
Abstract
Background:
We aimed to investigate the effect of Haglund deformity size on insertional Achilles tendinopathy (IAT) using a new measurement system and identify independent risk factors of IAT with Haglund deformity.
Methods:
We reviewed medical records of patients with IAT and age/sex-matched patients with diagnoses other than Achilles tendinopathy. Radiographs were reviewed to identify posterior heel spur, plantar heel spur, and intra–Achilles tendon calcification, and to measure Fowler-Philip angle, calcaneal pitch angle, and Haglund deformity angle and height. We introduced a new measurement system for Haglund deformity angle and height and evaluated its intraobserver and interobserver reliability. Multivariate logistic regression analysis was performed to identify independent risk factors of IAT with Haglund deformity.
Results:
Fifty patients (55 feet) were enrolled in the study group, equaling the size of the age/sex-matched control group. The new Haglund deformity measurement system showed excellent intraobserver and interobserver reliability. No significant differences between the 2 groups were noted in Haglund deformity angle and height: 6.0 degrees in both groups, and 3.3 mm vs 3.2 mm in the study and control group, respectively. The study group had significantly higher calcaneal pitch angle, incidence of posterior heel spur, plantar heel spur, and intra–Achilles tendon calcification: 5.2 vs 23.1 degrees (P = .044), 81.8% vs 36.4% (P < .001), 76.4% vs 34.5% (P = .003), and 67.3% vs 5.5% (P < .001), respectively. Multivariate logistic regression analysis identified independent risk factors of IAT: posterior heel spur (OR = 3.650, 95% CI = 1.063, 12.532), intra–Achilles tendon calcification (OR = 55.671, 95% CI = 11.233, 275.905), and increased calcaneal pitch angle (OR = 6.317).
Conclusion:
Based on our results, the actual size of Haglund deformity as we have reliably measured was not associated with IAT, suggesting a routine Haglund deformity resection may be unnecessary in the surgical treatment of IAT. If patients with Haglund deformity have posterior heel spur, intra–Achilles tendon calcification, or increased calcaneal pitch angle, a higher chance of IAT can be predicted.
Level of Evidence:
Level III, retrospective cohort study.
Keywords
Introduction
Haglund deformity, a posterosuperior calcaneal prominence, was first described by Haglund. 10 It is more commonly seen in middle-age, female, athletic people and those with pes cavus. 23 Haglund deformity causes pain from the bony prominence itself as an isolated symptom, but it also could lead to retrocalcaneal bursitis by mechanical impingement and be associated with insertional Achilles tendinopathy (IAT). These 3 findings are referred to Haglund syndrome or Haglund triad: Haglund deformity, retrocalcaneal bursitis, and IAT.
A variety of surgical techniques, ranging from open central tendon splitting approach to minimally invasive endoscopic calcaneal exostectomy, have been described for the treatment of Haglund triad, reporting good outcomes.4,17,25,26 Haglund deformity is routinely excised as a part of the surgical management of Haglund triad; however, the relationship between IAT and Haglund deformity is still questionable. Kang et al 13 reported the absence of association between the Haglund deformity and the IAT in their radiographic review study. Further, there is a lack of information about the effect of Haglund deformity size on IAT.
Haglund deformity was originally described as posterosuperior heel pain associated with wearing rigid low-back shoe gear by Haglund. 10 However, many physicians also refer to Haglund deformity as posterolateral calcaneal prominence, which can often be palpated on physical examination. 24 Many different terms have been used to describe this pathology since its first description, such as retrocalcaneal exostosis, winter heel, pump bump, calcaneal altus, high prow heels, cucumber heel, policeman’s heel, Mulholland deformity, and knobby heel.9,23,24 These inconsistent descriptions used in the literature creates confusion, and uniform and consistent description of Haglund deformity is essential for proper communication. Therefore, we clarified the definition of Haglund deformity, posterior calcaneal bony spur, and intra–Achilles tendon calcification in the study.
