2A). The ankle was placed in a neutral alignment for both partial- and full-weightbearing measurements. 14 The influence of foot placement was also assessed by taking measurements in subtalar joint neutral (STJN) and the resting calcaneal stance position (RCSP).30-32 STJN may be defined as an alignment of the foot such that it is neither pronated nor supinated. RCSP may be defined as a relaxed position of the foot with the medial longitudinal arch in its natural weightbearing alignment. To perform the measurements of first ray mobility, an independent recorder viewed MAP1st’s graticule with their aiming eye, in a perpendicular orientation, to avoid parallax error and recorded dorsal displacement.
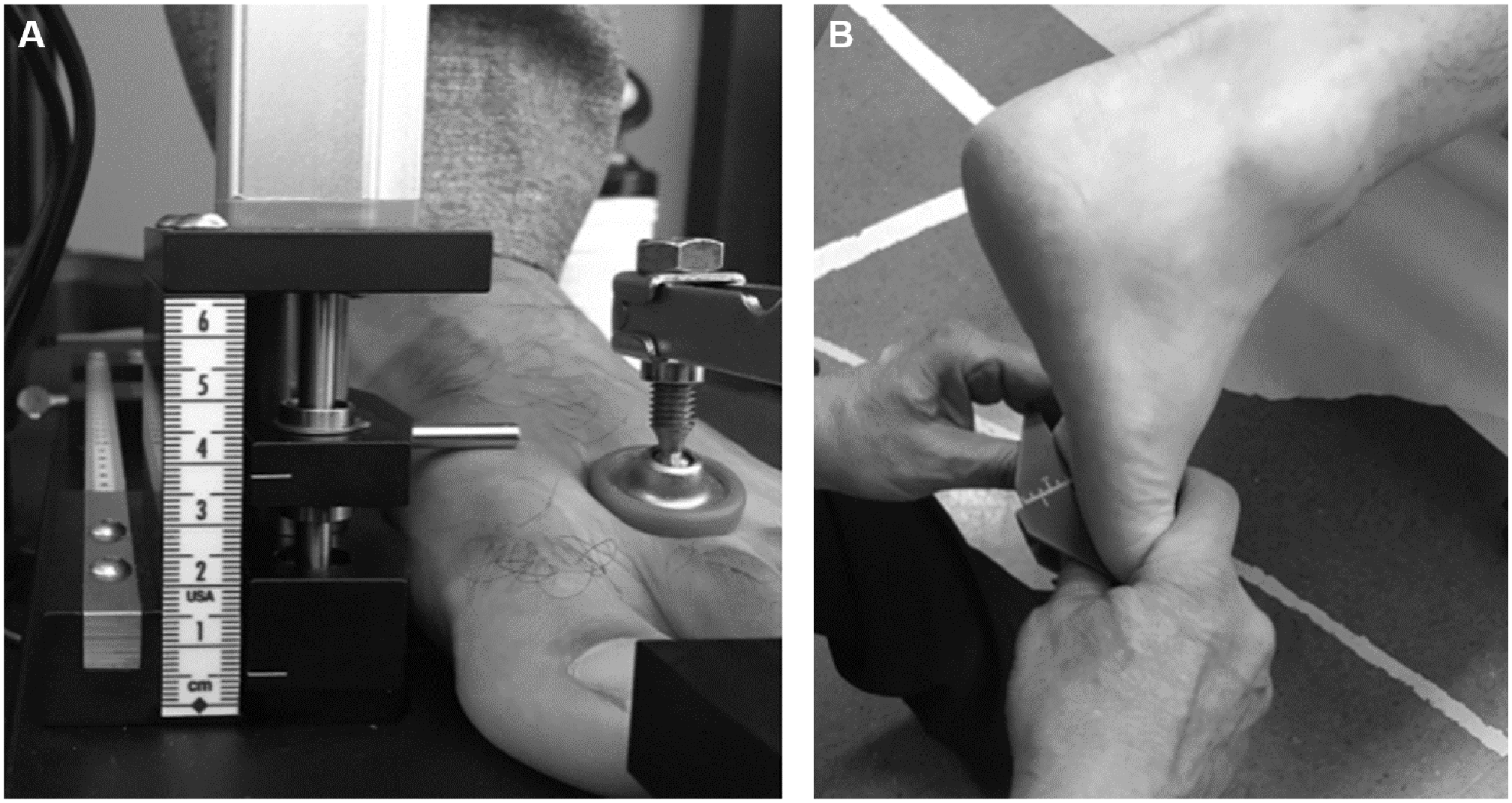
(A) MAP1st measuring first ray mobility while the subject is seated (partial weightbearing) and standing (weightbearing). (B) The handheld ruler measuring first ray mobility from the plantar aspect of the first metatarsal head while the subject is prone.
