
Abstract
Background:
Navicular stress fractures are becoming increasingly more common. There is no universal consensus on treatment. We provide an algorithm that we feel will be useful in determining treatment.
Methods:
A retrospective study was performed on all patients having operative treatment of navicular stress fractures during a 10-year period. Acute fractures were treated with open reduction internal fixation. Chronic fractures greater than 3 months were treated with open reduction and internal fixation (ORIF) and iliac crest bone grafting. Chronic fractures with evidence of sclerosis, avascular changes, or those who failed previous surgery were treated with ORIF, iliac crest bone grafting, as well as vascular bone grafting. Patients’ pain scores were recorded and a return-to-sports scale was used. Radiographic union was compared among the 3 groups using computed tomographic (CT) scans or radiographs.
Results:
Forty-three patients were identified. Fifteen received ORIF alone, 12 were treated with ORIF and bone graft, and 16 had ORIF with vascularized bone grafting. No difference was found among the median age of the 3 groups. In terms of radiographic healing, 3 patients in the ORIF group received radiographs alone. All other patients had follow-up CT scans. ORIF alone group had 80% union, ORIF with bone graft had 75% union, and ORIF with vascularized bone grafting had 100% union. Return to sports did not show any difference among the 3 groups.
Conclusion:
The algorithm dividing navicular stress fractures into 3 distinct groups with different operative techniques helped us address these difficult cases. Vascularized bone grafting certainly appeared to be beneficial for the more difficult cases.
Level of Evidence:
Level IV, case series.
Keywords
Introduction
Navicular stress fractures account for up to one-third of all foot and ankle stress fractures.1,3,8,9 Towne et al 17 first described navicular stress fractures in 1970. Since that time, the reported incidence has risen from 0.7% to 2.4%7,12 in the 1980s to 14% to 35%1,3,9 of all foot and ankle stress fractures. This has occurred because of changes in shoewear, increased participation in sports, increased athletic training and stresses, 13 heightened awareness, and better earlier recognition with enhanced diagnostic aids. 6
Despite increased awareness and incidence of navicular stress fractures, optimal management remains controversial. Factors thought to influence navicular fracture treatment are symptoms onset, time to diagnosis, patient age, patient activity level, and fracture characteristics. Considerations for fracture characteristics include (1) displaced vs nondisplaced, (2) complete vs partial, (3) comminuted vs simple, and (4) adjacent bony cystic and/or sclerotic changes.
Reported treatment options for navicular fractures are bracing during activity, activity restriction,2,14 weightbearing in a controlled ankle motion (CAM) boot or below-knee cast, 10 strict nonweightbearing in a below-knee cast, percutaneous fixation, and open reduction and internal fixation (ORIF).5,11 Torg et al, 16 in a multi-institutional study, compared outcomes of various weightbearing treatment protocols for management of 21 navicular fractures in 19 patients. The total cohort of 19 patients was diagnosed at an average of 7.5 months after onset of symptoms. The investigators diagnosed navicular fractures via anterior-posterior tomograms in 17 patients and via radionuclides in 14 patients. Final results were available only in 15 patients with 17 fractures. The authors reported that the 10 patients (47.6%) treated for 6-8 weeks in nonweightbearing casts had a 100% healing rate. Nine patients (42.8%) treated in walking casts could not resume sports because of pain. Similarly, all 3 patients treated operatively with ORIF healed (100%). Four patients (19%), including 2 professional basketball players, were deemed “disabled” for 16-42 months after treatment because of delayed union and refracture. The investigators did not use follow-up tomograms or computed tomographic (CT) scans to confirm union on all patients but rather radiographs. Burne et al 4 reported on 11 navicular stress fractures and 9 navicular stress reactions treated at their university’s sports medicine center between 1996 and 2002. Only 2 of the navicular stress fracture patients received the “recommended literature treatment of 6 weeks nonweightbearing in a cast”; 5 others were nonweightbearing for same length of time. Of these 11 patients, only 6 returned to sports at their previous level. Only 3 patients with navicular stress fractures regained normal imaging. Of 9 patients with navicular stress reactions, 7 developed clinical and radiographic features of navicular stress fractures, but 6 of 9 were able to successfully return to sports. Burne’s conclusion was that contemporary management of navicular stress fracture differs from the recommended 6 weeks’ nonweightbearing in the literature. Nonweightbearing immobilization prevented almost half of his participants from returning to sports at their previous level. Interestingly, imaging characteristics on CT scan did not correlate with clinical assessment of patients at long-term follow-up. Continued navicular symptoms and persistent radiographic findings despite appropriate conservative management typically prompt operative fixation.
The paucity of current literature and lack of high-quality evidence fail to guide the indications for optimal operative management for navicular stress fractures. For example, no evidence exists to dictate if adding bone graft to ORIF for navicular fractures leads to improved healing rates and outcomes. The aim of our study is to share our institution’s comprehensive experience with the operative management of navicular stress fractures. We hypothesized that the senior author’s treatment algorithm (Figure 1) would lead to equivalent results in pain or return to activity and radiographic healing for simple and complex navicular stress fractures.