Furthermore, there is no clear and reliable method for measurement of Haglund deformity associated with IAT though Fowler-Philip angle, parallel pitch lines, calcaneal Pitch angle, and Chauveaux-Liet angle are commonly used to assess Haglund deformity. Recent studies implemented new measurement methods evaluating calcaneal shape to find a correlation between IAT and Haglund deformity.1,22 However, their reliability and efficiency are uncertain. In our study, we introduce a new measurement method for Haglund deformity and report its interobserver and intraobserver reliability.
The purpose of this age/sex-matched case control study is (1) to investigate the effect of Haglund deformity size on IAT using a new measurement system, and (2) to identify independent risk factors of IAT with Haglund deformity through a multivariate logistic regression analysis.
Material and Methods
After institutional review board (IRB) approval, an age/sex-matched case-control comparison was conducted by reviewing electronic medical records and radiographic images of patients who visited the office under the diagnosis of IAT. All patients with diagnosis related to Achilles tendon were screened first, and their medical records were reviewed to identify patients only with IAT. The diagnosis was based on clinical examination and radiographic findings. Only those who had IAT with Haglund deformity were included. Patients were excluded if they (1) were younger than 18 years, (2) had any surgical history for Achilles tendon, (3) had a history of Achilles tendon injury in the past 6 months, (4) had noninsertional Achilles tendinopathy, and (5) did not have a Haglund deformity.
Fifty patients met the inclusion criteria for the study group. Patient demographics including age, sex, body mass index (BMI), medical comorbidities including diabetes mellitus, smoking, and rheumatoid arthritis were reviewed. This study was designed to have 1:1 matching with the criteria of sex and age (within 2 years). The control group was identified for those who visited the office with foot and ankle issues other than Achilles tendinopathy during the same period of the study. Plain radiographs for all candidates for the control group were reviewed, and only those who had Haglund deformity were included. Patients with any Achilles tendon disease or injury were excluded from the control group. The following diagnoses were included for the control group: hallux rigidus, hallux valgus, Morton’s neuroma, hammertoe deformity, midfoot arthritis, ankle instability, or foot and ankle tendinopathy other than Achilles tendon.
Standing lateral foot or ankle radiograph for both groups was reviewed to identify the presence of posterior heel spur, plantar heel spur, intra–Achilles tendon calcification, and the following several specific angles: Fowler-Philip angle, calcaneal pitch angle, Haglund deformity angle, and Haglund deformity height. In this study, we wanted to clarify the difference between Haglund deformity and posterior/posterolateral heel spur, which is often referred as Haglund deformity. We defined Haglund deformity as posterosuperior calcaneal prominence, which is the same as Haglund originally described (Figure 1). Posterior heel spur was defined as any bony prominence at posterior or posterolateral aspect of calcaneus, which is a step-off of the normal calcaneal contour but still connected to the calcaneus (Figure 2). We defined intra–Achilles tendon calcification as a calcification located in the Achilles tendon and separate from the calcaneus (Figure 3).

Haglund deformity.

Posterior heel spur.

Intra–Achilles tendon calcification: An arrow identifying intra–Achilles tendon calcification.