Measurements of first ray mobility using the handheld ruler were taken from the plantar aspect of the first metatarsal head, while the subjects were prone, on a flat treatment table. Their hip-knee-ankle was in 0-degree alignment (Figure 2B). The ankle was neutrally positioned, which has been shown to produce more reliable measures of first ray mobility. 14 The subject’s feet were placed in STJN during assessment with the handheld device. One side of the device was placed beneath the second metatarsal head and the other side beneath the head of the first metatarsal, adjacent to the opposing surface. Superior translation (mm) was then measured by applying a manual force to the first metatarsal head, viewing the changed position of the ruler with respect to the second metatarsal head.
Statistics
Two independent raters (rater 1, physical therapist, R.T.; rater 2, biomedical engineer, H.J.H.) performed the measurements (baseline [first measurement], test-retest [measurement repeated twice], and remove-replace [initial measurement taken and repeated after the rater had removed and replaced the foot in the device]), permitting estimation of intra- and interrater reliability for the test-retest and remove-replace assessments. Raters with both clinical and scientific backgrounds were selected to demonstrate the application of MAP1st in different research and clinical settings. Descriptive statistics were used to report means, standard deviations (SDs), and standard errors of measurement (SEMs). Three trials of first ray mobility were collected for each foot (right and left). Intra- and interclass correlation coefficients (ICCs) for test-retest and remove-replace reliability were computed for each rater in SPSS (version 26; IBM Corp, Armonk, NY). This reliability study employed 2 raters, who were considered to be representative of the pool of all raters. Every subject was evaluated by each rater and, hence, an ICC (2, 1) model was employed as described by Shrout and Fleiss. 35 All ICC parameter calculations were performed using the method of absolute agreement. Furthermore, 95% confidence intervals (CIs) for each ICC estimate were computed, as well as the SEM. Values of ICC reliability were classified as poor (<0.5), moderate (0.5-0.75), good (0.75-0.9), and excellent (>0.9). Additionally, Bland-Altman (B&A) plots were constructed to determine if fixed biases or substantial outliers were present between the trials of each rater. This method compared the differences and 95% CI (estimated as 1.96 times the SD) for the interrater measurements of mobility. 1 The 95% CI, which B&A termed the “limits of agreement,” assumes that the individual paired differences of the 2 raters are normally distributed. Best-fit regression lines were created for plots of FRM vs FRMI to understand the relationship between each parameter.
Results
MAP1st
Excellent intrarater ICC values (≥0.93) were obtained for test-retest conditions for FRM. Remove-replace conditions demonstrated lower intrarater ICC values. The interrater reliability for the RCSP weightbearing condition yielded an ICC of 0.52, which was greater than the handheld device (Table 3). Sample B&A plots for interrater reliability exhibited biases of 2.88 mm for partial-weightbearing STJN, 0.05 mm for weightbearing STJN, 0.28 mm for partial-weightbearing RCSP, and −0.68 mm for weightbearing RCSP (Figure 3A-D). The limits of agreement were typically inclusive of 95% of the mean differences for all conditions.
Mean, SD, SEM, and Intra- and Interrater Reliability Calculated Using FRM Measurements (linear displacement of the first ray).
