
Abstract
Background:
Malposition of the sesamoids relative to the first metatarsal head may relate to intersesamoid crista underdevelopment or erosion. Using 3-dimensional models created from weightbearing CT (WBCT) scans, the current work examined crista volume and its relationship to first metatarsal pronation and sesamoid station.
Methods:
Thirty-eight hallux valgus (HV) patients and 10 normal subjects underwent weightbearing or simulated WBCT imaging. The crista was outlined by the inferior articular surface, and a line was drawn to connect the lowest point of each sulcus on either side of the intersesamoidal crista throughout the length of the crista. The volume was calculated. Sesamoid station and first metatarsal pronation were calculated from the 3D reconstructions. The mean crista volumes between HV and normal patients were statistically compared, as were the crista volume and pronation angle between sesamoid stations.
Results:
The mean crista volume in HV patients was 80.10 ± 35 mm3 and in normal subjects was 150.64 ± 24 mm3, which differed significantly between the 2 groups (P < .001). Mean crista volumes were found to be statistically significantly different between the sesamoid stations (P < .001) with decreasing crista volumes significantly and strongly correlated with increasing sesamoid station (r = −0.80, P < .001). There was no difference in the mean pronation angle between the 4 sesamoid stations (P = .37). The pronation angle was not associated with crista volume (P = .52).
Conclusion:
HV patients have lower mean crista volume than normal patients. Crista volume is correlated with sesamoid station. Pronation of the first metatarsal was not associated with crista volume.
Clinical Relevance:
Crista volume may offer an additional determinant for the severity of hallux valgus.
Keywords
Introduction
Hallux valgus (HV) is one of the most common foot deformities that causes forefoot pain. HV can be assessed radiologically on plain films by measuring the intermetatarsal (IMA) and hallux valgus angles (HVA). HV, however, is increasingly understood to be a 3-dimensional deformity. Three-dimensional (3D) reconstructions of the metatarsals and first phalanx created from weightbearing computed tomography (WBCT) scans have demonstrated the means to quantify first metatarsal pronation, showing that 3-dimensional models are applicable to HV problems. 2
Since 1923, realignment of the sesamoids to their normal position is believed to be important for a successful bunion correction surgery. 17 Talbot and Saltzman showed that metatarsal-sesamoid subluxation is directly related to the HV deformity and that the tangential/axial sesamoid view is the most accurate view to evaluate sesamoid position on plain radiographs. 19 Kuwano et al 12 compared the sesamoid position determined from the AP view to that on the tangential sesamoid view and determined that the AP view is not valid for evaluating sesamoid position. However, the position of the sesamoids with subluxation has been found to correlate with both clinical outcomes and risk of recurrence of the HV deformity.3,15 Park and Lee 15 found that immediate postoperative metatarsal-sesamoid subluxation of greater than or equal to grade IV of VII following HV surgery resulted an increased likelihood of developing recurrence of the HV deformity when compared to patients with less subluxation, with an odds ratio of 9.7. Therefore, understanding the relationship of sesamoid position and HV deformity may have important surgical implications.
The progression of hallux valgus (HV) deformities results in relocation of the sesamoids relative to the first metatarsal, from their position under the plantar surface of the distal first metatarsal. With this translocation, it is possible that the crista separating the 2 sesamoids erodes as the contact of the medial sesamoid applies force against the crista with weightbearing. Although degenerative changes under the first metatarsal head are known to coincide with developing HV, the relationship of crista volume to the hallmark parameters of HV remains uncertain. It is also unknown whether this change in volume has a direct relationship to sesamoid station.
A previous study found that increasing HV deformity and first metatarsal-sesamoid location were associated with osteoarthritis of the sesamoid metatarsal joint; however, the study did not quantify the severity of the osteoarthritic changes or investigate its association with first metatarsal pronation, which is increasingly recognized as an important aspect of the triplanar HV deformity. 9 No studies have quantified the crista volume itself and the relationship of its volumetric change in the progression of HV.
The purpose of the current investigation was to examine the relationship of the volume of the crista to pronation, sesamoid station, IMA, and HVA using 3-dimensional models of patients’ deformities. We hypothesized that crista volume is associated with sesamoid position, intermetatarsal angle, hallux valgus angle, and first metatarsal pronation in HV deformities.
