
Abstract
Background:
We report the short-term outcomes of a retrospective cohort of Trabecular Metal total ankle arthroplasties (TAAs) via a transfibular approach from a single, nondesigner surgeon in Australia.
Methods:
This was a retrospective cohort study. Demographic, clinical, and patient-reported outcome measures (PROMs) were collected. The primary outcome was the Foot and Ankle Outcome Score (FAOS), and secondary outcomes included patient satisfaction, the EuroQol-5 Dimension (EQ5D), and complications including revision rates.
Results:
Between 2016 and 2019, 84 trabecular metal prostheses were implanted in 84 patients. Mean age (SD) at time of surgery was 68 (7.8) years, and 46 (55%) were male. Mean follow-up (SD) was 26.1 (13) months. There were significant (P < .001) improvements in the FAOS in the subscales of pain (47.9 to 79.1), activities of daily living (59.5 to 83.7), and quality of life (25.5 to 60.2) and EQ-5D (0.55 to 0.75) (P < .001), and overall satisfaction was 69.6%. The commonest complications were wound infection or breakdown (11.9%, n=10), fibular nonunion (3.5%), plate irritation (3.5%), and tibial nerve neuropathy (3.5%). There were no thromboembolic complications. Implant survivorship was 100%, with Trabecular Metal components retained in all patients. Two patients developed deep infection, with 1 requiring debridement and polyethylene exchange. No patients experienced implant loosening.
Conclusion:
Our results demonstrate that the trabecular metal survival rates are comparable with other total ankle implants in the Australian Orthopaedic Association National Joint Replacement Registry and as published in other international literature. Overall patient satisfaction was high, as were PROMs. However, the data highlight potential complications uniquely associated with this implant. The authors believe that these figures support TAA via a transfibular approach as a viable option in the treatment of ankle arthritis.
Level of Evidence:
Level IV, retrospective cohort study.
Introduction
Ankle arthritis is a common condition that is a major cause of chronic disability and decreased quality of life. 8 Historically, end-stage ankle arthritis has been managed with ankle arthrodesis. Recent advances in prosthesis design and surgical technique have meant that total ankle arthroplasty (TAA) has become a viable alternative with improved outcomes, function, and patient satisfaction equivalent or superior to arthrodesis.5,14,20,29 These improved outcomes have resulted in a growth in the popularity of TAA among both surgeons and patients. In Australia, a total of 374 TAAs were performed in 2020, which is an increase of 29.4% since 2019 and 141.3% since 2014. 1
Despite this recent increase in use of TAA, there is a paucity of literature examining these newer-generation prostheses, one of which is the Zimmer Trabecular Metal Total Ankle Implant (Zimmer-Biomet, Warsaw, IN). This is a non-mobile-bearing prosthesis with highly cross-linked polyethylene, inserted via a transfibular approach. Only a small number of studies have examined the efficacy of this prosthesis and approach, which has demonstrated promising early clinical results, but most of these studies were by surgeons involved in the design or otherwise affiliated with the implant.2,3,21-23
We present a single Australian surgeon’s early clinical experience with this implant. It is to our knowledge the largest cohort reported by authors without affiliation to the manufacturer. The aims of this study were to determine the early functional outcomes, patient satisfaction, and complication rates in a consecutive cohort of patients with end-stage ankle arthritis managed with the Zimmer Trabecular Metal Total Ankle Implant via the transfibular approach.
Methods
Patient Selection
This study was performed as a retrospective cohort study with surgeries performed between 2016 and 2019. Cases were retrieved from practice management records using procedure item codes and hardware order details.
Patients were included for analysis and approached for follow-up based on the following criteria: adults (>18 years) diagnosed with end-stage osteoarthritis of the ankle by the participating orthopaedic surgeon, and those elected to undergo a total ankle replacement after failing nonoperative management. Patients were excluded from the study if they had osteonecrosis of the talus that precluded the use of TAA, previous TAA or ankle arthrodesis, neuropathic arthropathy, active or prior infection, or a compromised soft tissue envelope.
Patients were initially contacted for consent and follow-up by phone, with subsequent opt-out consent obtained by electronic communication of study information for their data to be accessed and for their contributions to follow up. Research ethics approval was granted (St Vincent’s Hospital Sydney, HREA 2020/ETH01444 and 2020/ETH00615).