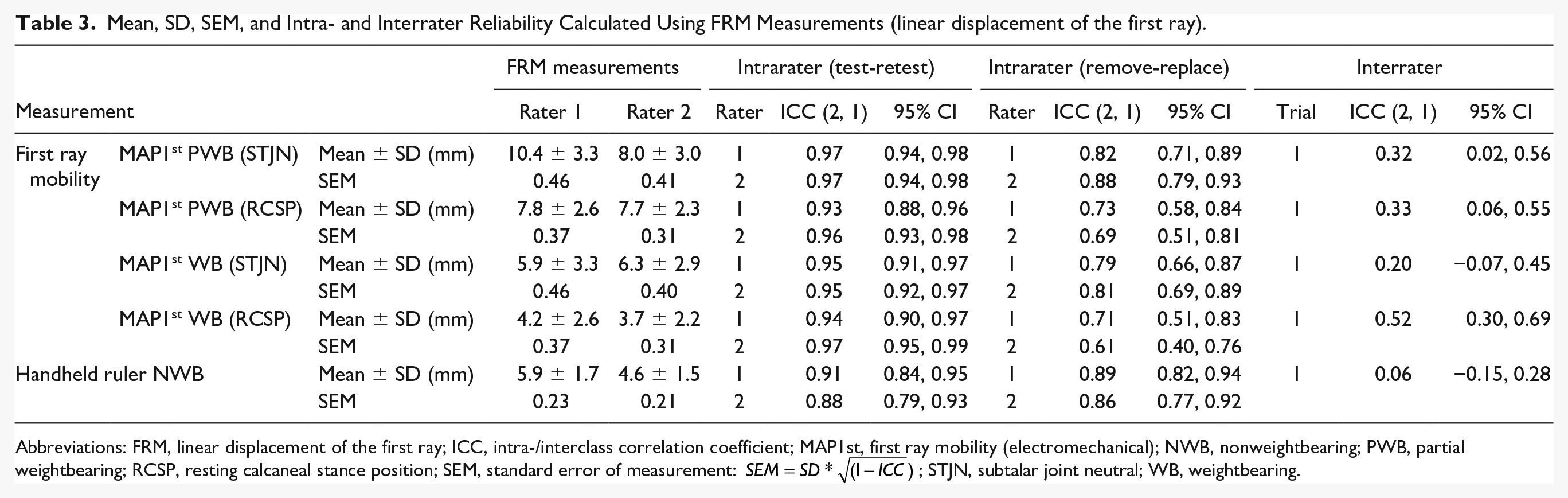
Abbreviations: FRM, linear displacement of the first ray; ICC, intra-/interclass correlation coefficient; MAP 1st, first ray mobility (electromechanical); NWB, nonweightbearing; PWB, partial weightbearing; RCSP, resting calcaneal stance position; SEM, standard error of measurement:
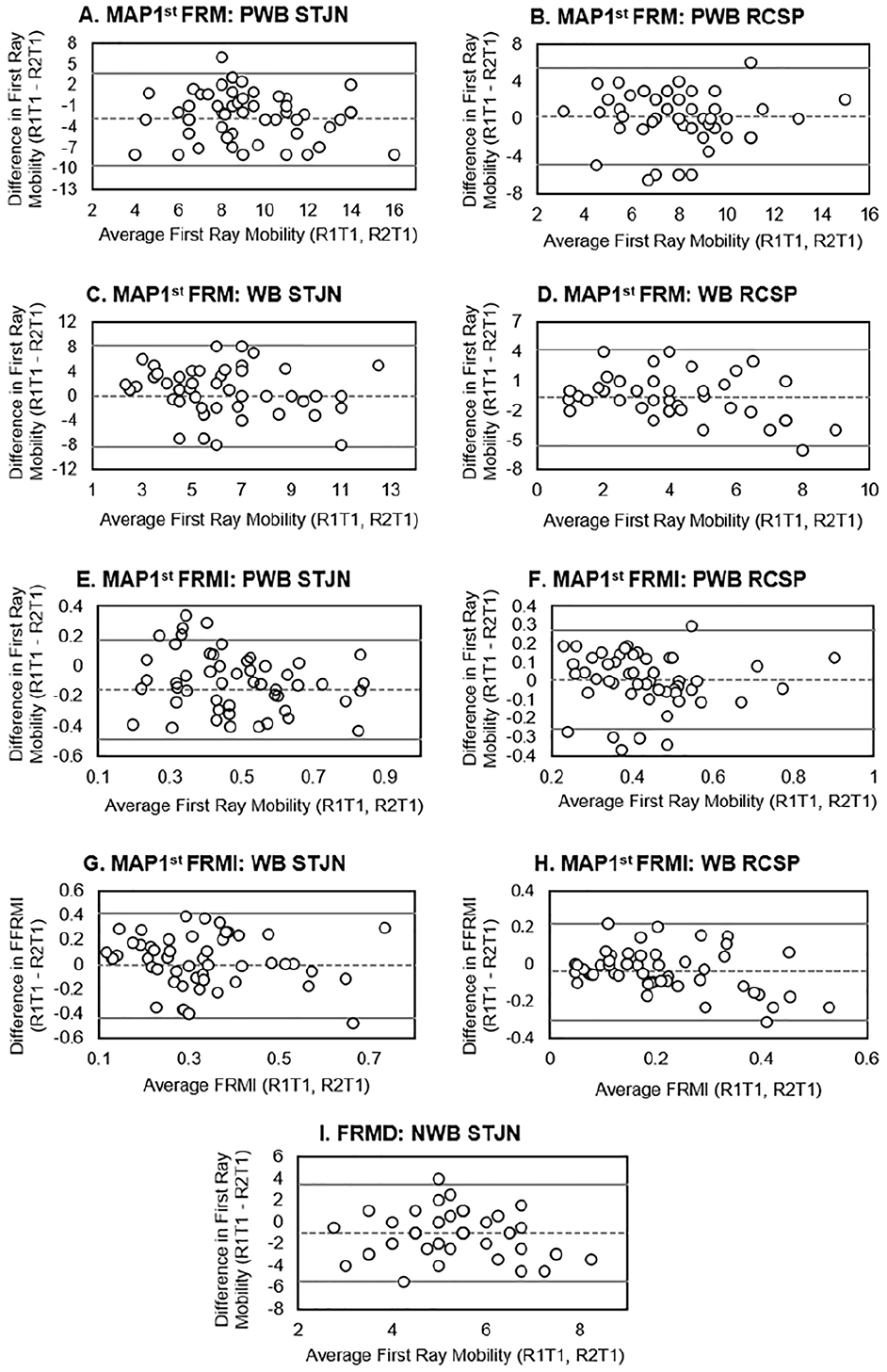
Bland-Altman analysis plots of the interrater reliability of first ray mobility measurements made using: (A-D) MAP1st FRM, (E-H) MAP1st FRMI, and (I) handheld ruler. The central dashed line represents the rater bias. The upper and lower solid lines represent the 95% confidence interval for the limits of agreement. FRM, linear displacement of the first ray; FRMI, first ray mobility index; NWB, nonweightbearing; PWB, partial weightbearing; RCSP, resting calcaneal stance position; STJN, subtalar joint neutral; WB, weightbearing.
Good to excellent intrarater ICC values (≥0.85) were obtained for test-retest conditions of FRMI. Remove-replace reliability demonstrated lower intrarater ICCs for all but one condition. The interrater reliability for the RCSP partial-weightbearing and weightbearing