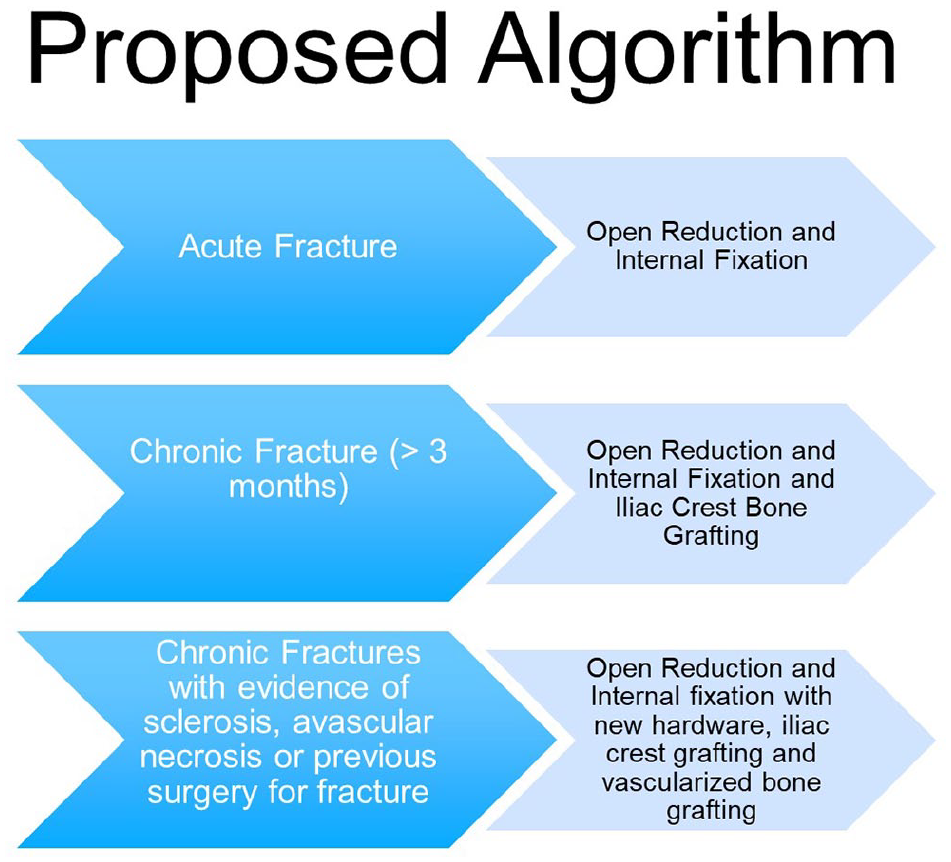
Treatment algorithm proposed by the senior author.
Our anticipation is that our experience will provide greater clarity in surgeons’ understanding of operative indications, operative technique, postoperative protocol, and patient education in the operative treatment of navicular stress fractures.
Methods
After institutional IRB approval, we performed a retrospective chart review on patients treated between 1996 and 2015 to determine the incidence and outcomes of patients undergoing operative treatment for navicular stress fractures. The inclusion criteria were skeletal maturity, complete chart records with history and physical examination, and follow-up radiographs. Outcomes collected in the chart reviews included pain scores, radiographic appearance, reoperations, complications, and the ability to return to sport. 14
Throughout the study time, our institution followed a standardized operative treatment of navicular fractures (Figure 1). Acute fractures were treated with open reduction and internal fixation (ORIF). Nonoperatively treated fractures with delayed union (>3 months) were treated with ORIF and iliac crest bone grafting. Nonunions, that is, chronic fractures without progression toward healing and those failing previous surgery, were treated with ORIF, iliac crest bone grafting, and vascularized bone grafting.
Patients’ pain scores recorded in clinic and at the level of return to sport were compared among the 3 groups. We used a pain / return to sport scale as follows: no pain / patient returns to same prior level of activity without pain; mild pain / patient returns to lower level of activity than before stress fracture with mild resolving pain; and moderate pain / patient could not return to any level of play and had pain with activity.
Radiographic union was compared among the 3 groups using CT scan or radiography. Radiographic union was defined by one of the following: report from the radiologist or treating surgeon of trabeculation across the old fracture site, unable to view the old fracture site, or statement that the fracture had healed.
Distribution and frequencies for categorical variables are presented as counts and percentages for nonmissing data, and continuous variables are presented as means, standard deviations, medians, the interquartile 25th (Q1) and 75th (Q3) percentiles, and the range, dependent on the variable distribution. Differences across operative groups (ORIF alone, ORIF with bone graft, and ORIF with vascularized bone graft) for continuous variables were evaluated using the Kruskal-Wallis test. For categorical variables, differences across groups were measured using either the chi-square test or Fisher exact test (expected cell counts < 5).
All analyses were performed using SAS, version 9.4 (SAS Institute, Inc, Cary, NC), by the Duke Department of Biostatistics and Bioinformatics (Durham, NC). A P value <.05 was considered statistically significant.
Operative Technique for Vascularized Bone Grafting
We adequately anesthetized the patient, placed the patient supine on the operating room table, and prepped and draped the operative lower extremity. In cases requiring iliac crest bone graft, we prepped and draped the ipsilateral iliac crest into a sterile field. We exsanguinated the lower extremity with an Esmarch bandage and elevated a thigh tourniquet to 250 mm of mercury. We used a dorsal midfoot skin incision that extended from the level of the ankle joint to the tarsal metatarsal joint. In revision cases, we used the previous incision. We dissected free the superficial peroneal nerve and carefully retracted it within a rubber dam. We opened the EHL tendon sheath and retracted the EHL tendon to expose the deep peroneal nerve and anterior artery and veins. Under loop magnification, the deep peroneal nerve was separated from the artery and vein. Proximally, at the level of the talonavicular joint, we dissected the anterior tibial artery and vein to identify arterial and venous branches to the first and third cuneiforms (Figure 2). We isolated the arterial and venous branches that were the largest in diameter and length to use for the vascularized transfer. We dissected these vessels to the distal end of the cuneiform selected for transfer. We were careful not to disrupt the selected vascular pedicle’s communication with the respective cuneiform’s periosteum.