Surgical Procedure
In all patients, the Zimmer Trabecular Metal Total Ankle (Zimmer-Biomet, Warsaw, IN) prosthesis was used. This is a 2-component, semiconstrained, fixed-bearing prosthesis with highly cross-linked polyethylene on a metal bearing surface. All surgeries were performed by the senior author, a fellowship-trained orthopaedic surgeon with extensive TAA experience, across multiple academic institutions, using the standard operative technique as per manufacturer’s recommendations as previously described.3,21 Any concomitant procedures that were required to achieve a balanced prosthesis and a plantigrade foot were performed concurrently. Postoperatively, patients were placed in a well-padded short-leg backslab and kept nonweightbearing. Prophylaxis against thromboembolic complications was low-molecular-weight heparin (enoxaparin) 40 mg subcutaneously daily in hospital followed by rivaroxiban 10 mg oral daily until 2 weeks postoperatively. At 2 weeks postoperatively, weightbearing was initiated in a walking boot and ankle range of motion exercises were commenced. At 6 weeks, patients were instructed to gradually wean out of their boot and physiotherapy was encouraged.
Data Collection and Outcome measures
Preoperative baseline demographics, comorbidities, ankle arthritis etiology, and Canadian Orthopaedic Foot and Ankle Society (COFAS) 12 classification were collected as part of routine clinical practice along with patient-reported outcome measures (PROMs) using paper scores, that were converted to electronic format for the analysis using a custom form (Google Form, Google LLC, Palo Alto, CA). Data retrieval from the practice management system (Genie v9.4.2; Genie Medical Solutions, Fortitude Valley, QLD, Australia) was performed retrospectively and transferred into a spreadsheet also matched using identifier codes to the study record. The COFAS classification for end-stage ankle arthritis severity 12 was retrospectively graded from electronic retrieval of the baseline radiograph, reviewed by a single observer. Follow-up PROMs were collected electronically, with patients contacted via email with a link to a form without identifiable information included. A code was used to match the form responses to a study record. If patients were unable to use a computer, they were followed up with phone interviews by a surgical trainee, with patient verbal responses transcribed through the form (4 patients used this method to complete the follow-up questionnaire). Surgical outcomes (adverse events, reoperation, and revision) were also retrieved by manual chart review and were recoded using previous published guidelines on reporting TAA adverse events.26,28
The primary outcome was the Foot and Ankle Outcomes Score (FAOS). It is a region-specific questionnaire that is used in the measurement of many foot and ankle pathologies including ankle arthritis. 16 It contains 42 questions divided into 5 subscales: pain, symptoms, activities of daily living (ADLs), sports and recreational activities, and foot- and ankle-related quality of life (QoL). Patients respond to each question on a scale from 0 to 4, with each subscale ranging from 0 to 100 (in which a lower score reflects a worse outcome). 19
Global function was measured as a secondary outcome using the EuroQol 5-dimension, 5-level (EQ-5D-5L) quality of life questionnaire. 10 The EQ-5D-5L is a generic tool for measuring quality of life, describing health in terms of 5 dimensions: mobility, self-care, usual activities, pain and discomfort, and anxiety and depression. Patients respond to each item on a 5-level range of severity, following the format of no problems, slight problems, moderate problems, severe problems, and unable to or extreme problems. The EQ-5D-5L has been shown to have good validity and discriminatory power in a range of chronic health conditions, 11 including ankle osteoarthritis. 15 Patient satisfaction was analyzed using a 5-point Likert scale with the patient asked, “If you had to spend the rest of your life with the symptoms you have right now, how would you feel about it?" as has previously been described. 29 Satisfaction was analyzed both as a 5-level ordinal outcome and as a binary outcome, with scores of 1-3 points grouped as “dissatisfied” and scores of 4-5 points grouped as “satisfied.”
Data and Statistical Analysis
Surgical outcomes (complication, reoperation, and revision) text descriptions retrieved from chart review were graded according to Younger et al 28 and the incidence summarized. Subscale scores were calculated for the FAOS as described in Herdman et al, 10 and the EQ5D Index using UK normative data. 6
Missing Data
Missing data for FAOS subscales (pain, symptoms, ADL, QoL) and EQ-5D Index (EQ-5D Index-pre) and BMI were imputed with sequential chained equations based on partial mean matching drawing on a pool of 3 nearest neighbors (k) for a total of 20 (m) imputed data sets. The sequence was BMI, FAOS, and EQ5D. Posterior estimates of model parameters were obtained using sampling replacement (bootstrap). The variables included in the imputation model were:
Age at surgery (years)
Sex (male; female)
Complication status (yes/no)
Comorbidity status (yes/no): Defined as to whether any of the listed condition appears as part of the included conditions on the Charlson Comorbidity Index
Duration from first case (days): The difference between the date of surgery and the first surgery in the series
COFAS grade (1-4)
Surgery to follow-up (days): The difference between the date of follow-up and the date of surgery
Timepoint (baseline; follow-up)
The imputation process was performed using the mi function of Stata (Stata SE, v16.1; StataCorp LLC, College Station, TX, USA). The imputed data were used for the primary analysis assuming that missingness occurred at random (MAR).
