
Abstract
Background:
Intraoperative evaluation of hindfoot alignment is one of the factors that may affect outcomes for foot and ankle reconstructive surgery. The present study was performed to evaluate the effect of simulated weightbearing fluoroscopy on the intraoperative assessment of hindfoot alignment reconstruction.
Methods:
The medical records of patients diagnosed with disorders of the foot and ankle with abnormal hindfoot alignment were retrospectively reviewed from November 2014 to November 2021. Hindfoot alignment view (HAV) fluoroscopy in the simulated weightbearing position and HAV radiographs were routinely recorded during and after surgery, respectively. The hindfoot alignment angle (HAA) and hindfoot alignment ratio (HAR) were measured on intraoperative and postoperative images, respectively.
Results:
Seventy-two women and 82 men (155 ankles) with a mean age of 45.48 years were included in the present study. The intraobserver and interobserver reliabilities of the HAA and HAR measurements were satisfactory. The intraoperative and postoperative HAA was −0.7 ± 4.8 degrees and −0.2 ± 5.0 degrees, respectively. The mean HAR on intraoperative fluoroscopy and postoperative radiographs was 37.4% ± 19.7% and 40.4% ± 18.2%, respectively. Simple regression analysis revealed a correlation between the intraoperative and postoperative HAA (R2 = 0.631, P < .001) and HAR (R2 = 0.262, P < .001). Univariate analysis suggested that the difference between the intraoperative and postoperative HAA was positively affected by the body mass index (P < .001).
Conclusion:
The present study showed that intraoperative HAV fluoroscopy in the simulated weightbearing position is a potentially useful method to predict postoperative hindfoot alignment in the weightbearing position. Patients with a lower body mass index had smaller HAA deviations between intraoperative and postoperative measurements of hindfoot alignment.
Level of Evidence:
Level IV, retrospective case series.
Keywords
Introduction
Hindfoot malalignment is associated with many foot and ankle disorders, 16 such as excessive subtalar pronation, restricted subtalar motion, malunion of triple arthrodesis, instability, and impingement syndrome. Appropriate treatment is essential to restore foot and ankle function and improve patients’ quality of life.9,14 Conservative treatment includes shoe modification, physical therapy, and biomechanical orthotic therapy. 18 Surgical reconstruction is an effective method to correct malalignment; techniques include realignment osteotomy, ligament reconstruction, tendon transfer, and arthrodesis.6,17-19
Thorough intraoperative evaluation may help to correct hindfoot alignment and achieve satisfactory surgical outcomes.1,5,12 Intraoperative assessment of coronal hindfoot alignment includes visual inspection, anteroposterior (AP) fluoroscopy, hindfoot alignment view (HAV) fluoroscopy with simulated weightbearing, navigation, and pedobarography.1-3,13,15,16 Visual inspection depends on the surgeons’ experience and often lacks reliability. Routine AP fluoroscopy of the ankle joint is limited because of the superimposition of bones, precluding the acquisition of distinct images for surgeons to determine hindfoot alignment. To better observe the osseous anatomy, simulated weightbearing HAV fluoroscopy was developed for quantitative assessment of hindfoot alignment during surgery.
The HAV, described by Saltzman and El-Khoury and modified by Cobey, is considered the gold standard for evaluating hindfoot alignment.4,5,11,16,20 Several scholars have applied HAV fluoroscopy in the simulated weightbearing position during foot and ankle surgery, showing that this technique may be useful for intraoperative assessment of hindfoot alignment. Jeon et al 8 retrospectively compared hindfoot alignment between preoperative standard HAV and intraoperative HAV fluoroscopy in patients without hindfoot pathology. They reported no significant difference in hindfoot alignment between the preoperative standing radiograph and intraoperative fluoroscopy findings. A short-term retrospective analysis by Boffeli et al 1 showed that intraoperative simulated weightbearing lateral fluoroscopy was a valuable method to predict postoperative sagittal plane alignment in patients undergoing flatfoot reconstructive surgery. However, few studies have investigated the consistency between intraoperative simulated weightbearing fluoroscopy and postoperative weightbearing radiographs in patients undergoing hindfoot alignment reconstruction surgery. The clinical value of intraoperative HAV fluoroscopy in reflecting postoperative hindfoot alignment remains unknown. Therefore, the present study was performed to evaluate the effect of simulated weightbearing fluoroscopy on the intraoperative assessment of hindfoot alignment reconstruction. We hypothesized that only slight deviation of hindfoot alignment is present between intraoperative simulated weightbearing HAV fluoroscopy and postoperative weightbearing radiographs.
