
Abstract
Background:
There has been concern about lateral prominence pain at the osteotomy site following medial displacement calcaneal osteotomy (MDCO). However, no study has investigated this complication. This study aimed to investigate the incidence of lateral prominence pain following MDCO and examine the efficacy of crushplasty as a surgical technique to minimize this complication.
Methods:
This was a retrospective cohort study in which 137 patients (148 feet) who underwent MDCO were divided into 2 groups by whether they had concurrent crushplasty at the time of MDCO (crushplasty [n = 81] vs noncrushplasty group [n = 67]). Crushplasty was performed by flattening the bony step-off using a rongeur and bone impactor. Lateral prominence pain was defined as pain or irritating symptoms over the osteotomy site that persisted over 12 months after MDCO. The overall incidence of lateral prominence pain after MDCO and within each group was investigated. Multiple logistic regression analysis was used to determine the influence of possible risk factors on the development of postoperative lateral prominence pain.
Results:
The overall incidence of lateral prominence pain was 9.5% (14 of 148): 3.4% (3 of 87) in the crushplasty group, and 18% (11 of 61) in the noncrushplasty group, and χ2 analysis showed a statistically significant relationship between crushplasty and lateral prominence pain (P < .05). A relationship between the amount of medial displacement and the development of lateral prominence pain was observed in the noncrushplasty group (OR = 5.31, 95% CI 2.35-16.4, P < .05), but this was not observed in the crushplasty group (P = .641). The amount of medial displacement was an independent risk factor for the development of lateral prominence pain (OR = 2.72, 95% CI 1.54-4.79, P < .05), and concurrent crushplasty had a negative relationship with lateral prominence pain development (OR = 0.12, 95% CI 0.03-0.57, P < .05).
Conclusion:
This study revealed that lateral prominence pain is a significant complication of MDCO, especially in the setting of a larger displacement. The crushplasty following MDCO may minimize this complication, particularly when a greater degree of hindfoot correction is attempted.
Keywords
Introduction
Medial displacement calcaneal osteotomy (MDCO) is a frequently performed procedure to correct hindfoot valgus deformity caused by a variety of etiologies.3,4,7,8,14,17 This surgical procedure shifts the posterior calcaneus medially, which functionally realigns the axial vector of the Achilles and redistributes weightbearing load of the foot.2,5,11 Although there are several variations in operative techniques,1,6,9,12,15 an oblique lateral approach followed by single or double compression screw osteotomy fixation is most commonly employed.4,16
Because of the nature of the displacement osteotomy, the formation of a bony step-off along the lateral calcaneal wall after osteotomy fixation is inevitable. This step-off is more pronounced with a greater degree of displacement to achieve more significant heel alignment correction. Consequently, there has been a concern that a significant lateral step-off may be the source of postoperative pain due to compression of the sural nerve and overlying soft tissues.4,13,17 However, this lateral prominence pain has not yet been investigated as a complication following MDCO, and its true incidence is unknown.
“Crushplasty” has been previously described as a potential method to decrease lateral prominence pain by recontouring the step-off following osteotomy fixation. 13 The original authors argued this would provide a smoother and more anatomic lateral wall without having to compromise on medial displacement. However, the efficacy of crushplasty for preventing lateral prominence pain has not yet been reported.
This study aimed to investigate the incidence of lateral prominence pain following MDCO and determine the factors associated with its development. Additionally, the efficacy of concurrent crushplasty was assessed by comparing the incidence of postoperative lateral prominence pain. The authors hypothesized that unaddressed step-off following MDCO would be associated with postoperative lateral prominence pain, and that crushplasty would be a useful procedure to minimize this complication.
Methods
Establishing Study Cohort
The study protocol was approved by institutional review board, and informed consent was obtained from all patients under the Declaration of Helsinki. This study retrospectively reviewed prospectively collected data of consecutive patients who underwent MDCO in our institution between 2016 and 2018. All patients were indicated for MDCO in the setting of hindfoot valgus deformity because of a variety of associated diagnoses, including progressive collapsing foot deformity, accessory navicular syndrome, and ankle arthritis. These patients had isolated MDCO without undergoing any other concurrent calcaneal osteotomies (i.e., lateral column lengthening). Patients who underwent MDCO with compression screw fixation and completed minimum 1-year follow-up were included in the study cohort. Patients who (1) underwent MDCO with lateral step plate for osteotomy fixation, (2) had revision MDCO, (3) had incomplete follow-up, or (4) had a postoperative infection were excluded. In addition, patients who underwent concurrent lateral ligament repair, os trigonum excision, Haglund excision, and/or superior peroneal retinaculum repair were excluded because of the proximity of the lateral incision.
Ultimately, 148 feet in 137 patients remained for analysis after applying inclusion and exclusion criteria. Overall, the mean age of patients was 23.7 years (range, 19-51), and the mean body mass index (BMI) was 24.2 (range, 17.7-36.0). The mean follow-up was 17.2 months (range, 12-27). Patients were allocated into 2 groups (crushplasty group and noncrushplasty group) depending on whether they had concurrent crushplasty at the time of MDCO. Earlier in the study period, the senior author did not routinely perform the crushplasty. However, after encountering several patients with lateral prominence pain after MDCO, the procedure shifted to perform concurrent crushplasty routinely after osteotomy fixation. The crushplasty group consisted of 87 feet in 85 patients, with a mean age and BMI of 23.6 years (range, 19-51) and 24.2 (range, 17.7-32.9), respectively. The noncrushplasty group consisted of 61 feet in 59 patients, with a mean age and BMI of 24 years (range, 19-50) and 24.2 (range, 19.2-36), respectively. The demographic characteristics of both groups are tabulated in Table 1.