conditions yielded ICC values of 0.58 and 0.57, respectively (Table 4). Sample B&A plots for interrater reliability exhibited biases of −1.16 for partial-weightbearing STJN, 0.01 for weightbearing STJN, 0.00 for partial-weightbearing RCSP, and 0.04 for weightbearing RCSP (Figure 3E-H). Similar to FRM measurements, the limits of agreement were typically inclusive of 95% CI of the mean differences for all conditions.
Means, SD, SEM, and Intra- and Interrater Reliability Using FRMI Measurements (Normalized by Truncated Foot Length).
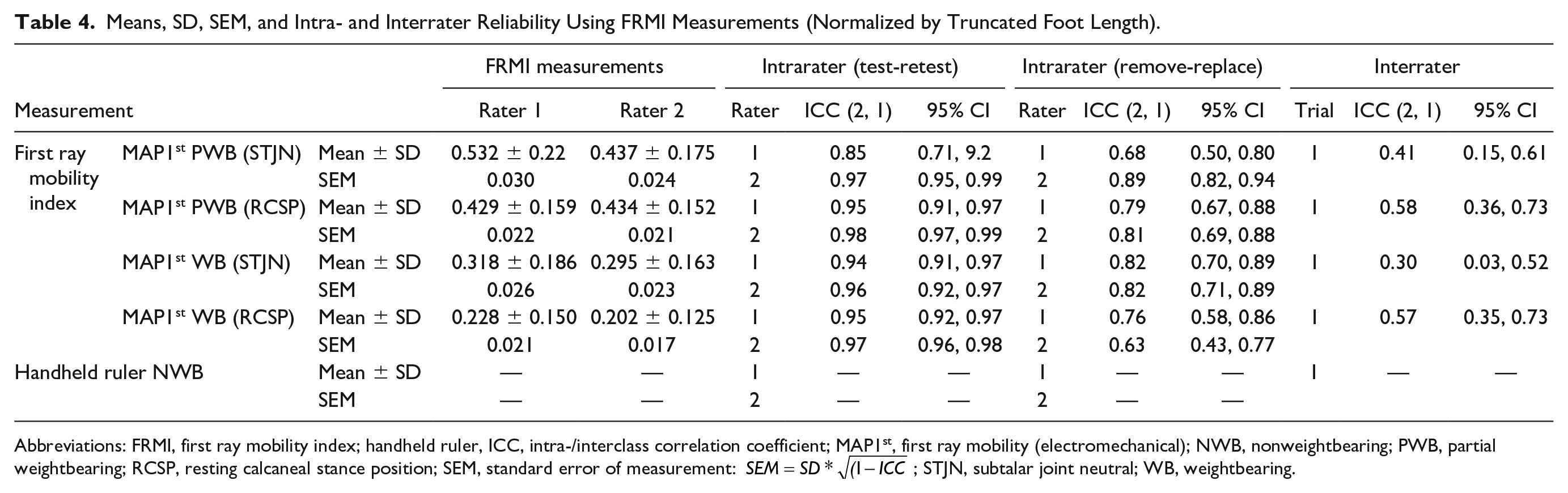
Abbreviations: FRMI, first ray mobility index; handheld ruler, ICC, intra-/interclass correlation coefficient; MAP1st, first ray mobility (electromechanical); NWB, nonweightbearing; PWB, partial weightbearing; RCSP, resting calcaneal stance position; SEM, standard error of measurement:
Linear regression of partial-weightbearing RCSP measurements for FRM vs FRMI with MAP1st demonstrated an R 2 of 0.95 for rater 1 and R 2 of 0.93 for rater 2 (Figure 4A and B). Full-weightbearing measurements of FRM versus FRMI exhibited an R 2 of 0.98 for both raters (Figure 4C and D).