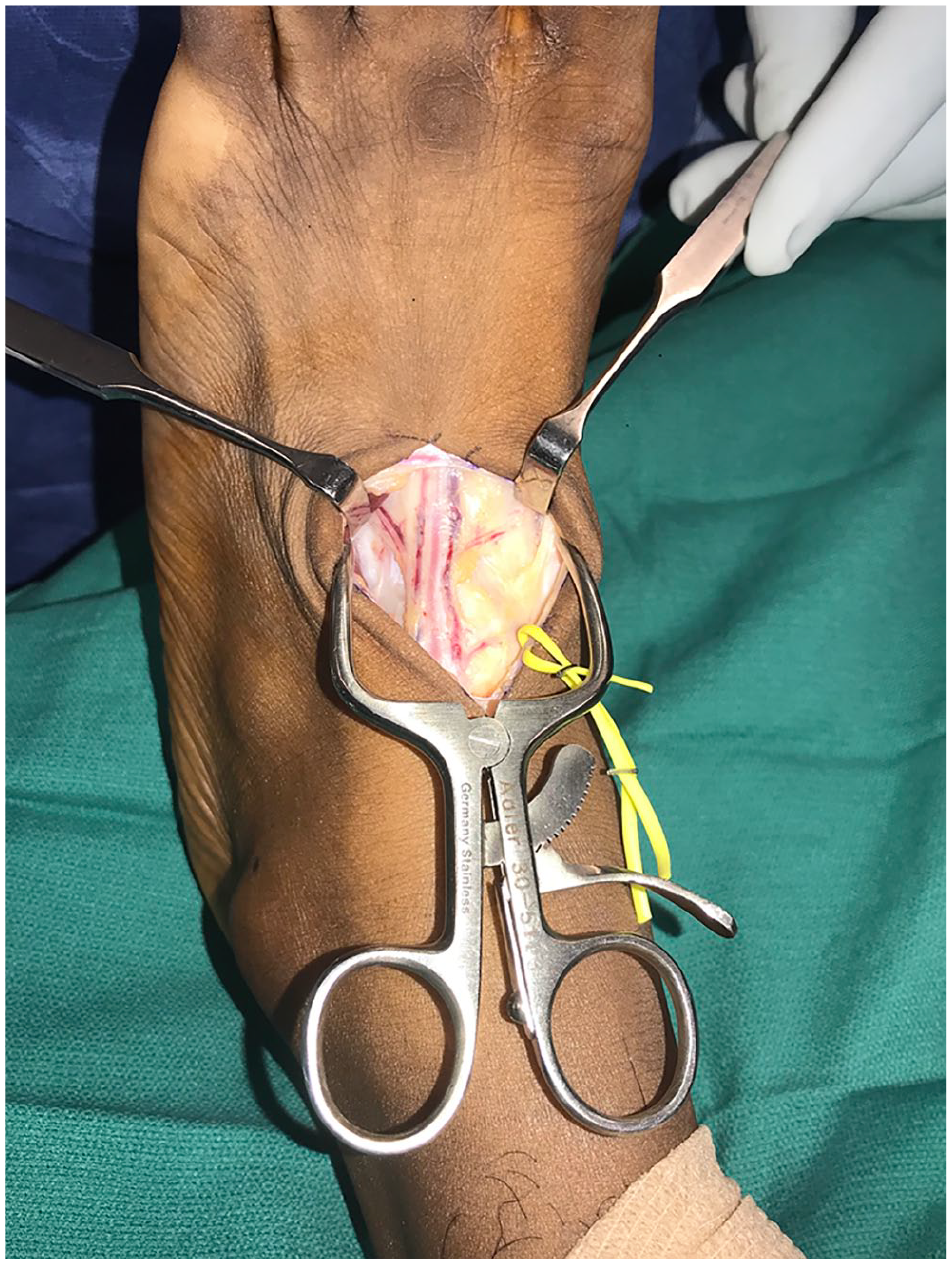
Dorsalis pedis artery with veins and deep peroneal nerve. Medially the artery is going to the first cuneiform, and laterally the vessel is going to the third cuneiform.
At the navicular, we used fluoroscopy and a probe or 22-gauge needle to identify the nonunion site. With minimal periosteal stripping, we made a longitudinal incision directly over the nonunion site. The overlying periosteum was stripped only 2 to 3 mm medially and laterally. Using a Beaver blade, small curette, and small rongeur, we debrided all fibrous tissue from the nonunion site to expose cancellous bone with potential for healing (Figure 3).
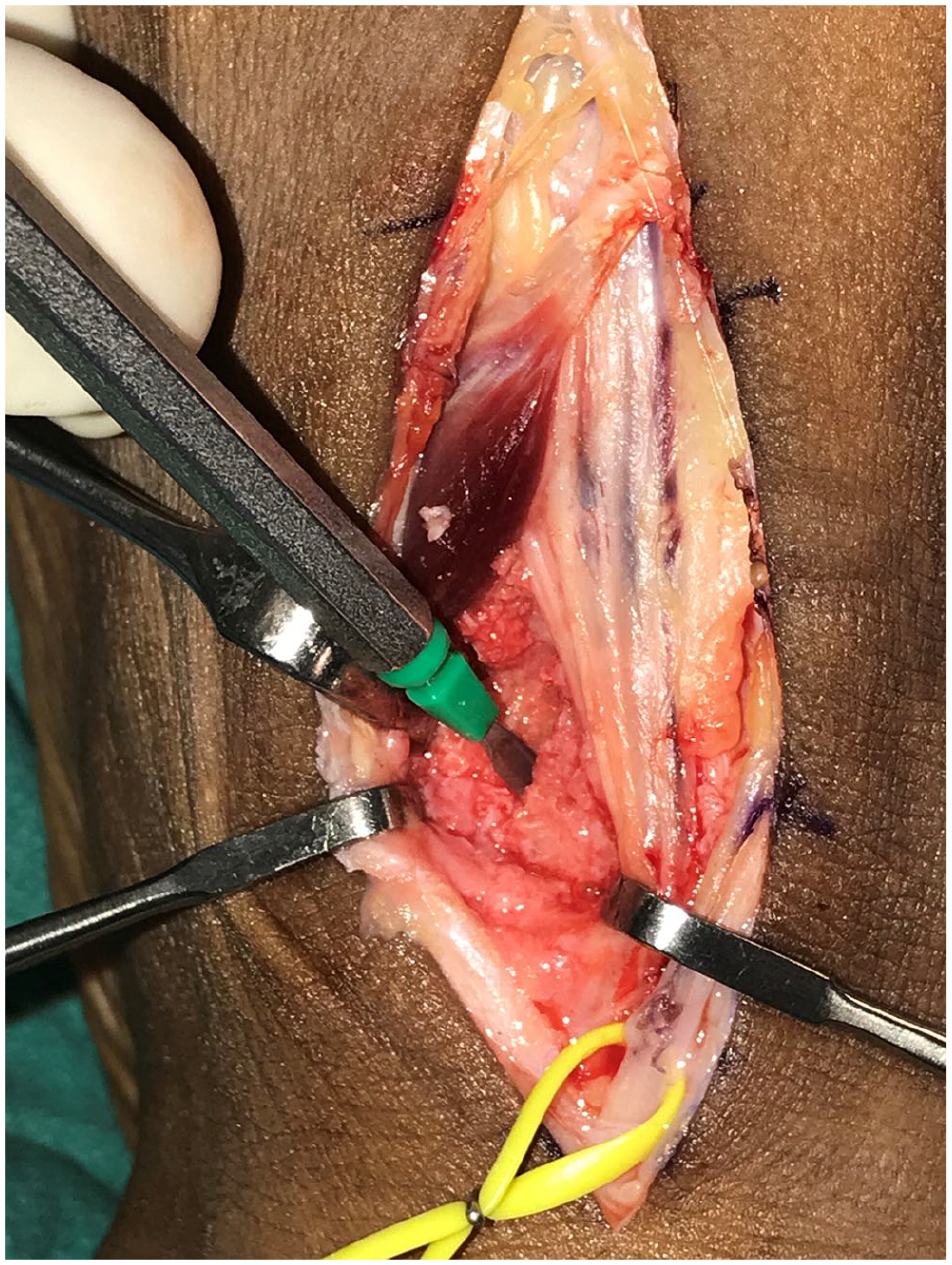
Nonunion site in the lateral navicular is identified with the use of a Beaver blade.