Methods
Patients
We retrospectively reviewed the medical records of patients diagnosed with foot and ankle disorders with abnormal hindfoot alignment at our hospital from November 2014 to November 2021. Angles of 0-5 degrees, less than 0 degrees, and more than 5 degrees between the tibial axis and the calcaneal axis indicated normal hindfoot alignment, varus, and valgus, respectively. Patients who underwent surgery with hindfoot alignment correction and had complete follow-up data were included in our study. The patients’ data were gathered, including demographic information, diagnosis, surgical management, and radiologic evaluation.
HAV Acquisition
The HAV radiograph was routinely recorded during and after surgery for each patient. Intraoperative HAV fluoroscopy in the simulated weightbearing position was performed after completion of definitive correction procedures for hindfoot alignment (Figure 1). The patient lay on a radiolucent table in the supine position. A radiolucent L-shaped plate was used to keep the foot in a neutral position. The vertical part of the plate was closely placed on the plantar surface of the affected foot. Manual pressure was loaded onto the plastic plate in the cranial direction to keep the foot in a neutral position. The C-arm (Siremobil Compact L, Cios Spin, Cios Select S5, and ARCADIS Orbic 3D; Siemens Healthineers, Erlangen, Germany) was placed at an approximately 20-degree caudal angle in the sagittal plane. Each patient’s intraoperative fluoroscopy images were exported for routine recording. Full weightbearing radiographs at 12 weeks postoperatively were obtained according to the standard Saltzman method. The postoperative radiographs were acquired and analyzed using a picture archiving and communication system.

The illustration of intraoperative hindfoot alignment view fluoroscopy in the simulated weightbearing position.
Leg rotation seriously affects the accuracy of hindfoot alignment judgment. During the operation, we routinely performed standard AP fluoroscopy to evaluate leg rotation before performing HAV fluoroscopy. The lateral tibia overlapped approximately 10% to 20% of the width of the fibula, indicating no significant rotation of the lower leg. The projection of the second toe appeared on the medial side of the midline of the tibial projection if there was no adduction or abduction deformity of the foot. Intraoperative HAV fluoroscopy was performed in the same position without obvious leg rotation.
Assessments
To investigate the effect of simulated weightbearing fluoroscopy on the assessment of hindfoot alignment during reconstructive surgery, the hindfoot alignment angle (HAA) and hindfoot alignment ratio (HAR) were measured on intraoperative HAV fluoroscopy in the simulated weightbearing position and postoperative HAV radiographs in the weightbearing position, respectively. The measurement methods for the HAA and HAR are displayed in Figures 2 and 3. The HAA was defined as the angle between the tibial axis and the calcaneal axis. Two horizontal lines were drawn at the level of the narrowest segment and the widest distal segment of the calcaneus. At the narrow level, the line was divided equally by a point. At the wide level, the line was divided by another point in a ratio of 3:2, with a longer tibial segment and a shorter fibular segment. The calcaneal axis was determined by the above 2 points. The tibial axis was represented by a line parallel to the tibia. The HAR was defined as the ratio of the medial segment width to the calcaneus width. The calcaneus width was divided by the tibial axis to obtain the medial segment. A positive and negative HAA indicated hindfoot valgus and varus, respectively.