Demographic Characteristics of Each Group.
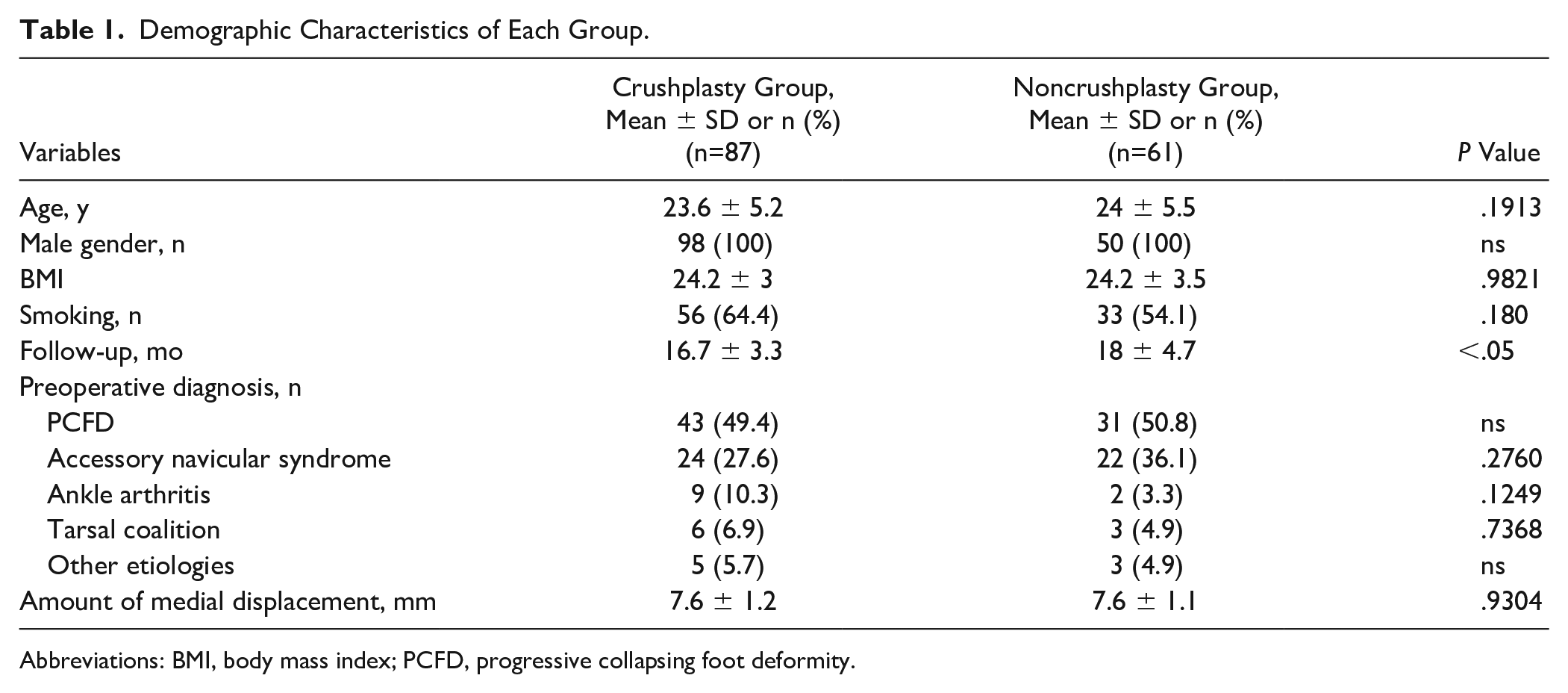
Abbreviations: BMI, body mass index; PCFD, progressive collapsing foot deformity.
The primary outcome of the current study was the presence of lateral prominence pain that persisted a year following the index MDCO. Lateral prominence pain was defined as pain and irritation over the osteotomy site caused by direct pressure from footwear and/or the floor, impairing daily activities. Pain was assessed through a binary question asked by the senior author—who was the treating provider—during patients’ postoperative clinical visits. Patients were asked whether they had the above-mentioned symptoms. If positive, this was followed by a physical examination to confirm the location of pain and to distinguish it from other potential etiologies, including sural neuritis, neuromas, lateral foot pain in other locations, such as the calcaneocuboid joint and fifth metatarsal base.
Crushplasty
After completion of osteotomy fixation, the sharp edge of the cortex of the lateral calcaneal wall was debrided with a rongeur, and the surface was flattened with a bone impactor and mallet (Figures 1 and 2). The surface of the osteotomy site below the incision was palpated along the surface to check whether it was smoothened adequately. Excised bony fragments were used as an autologous bone graft when there was a gap within the osteotomy site. If there was any prominence remaining, additional flattening was performed to confirm an even surface between the osteotomy site. Postoperatively, a short-leg splint was applied for 2-6 weeks, depending on the type of concurrent procedures. Tolerable weightbearing with crutches was followed, and full weightbearing was allowed after 6 weeks.