All measurements were performed using the measuring tool within the hospital PACS system. In this study, we introduce a new measurement system for Haglund deformity angle and height to evaluate the size of Haglund deformity (Figure 4), and investigated its intraobserver and interobserver reliability. To measure the Haglund deformity angle, on a lateral foot or ankle radiograph, a line was drawn (line AB) connecting the most inferior margin of the calcaneus (point A) and calcaneocuboid joint (point B). A second line was drawn (line CD), parallel to the first line, originating at the most superior margin of the posterior facet of subtalar joint (point C). A third line was drawn (line CE) connecting point C to the peak of Haglund deformity (point E). The Haglund deformity angle was measured as the angle between lines CD and CE. To measure the Haglund deformity height, a perpendicular line was drawn from line CD to the peak of the Haglund deformity (point E). The measurements for Fowler-Philip angle and calcaneal pitch angle were described in previous studies (Figure 5).9,13
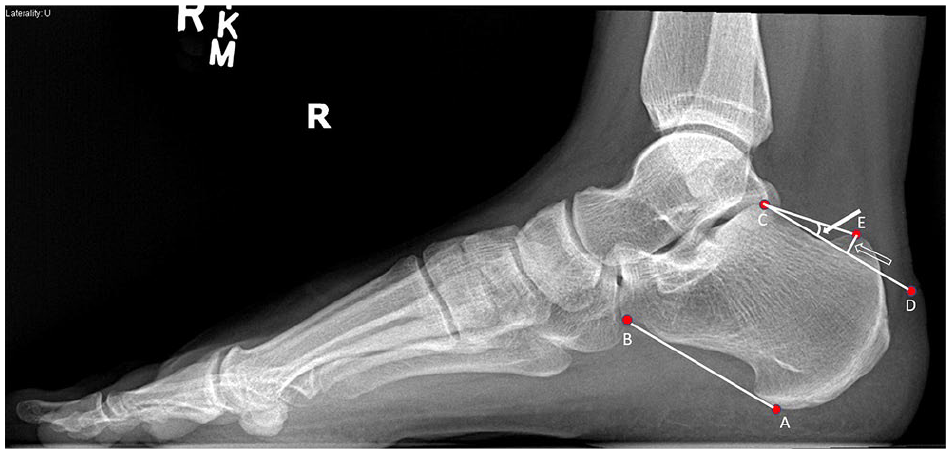
The new measurement system of Haglund deformity angle and height: Haglund deformity angle (an arrow), formed between Lines CD and CE; Haglund deformity height (an empty arrow), a perpendicular line drawn from line CD to the peak of the Haglund deformity (point E).

Fowler-Philip angle and calcaneal pitch angle: an arrow identifying Fowler-Philip angle; an empty arrow indicating calcaneal pitch angle.
Two evaluators (M.G. and C.C.) independently recorded all radiographic measurements and reviewed the same radiographs of the whole cohorts twice 3-4 weeks apart to assess interobserver and intraobserver reliability. The mean value of the 2 observers’ measurements were used to determine all angles and height in this study. The intraclass correlation coefficient (ICC) was used to quantify the degree of correlation between the same measurements for the size of Haglund deformity on radiographs. ICC values less than 0.5 are indicative of poor reliability, values between 0.5 and 0.75 indicate moderate reliability, values between 0.75 and 0.9 indicate good reliability, and values greater than 0.90 indicate excellent reliability.3,19
Demographic data and radiographic findings were compared between the study and control groups, and a multivariate logistic regression analysis was performed to identify independent risk factors of IAT with Haglund deformity.
Statistical Analysis
Data are presented as the mean and standard deviation. Student t test was used to compare continuous variables such as age and overall BMI, and χ 2 test or Fisher exact test was used to compare categorical variables. Variables that can have an effect on IAT were investigated from the literature review, and through the comparison of demographic and radiographic data between the study and control groups in our study. Then, a multivariate logistic regression analysis was performed to identify independent risk factors of IAT with Haglund deformity. The level of statistical significance was set as P <.05. All statistical analyses were performed with SPSS software (version 21.0; IBM, Armonk, NY, USA).
Results
There were 50 patients enrolled in the study group (IAT with Haglund deformity), and an equal number of patients were included in the age/sex-matched control group (without IAT but with Haglund deformity). Both groups had 86.0% (43/50) female and 14.0% (7/50) male subjects. The mean age was 56.3 years in the study group and 56.2 years in the control group. No significant differences in patients’ demographics were noted between the study and control groups except for BMI (Table 1).
Patient Demographics.