Descriptives for continuous variables were reported using means and standard deviations; counts and proportions were reported for categorical variables. Complications were recoded using published guidelines,26,28 and a Kaplan-Meier survival curve (with 95% CIs) was generated. The imputed PROMs data were modeled using mixed effects models (1 per subscale) with patient ID as a random factor, with adjustment for the following variables:
Age at surgery (years)
Sex (male; female)
Comorbidity status (yes/no):
COFAS grade (1-4)
Surgery to follow-up (days)
Timepoint (baseline; follow-up)
OA diagnosis (yes/no)
The mi estimate: mixed functions were used (Stata SE v16.1, StataCorp LLC) with each model fit under conditions of residual maximum likelihood. Alpha was set at 0.05 assessing model estimates.
Results
Between 2016 and 2019, a total of 84 unilateral TAAs were performed, with 80 patients providing consent to participate. The mean (SD) follow-up was 26 (13) months. Patient demographics are summarized in Table 1. Seventy-four patients provided preoperative PROMs data. Sixty-nine patients provided pre- and postoperative PROM data. All 80 consented patients were assessed for complications and reoperation.
Characteristics of patient cohort.
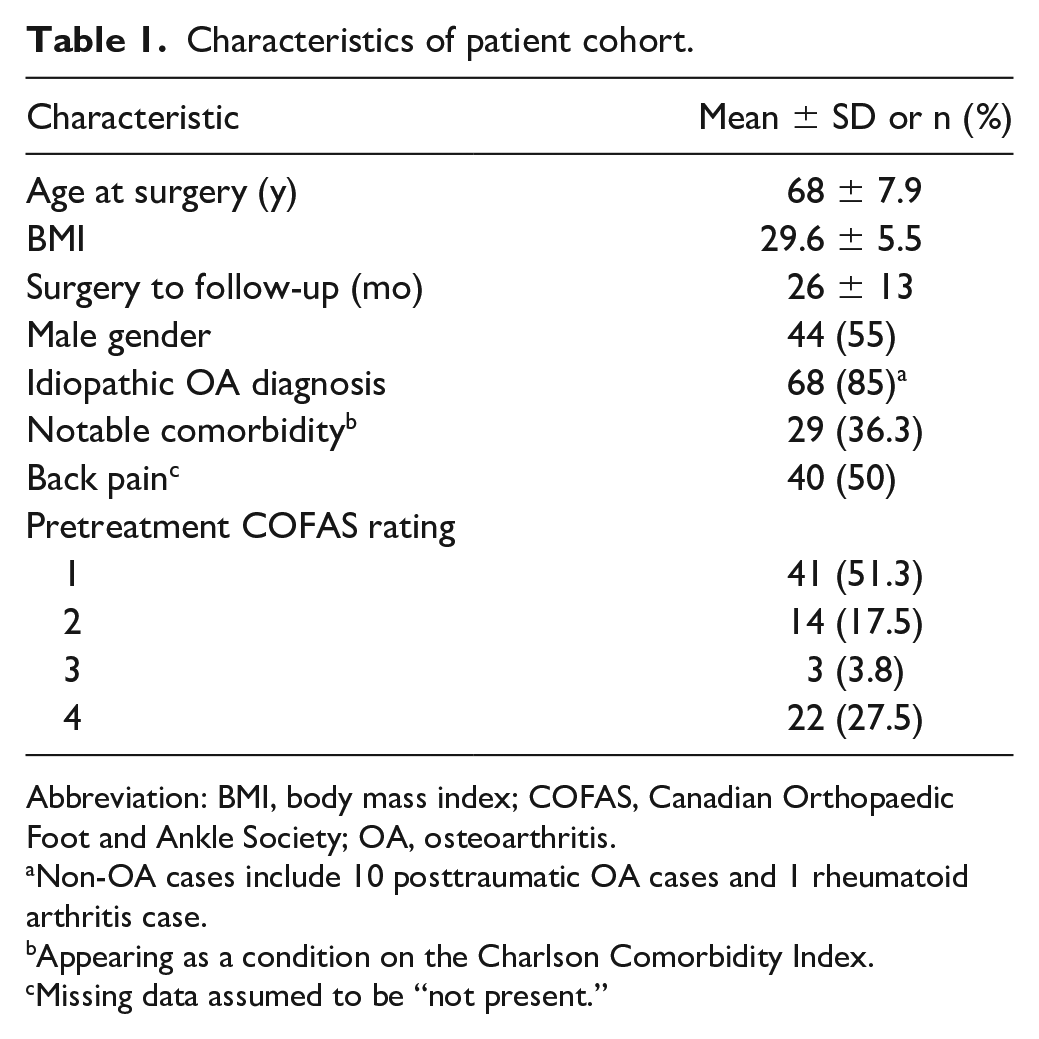
Abbreviation: BMI, body mass index; COFAS, Canadian Orthopaedic Foot and Ankle Society; OA, osteoarthritis.