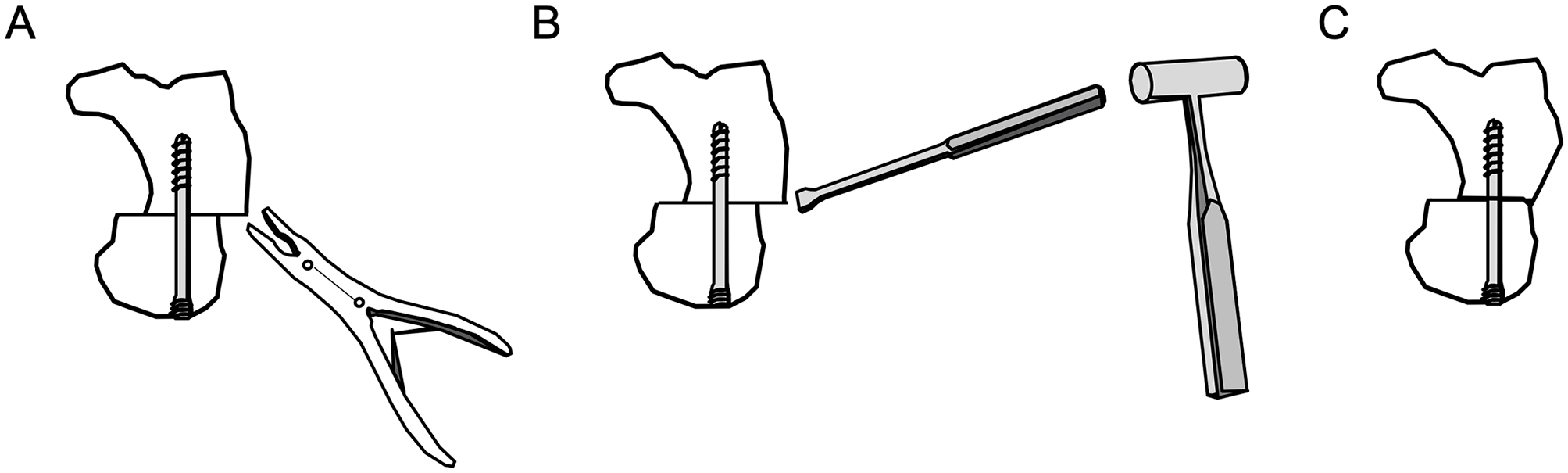
An illustration demonstrating crushplasty procedure. (A) After calcaneal osteotomy and fixation with a screw, the bony step-off was cracked down with a rongeur. (B) A bone impactor and mallet were used to flatten and recontour the lateral calcaneal wall. (C) After crushplasty, a smoother and more anatomic lateral calcaneal wall is identified.
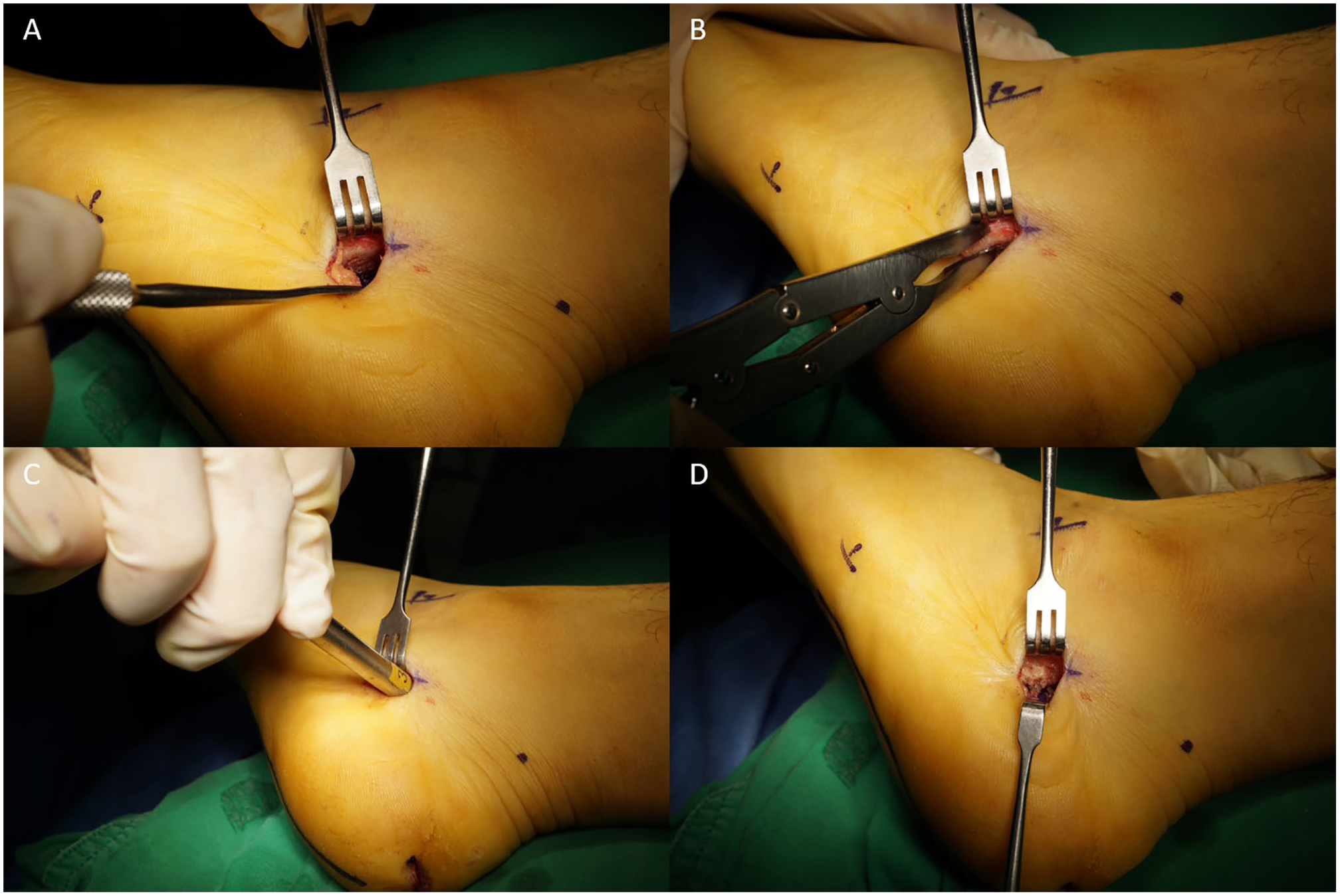
Intraoperative images demonstrating crushplasty procedure. (A) A significant amount of bony step-off after medial displacement calcaneal osteotomy. (B) The bony step-off is crushed down with a rongeur. (C) A bone impactor and mallet were used to flatten and recontour the lateral calcaneal wall. (D) A flattened, more anatomically contoured lateral calcaneal wall after crushplasty.
Measurement of the Amount of Displacement