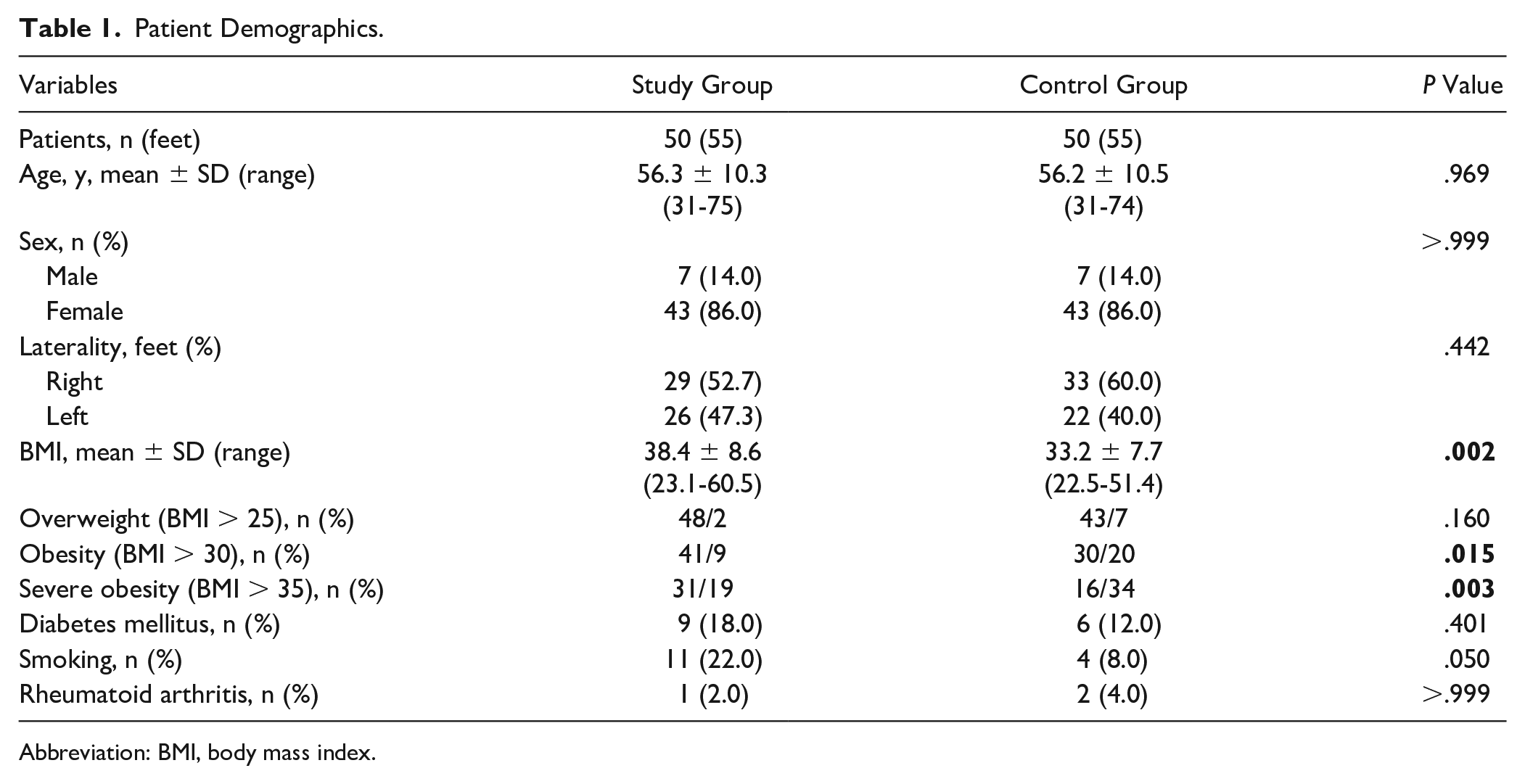
Abbreviation: BMI, body mass index.