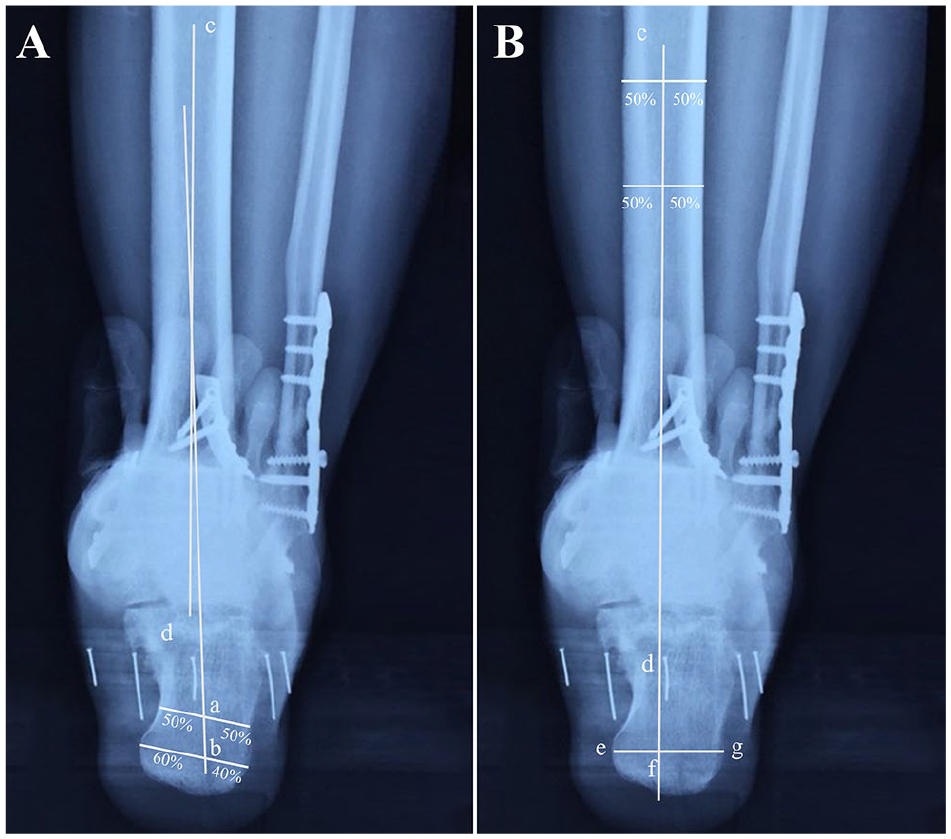
The demonstration of measurement methods of the hindfoot alignment angle (HAA) and hindfoot alignment ratio (HAR). (A) The HAA was defined as the angle between the tibial axis and the calcaneal axis. Two horizontal lines were drawn at the level of the narrowest segment and the widest distal segment of the calcaneus. At the narrow level, the line was divided equally by point (a). At the wide level, the line was divided by point (b) in a ratio of 3:2, with a longer tibial segment and a shorter fibular segment. The calcaneal axis was determined by the above two points (line ab). The tibial axis was represented by a line parallel to the tibia (line cd). The HAA was the angle between line ab and line cd. (B) The HAR was defined as the ratio of the medial segment width (line ef) to the calcaneus width (line eg). The calcaneus width was divided by the tibial axis to obtain the medial segment (line ef). The HAR was calculated as the ratio of line ef to line eg.
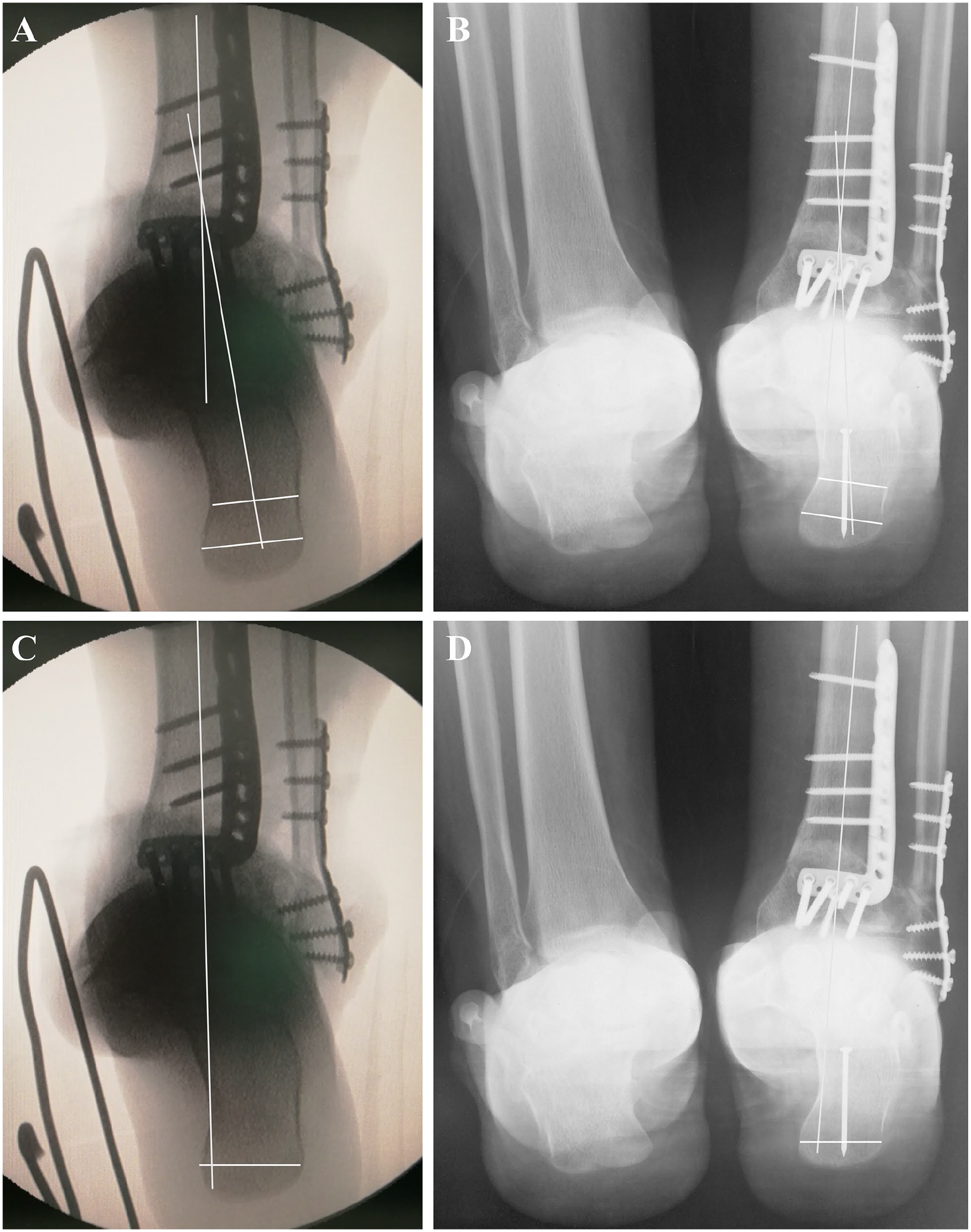
A male patient underwent supramalleolar osteotomy to correct hindfoot alignment. The small deviation of hindfoot alignment angle and hindfoot alignment ratio between intraoperative HAV fluoroscopy in the simulated weightbearing position (A and C) and postoperative HAV radiographs in the weightbearing position (B and D) were displayed. HAV, hindfoot alignment view.
The measurements were performed by 2 experienced foot and ankle surgeons and examined by 1 senior surgeon. The intraobserver and interobserver reliabilities were assessed by intraclass correlation coefficients. Thirty images were randomly selected from the database. All surgeons were asked to measure the HAA and HAR twice at a 2-week interval.
The HAA and HAR of intraoperative HAV fluoroscopy in the simulated weightbearing position vs those of postoperative HAV radiographs in the weightbearing position were compared to determine the effect of intraoperative fluoroscopy on evaluation of hindfoot alignment in reconstructive surgery. The univariate analyses and multivariate regression analyses were performed to determine the influence of different variables on the assessment effect, including body mass index (BMI), diagnosis, operation type, and weightbearing time.
Statistical Analysis
Statistical analyses were performed using SPSS software (version 19.0; IBM Corp, Armonk, NY). Intraclass correlation coefficients were used to assess intraobserver and interobserver reliabilities. The Kolmogorov-Smirnov test was applied to determine data normality. Simple regression analysis was performed to understand the relationship between intraoperative and postoperative images regarding the HAA and HAR. Univariate analyses and multivariate regression analyses were performed to determine the effect of variables on the differences between intraoperative and postoperative images. P values of <.05 were considered statistically significant.