To assess the association between lateral prominence pain and the amount of medial displacement performed, axial images from CT scans were evaluated. In our practice, the CT scan was routinely performed during the follow-up period to confirm the union of osteotomy and determine the time of weightbearing. The reason a CT scan was done as opposed to conventional radiographs was to confirm union rate in order to determine time to weightbearing in this young, active population for whom we allowed earlier weightbearing. A 64-channel multidetector CT scan (Brilliance 64, Philips Healthcare, Cleveland, OH) was used to obtain an axial CT image. The maximum distance between the most medial border of the medialized calcaneus to the contact point of the osteotomy was measured and recorded as the amount of displacement (Figure 3).
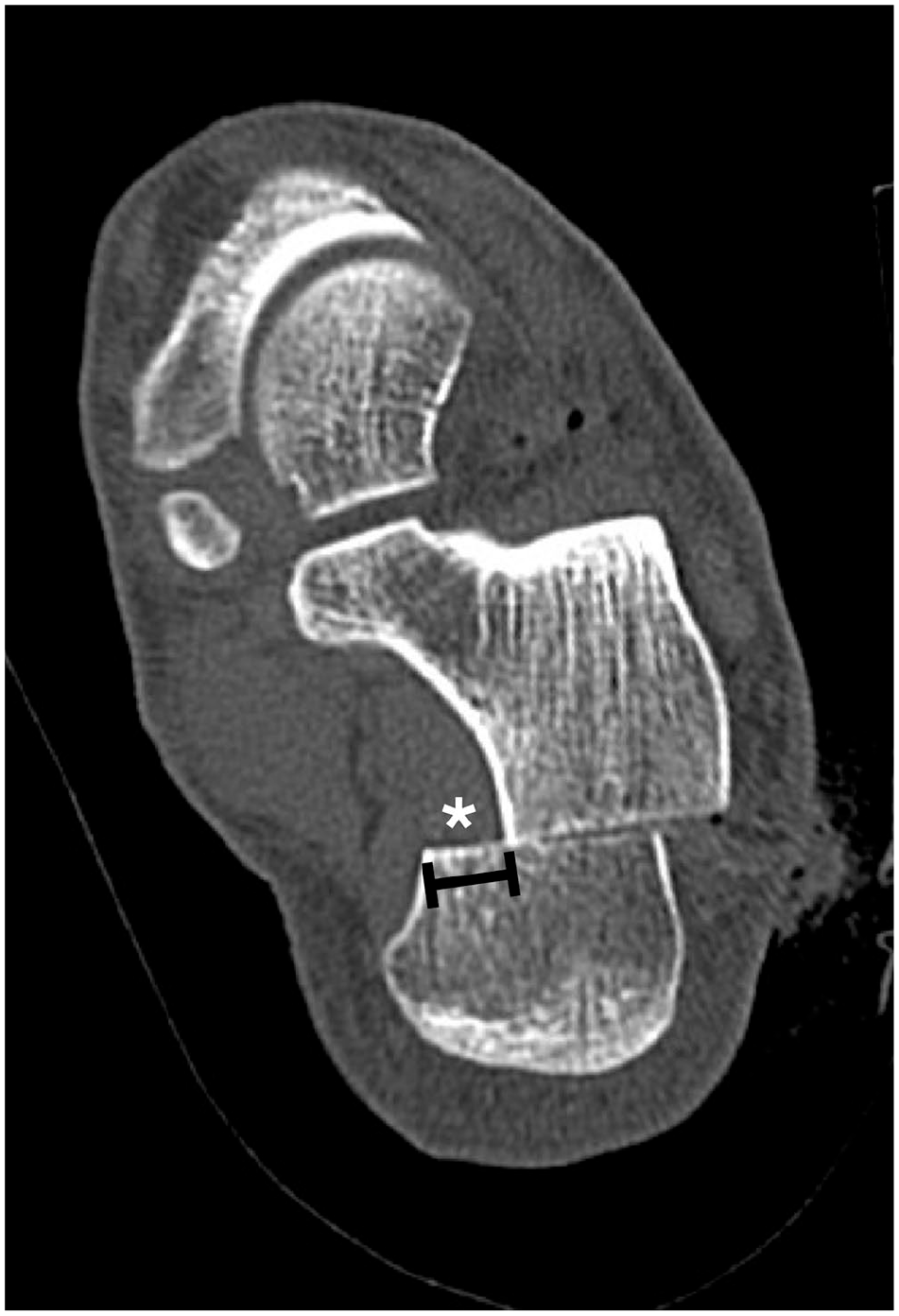
An axial CT image demonstrates the method of measuring the amount of medial displacement. The amount of the maximum distance between the most medial border of the medialized calcaneus to the contact point of the osteotomy was measured and recorded as the amount of displacement.