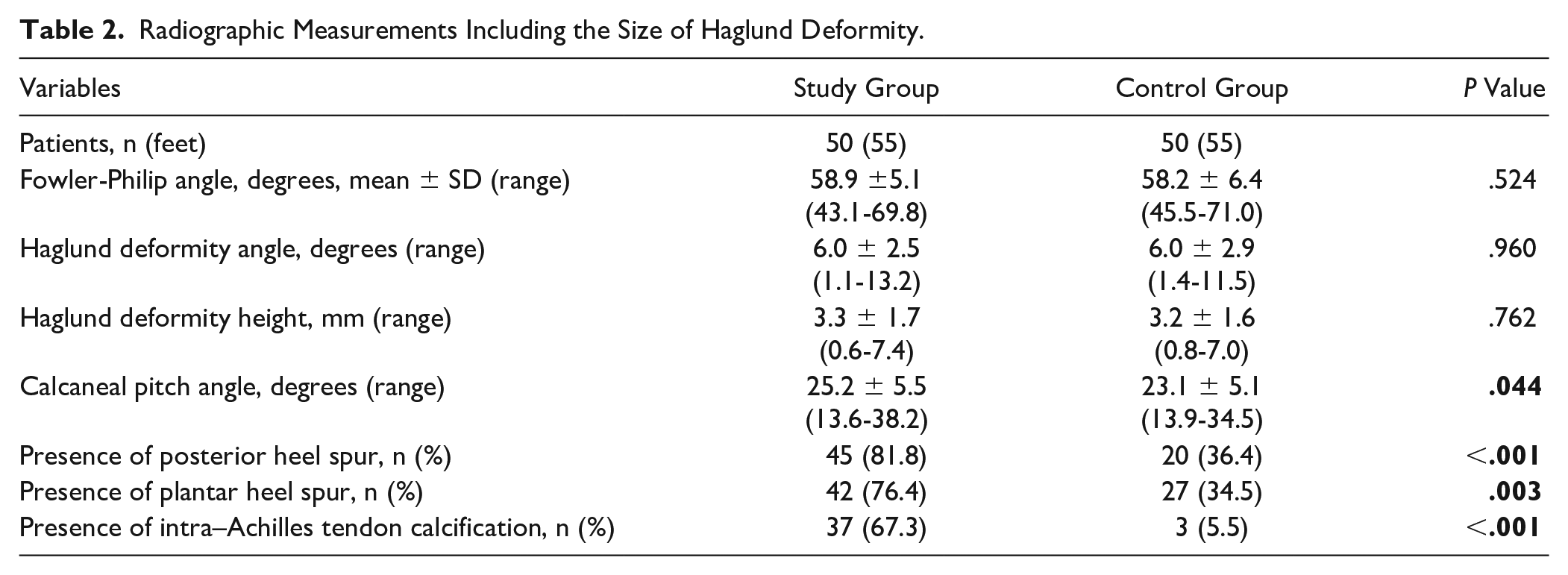
There was no significant difference in the size of Haglund deformity between the 2 groups: Haglund deformity angle and height (Table 2). The mean Haglund deformity angle was 6.0 degrees in both groups. The mean Haglund deformity height was 3.3 and 3.2 mm in the study group and the control group, respectively. Calcaneal pitch angle was significantly higher in the study group: 25.2 degrees vs 23.1 degrees (P = .044
Radiographic Measurements Including the Size of Haglund Deformity.
Intraobserver and Interobserver Variability for Haglund Deformity Size.
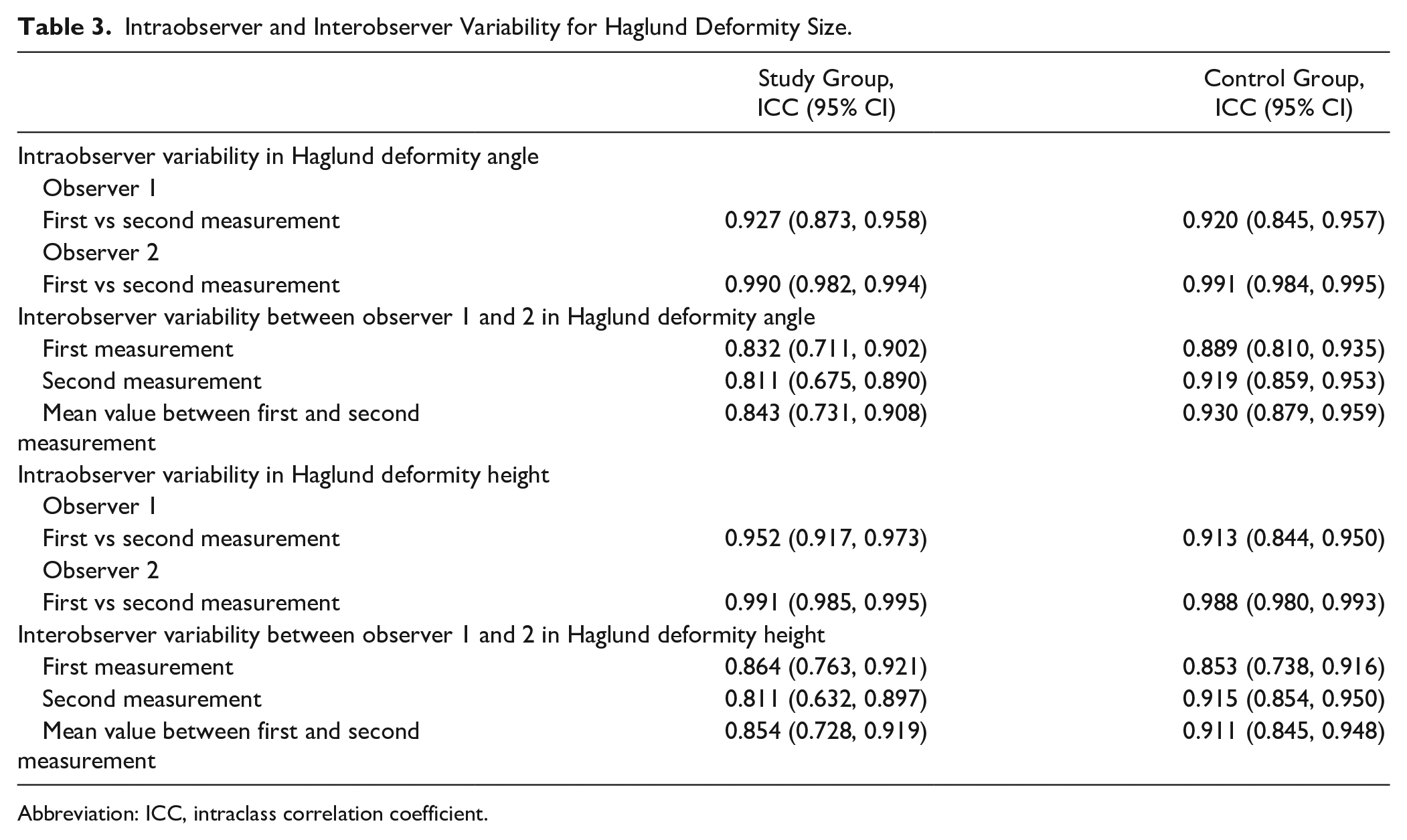
Abbreviation: ICC, intraclass correlation coefficient.
A multivariate logistic regression analysis was conducted to identify independent risk factors of IAT. The results are shown in Table 4. The presence of posterior heel spur (OR: 3.650), intra–Achilles tendon calcification (OR: 55.671), and increased calcaneal pith angle (reference: 23.3 degrees; OR: 6.317) were identified as independent risk factors of IAT with Haglund deformity. The mean value of all cohorts in this study was used as a reference regarding age and calcaneal pitch angle for this multivariate logistic regression analysis.
A Multivariate Logistic Regression Analysis Identifying Risk Factors of Insertional Achilles Tendinopathy With Haglund Deformity.
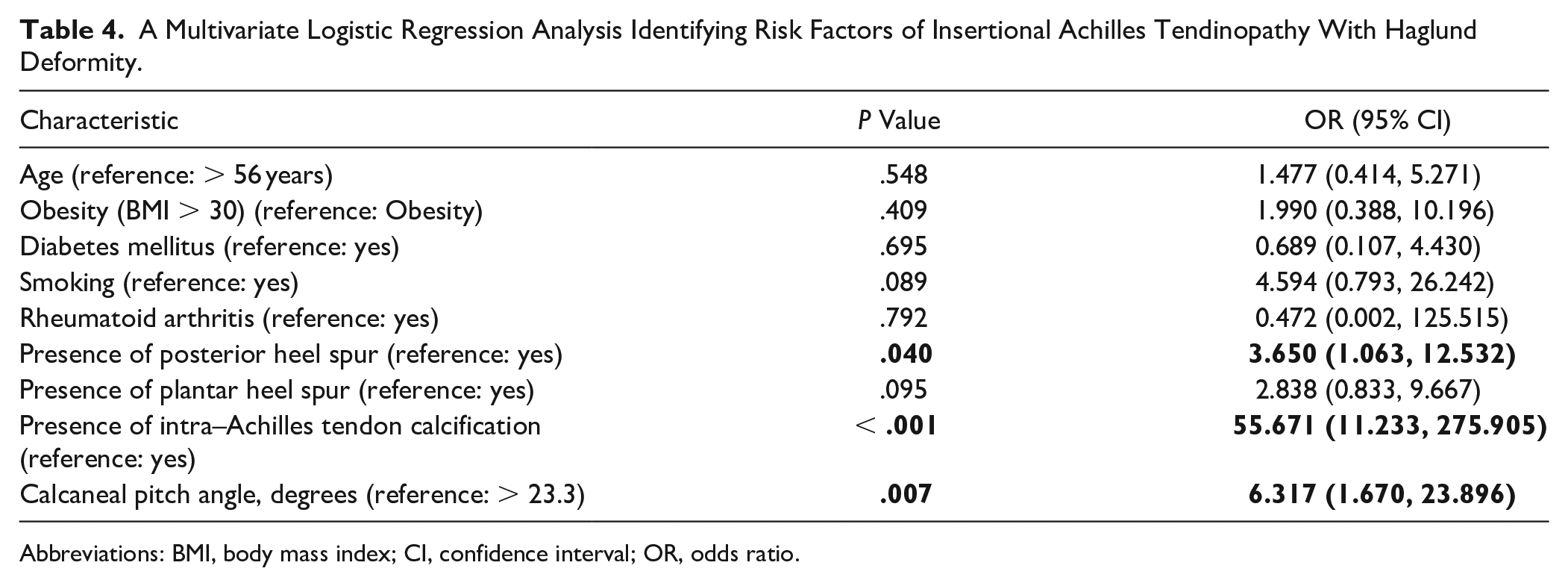
Abbreviations: BMI, body mass index; CI, confidence interval; OR, odds ratio.
Discussion