Methods
Study Cohort
Thirty-eight HV patients who were indicated for surgical correction and 10 normal subjects composed the subject population for this study. None of the patients in this study were indicated for a first metatarsophalangeal (MTP) joint fusion for degenerative changes at the first MTP joint. Of the 38 patients (average age 52±10 years) indicated for surgical correction, 29 were patients from the Hospital for Special Surgery, New York, NY and 9 (average age 46±14) were patients at UPMC Passavant Hospital, Pittsburgh, PA. The 10 normal patients were from the general population of Pittsburgh, PA. Weightbearing images were obtained in a PedCat (CurveBeam, Inc) for subjects in New York, and weightbearing images were obtained with a weightbearing equivalence pedal device in a LightSpeed VCT (GE, Inc) in Pittsburgh.2,7,8 It has been shown that the pedal device provides an equivalent loading situation.7,8
Sesamoid Position and Crista Volume Measurements
Using the program Mimics, each patient’s WBCT scans were uploaded to a computer and processed. The coronal, axial, and sagittal views of the WBCT scans, along with a 3-dimensional reconstructive view, each provided specific data about the forefoot. The coronal plane yielded a tangential sesamoid view, which was used to determine the sesamoid position of each patient, using the 4-stage American Orthopaedic Foot & Ankle Society (AOFAS) scale (0 = sesamoid completely medial to mid-axial line, 1 = sesamoid less than 50% overlapping the line, 2 = sesamoid greater than 50% overlapping the line, and 3 = sesamoid completely lateral to the line; Figure 1).
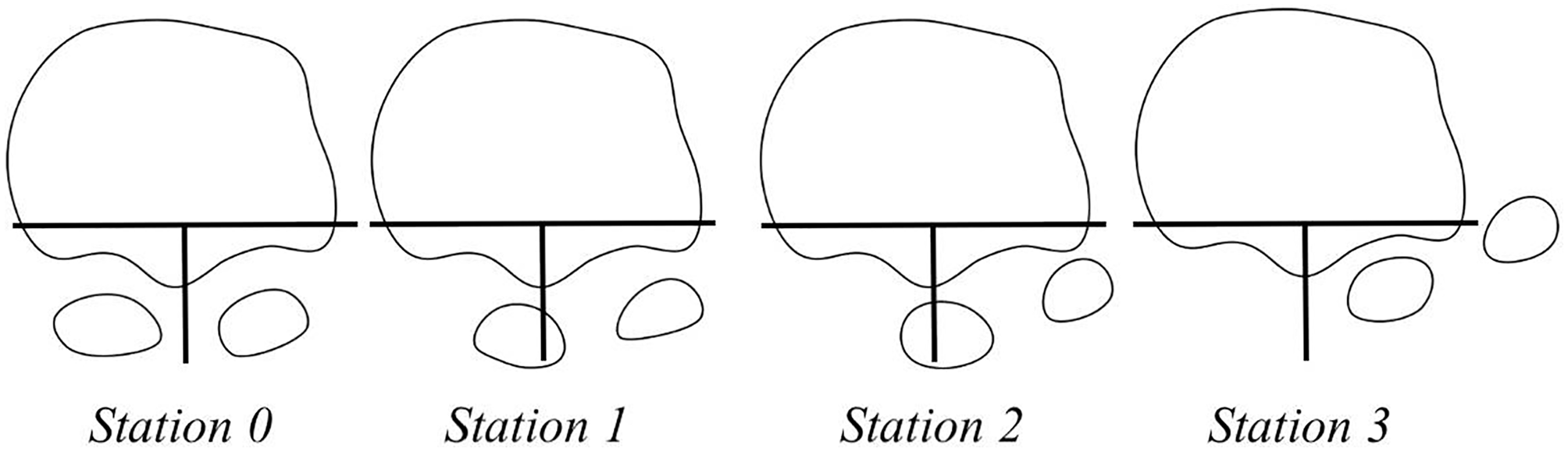
Sesamoid grading according to the position of the tibial sesamoid relative to the crista (intersesamoid ridge).