In revision surgery, we used fluoroscopy to identify and assist in removing previous hardware. Often we needed an additional incision to gain optimal access to the hardware for its extraction. Nonunion sites may vary in size and depth, some requiring more bone graft than afforded by the vascularized bone transfer alone.
For iliac crest graft bone graft harvest, we injected 1% lidocaine with epinephrine over the anterior iliac crest. We created a 5-mm skin incision, carefully dissected to the iliac crest and centered a standard 4.5-mm drill guide on the superior iliac crest surface. We advanced the drill guide into the bone, protecting the soft tissues and easily accessing the cancellous bone between the 2 iliac crest tables. When retracted, the drill guide contains the bone harvest. We repeated these steps 2 to 3 times through the same aperature created in the iliac crest but directing the drill guide anteriorly and posteriorly between the iliac crest tables. Ideally, the harvested cancellous bone plugs a centimeter in length and 4 mm in diameter. Alternatively, bone biopsy instrumentation may be utilized. We then morselized the harvested bone to contour optimally into the nonunion site.
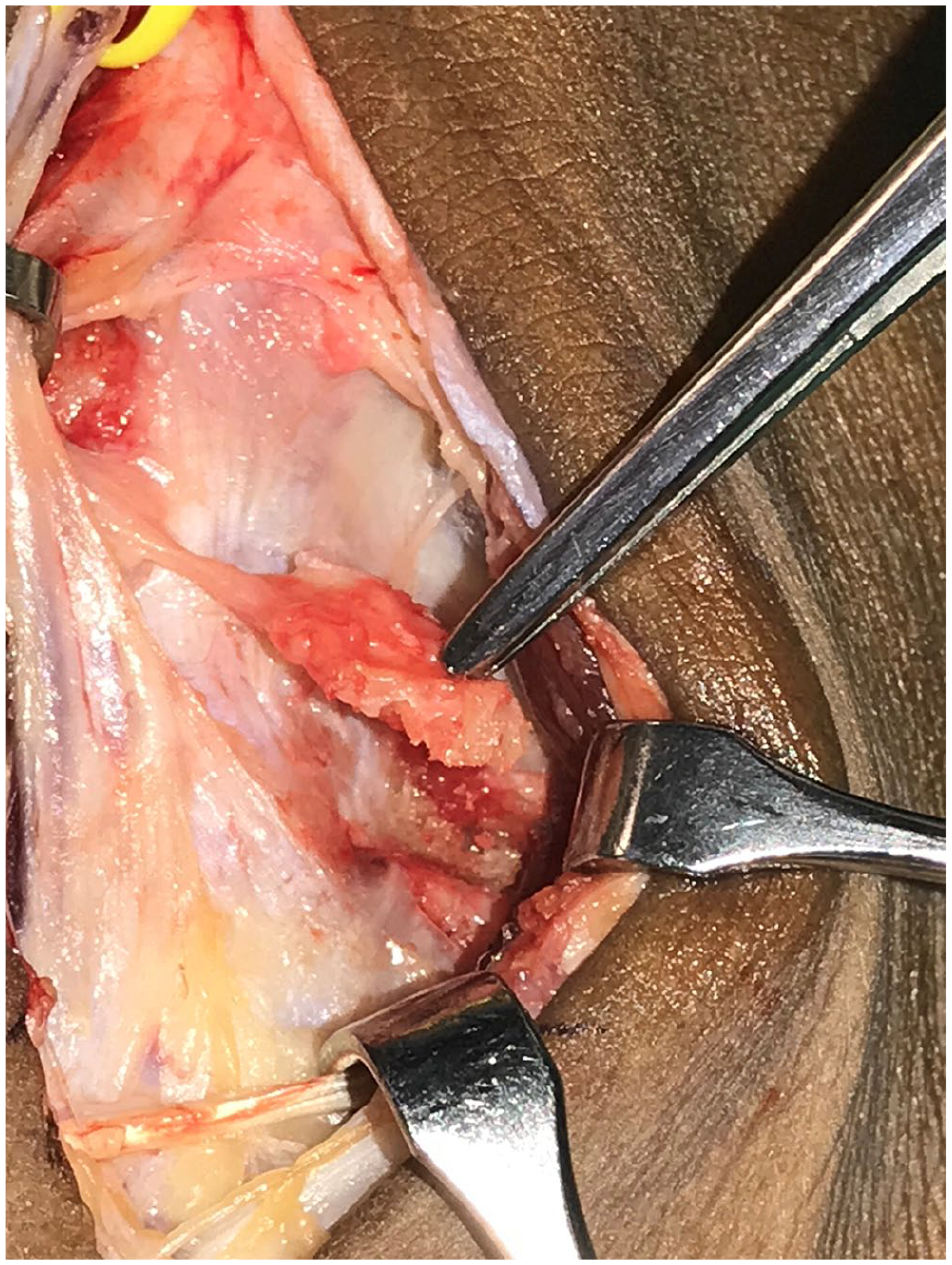
We placed the iliac crest bone graft into the nonunion site (Figure 4). We compressed the nonunion site with a large pointed bone reduction clamp placed on the medial and lateral navicular, confirming ideal clamp position fluoroscopically. Next, under fluoroscopic guidance we percutaneously placed a cannulated screw guide pin from the lateral navicular across the nonunion site and confirmed that the pin did not violate the adjacent talonaviclular or naviculocuneiform joints. We used fluoroscopy in multiple planes to confirm the optimal pin position. Once the pin position was in the desired position, depth was measured to determine screw length. We recommend then carefully driving the guide pin through bone and through soft tissues on the opposite side of the foot from the pin entry site. This maneuver allows extraction of the entire guide pin in the event it should break during drilling. We then overdrilled the guide pin with the cannunlated drill. With compression maintained across the nonunion site, we removed the guide pin and used a solid fully threaded 3.5-mm screw across the nonunion; a partially threaded screw may also be used, but compression will already be applied via the clamp, and a fully threaded screw may afford greater bone fixation on either side of the nonunion.