Statistical Analysis
Descriptive statistics are displayed as mean (range) for continuous variables and frequency (percentage) for categorical variables. Assessment of normality in the radiographic measurements of each group was performed using the Shapiro-Wilk test. The Student t test, χ2 test, and Fisher exact test were used to compare the 2 groups. A binomial logistic regression analysis was used to assess an association between the amount of medial displacement and the occurrence of lateral prominence pain within each group. The decision boundary of this curve was calculated and identified as the threshold of displacement, resulting in lateral prominence pain. Multiple logistic regression analysis was used to determine the influence of possible risk factors (age, BMI, smoking, amount of medial displacement, crushplasty) on the likelihood of having postoperative lateral prominence pain. Statistical significance was determined as a P value of less than .05. All statistical analysis was performed in Prism 8 for Mac (GraphPad Software, San Diego, CA).
Results
The overall incidence of lateral prominence pain was 9.5% (14 of 148): 3.4% (3 of 87) in the crushplasty group and 18% (11 of 61) in the noncrushplasty group (Figure 4). The incidence was significantly lower in the crushplasty group with an estimated odds ratio (OR) of 0.16 (95% CI: 0.05-0.58; P < .05).
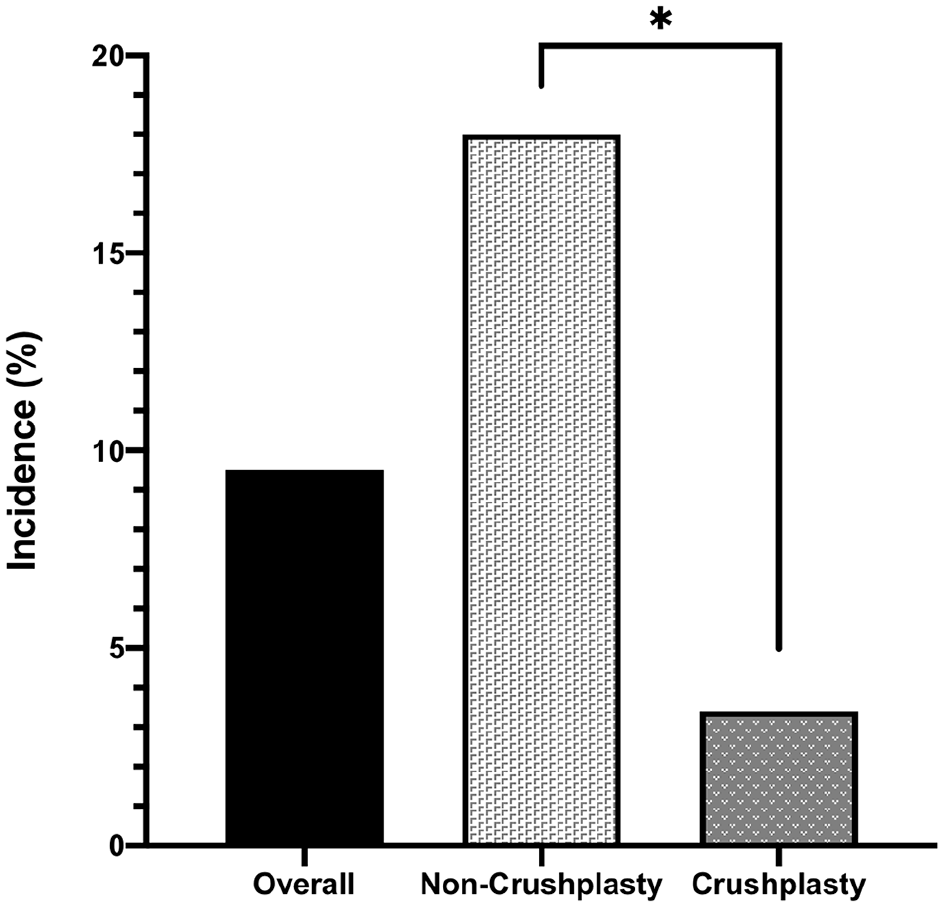
A bar graph shows the incidence of lateral prominence pain after medial displacement calcaneal osteotomy. *Statistically significant (P < .05).