Volumetric measures of the crista using the CT images were then determined. Using coronal cross sections of the crista in each axial CT slice, a line segment was drawn connecting the lowest point of each sulcus on either side of the intersesamoidal crista in each slice of the weightbearing image. To make all measurements consistent for every patient, the start and end point in the anteroposterior direction for the crista was chosen as the points at which both sulci were no longer visible. This choice ensured that the entire structure was included. Each slice of the crista was carefully examined and highlighted from the WBCT image (Figure 2). Using the known slice thickness from the CT scan, the volume was computed.
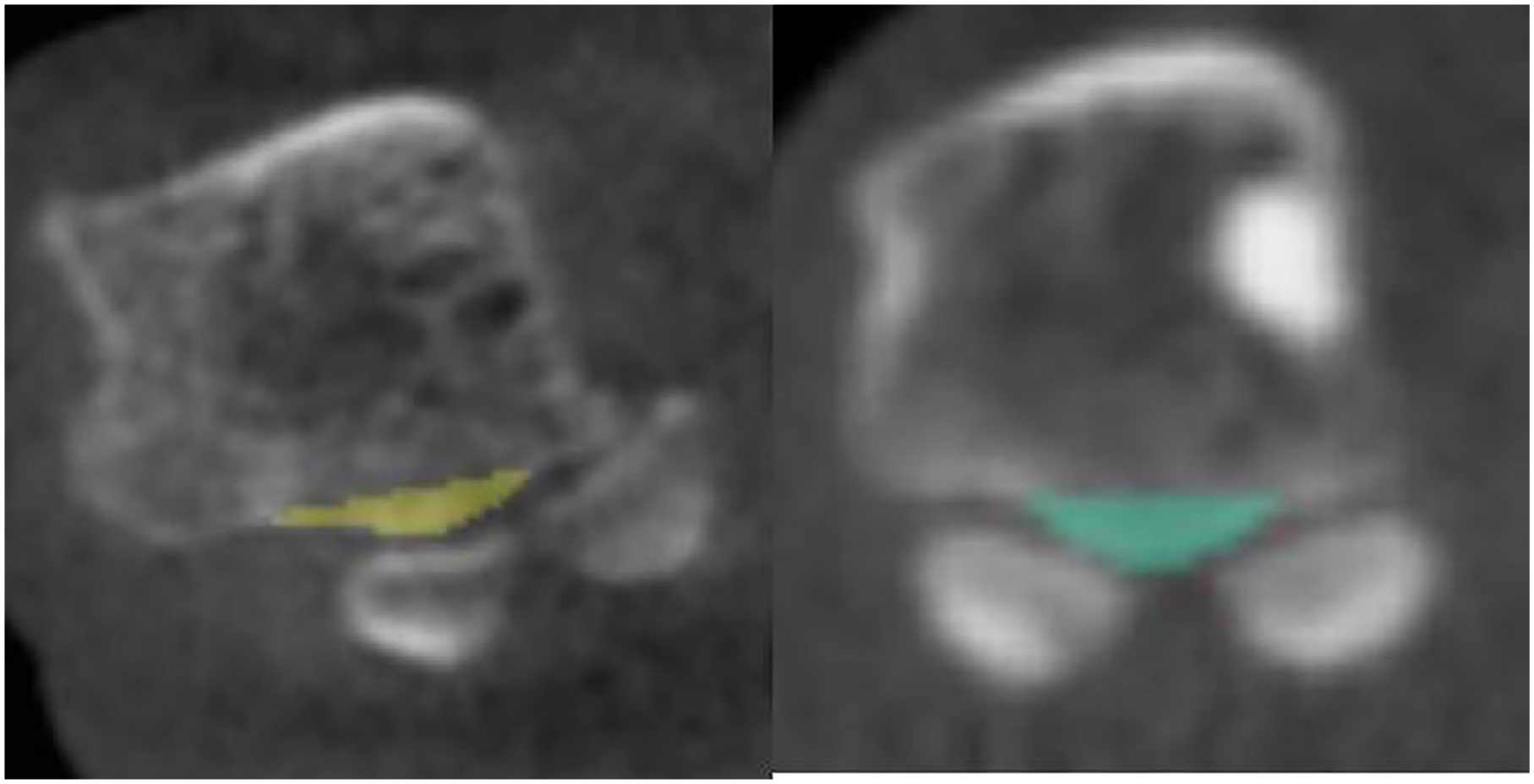
Calculation of the crista volume on weightbearing CT scans. On the left, the crista has eroded as the medial sesamoid subluxed laterally. On the right, the crista volume is significantly higher as the medial sesamoid tracked normally.