Cancellous dowel grafts obtained from iliac crest placed into navicular nonunion site.
At the vascularized bone graft harvest site, under fluoroscopic guidance, we placed 25-gauge needles in all 4 joints surrounding the selected cuneiform. Next, we used a 1.1-mm drill to create multiple 1-cm-deep perforations to define the desired vascularized bone graft. We used a drill guide pressed firmly into the periosteum to protect the vascular pedicle from the small-diameter drill. In addition to marking the cuneiform with the surrounding 25-gauge needles, we used fluoroscopy to confirm the distal extent of the graft harvest. We connected the drill holes with a small hand osteotome followed by a curved osteotome to gently elevate the corticocancellous vasculized bone graft from the cuneiform (Figure 5). We ensured that the graft’s vascular pedicle remains patent, and we trimmed the graft’s cancellous bone to fit optimally into the dorsal aspect of the nonunion site (Figure 6). In some cases, the cortical bone at the dorsal navicular nonunion site must be tailored with a rongeur to accommodate the graft. We created a gentle press fit of the graft into the nonunion site. While protecting the vascular pedicle and avoiding excessive tension on the periosteum, we sutured the graft’s periosteum to the navicular periosteum and capsule with 4-0 Vicryl suture. We released the tourniquet to confirm arterial flow into the vascularized graft. We then closed the extensor retinaculum with 2-0 or 3-0 Vicryl, taking care to protect vascular pedicle deep to the retinaculum and the superficial peroneal nerve above the retinaculum. We closed the subcutaneous layer with 3-0 Vicryl, and reapproximated the skin with 4-0 nylon. Finally, we applied sterile dressings, adequate padding, and a posterior/sugar tong splint with the ankle in neutral position.

Four small K-wires placed around the midportion of the vessel and inserted into the first cuneiform to identify boundaries for bone graft elevation.
The vascularized bone graft is rotated on its pedicle into navicular nonunion site dorsally.
Our postoperative routine included nonweightbearing for 6 weeks. We saw patients for wound check, suture removal and conversion to short leg cast at 3 weeks postoperatively. At 6 weeks, we transitioned from cast to CAM boot and allowed patients to gradually advance to full weightbearing over the next 4 weeks. We obtained foot radiographs at 6, 12, and 18 weeks. To ensure that patients were safe to transition from boot to shoe, we routinely obtained the first CT scan at 12 weeks and then subsequent CTs to confirm union. If union was not complete, then we had the patients continue protected weightbearing in the CAM boot for another 6 weeks.
Results
Between 1996 and 2015, the senior investigator performed operative treatment on 43 patients for navicular stress fractures. According to the algorithm, 15 acute stress fractures (34.9%) received ORIF alone, 12 subacute fractures (27.9%) were treated with ORIF plus bone graft, and 16 nonunions (37.2%) had ORIF with vascularized bone graft. Patient-level data are presented in Tables 1 through 3 by surgery treatment group.
Open Reduction and Internal Fixation (n = 15).
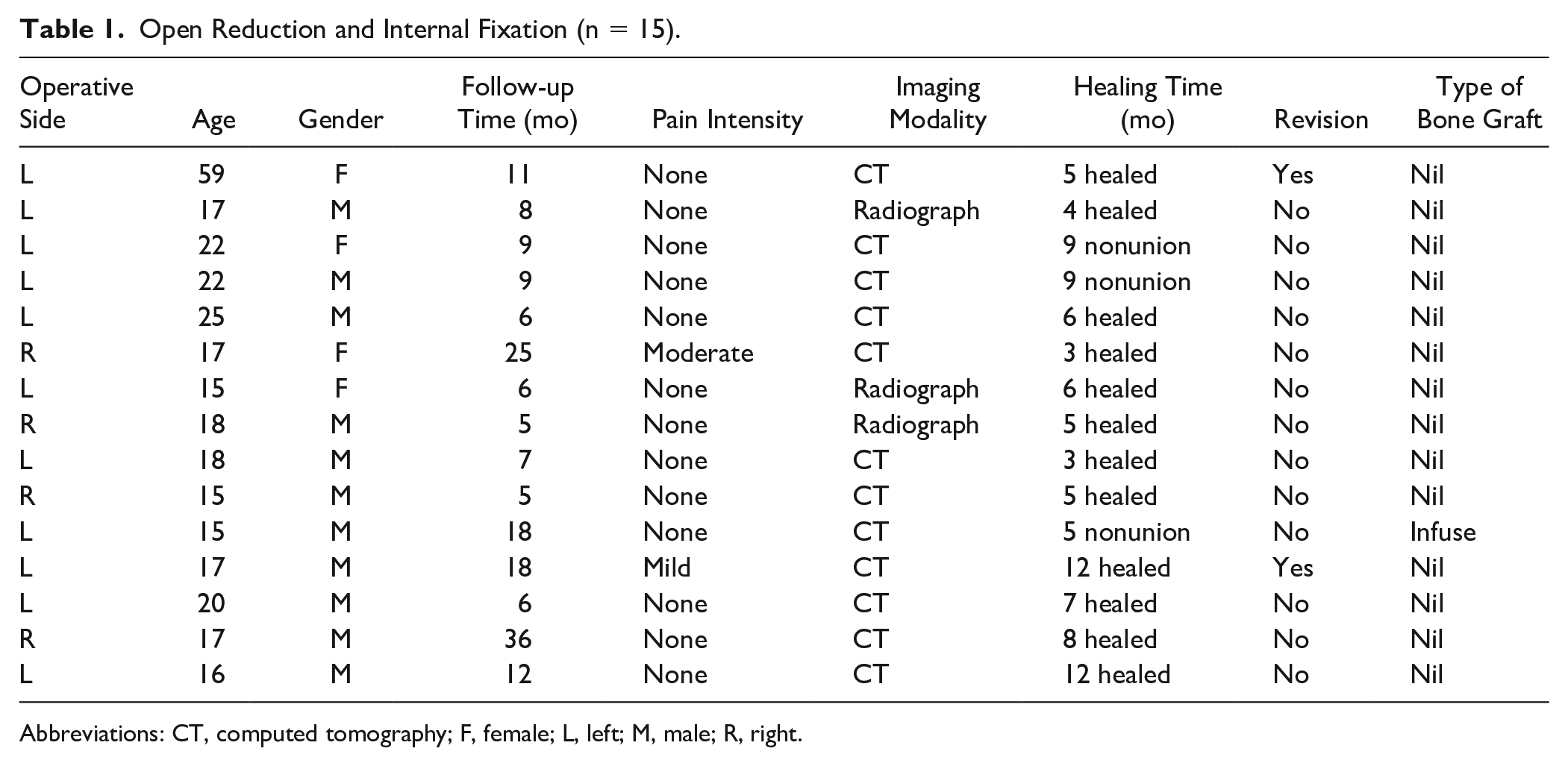
Abbreviations: CT, computed tomography; F, female; L, left; M, male; R, right.