Non-OA cases include 10 posttraumatic OA cases and 1 rheumatoid arthritis case.
Appearing as a condition on the Charlson Comorbidity Index.
Missing data assumed to be “not present.”
Patient-Reported Outcomes
Patient-reported outcomes were characterized by statistically significant improvements in FAOS subscales and EQ5D Index (Table 2) between baseline and follow-up when adjusted for covariates, with larger improvements in FAOS pain and QoL compared to symptoms and ADL subscale scores. Patient satisfaction indicated that 69.6% were somewhat or very satisfied with their outcome (Figure 1).
Summary of PROMs at Baseline and Follow-up, With Change Scores Adjusted for Covariates. a
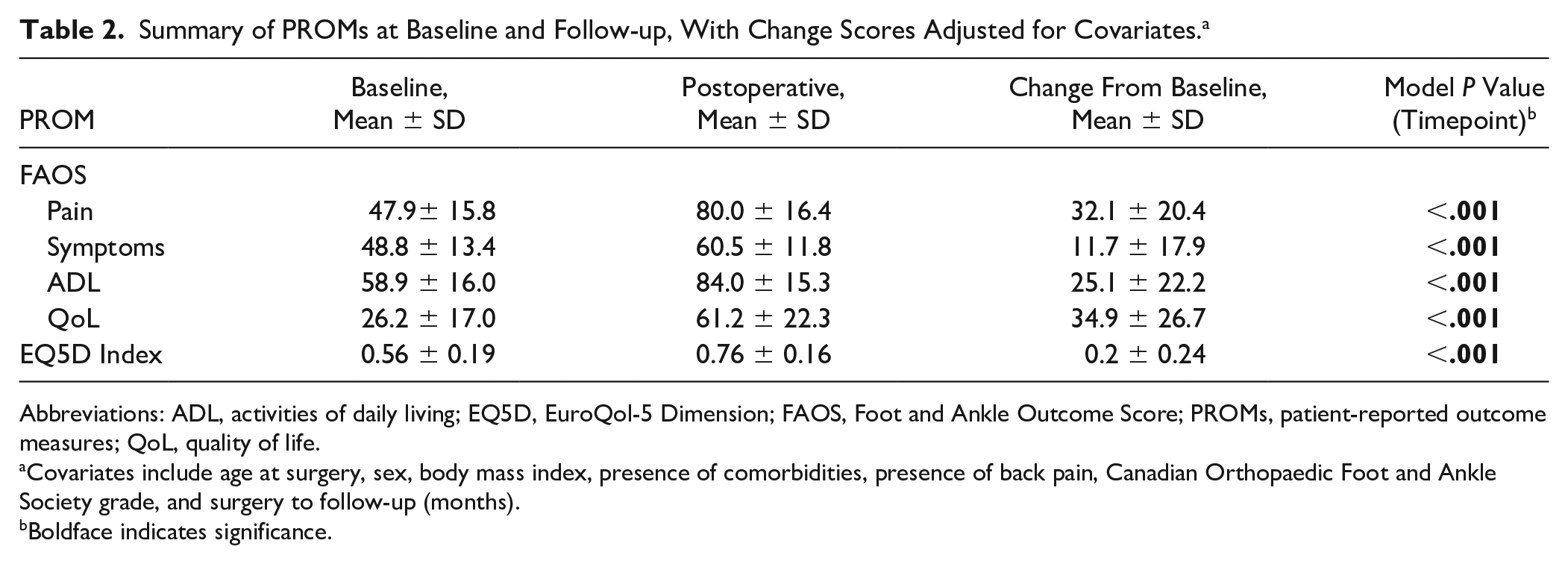
Abbreviations: ADL, activities of daily living; EQ5D, EuroQol-5 Dimension; FAOS, Foot and Ankle Outcome Score; PROMs, patient-reported outcome measures; QoL, quality of life.
Covariates include age at surgery, sex, body mass index, presence of comorbidities, presence of back pain, Canadian Orthopaedic Foot and Ankle Society grade, and surgery to follow-up (months).
Boldface indicates significance.