Binomial logistic regression analysis revealed a positive relationship between the amount of medial displacement and the development of lateral prominence pain in the noncrushplasty group (OR=5.31, 95% CI: 2.35-16.4, P < .05). This relationship was not observed in the crushplasty group (P = .641). Multiple logistic regression analysis (Table 2) revealed that the amount of medial displacement was an independent risk factor for the development of lateral prominence pain with an OR of 2.72 (95% CI: 1.54-4.79, P < .05). A concurrent crushplasty was associated with a decreased likelihood of lateral prominence pain development (OR=0.12, 95% CI: 0.03-0.57, P < .05).
Multiple Logistic Regression Analysis for Development of Lateral Prominence Pain.
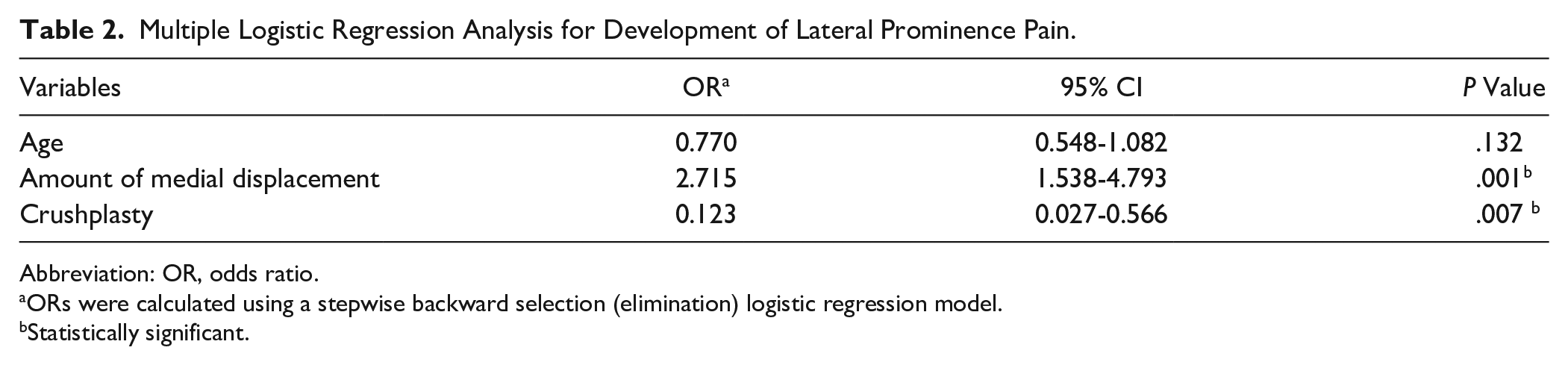
Abbreviation: OR, odds ratio.
ORs were calculated using a stepwise backward selection (elimination) logistic regression model.
Statistically significant.
The decision boundary analysis of the binomial regression showed that there was an increased likelihood of developing lateral prominence pain when the amount of medial displacement is made more than 10.8 mm (Figure 5).
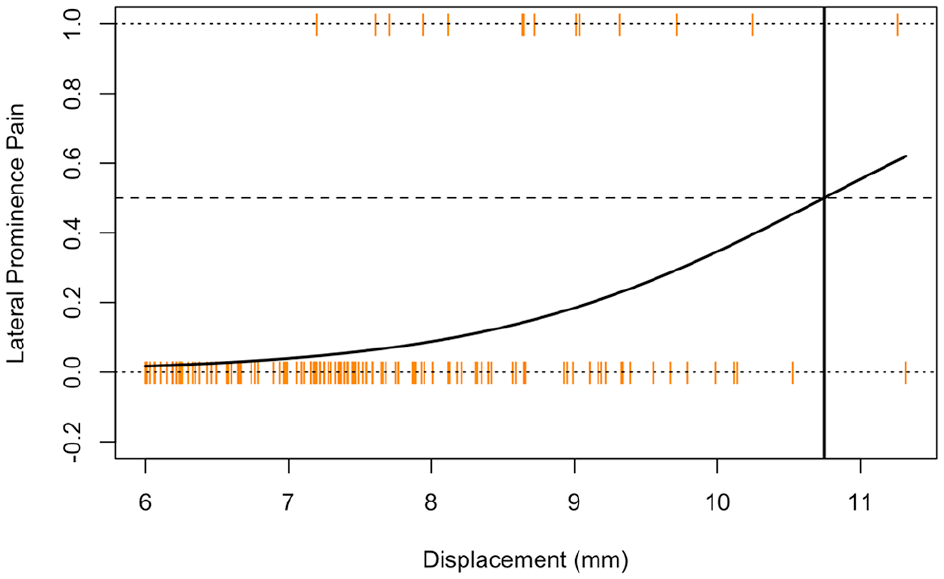
Binomial logistic regression of displacement vs lateral prominence pain with decision boundary at 10.8 mm.
Of 14 patients with lateral prominence pain, 3 from noncrushplasty group underwent additional ostectomy of the prominence because of prolonged symptoms despite lifestyle modification. This procedure was performed at an average of 13 months (range, 12-14) after the index MDCO. In these patients, lateral prominence pain relief was observed following the second operation.
Of note, there were no incidences of nonunion in the study cohort.