There is a paucity of information from studies reporting the effect of Haglund deformity size on IAT. We included only patients who had Haglund deformity for both the patient group with IAT and the control group without IAT and compared their demographics and radiographic findings. The results showed no significant difference in the size of Haglund deformity between the 2 groups, suggesting the Haglund deformity actual size is not in itself associated with IAT. Through multivariate logistic regression analysis, we identified several independent associated factors of IAT with Haglund deformity, including the presence of posterior heel spur, intra–Achilles tendon calcification, and increased calcaneal pitch angle. In this study, we also introduce a new measurement system for Haglund deformity angle and height, which showed good to excellent intraobserver and interobserver reliability.
Currently, several measurements on plain radiographs are used to evaluate Haglund deformity, but their efficacy and usefulness has been in doubt. Parallel pitch lines are one of the most commonly used measurement systems and are composed of 2 lines: the first line formed from the calcaneal pitch and the second line parallel to the first line, from the posterior lip of the talar articular surface. 9 Any prominence of the posterosuperior aspect of the calcaneus above the second line is called a Haglund deformity. The efficacy of parallel pitch lines was reported variably, and some studies reported no significant difference between symptomatic and asymptomatic patients with Haglund deformity.9,13,16,20 Another measurement, the Fowler-Phillip angle, is formed by one line tangential to the posterosuperior border of the calcaneus and the calcaneal tuberosity and the other line connecting the most inferior margins of the calcaneus and calcaneocuboid joint. 