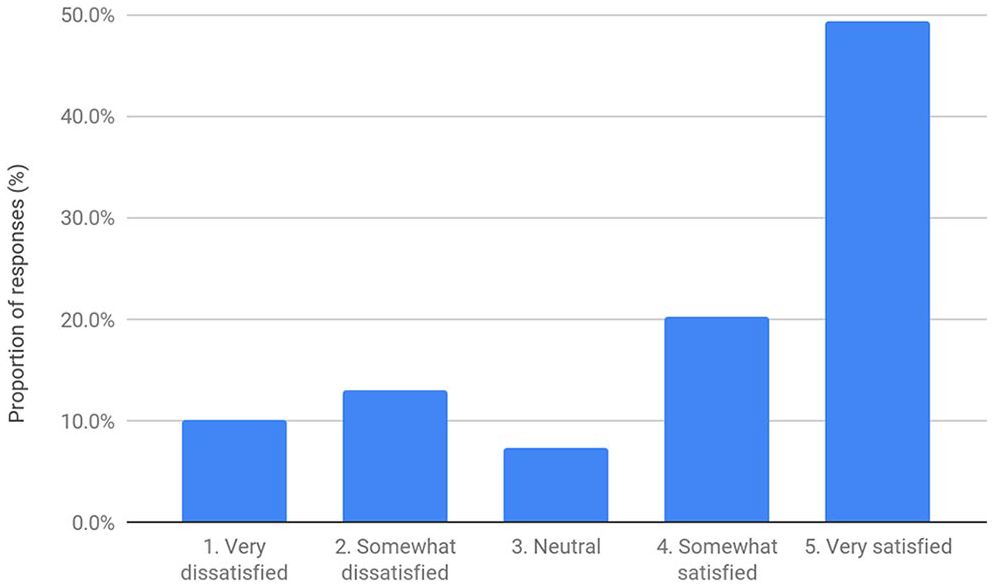
Breakdown of satisfaction at follow-up.
Adverse Events
There were no instances of thromboembolic events. Adverse events related to surgery were detected in 22 cases (overall incidence 27.5%) at a median of 4.9 months (interquartile range 1.7-13.5). They were most commonly treated with operative debridement for superficial infection and hardware removal related to TAA (Table 3). Kaplan-Meier survival curve for all-cause adverse events requiring additional surgery is shown in Figure 2. Overall implant survival as defined by retention of the trabecular metal components was 100%. One patient experienced deep infection of the TAA within the first month postoperatively. This was managed with polyethylene exchange and retention of the metal implant followed by long-term antibiotic therapy, which was successfully ceased 1 year later.