Discussion
This study investigated the incidence of lateral prominence pain following MDCO and assessed the efficacy of the crushplasty technique in preventing such a complication. The overall incidence of lateral prominence pain was 9.5% in the current study, with the crushplasty group demonstrating a significantly lower incidence of lateral prominence pain compared to the noncrushplasty group. In addition, the occurrence of lateral prominence pain was associated with a larger amount of correction in the noncrushplasty group, although this association was not observed in the crushplasty group. These findings suggest that step-off should be addressed to prevent postoperative lateral prominence pain when performing an MDCO, especially when a higher degree of hindfoot correction is made.
Among several approaches for performing a MDCO, a lateral approach with an oblique incision has been traditionally performed to guide the direction of the osteotomy. 4 However, with the osteotomy site just beneath the incision, concerns about the potential for soft tissue irritation and scarring due to the step-off created by medial displacement have been reported.4,10,13,17 In 1996, Schon and Bell introduced the crushplasty technique to prevent postoperative irritation over the lateral prominence after MDCO. 13 Since this original study, no reports to date have presented clinical results of crushplasty, and the incidence of lateral prominence pain following open MDCO. Furthermore, the efficacy of this preventive technique has been largely unexplored.
In the present study, the incidence of lateral prominence pain was 18% if the step-off was retained. Interestingly, this rate is consistent with reported rates of painful hardware removal of the lateral plate used for MDCO, which ranges from 0% to 21.4%.1,6,12 This suggests that lateral calcaneal wall irritation symptoms are significant enough to seek repeat surgery in order to alleviate pain and discomfort. Therefore, lateral prominence pain due to bony step-off should be considered a complication after MDCO with a lateral oblique incision.
It is important to note that although the rate was significantly lower than the noncrushplasty group, 3.4% of patients in the crushplasty group still exhibited lateral prominence pain. This raises suspicion that the etiology of lateral prominence pain may be multifactorial and not only caused by the bony step-off itself. However, we believe this pain is different from peroneal tendon irritation or sural nerve symptoms, as our surgical incision lies far beyond the course of these structures. We defined lateral prominence pain as pain prolonging more than 1 year after the index surgery to distinguish it from scar pain at the incision site (Figure 6). Although longer-term observations of this cohort may be warranted to further support our hypothesis, there is strong evidence that immediate pain relief in patients who underwent secondary surgery (ostectomy) suggests that the pain was mostly from the prominence itself (Figure 7).

Intraoperative image of the lateral calcaneal wall in a patient who had persistent lateral prominence pain and underwent secondary ostectomy to relieve the pain. Pain and irritation symptoms were located anterior and inferior to the incision site where osteotomy was performed, not the incision site. (Black arrowheads indicate the prominent area where the osteotomy was made, and the white arrowheads indicate callus formation due to continued irritation.)
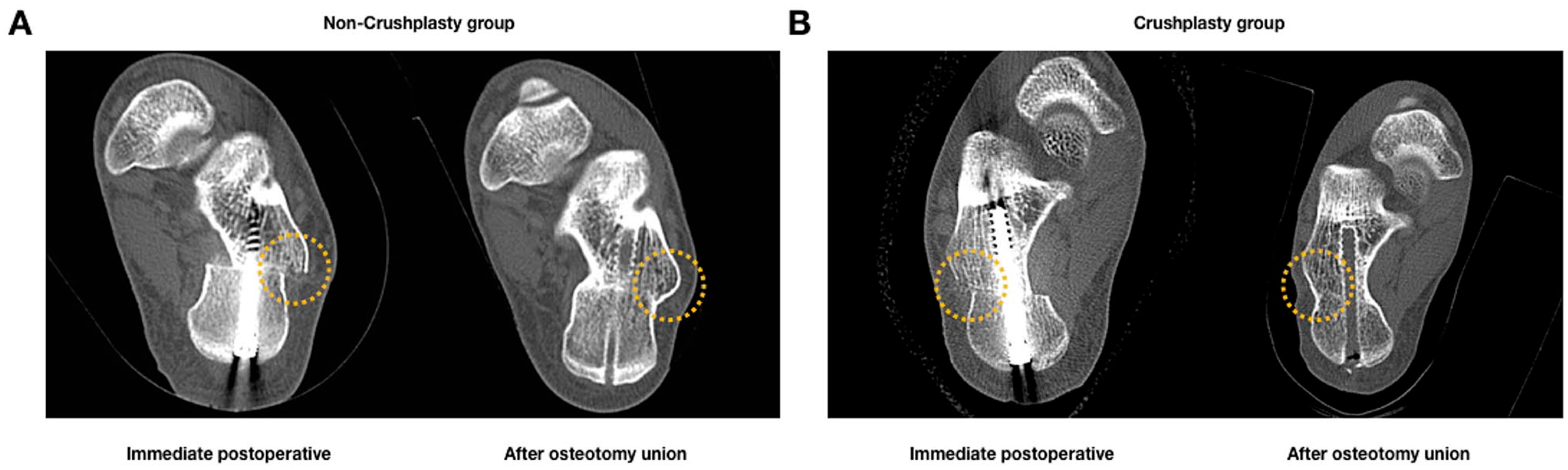
Computed tomography (CT) images are showing lateral calcaneal wall immediately after medial displacement calcaneal osteotomy and after osteotomy healing. (A) CT images of a patient in the noncrushplasty group. An immediate postoperative image (left) shows that a substantial ridge (bony step-off) along the lateral calcaneal wall is created after osteotomy. The bony step-off left a significant amount of prominence in the lateral calcaneal wall (right). (B) CT images of a patient in the crushplasty group. A smoother and anatomical contour of the lateral calcaneal wall is observed.