Results
Patient characteristics
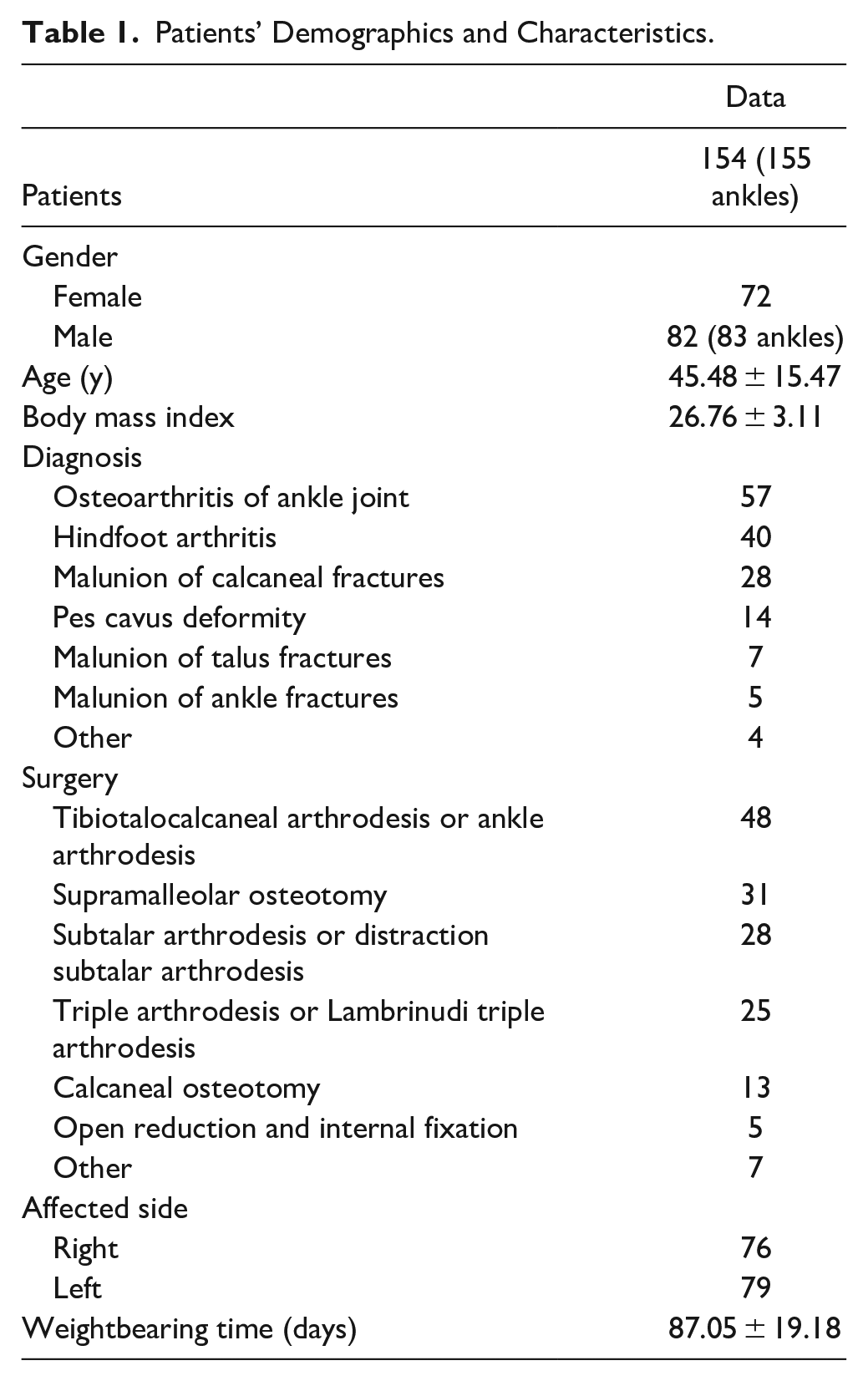
The patients’ demographic information is displayed in Table 1. In total, 154 consecutive patients (72 women, 82 men; 155 ankles) with a mean age of 45.48 years were included in the present study. The mean follow-up was 87.05 days. The diagnoses and operations in the study cohort are shown in Table 1.
Patients’ Demographics and Characteristics.
Radiographic Measurements
The intraobserver and interobserver reliabilities of the HAA and HAR were satisfactory (Table 2). The results of the Kolmogorov-Smirnov test showed that the data of our study accorded with the normal distribution (Table 3). The mean difference in the HAA between intraoperative fluoroscopy and postoperative radiographs was 2.5 ± 2.0 degrees. The intraoperative measurement (HAA = −0.7 ± 4.8 degrees) was slightly more inclined to varus than the postoperative radiographs (HAA = −0.2 ± 5.0 degrees). Simple regression analysis showed a close correlation between the intraoperative and postoperative HAA (R2 = 0.631, P < .001). The results of the univariate analysis suggested that the difference between the intraoperative and postoperative HAA was positively affected by the BMI (P < .001). The HAA deviation was not affected by diagnosis (P = .235), surgery type (P = .275), and weightbearing time (P = .696).