Open Reduction and Internal Fixation With Bone Graft (n = 12).
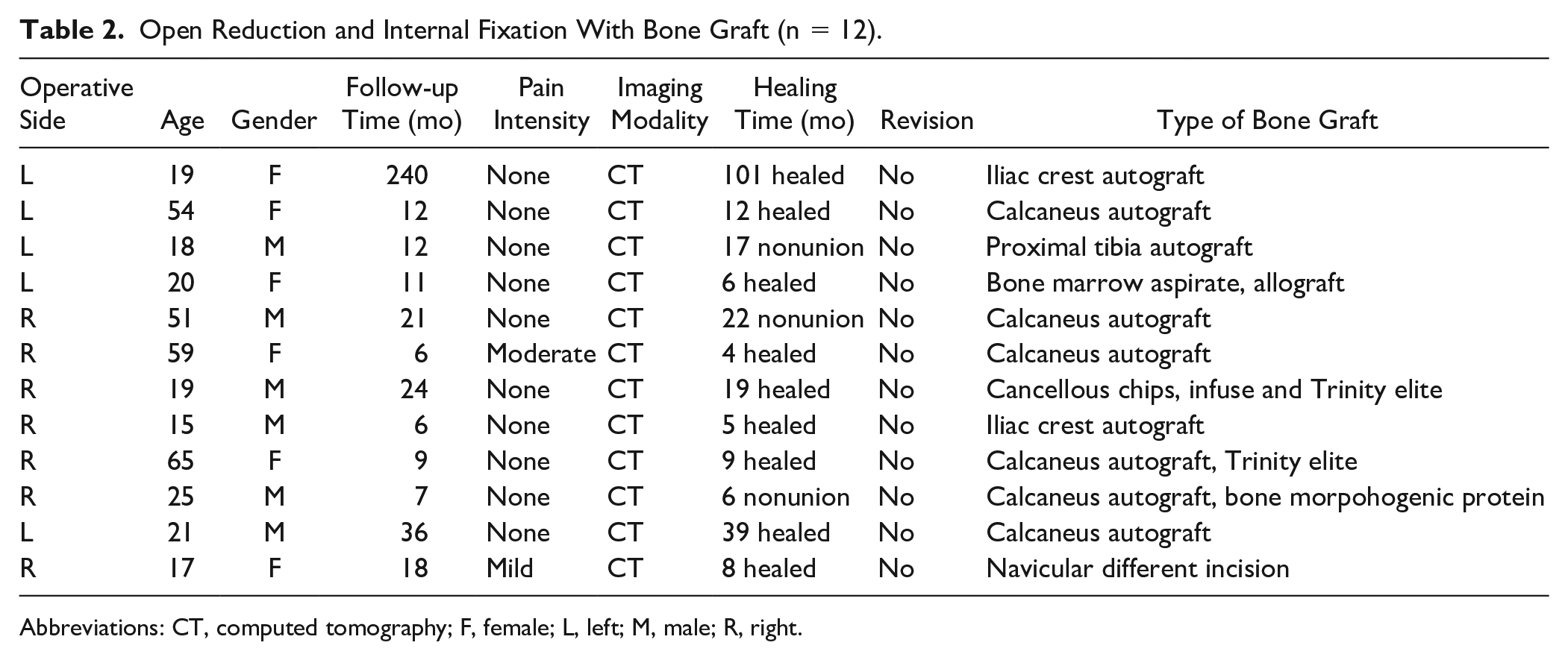
Abbreviations: CT, computed tomography; F, female; L, left; M, male; R, right.
Vascularized (n=16).
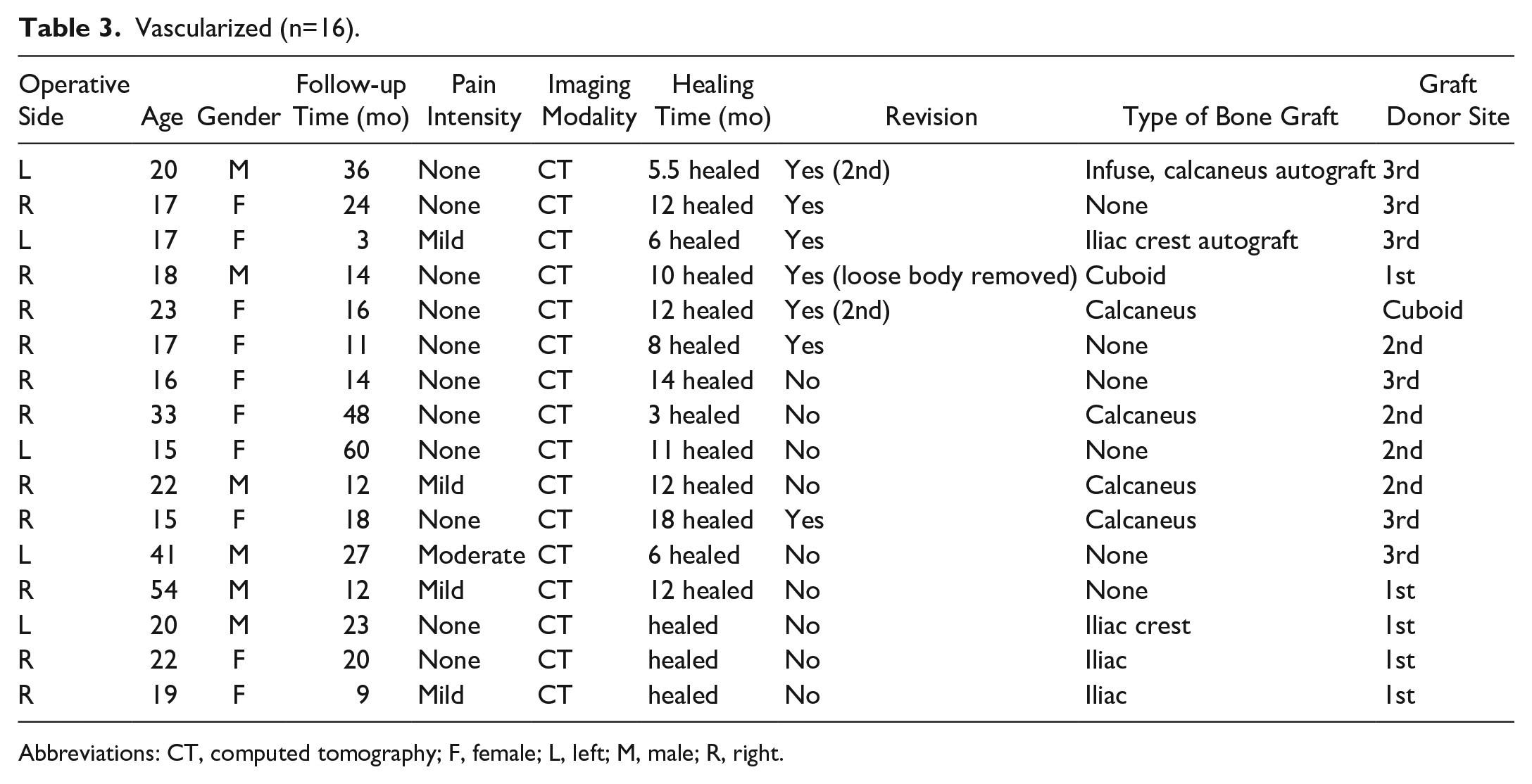
Abbreviations: CT, computed tomography; F, female; L, left; M, male; R, right.
Twenty-three male (53.5%) and 20 female patients (46.5%) were included in the study, and their distribution was not significantly different across the 3 groups (P = .127). Twenty-two right (51.2%) and 21 left (48.8%) navicular stress fractures were