We found that a larger correction was associated with a higher occurrence of lateral prominence pain when crushplasty was not performed. This correlation was not observed in the crushplasty group. Further analysis confirmed that the amount of medial displacement was an independent risk factor for developing lateral prominence pain, and the predicted threshold for developing the pain was found to be 10.8 mm by our decision boundary curve. On the other hand, concurrent crushplasty was negatively associated with the development of lateral prominence pain. These findings suggest that when MDCO is performed in patients with severe hindfoot valgus, the step-off following osteotomy should be properly addressed to prevent postoperative lateral prominence pain.
The question remains whether there is a specific displacement cutoff where crushplasty will be most helpful. In this study, we did calculate a boundary of 10.8 mm in our cohort where crushplasty was most beneficial. However, this amount of displacement may not be a generalizable cutoff for surgeons to follow when deciding when to perform crushplasty, as the population of this study was relatively homogenous and does not reflect the average patient undergoing MDCO, and because the amount of displacement may differ between surgeons depending on their own experience. In general, a crushplasty may be most helpful when performing a notably larger than average amount of displacement, though the decision should ultimately be based on clinical judgment in the operating room. In the authors’ practice, a crushplasty is now performed in all patients undergoing MDCO because of the minimal harm and ease of this procedure.
Crushplasty detailed in this study is not technically difficult and can be easily reproduced. Moreover, this procedure can be performed without the use of electric devices such as a saw or burr. Although the original description of crushplasty suggested predrilling the cortex with a drill bit in younger patients with harder bones, 13 we found that debriding the bone edge with a rongeur and flattening it with an impactor was enough to reduce the prominence in our cohort of relatively young adults. However, caution is needed when managing osteoporotic bone in older patients. Although we have not experienced intraoperative fixation failure during crushplasty, we acknowledge the risk of loss of correction when tamping with a mallet and consider the use of electrical saws and burrs to reduce this risk in these cases.
Our study is not without limitations. First, this retrospective design did not include all patients who underwent MDCO within the study period, in order to control for potential overshadowing differential diagnoses of lateral bony prominence pain. However, we believe this study is the first to report the incidence of lateral prominence pain after MDCO, and the results will stimulate conversation about this issue. Additionally, this study is limited by the subjective nature of assessing the presence of lateral prominence pain, as we did not use an objective scale to rate lateral prominence pain. We chose not to use an objective scale because we believed the nature of this discomfort is unable to be fully captured in objective outcome measures owing to its specificity of location and symptoms. Despite this weakness, we believe it is necessary to report this type of discomfort and potential ways to avoid it. We also acknowledge that because only 3 of the 14 patients with lateral prominence pain elected to undergo subsequent ostectomy, the severity of pain may be called into question. However, we emphasize that all patients did report significant lateral prominence pain subjectively, and the decision to undergo ostectomy may have varied among patients after individual cost-benefit analysis of undergoing another surgery. There is also potential for observer bias since the senior author’s awareness of the lateral prominence pain may have increased throughout the study period, which led to a change in surgical practice. Next, the study population consists of patients of Asian cultural background, whose lifestyle incorporates frequent sitting in a crossed leg position, exposing the lateral calcaneal wall to direct floor contact pressure. Thus, the incidence may vary depending on the lifestyle of the patient cohort. However, this study suggests that crushplasty may help prevent lateral prominence pain and may be beneficial in patients whose lateral calcaneal wall is frequently exposed to the floor or the hard heel counter of the shoe. The lack of females in this study is another limitation. Additionally, although the examiner determined that the lateral prominence pain was not associated with sural nerve irritation based on the absence of symptoms such as tingling or burning, there is a possibility of nerve branch injury that existed concurrently with prominence pain or was not detected because the incision is located near a branch of the sural nerve. However, the resolution of symptoms following bone excision suggests that the symptoms were caused by bone protrusion rather than nerve irritation. Lastly, patient-reported outcome scores were not used for the analysis because of inhomogeneity of indications for MDCO. We believe that future prospective studies will help us understand the actual incidence of lateral prominence pain and its clinical impact.
In conclusion, this study suggests that lateral prominence pain can be a significant complication of MDCO, especially in the setting of a larger displacement. Concurrent removal of the bony step-off may prevent development of pain over the lateral calcaneus. We recommend performing crushplasty following MDCO to minimize these clinical symptoms, particularly when a larger amount of hindfoot correction is attempted.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007221108098 – Supplemental material for Incidence of Lateral Prominence Pain Following Open Medial Displacement Calcaneal Osteotomy and the Efficacy of Crushplasty as a Preventive Technique
Supplemental material, sj-pdf-1-fai-10.1177_10711007221108098 for Incidence of Lateral Prominence Pain Following Open Medial Displacement Calcaneal Osteotomy and the Efficacy of Crushplasty as a Preventive Technique by Jaeyoung Kim, Chul-Ho Kim, Jonathan Day, Jesse Seilern und Aspang, Lavan Rajan and Prashanth Kumar in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from Institutional review board of Armed Forces Medical Command (AFMC-19047-IRB-19-029).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.