Number of COFAS FAI Complication Grades in Patients With a Documented Adverse Event (n = 22).
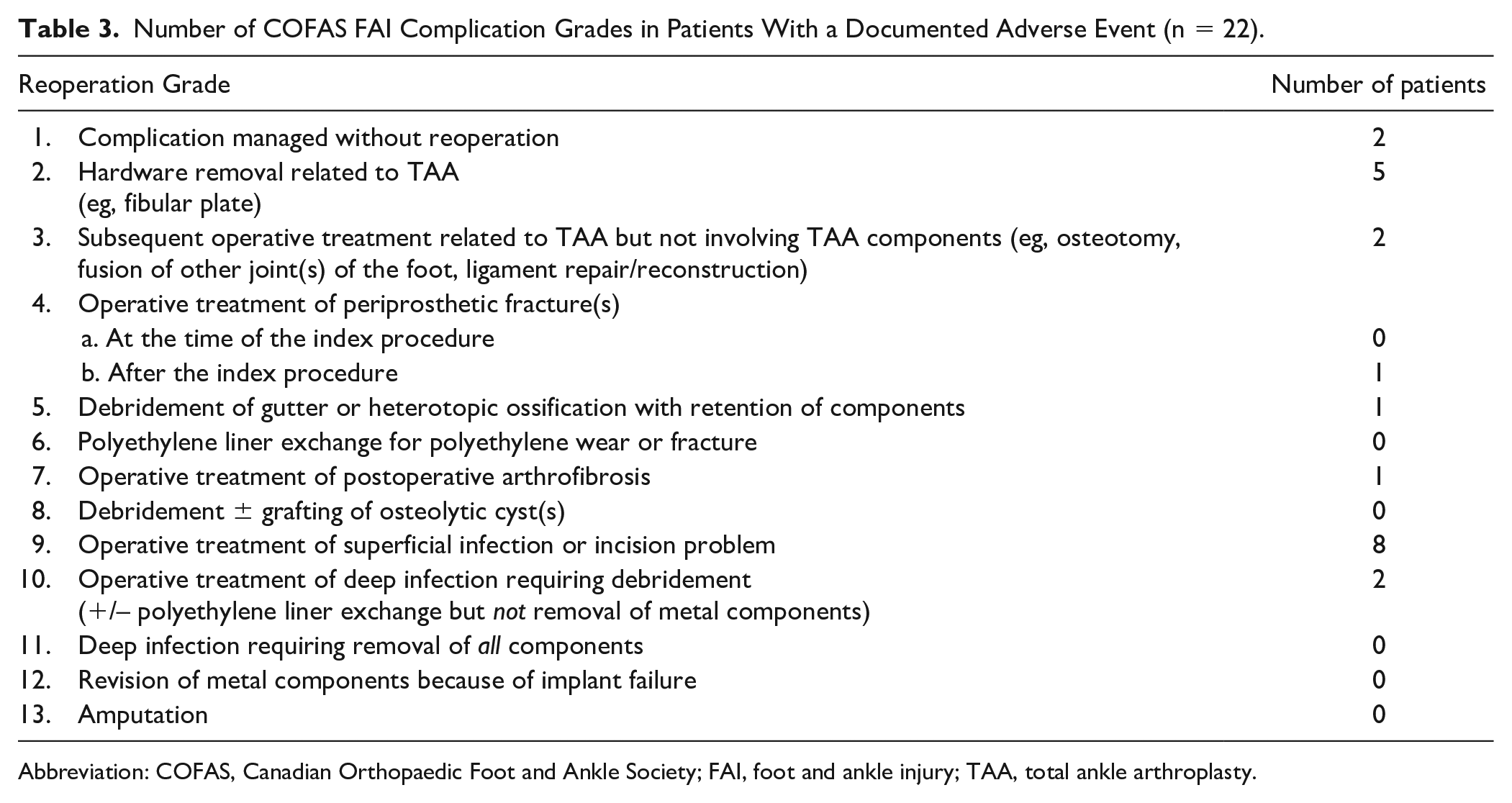
Abbreviation: COFAS, Canadian Orthopaedic Foot and Ankle Society; FAI, foot and ankle injury; TAA, total ankle arthroplasty.
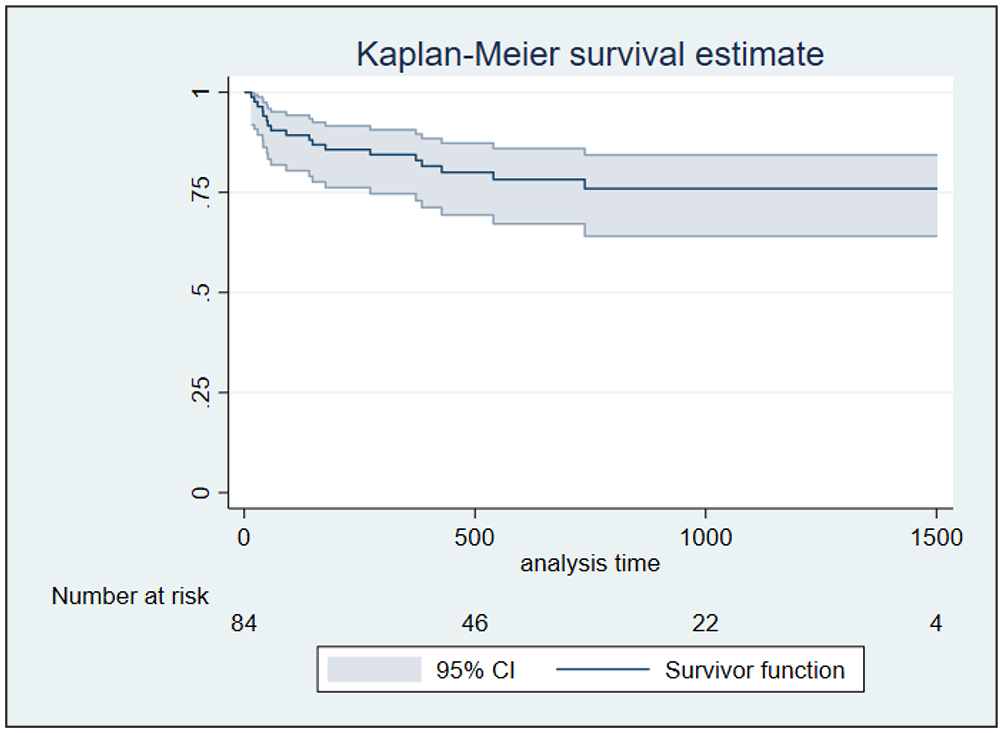
Kaplan-Meier survival curve for all-cause complications requiring additional surgical intervention with 95% CIs.
Discussion
To our knowledge, this is the largest retrospective cohort and the only study without author affiliation to the implant manufacturer. It represents ~95% of all Trabecular Metal implants recorded in Australia during the time period. 1 Overall, outcomes were satisfactory, with modest improvements in PROMs and acceptable rates of adverse events.