observed, and operative side was also not statistically significant across the 3 groups (0.058). No significance difference (P = .142) was found among the median (Q1, Q3) age of patients within the 3 groups, including 17 (16, 22) in the ORIF-alone group, 20.5 (18.5, 52.5) in the ORIF with bone graft group, and 19.5 (17.0, 22.5) years in the ORIF with vascularized bone graft group (Table 4).
Patient Characteristics by Operative Treatment Group. a
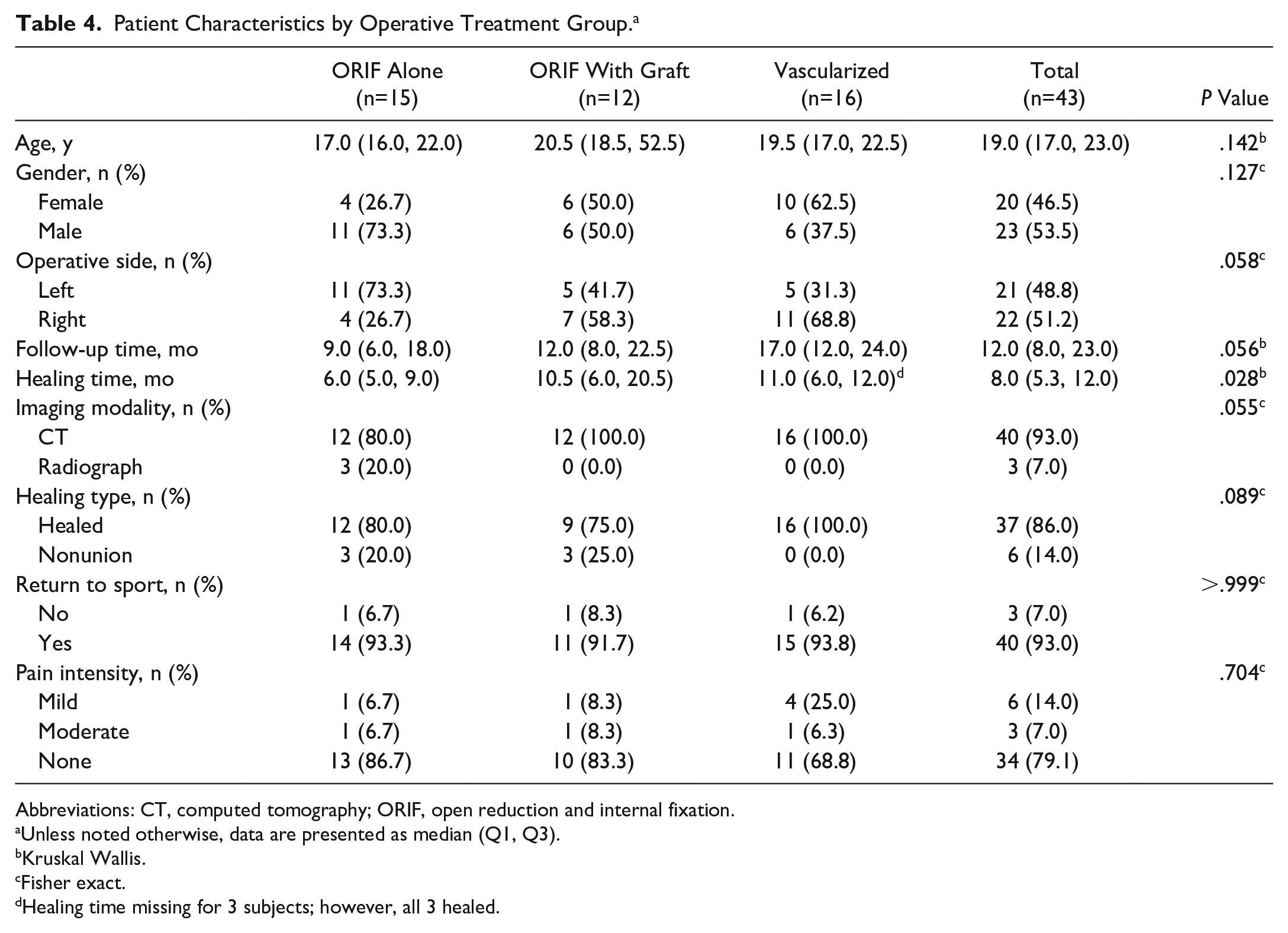
Abbreviations: CT, computed tomography; ORIF, open reduction and internal fixation.