Using the program Disior Bonelogic (Disior Ltd), auto-segmentation was completed from the WBCT scans of each patient. With the 3D reconstructions from Disior, the pronation of the first metatarsal was then calculated with respect to the second metatarsal. The orientations of the first and second metatarsals were determined from coordinate systems established by selecting landmarks with the program Geomagic (3D Systems, Research Triangle Park, NC). The coordinates of the landmarks (points) were exported from Geomagic and used in a calculation to geometrically determine the 3D orientation angles using the aeronautical system of yaw-pitch-roll. The point-picking method used to calculate pronation has been previously described and validated by Campbell et al. 2 IMA and HVA were then quantified from weightbearing radiographs using the techniques described in Campbell et al.2,18
Statistical Analysis
Parametric tests, or their nonparametric equivalent, were used to calculate the differences between groups. Because sesamoid station is an ordinal variable, the median sesamoid station is reported, and sesamoid stations between the hallux valgus and normal patients were compared using a Mann-Whitney U test. To determine if there were differences in mean crista volume between the HV and control patient groups, t tests were employed. The sesamoid stations for all patients were grouped using the 4-stage AOFAS scale, and crista volume, IMA, HVA, and pronation angle between these 4 groups were compared using 1-way analysis of variance and Tukey-Kramer post hoc tests if the relevant ANOVA proved significant. Spearman rank coefficient (rho) was used to test the relationship of sesamoid station with the IMA, HVA, crista volume, and pronation angle. Linear regressions were performed to determine whether the volume of the crista was associated with the IMA, HVA, and the pronation angle. Statistical significance was set to P <.05. All statistical tests were performed in Excel.
Results
A total of 48 radiographs and WBCT scans of 48 patients were evaluated, of which all were female. The age range was between 26 and 76 years (mean 53 years, SD 13 years).
The median sesamoid stations were at station 2 (interquartile range 1 [IQR 1]) in HV subjects and station 0 (IQR 0) in the non-HV group; the 2 groups were found to be statistically significantly different from each other (P < .001). The mean crista volume in HV patients was 80.1 mm3 (range 18-147, SD 35 mm3) and in normal subjects it was 150.6 mm3 (range 114-190, SD 24 mm3), which differed significantly between the 2 groups (P < .001).
The mean crista volume, IM angle, and HV angle were found to be significantly different between the 4 sesamoid stations (all P values < .001) (Table 1). The mean first metatarsal pronation did not differ between the 4 sesamoid station groups (P = .370). The mean values of the crista volume were 154.4 mm3 for grade 0, 98.2 mm3 for grade 1, 78.5 mm3 for grade 2, and 44.8 mm3 for grade 3 (Figure 3). The post hoc tests showed there was a significant difference in crista volume between sesamoid grades (all P values < .005), except for grades 1 and 2 (P = .08). The mean IMA values were 9.8 degrees for grade zero, 13.4 degrees for grade one, 16.4 degrees for grade 2, and 17.5 degrees for grade 3. The post hoc test showed there was significant difference in IMA between sesamoid grades (all P values < .05), except for grades 2 and 3 (P = .35). The mean HVA values were 11.6 degrees for grade 0, 24.5 degrees for grade 1, 31.3 degrees for grade 2, and 41.8 degrees for grade 3. The post hoc test showed there was significant difference in HVA between each sesamoid grade. The age of the subjects in the 4 sesamoid station groups were found to not be statistically different (P = .08).