PROMS are increasingly important as a metric of surgical success, and some subscales of the FAOS appear to have utility for monitoring change in patient-reported outcome following surgery for ankle arthritis. 16 In this study, there were significant improvements in FAOS scores and the EQ-5D. FAOS subclass scores significantly improved for pain, ADLs, and QoL. Since the implant’s US Food and Drug Administration approval in 2012, 6 studies have sought to clarify its potential benefits, in which the visual analog scale (VAS) pain questionnaire was the predominant PROM used. Barg et al 2 recorded significantly greater improvements in VAS scores following TAA with this implant than other studies. Whether the VAS can be reliably compared to the inverse FAOS pain subscale is unclear. The FAOS pain subscale assesses a patient’s pain according to frequency, as well as severity while performing 8 movements relevant to activities of daily living. These data therefore offer a more detailed assessment of pain than the VAS. 9
This study adds new knowledge on outcome subscales other than pain. The FAOS functional subclasses of ADLs and QOL saw modest improvements. The FAOS symptoms subscale scores improved to a lesser magnitude than other subscales’. This is consistent with previous literature demonstrating the comparatively poorer responsiveness of the symptoms subscale to surgery for ankle arthritis in general. 16 The specific contribution of this implant’s unique design to functional and symptomatic outcomes remains unclear, and future comparative studies are needed.
Recently, there has been increased interest in using patient satisfaction as a discrete measure of operative outcome in joint replacement surgery.17,18,27,29 Our patients’ satisfaction scores were mostly positive, with 70% somewhat satisfied or very satisfied with surgery. This is similar to the findings of Bianchi et al, 3 who reported 91% patients were satisfied or very satisfied, and Tiusanen et al, 22 who reported 65% being very satisfied with the implant. There remains room for improvement in patient satisfaction, which may be influenced by implant design, setting patient expectations appropriately and avoiding adverse outcomes.
Overall, our adverse event rate was 26% (n=22) and the reoperation rate was 23% (n=20). The majority of these were low-grade, requiring minimal surgical intervention. This reoperation rate is comparable to the previously cited literature for this implant (18%-25%) and to overall TAA reoperation rates (17%). 13 Tan et al 21 assessed for early complications in 20 consecutive patients over 18 months, noting a 21% reoperation rate. Our implant survivorship as defined by retention of metallic prosthesis was 100% and including polyethylene exchange was 99% at an average of 26 months. This is comparable to previously studied cohorts.
In our cohort, wound complication or infection resulted in reoperation in 11.9% cases (n=10). Major wound complication requiring flap coverage was required in 2 patients; however, the prosthesis was not involved and it was retained. One of these patients had risk factors for wound issues postoperatively, because of long-term corticosteroid use for polymyalgia rheumatica and Hashimoto thyroiditis. Despite the need for additional intervention, both patients were very satisfied with the procedure at follow-up. One patient experienced early postoperative infection at a tibial jig pin-site that resolved with surgical debridement. To our knowledge, this is the first recorded complication related to this guide’s pin-sites.
Despite the theoretical benefits, it remains unclear whether the lateral approach to TAA is superior to the traditional anterior approach with regard to wound-related complications. Barg et al 2 experienced a 7% wound complication rate via a transfibular approach. One retrospective cohort study has demonstrated no significant difference in infection between transfibular and traditional anterior approaches at 1 year. 24 Another retrospective cohort study found an increased reoperation rate via the lateral approach (odds ratio 6.1); however, the majority of these reoperations were for prominent fibula hardware rather than infection. 7
Complications related to the fibula osteotomy present a clear disadvantage to this surgical technique. Of the 3 fibular osteotomy nonunions, 2 were instances of late fibula plate fracture requiring reoperation and 1 instance of radiographic nonunion managed nonoperatively. The latter patient was very dissatisfied with their outcome. All 3 nonunions were in patients who were nonsmokers and nondiabetic. Fibula union was found to be near-universal in previous studies.2,3,21 Barg et al 2 assessed fibula union clinically and radiographically and observed no instances of delayed or nonunion, with the latest fibula healing occurring at 18 weeks. Bianchi et al 3 reported 1 instance of fibula nonunion requiring bone grafting without any predisposing risk factors. Symptomatic, noninfected fibular plates were removed for 3 of our patients (4%) similar to the experience of Tan et al 21 (15%) and Gagne et al 7 (33%). In a retrospective comparative study, Usuelli et al 25 demonstrated significantly improved incidence of plate removal and wound dehiscence by using a modified fibular osteotomy, allowing for fixation with screws alone and obviating the need for a plate. Our surgical technique did not include this practice. Future improvements may include employing Usuelli et al’s 25 lag screw technique, intramedullary fibula nail fixation, or a lower-profile plating option.