6 Several studies reported that a false negative rate of Fowler-Phillip angle would be variable, up to 100%.9,20 Lu and his colleagues 16 analyzed the predictive value of Fowler-Phillip angle and parallel pitch lines to evaluate bursal impingement and investigated if osseous variations are associated with the development of Haglund syndrome. They concluded that Fowler-Phillip angle and parallel pitch lines showed little predictive value for the Haglund syndrome.
Kang et al 13 compared Haglund deformity peak angle and height using their measurement system between the patients with and without IAT and found no significant differences between the 2 groups. However, they reported that the positive parallel pitch sign was only 41.7% and 60.0% in the patients with and without IAT, respectively, in their study. This indicates that they measured Haglund deformity peak angle and height for not only patients with Haglund deformity, a posterosuperior calcaneal prominence, but also those who did not have a true Haglund deformity. Further, only one individual performed the measurements, providing no information about interobserver reliability though they reported correlation coefficients of at least 0.90 for all measurements. Also, patients’ variant bony shape and contour makes it difficult to draw the line at the base of posterosuperior calcaneal prominence and anterior/posterior slope for some patients, which is required to measure the Haglund deformity angle and height according to their study’s measuring system. We suggest a new measurement system for the Haglund deformity angle and height that is less affected by patients’ bony shape and contour and demonstrated excellent intraobserver reliability and at least good interobserver reliability.