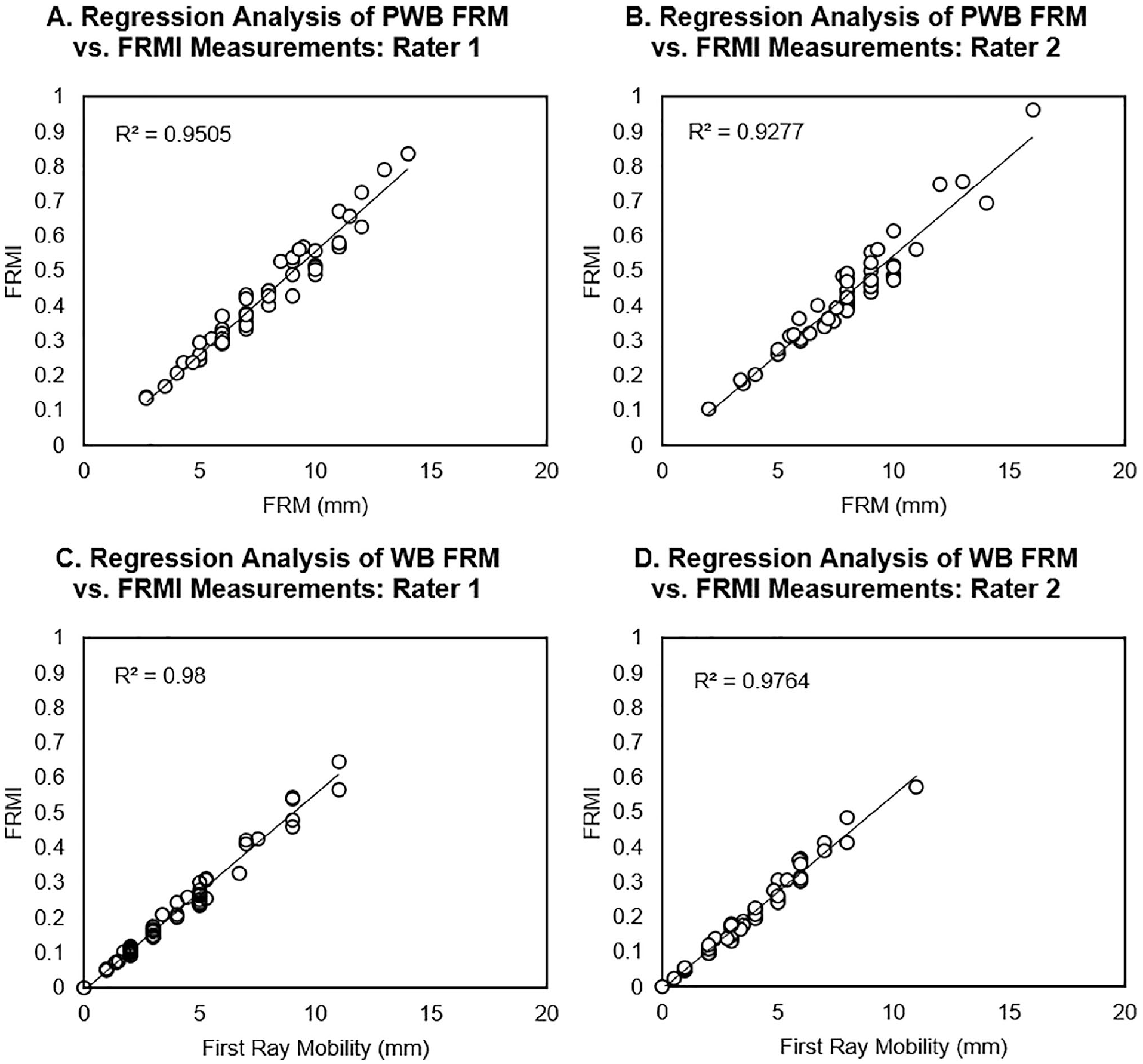
Regression analyses of FRM versus FRMI measurements of first ray mobility for (A) rater 1 partial weightbearing, (B) rater 2 partial weightbearing, (C) rater 1 weightbearing, and (D) rater 2 weightbearing. FRM, linear displacement of the first ray; FRMI, first ray mobility index; PWB, partial weightbearing; WB, weightbearing.