Three patients experienced tibial nerve neuropathy, a complication that has not previously been described. These symptoms manifested as plantar pain or numbness in the distribution of the medial and lateral plantar nerves. Two patients underwent subsequent tarsal tunnel release with improvement of their symptoms. The third was managed conservatively with symptoms slowly improving over an 18-month period. These patients all underwent significant correction of varus deformity. The authors therefore recommend intermittent relaxation of retractors during preparation of bony cuts as well as consideration of prophylactic tarsal tunnel release when correcting significant varus deformity.
One of the proposed advantages of the transfibular approach is a theoretically reduced risk of iatrogenic medial malleolar fracture. We experienced 1 medial malleolar fracture at day 40 postoperation requiring ORIF and 1 medial malleolar stress fracture at 7 months postoperatively managed conservatively with a walking orthosis. These fractures were spontaneous and their etiology unclear, although it is conceivable that the earlier fracture represents an unrecognized intraoperative complication. The literature reports only 1 previous case of medial malleolar fracture with this implant, sustained intraoperatively and recognized as an ankle dislocation on day 1 postoperatively. 3 Our recommendation would be to exercise caution during the far-side resection and regular checking of saw depth in the anteroposterior plane with fluoroscopy.
We experienced no cases of symptomatic loosening at a mean follow-up of 26.1 months. This is equivalent to Tan et al’s 21 finding of zero cases of implant failure at a mean follow-up of 18 months. Barg et al’s 2 longer follow-up (mean 26 months) observed radiolucency of the tibial component in 35% of the patients with a 5% revision rate for aseptic loosening of the tibial component. The lack of clinically relevant implant loosening in our cohort—the largest so far studied with this implant—appears promising.
This study is not without limitations. First, this is a single-surgeon retrospective study; however, it is the largest nondesigner series and represents 95% of the Trabecular Metal implants used in Australia during the study period. Second, we have only assessed short-term outcomes (~26 months); nevertheless, this is a newer-generation prosthesis and patients will continue to be followed. Third, we did not include radiologic evaluation to assess for loosening; however, this will form the basis of future research. The mixed methodology (telephone with an interviewer, vs electronically self-administered) for delivering postoperative patient-reported outcome measures may inflate some ratings of function or satisfaction because of interviewer or social desirability bias; however, this is expected to be relatively minor if present as all except 4 patients completed the outcome measures electronically.
We chose to use the FAOS as a multidimensional index of pain, function, and quality of life. However, this outcome measure has not been extensively validated in this patient population, and we therefore advise caution when interpreting our PROM findings. 4 A recent assessment of the FAOS for ankle arthritis found that the symptoms subscale was not responsive to change after surgery, and ceiling effects were observed in the sports/recreation subscale. 16 However, the remaining subscales performed at least moderately well regarding construct validity, internal consistency, and responsiveness to change. The minimal clinically important difference for FAOS scores in the setting of ankle arthritis has not been fully established and would be a useful benchmark to assess the clinical utility of the results.
Furthermore, our study did not ask patients about their expectations prior to surgery. Studies in hip and knee arthroplasty have shown that when preoperative expectations are met, patients are more likely to be satisfied, whereas unmet expectations and dissatisfaction often lead to litigation.9,17,18 Patients undergoing TAA have been found to harbor higher expectations prior to TAA surgery than than those undergoing arthrodesis, with expectation more likely to be met by TAA. 28 It may have therefore been useful to assess satisfaction in this context. Finally, future prospective, comparative studies are required to better investigate the differences between transfibular TAA and traditional TAA and arthrodesis.
Our results demonstrate that the Trabecular Metal TAA implant is safe and effective in achieving acceptable PROMs and patient satisfaction. Complication and implant survival rates are comparable to previous international literature on the Trabecular Metal and other TAA implants. Importantly, the results highlight potential complications uniquely associated with this implant. The authors believe that these figures support TAA via a transfibular approach as a viable option in the treatment of ankle arthritis.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007221131818 – Supplemental material for Early Clinical Outcomes and Complications of Transfibular Total Ankle Arthroplasty: The Australian Experience
Supplemental material, sj-pdf-1-fai-10.1177_10711007221131818 for Early Clinical Outcomes and Complications of Transfibular Total Ankle Arthroplasty: The Australian Experience by Ellery Clugston, Nalan Ektas, Corey Scholes, Michael Symes, Alex Wilton, Andrew Wines and Rajat Mittal in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andrew Wines reports grants or contracts and institutional funding for teaching workshops from Zimmer Biomet. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.