Mean Crista Volume, IMA, HVA, and First Metatarsal Pronation by Sesamoid Grade (N = 48). a
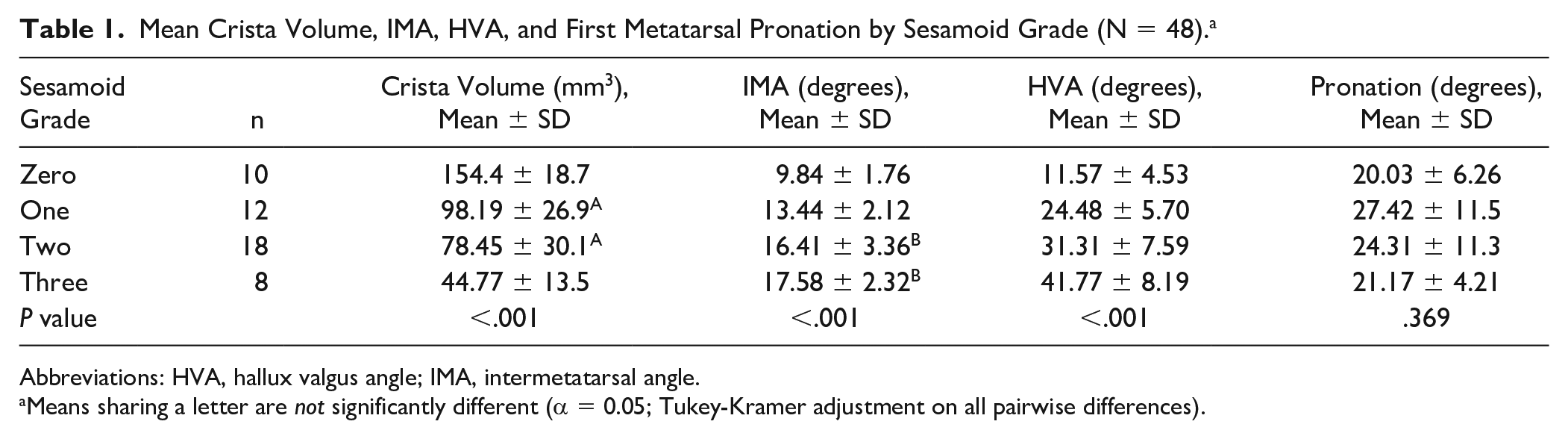
Abbreviations: HVA, hallux valgus angle; IMA, intermetatarsal angle.
Means sharing a letter are not significantly different (α = 0.05; Tukey-Kramer adjustment on all pairwise differences).
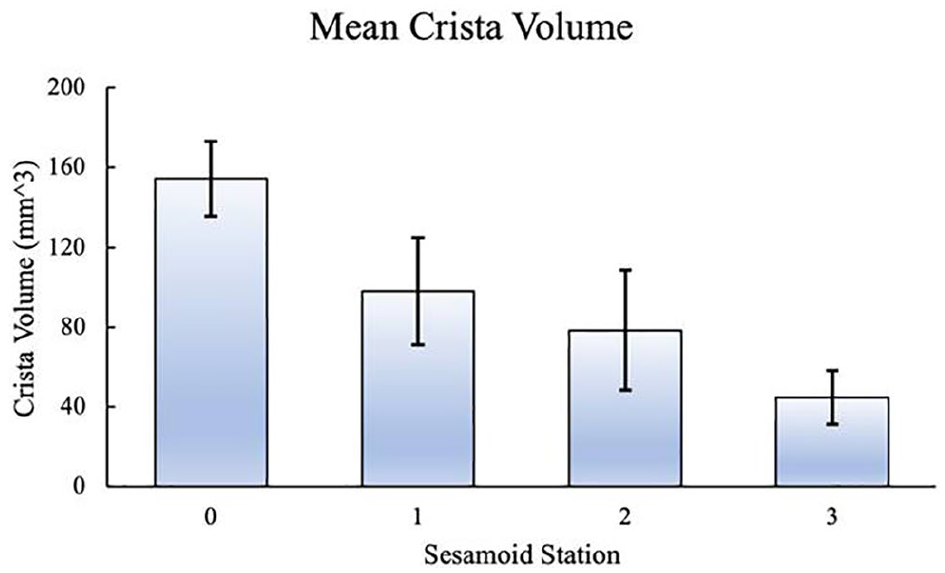
Crista volume averages and SD for each sesamoid station.
A statistically significant correlation was noted between sesamoid station and IMA (rho = 0.73, P < .001), sesamoid station and HVA (rho = 0.81, P < .001), and sesamoid station and crista volume (rho = 0.80, P < .001). No statistical significance was found between sesamoid station and pronation angle (P = .66).