The Intraobserver and Interobserver Reliabilities.
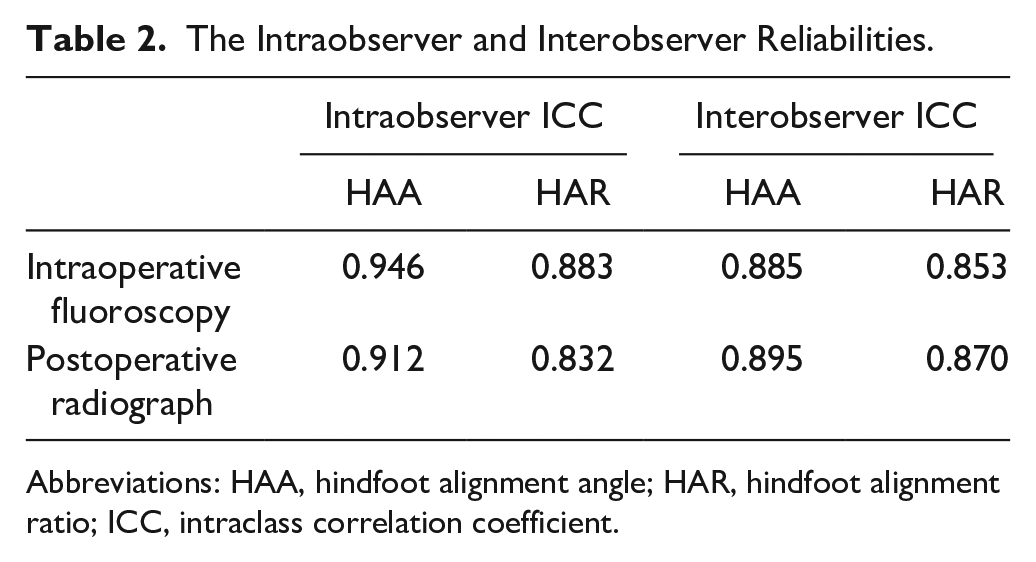
Abbreviations: HAA, hindfoot alignment angle; HAR, hindfoot alignment ratio; ICC, intraclass correlation coefficient.
The Results of Kolmogorov-Smirnov Test.
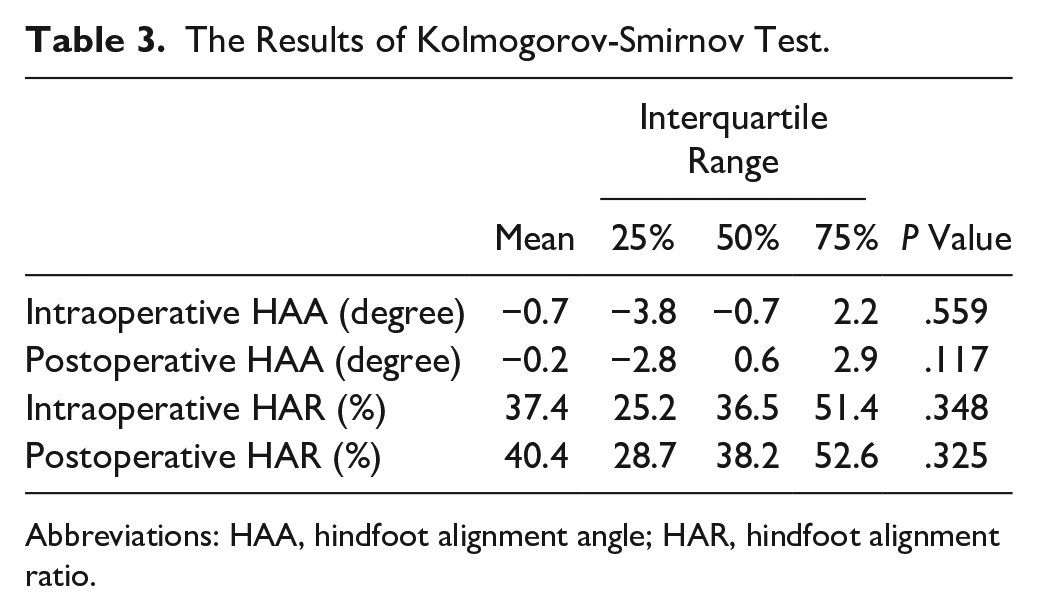
Abbreviations: HAA, hindfoot alignment angle; HAR, hindfoot alignment ratio.