Handheld Ruler
Despite good to excellent intrarater ICC values for test-retest (≥0.88) and remove-replace (≥0.86), the interrater reliability was poor at 0.06, when using the handheld ruler (Table 3). The B&A plots for interrater reliability showed that the handheld ruler presented a bias of −1.26 mm with the limits of agreement spanning −5.54 mm to 3.49 mm (Figure 3I).
Discussion
Several studies have presented novel mechanical6,9,21 and handheld19,25,38 devices to measure first ray mobility. They reported measurements in non- or partial weightbearing that did not account for the effect of foot size. Grebing and Coughlin 14 studied the influence of ankle position on the reliability of first ray mobility measurements, but the effect of foot position has not been examined in the literature. The present research investigated partial- and full-weightbearing STJN and RCSP orientations of the foot, as well as measurement normalization to foot length. Future research or clinical use with the MAP1st may be conducted in partial or full weightbearing while the foot is in RCSP. Although measurements of FRMI presented superior reliability to FRM, linear regression of these parameters demonstrated a strong relationship that suggested foot length had no effect on first ray mobility. Despite good to excellent intrarater reliability of the handheld device, poor interrater reliability was obtained. Consistent with previous research,6,9 this handheld device and the common clinical examination that it represented should not be applied in clinical care or research, where multiple individuals may compare or combine their measurements.
Of the mechanical devices used to quantify first ray mobility, the most widely published were designed by Klaue et al 21 and Glasoe et al 12 in the 1990s. Though different in design, neither device performed measurements in full weightbearing (Table 5). The capability of MAP1st to reliably quantify partial- and full-weightbearing first ray mobility presents an advantage over these predicate devices. Roukis et al 33 demonstrated an interaction between increased translational mobility of the first ray and decreased rotational first metatarsophalangeal (MTP) joint flexibility. Their findings indicated that, in weightbearing, first ray hypermobility may increase passive tension in the plantar fascia, placing the “Windlass mechanism” at the end of its available motion and limiting first MTP joint dorsiflexion. Several investigators have postulated that over time, repetitive overloading at the joint’s dorsal articular surfaces may occur, leading to onset and development of hallux rigidus.13,16,33 Future weightbearing measurements may better represent underlying aberrant structural and functional characteristics of the first ray, which may not be fully appreciated when the foot is unloaded.
Design Feature Comparison of the Klaue Device, Glasoe Device, and MAP1st. a
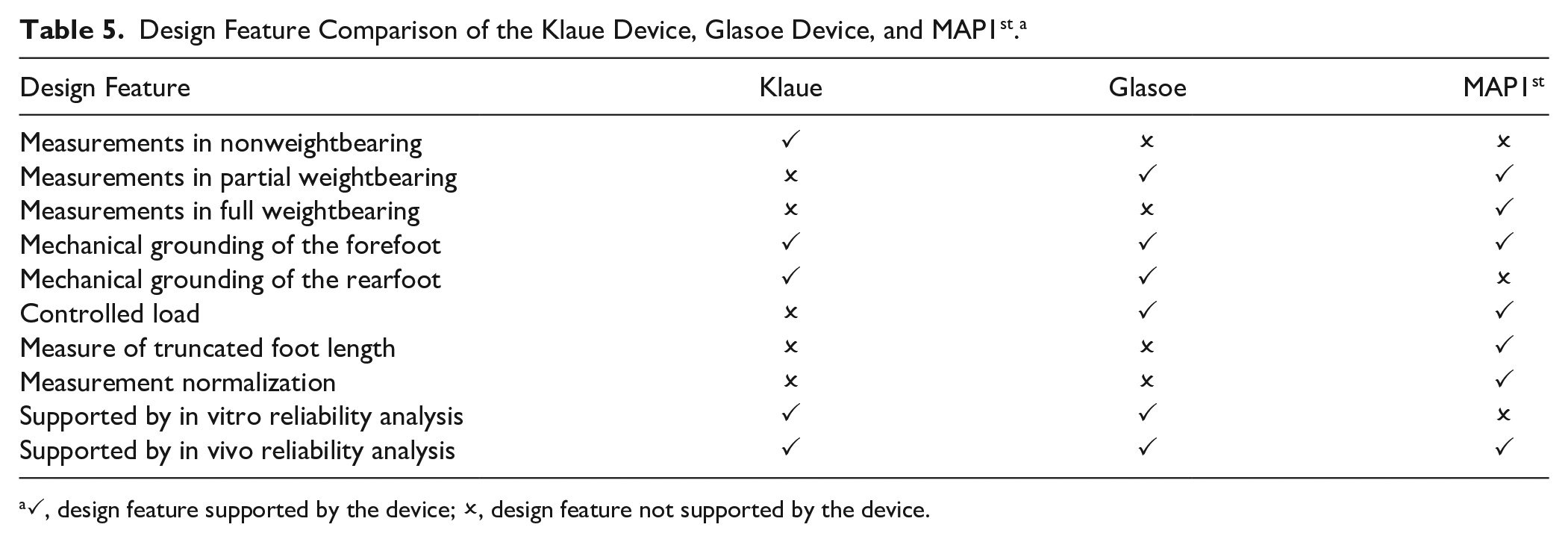
✓, design feature supported by the device; ×, design feature not supported by the device.