A linear regression analysis demonstrated that the crista volume was not associated with the amount of first metatarsal pronation (P = .52) or age (P = .28). However, the regression of crista volumes against the HVA demonstrated statistical significance (P < .001) and a Pearson correlation coefficient of 0.75. The regression of crista volumes against the IMA also showed statistical significance (P < .001), with a Pearson correlation coefficient of 0.65.
Discussion
Reduced prominence of the crista is commonly encountered in patients with HV. 6 However, no studies have sought to relate crista volume with sesamoid position and the magnitude of the HV deformity on WBCT scans. Reduction of crista volume may be an underrecognized component of the HV deformity. Our study found that IMA, HVA, and sesamoid position were all correlated with crista volume in a cohort of normal and HV patients. Increasing sesamoid station was associated with greater AP radiographic deformities, including IMA and HVA and a lower crista volume on WBCT scans.
The sesamoid complex is connected to the second metatarsal with strong ligamentous fibers while the connection between the first and second metatarsal is weak. 10 Medial deviation of the first metatarsal over the relatively fixed sesamoids results in displacement of the sesamoids from their grooves relative to the metatarsal. Because the translocation of the medial sesamoid from position 0 to position 3 occurs over time, it is possible that either cristae underdevelopment predisposes this shift or crista erosion from medial sesamoid wear increases with increasing station. Because we did not follow these patients over time, an alternative explanation for our findings is that decreased crista volume in HV patients is due to an intrinsic underdevelopment of the crista resulting in the deformity. Decreased crista volume in HV patients may contribute to a worse IMA, HVA, and sesamoid position.
Pronation of the first metatarsal, however, was not correlated with the sesamoid position. This is in keeping with Conti et al, 5 who demonstrated poor correlation between first metatarsal pronation and sesamoid position in patients with hallux valgus, and with Kim et al, 11 who defined a subgroup of pronated first metatarsals that had no sesamoid deviation. Because first metatarsal pronation and sesamoid position are independent deformities, it is not surprising that crista volume was found to be associated with sesamoid station and not first metatarsal pronation. This supports the hypothesis that displacement of the sesamoids from their grooves leads to degenerative changes of the crista. Our results also suggest that a coronal WBCT scan view may help to quantify degenerative changes at the first metatarsal-sesamoid articulation. 19 In our study, medial sesamoid location as determined by sesamoid station was associated with volume of the crista. However, the clinical significance of degenerative changes at the first metatarsal-sesamoid joints has not yet been clearly elucidated.
Katsui et al 9 looked at the relationship between degenerative changes of the sesamoid metatarsal joint and lateral shift of the sesamoids in 269 feet with hallux valgus using simulated WBCT scans. Degenerative changes of the sesamoid metatarsal joint were categorized into osteoarthritis-negative and osteoarthritis-positive groups. Patients in the osteoarthritis-negative group had an intact crista without bony changes, whereas patients in the osteoarthritis-positive group had erosive or cystic changes of the sesamoid metatarsal joint or erosion of the crista on simulated WBCT scans. As the sesamoid moved farther from their native position, the percentage of patients with osteoarthritic changes of the sesamoid-metatarsal joint increased. Additionally, the mean HVA and IMA increased with increasing grades of sesamoid malposition. This study was limited by the binary classification of osteoarthritis changes of the sesamoid metatarsal joint and inability to determine if first metatarsal pronation had an effect on crista size. However, their findings are consistent with the findings of our study. Degenerative changes of the sesamoid metatarsal joint as determined from decreasing crista volumes in our study were correlated with increased sesamoid station. Additionally, increasing sesamoid station was also associated with increased HVA and IMA deformities.
Chen et al 3 investigated the role of postoperative tibial sesamoid position on patient-reported outcomes using the visual analog scale, the AOFAS hallux metatarsophalangeal-interphalangeal scale, and patient satisfaction following surgery for hallux valgus deformity in 250 feet. They used the Hardy and Clapham tibial sesamoid position classification system to grade sesamoid position (grades I-VII) based on the longitudinal axis of the first metatarsal. Patients with higher postoperative sesamoid position grades (grades V-VII) were considered “outliers.” They found that the VAS score was 1 point better and the AOFAS Hallux score was 6 points better in the normal group compared to the outliers group. Additionally, patients in the outliers group were more likely to be dissatisfied with their surgery than patients in the normal group. The authors concluded that postoperative sesamoid position influenced 2-year postoperative patient-reported outcomes and that patients with more aberrant sesamoid positions on AP radiographs had worse clinical outcomes.