Unless noted otherwise, data are presented as median (Q1, Q3).
Kruskal Wallis.
Fisher exact.
Healing time missing for 3 subjects; however, all 3 healed.
Follow-up times across the 3 groups were trending differently but also did not reach statistical significance (P = .056) with the median (Q1, Q3) follow-up time in months being 9 (6, 18) for ORIF, 12 (8, 22.5) for ORIF with bone graft, and 17 (12, 24) months for ORIF with vascularized bone graft (Table 4).
Radiographic healing was compared across the 3 groups. Three patients in the ORIF group only received radiographs to evaluate healing. All of the other patients in all 3 groups had CT scans used for follow-up. The 3 patients who only had radiographic imaging were healed on routine imaging. The ORIF group had an 80% union rate (12/15). The ORIF with bone graft group had a 75% union rate (9/12), and the ORIF with vascularized bone graft group had a 100% union rate (16/16). There was no statistically significant difference in radiographic union rates across groups when compared using Fisher exact test (P = .089) (Table 4).
Return to sport (yes vs no) also did not show any significant difference among the 3 groups (P > .999). When evaluating return to sport based on level of pain, 86.7% (13/15) returned to the same level of preinjury sport within the ORIF-alone group without pain compared with 83.3% (10/12) in the ORIF with bone graft and 68.8% (11/16) in the ORIF with vascularized bone graft. Each group had 1 patient who was unable to return to sport without pain. In the ORIF with vascularized bone graft group, this patient had significant talonavicular degenerative changes prior to surgery and was counseled on these findings preoperatively. He went on to have a talonavicular arthrodesis as a secondary surgery and was then pain free with activity. Six patients were able to return to a lower level of sport with pain that eventually resolved, including 1 in the ORIF group, 1 in the ORIF with bone graft group, and 4 in the ORIF with vascularized bone graft group. We did not find a significant difference when evaluating level of pain when returning to sport across operative groups using Fisher exact test (P = .704) (Table 4).
Lastly, we compared radiographic union to return to sport pain level and found that there was not a statistically significant correlation (P = .726). All 6 (100%) of the nonunions and 28 (75.7%) of the 37 unions were able to return to sport without pain. Six (16.2%) radiographic unions were able to return to a lower level of sport with resolving pain, whereas 3 (8.1%) radiographic unions were not able to return to sport without pain.
Discussion
Frequently, navicular stress fractures are misdiagnosed acutely and often present after some delay. Symptoms may persist for months before patients are accurately diagnosed. 8 The navicular’s unique vascularity predisposes it to a relatively high nonunion rate after stress fracture; appropriate treatment, even ORIF with or without iliac bone grafting, does not always lead to healing of these fractures.5,12 Our aim was to apply the senior authors’ treatment algorithm over a 20-year period to determine if complex and revision cases treated with vascularized grafting would have similar outcomes to more traditional treatment with ORIF with or without bone grafting. To our knowledge, our study is the largest cohort of navicular stress fractures that proposes a treatment algorithm to include symptom duration, failed prior surgery, and radiographic findings. Our investigation affords surgeons evidence-based approximations of rates of radiographic union of navicular stress fractures and patients’ potential return to sport. Although 43 patients do not constitute a large cohort, it is a large number of patients for this relatively rare fracture. Another strength of this study is that the senior author was involved in all cases, thus maintaining consistency in operative management.
In their 2010 meta-analysis, Torg et al 15 showed strong evidence supporting conservative management of acute navicular stress fractures. The authors reported no difference in healing rates being nonweightbearing with or without immobilization.
Our investigation suggests that there is no significant difference in radiographic healing between ORIF for acute fractures, ORIF with bone graft for subacute fractures, and ORIF with cancellous bone graft and vacularized bone grafting. Likewise, there is no difference in return to sport between the 3 groups. Using the senior authors’ algorithm for the treatment of navicular stress fractures, we demonstrated an equivalent rate of radiographic healing for nonunions treated with vascularized bone grafting compared to acute and subacute fractures treated without vascularized grafting. The number of patients and the 3 techniques are too small to test for statistical differences. It is our opinion that this approach is reasonable as it has worked well in our hands. Our findings correlate duration of symptoms and radiographic findings with optimal operative management of navicular stress fractures.
Our investigation’s limitations include small sample size, retrospective analysis, and short follow-up. Despite being one of the largest operative cohort of navicular stress fractures, this comparative study’s cohorts are small in number and therefore underpowered in our effort to determine statistical significance. A prospective, randomized controlled study may yield more evidence-based outcomes than our retrospective comparative methods. However, our aim was to analyze the senior author’s algorithm, which would not be possible using a prospective randomized protocol and may not have been appropriate in cases of nonunion. Although we could glean patients’ ability to return to sport, the retrospective nature also limited our ability to capture exact dates of patients’ return to sport. Furthermore, many patients traveled to our tertiary referral center for treatment, especially patients with nonunions opting for ORIF with vascularized bone grafting. Select patients’ most recent follow-up visits at our institution were relatively short, and follow-up data included combinations of our investigators’ evaluations and reports forwarded by local providers who assumed the patients’ longer follow-up care. Finally, since this cohort was treated, we have begun to use the medial geniculate artery free flap from the medial femoral condyle to transfer larger amounts of cancellous bone and, if needed, inclusion of a skin paddle, which was not studied or reported on in the current investigation
Conclusion
Application of the senior author’s treatment algorithm of navicular nonunions, rates of radiographic union and return to sport were equivalent for acute fractures treated with ORIF, subacute fractures treated with bone grafting and nonunions treated with ORIF plus vascularized bone grafting. It is our opinion that the algorithm developed and used in the populations presented has worked well in our hands and is an approach that can be taken with these difficult fractures.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007211034812 – Supplemental material for Treatment of Navicular Stress Fractures With an Algorithmic Approach
Supplemental material, sj-pdf-1-fai-10.1177_10711007211034812 for Treatment of Navicular Stress Fractures With an Algorithmic Approach by James A. Nunley, Cynthia Green, Joel Morash and Mark E. Easley in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.