Prior assessments of first ray mobility were conducted with no reported foot position,19,23,29,38 in STJN25,34 or mechanically constrained by an orthotic.7,21 Root et al30-32 advocated the use of STJN to characterize normal and abnormal foot function. Shirk et al 34 suggested that STJN combined with a neutral ankle alignment 14 was necessary to reliably measure first ray mobility. In contrast, the present study found that an STJN position diminished interrater reliability. Good to excellent intra- and interrater ICCs ≥0.85 and ~0.58, respectively, were achieved for RCSP measurements. The reliability of RCSP measurements demonstrated equivalent reliability to the Glasoe et al9,12 and Klaue et al devices. Furthermore, B&A plots demonstrated lower biases in RCSP compared with STJN for both FRMI (0.02 ± 0.03 vs 0.59 ± 0.81) and FRM (0.5 ± 0.3 mm vs 1.5 ± 2.0 mm). Feet are often categorized into 3 general structures: planus (a low arch with an everted calcaneus and/or varus forefoot); rectus (a moderate arch with the posterior surface of the calcaneus close to perpendicular with the ground); and cavus (a high arch with inverted calcaneus and/or valgus forefoot). 22 An STJN position may artificially reduce or increase first ray mobility measurements in planus and cavus feet, respectively, by forcing an inversion or eversion of the foot. As such, neutralizing the foot’s arch alignment may affect the flexor and extensor muscle-tendon systems and passive tension in the plantar fascia, which are fundamental in foot type–specific kinematics and muscular activity.2,26 Therefore, placement of the foot in RCSP may not only promote greater reliability but also elucidate a potential interaction between foot type and first ray mobility not appreciated in STJN. Specifically, greater prevalence of first ray hypermobility has been theorized in planus individuals, leading to greater odds of foot injuries, 18 increased first MTP joint flexibility, 28 and higher plantar loading of the medial forefoot. 15
Many investigations of first ray mobility have presented linear translational measurements (mm) that did not account for foot size.6,7,9,10,12,21,25,36 In the present study, normalization of first ray mobility by foot size, to provide a FRMI, demonstrated strong agreement with the traditional linear displacement of FRM. This finding indicated that foot size had no effect on first ray mobility. While measurements of FRMI exhibited greater ICC reliability, FRM measurements presented a SEM of 0.1 mm, demonstrating near-identical outcomes between raters. Furthermore, B&A analyses found a between-rater fixed bias of 0.5 mm. Based on these findings, FRM may be given in conjunction with FRMI for comparison with previous research. Prior work from Tavara-Vidalon et al 36 and Jones et al 17 reported mean FRM values of 6.5 mm and 7.4 mm with radiographic measurements. In comparison to these data, the mean FRM obtained with MAP1st was approximately ±1 mm in RCSP and ±3 mm in STJN, further supporting RCSP assessments in future research as well as providing indirect validation of MAP1st. Direct validation testing, with radiographic data, should be conducted to fully understand the device accuracy.