However, another study found that AP radiographs were not adequate to assess sesamoid relocation. 11 Kim et al compared sesamoid position on weightbearing AP radiographs using the Hardy and Clapham tibial sesamoid position classification to the position of the sesamoids on simulated WBCT scan coronal views in 166 feet with hallux valgus. They described a group of patients who had “pseudo-sesamoid subluxation,” which was defined as a high-grade sesamoid position (grades V-VII) on the AP radiograph but a grade 0 (reduced) sesamoid subluxation on the axial WBCT view. The authors reported that “pseudo-subluxation” of the sesamoids occurred in 25.9% of patients and may be due to increased first metatarsal pronation. Consequently, weightbearing AP radiographs may not be a reliable tool to assess postoperative sesamoid position and that first metatarsal pronation may be an important variable to consider when discussing changes of the first metatarsal-sesamoid articulation.
Patient discomfort from HV has been attributed to shoe fit, prominence of the medial eminence, capsuloligamentous stretch around the first metatarsophalangeal joint, and incongruency of the first MTPJ.14,16 Although these theories have been promoted, there have been no demonstrated anatomic descriptions of disease in the tissues thought to cause pain. Treatments have often been based on concepts of the disease; for example, if ill-fitting footwear was thought to cause pain, then the logical treatment would be for the patient to obtain a larger shoe. Following surgical treatment, approximately 10.6% of patients remain dissatisfied following surgical correction of their HV deformity. 1 A few investigators have discussed first metatarsosesamoid changes as the primary source of discomfort. Law et al 13 indicated that earlier surgery does not lead to higher complication rates, and surgeons may consider earlier surgery with the goal of realigning the sesamoids both statically and dynamically in their submetatarsal grooves as a possible way of improving surgical outcomes. Because of the cross-sectional nature of our study and lack of patient-reported outcomes, we were not able to determine if earlier intervention might result in less sesamoid-metatarsal osteoarthritis, or different crista volumes or better patient-reported outcomes. Recent clinical emphasis has been placed on correcting the triplanar deformity of the first metatarsal, including pronation. Our groups previous research suggests that sesamoid position may be an important component of the HV deformity that surgeons may need to consider during their surgical planning. 4 The potential relationship of sesamoid-metatarsal arthritis and crista volume as a source of preoperative pain or their relationship to postoperative patient outcomes requires further investigation.
There are clear limitations to this study. First, our study is limited by the small sample size of the HV patients (n=38) and normal control patients (n=10). A greater number of patients might reveal a relationship between first metatarsal pronation and crista volume or sesamoid station; our work is in line with previous work demonstrating no relationship between sesamoid position and pronation. Second, we performed a cross-sectional study. We cannot attribute causality with this study design. Additionally, we used 2 different types of WBCT scan devices including a standing device and performing simulated WBCT scans in a device that has been previously used and validated.2,7 This device difference may result in differences between sesamoid position between the 2 groups. Technically, the determination of first metatarsal pronation using strictly methods based on mass distribution (ie, inertial principal axes) would perhaps improve measures of pronation. However, point-picking methods to determine first metatarsal rotation have been previously used and were therefore adopted in the current work. Finally, the clinical implications of decreased crista volume are unclear as of this writing. Although it may be that decreased crista volume is developmental or is, alternatively, related to degenerative changes of the sesamoid metatarsal joint and sesamoid malposition and associated with increased pain and more debilitating symptoms, we could not study this with our approach.
Conclusion
In this article, we have shown in a relatively small cohort that increased IMA and HVA increases are associated with increased sesamoid station and decreased crista volume.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007211061363 – Supplemental material for The Association of Crista Volume With Sesamoid Position as Measured From 3D Reconstructions of Weightbearing CT Scans
Supplemental material, sj-pdf-1-fai-10.1177_10711007211061363 for The Association of Crista Volume With Sesamoid Position as Measured From 3D Reconstructions of Weightbearing CT Scans by Audrey J. Clarke, Stephen F. Conti, Matthew Conti, Amr A. Fadle, Scott J. Ellis and Mark Carl Miller in Foot & Ankle International
Footnotes
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.