The mean HAR on intraoperative fluoroscopy and postoperative radiographs was 37.4% ± 19.7% and 40.4% ± 18.2%, respectively. A correlation (R2 = 0.262, P < .001) was found between the intraoperative and postoperative HAR according to simple regression analysis. The difference between the intraoperative and postoperative HAR was affected by the BMI (P = .030) and diagnosis (P = .031) in the univariate analysis. However, the effects of the BMI and diagnosis disappeared in the multivariate regression analysis (P = .132 and = .069). The HAR deviation was not affected by surgery type (P = .287) and weightbearing time (P = .486).
Discussion
The current study showed that the mean differences in the HAA and HAR between intraoperative fluoroscopy and postoperative radiographs were slight. Our results suggest that intraoperative HAV fluoroscopy in the simulated weightbearing position is an effective method to predict postoperative hindfoot alignment in the weightbearing position. Furthermore, the accuracy of prediction was related to the BMI. The difference in the HAA between intraoperative fluoroscopy and postoperative radiographs was smaller in patients with a lower BMI.
The significance of hindfoot alignment in reconstructive surgery is nonnegligible for foot and ankle surgeons. However, accurate measurement of hindfoot alignment during surgery is challenging. Although navigation, pedobarography, and hindfoot alignment guide instruments were introduced to intraoperatively measure hindfoot alignment, these novel methods have not been widely applied because of their high costs, low applicability, and high radiation exposure.1-3,13,15,16 HAV fluoroscopy with simulated weightbearing is still a potentially effective method in the operation room. Previous studies have shown that intraoperative HAV fluoroscopy is a valuable method to understand hindfoot alignment and predict postoperative sagittal alignment.1,8 However, there is a paucity of studies investigating the measurement consistency of hindfoot alignment between intraoperative simulated weightbearing fluoroscopy and postoperative weightbearing radiographs in reconstruction surgery.
The results of the current study suggest that intraoperative HAV fluoroscopy with simulated weightbearing is an effective method to predict postoperative hindfoot alignment with acceptable differences. Foot and ankle surgeons can gain an understanding of the effect of hindfoot alignment correction through simulated weightbearing fluoroscopy in the operation room. In our experience, our preferred C-arm placement can reduce the difference between intraoperative and postoperative measurements. Theoretically, the C-arm must be tilted about 20 degrees caudally and as close to the affected foot as possible. Slight differences may eventually affect the accuracy of the hindfoot alignment measurement. In addition, to obtain a standard image, AP fluoroscopy should be routinely performed to understand leg rotation. Matuszewski et al 12 performed a cadaveric experiment to determine the radiographic landmarks that may help surgeons to identify rotation. The authors found that a 50% to 100% overlap of the fibula over the fifth metatarsal base was a reliable indicator of 0 to 5 degrees of valgus. From our experience, AP fluoroscopy should be routinely performed as a standard image to understand leg rotation. The lateral tibia overlapped approximately 10% to 20% of the width of the fibula, indicating no significant rotation of the lower leg. The projection of the second toe appears on the medial side of the midline of the tibial projection if there is no adduction or abduction deformity of the foot. HAV fluoroscopy should be performed in the same position without obvious leg rotation.
Furthermore, we investigated the influence of the BMI, diagnosis, operation type, and weightbearing time on the measurement consistency in this study. The results revealed no significant correlation of the diagnosis, operation type, or weightbearing time with deviation of the HAA or HAR measurement. This result demonstrates that intraoperative HAV fluoroscopy with simulated weightbearing is a general method in foot and ankle surgery and is not limited by the above factors. However, the results also indicated that the patients with a lower BMI had a smaller difference between the intraoperative and postoperative HAA. Consistent intraoperative fluoroscopy may be difficult to obtain for patients with a higher BMI. In addition, the distance between the hindfoot and radiolucent plate of patients with a higher BMI is longer than that in patients with a lower BMI, which may cause differences in magnification and image distortion. We usually take radiographs with a postoperative Saltzman view after bony union and full weightbearing. During the interval from the operation to the postoperative radiographs, patients who undergo too-early postoperative weightbearing and improper rehabilitation may develop hindfoot alignment change and measurement deviation. These effects may be more pronounced in patients with a high BMI because their ankles sustain larger stresses and because of the adverse effects of weight and excessive soft tissue. Previous studies have demonstrated that the BMI has a great influence on the alignment of the lower limb. Krushell and Fingeroth 10 reported that obese patients tended to develop varus changes in the lower limbs after total knee arthroplasty. Another study showed that patients with a high BMI were more likely to have abnormal alignment than nonobese patients after total knee arthroplasty. 7 However, the small sample size and retrospective design of our study did not seem to provide strong enough evidence to interpret the relationship between the BMI and HAA deviation. Prospective controlled trials with larger sample sizes are necessary.