Measurements using the handheld ruler can be considered analogous to the clinical examination. 37 Poor interrater ICC reliability of this method (0.06) suggests that, despite its simplicity, it is not an accurate method for measurements between raters. This finding was supported by Glasoe et al, 6 who observed significant variability in the manual measurements made by 3 clinicians with different levels of clinical experience. Fat pad compression from plantar measurements has been shown to underestimate first ray mobility. 7 Several handheld devices that performed dorsal measures have been studied in the literature.6,19,23,25,38 Glasoe et al 6 assessed the interrater reliability of dorsal mobility measurements using a handheld ruler advocated by Lee et al. 23 Their findings demonstrated similar interrater ICC reliability (0.05) 9 to the handheld device used in the present work. In contrast, a later study of the same device found improved reliability comparable to that of the mechanical system developed by Klaue et al. 21 More recently, a novel handheld device, which accounted for the arc of first ray dorsal motion, demonstrated excellent intra- and interrater ICC reliabilities of 0.89 and 0.93. 25 While the handheld method used in the present research was not performed at the dorsal aspect of the foot, the study aim was to re-create the clinical examination reported by Voellmicke and Deland. 37 The addition of the handheld ruler enabled first ray mobility to be quantified. Neither the Glasoe, Klaue, or handheld devices discussed are widely used in a clinical setting. While these devices represent the current state of the art, they could not provide comparison as a method that represented the most common technique. The clinical examination, which is the most widely used technique to date, may not provide an objective, quantifiable method of studying first ray mobility in large, population-based research where multiple examiners are involved. The same concern would be reasonable in a group practice of multiple clinicians.
There are several potential clinical applications of MAP1st. The device may be used to evaluate the efficacy of conservative treatments, including the prescription of orthotics and first ray stabilizing surgeries such as bunion correction, Lapidus arthrodesis, or distal crescentic osteotomy of the first metatarsal. To assess orthotics, arthrodesis, and osteotomy, measurements of first ray mobility may be taken before and after intervention to quantify the efficacy of these treatment modalities in stabilizing the medial forefoot. The potential to improve assessment procedures for the weightbearing mobility and elevation of the first ray in pathologic individuals may help to optimize contemporary treatment methods. Furthermore, MAP1st may be used to discriminate between the first ray mobility of planus, rectus, and cavus foot types, to identify structural and functional differences related to common conditions including flatfoot deformity, hallux valgus, and hallux rigidus.
Our study is not without limitations. Given the viscoelastic nature of soft tissue, it was possible that a time-dependent stretch of the plantar fascia and ligaments could have occurred between trials. This phenomenon is difficult to measure and may have differed between subjects. In order to minimize this potential effect, each subject began testing with 10 translational excitations to control for the recent strain history. Furthermore, to measure FRM with MAP1st, it was necessary to record the height of the first metatarsal head, at baseline, before load deformation testing. In the current protocol, first metatarsal head height was recorded just once for each subject at baseline. However, first metatarsal head height was not recorded during remove-replace. It was possible that the initial metatarsal head height changed upon replacing the foot into the device for the final trial. Therefore, the remove-replace reliability of MAP1st may have been improved had a new baseline for metatarsal head height been recorded. Finally, direct validity of MAP1st compared with radiographic measures from the same subject was not investigated in the current work.
Conclusion
A novel device that measures first ray mobility was developed to address the limitations of current methods. Equivalent reliability was found compared with predicate mechanical devices, in addition to greater reliability than the standard clinical examination. Measurements may be performed in partial- and full-weightbearing RCSP, which may facilitate investigation of aberrant foot mechanics not fully appreciated in nonweightbearing or STJN. Future research or clinical use of MAP1st should abide by recording measurements in RCSP that are normalized for FRMI. However, the measurements of FRM may be given in conjunction with normalization to provide comparison with previous research. In summary, the present method may provide reliable assessments of first ray mobility and be used to elucidate theoretical relationships between first ray function and aberrant biomechanics as a pathway to common orthopaedic disorders of the foot.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007211020345 – Supplemental material for Comparative Reliability of a Novel Electromechanical Device and Handheld Ruler for Measuring First Ray Mobility
Supplemental material, sj-pdf-1-fai-10.1177_10711007211020345 for Comparative Reliability of a Novel Electromechanical Device and Handheld Ruler for Measuring First Ray Mobility by Oliver J. Morgan, Rajshree Hillstrom, Robert Turner, Jonathan Day, Ibadet Thaqi, Kristin Caolo, Jinsup Song, Roland Russell, Scott Ellis, Jonathan T. Deland and Howard J. Hillstrom in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.