Our results suggested a weak correlation (R2 = 0.262, P < .001) between the intraoperative and postoperative HAR. Although the statistical outcomes were nonideal, we believe that potential clinical significance remains, considering the approximate values of the mean HAR in the intraoperative and postoperative measurements (37.4% ± 19.7% and 40.4% ± 18.2%). We assumed that intraoperative fluoroscopy with simulated weightbearing may not be an efficient tool but is a helpful method to understand the correlation between the intraoperative and postoperative HAR. Considering these findings combined with the ideal results of the HAA, we believe that intraoperative fluoroscopy with simulated weightbearing is still a meaningful method for intraoperative assessment of hindfoot alignment. However, prospective studies are required to better evaluate the HAR.
This study had several limitations. First, the retrospective design of the study inherently led to research bias and weakening of the accuracy of the present findings. Second, the C-arms used in the operation room were different in our study. It is difficult to avoid the influence of different equipment on measurement results. However, almost all C-arms used during surgery were of the same brand, and the errors generated by qualified medical equipment are acceptable. Third, the follow-up time was controversial. Long-term follow-up is conducive to obtaining more accurate results regarding ankle function. However, full weightbearing, high activity levels, and other uncontrollable factors may change the hindfoot alignment during long-term follow-up. In clinical practice, the patients were asked to start weightbearing walking around 12 weeks after surgery. Although patients may distribute body weight as incomplete appropriate posture because of pain and swelling when taking HAV radiographs, we believe that hindfoot alignment at 12 weeks postoperatively without full weightbearing and strenuous exercise may effectively reflect the intraoperative situation. Fourth, the method of eliminating leg rotation was not standardized, which may have led to research bias. We used intraoperative AP fluoroscopy to evaluate leg rotation and ensured that simulated weightbearing fluoroscopy was performed without obvious leg rotation. Fifth, the addition of nonweightbearing fluoroscopy during surgery is an effective method to eliminate interference factors, which make the simulated weightbearing conditions the isolated variable. However, clear images of hindfoot alignment are not easy to obtain because of superimposition of bones when dorsal flexion is insufficient. Nonweightbearing fluoroscopy during surgery was not routinely applied. Because this was a retrospective study, we could not collect enough nonweightbearing fluoroscopy data for comparison. Sixth, the manual pressure applied during surgery was not absolutely standardized. Although there is no absolute standard for applying pressure, we asked an assistant to apply manual pressure to keep the foot in a neutral position as a relative standard in clinical practice, which may keep the measurement condition unified. In future research, a sophisticated experimental design may make up for these limitations.
Conclusion
The present study showed that intraoperative HAV fluoroscopy with simulated weightbearing is an effective method to correlate early postoperative hindfoot alignment in the weightbearing position. Patients with a lower BMI had less HAA deviation between intraoperative fluoroscopy and postoperative radiographs. Foot and ankle surgeons may use intraoperative HAV fluoroscopy to estimate early postoperative radiographic hindfoot alignment.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231159377 – Supplemental material for Simulated Weightbearing Fluoroscopy to Assess Intraoperative Hindfoot Alignment
Supplemental material, sj-pdf-1-fai-10.1177_10711007231159377 for Simulated Weightbearing Fluoroscopy to Assess Intraoperative Hindfoot Alignment by Ying Li, Wenjing Li, Ning Sun, Baozhou Zhang and Yong Wu in Foot & Ankle International
Footnotes
Acknowledgements
The authors thank AJE company (Durham, NC) and Angela Morben, DVM, ELS, from Liwen Bianji (Edanz) for editing the English text of a draft of the current article.
Ethical Approval
Ethical approval for this study was obtained from the Ethics Committee of Beijing Jishuitan Hospital (No. K2022-106-00).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.