Haglund deformity, one of the components in Haglund triad (syndrome), has been considered as one of risk factors affecting IAT as its bony prominence can cause chronic irritation along the Achilles tendon with repetitive pressure. Therefore, surgical treatment of IAT routinely involves removal of Haglund deformity. Traditionally, Haglund deformity resection requires an open procedure, but endoscopic/fluoroscopic minimally invasive procedures have become popular.2,4,5,11,12,15,17,18,25 Furthermore, good clinical outcomes have been reported with the dorsal closing wedge calcaneal osteotomy combined with Haglund deformity removal.2,7,8 However, the association between Haglund deformity and insertional Achilles tendinopathy is still debatable. Several previous studies reported that a Haglund deformity was not indicative of IAT, questioning the necessity of routine excision of Haglund deformity for the treatment of IAT.13,21 Kunkle et al 14 investigated risk factors for failure of conservative management of IAT. They reported that Haglund deformity on physical examination was one of the risk factors leading to a surgical treatment, whereas Haglund deformity on radiograph was not. They defined “Haglund deformity on radiograph” as when positive parallel pitch lines were present on radiographs and “Haglund deformity on physical examination” as the presence of a palpable bony enlargement on the posterior aspect of the heel near the insertion of the Achilles tendon. Their different definitions of Haglund deformity can provoke confusion. It was unclear if they included only true Haglund deformities, posterosuperior calcaneal prominences, or if they also included posterior/posterolateral calcaneal bony prominences as clinical Haglund deformity. This difference between the definitions of radiographic and clinical Haglund deformity could be due to the lack of insight about the Haglund deformity size in the study. If the size of Haglund deformity was too small to appreciate on physical examination, it could result in a statistical analysis error with inaccurate data. For more accurate comparison of Haglund deformity size between the study and control group, we included patients who had Haglund deformity in both groups. We clarified the difference between Haglund deformity, posterior heel spur, and intra–Achilles tendon calcification in our study to minimize confusion regarding the definition of bony structures. Our results demonstrated that Haglund deformity size does not matter to IAT. There was no significant difference in Haglund deformity size between the patients with and without IAT.
Our multivariate logistic regression analysis identified the presence of posterior heel spur, intra–Achilles tendon calcification, and increased calcaneal Pitch angle as independent risk factors of IAT with Haglund deformity, which is comparable to the results from previous studies.13,16 Lu et al compared radiographic findings including Fowler-Phillip angle, parallel pitch lines, posterior calcaneal step spur, and plantar bony spur between the patients with symptomatic Haglund syndrome and those without posterior heel pain. They reported that posterior calcaneal step spur (56.8% vs 5%, P < .001) and intra–Achilles tendon calcification (78.4% vs 12.5%, P < .001) were present significantly more frequently in the symptomatic Haglund syndrome group. Kang et al 13 also found that most patients with IAT have calcification at the Achilles tendon insertion (73%, 35/48). Several previous radiographic comparison studies report a significant difference in the calcaneal pitch angle between the Haglund syndrome group and the healthy control group.1,22 Bulstra et al 1 reported significantly increased calcaneal pitch angle in their Haglund syndrome cohort compared to the non–Haglund syndrome cohort. Our results echo their findings. This can be explained by the abnormally steep calcaneal slope that can be seen more commonly in high-arch feet, creating more tension along the Achilles tendon at the insertion area and impingement between the Achilles tendon and the posterosuperior calcaneal prominence.1,22
This study is not without limitations. First, the retrospective design of the study creates an inherent risk of bias. The completeness and validity of the data relied on the content of the medical record. Second, patients included in this study are from a single institution, which may affect sample size and selection bias. Third, as the major portion of this study is a radiographic review, all possible clinical risk factors of IAT such as patients’ activity level and Achilles tendon/gastrocnemius muscle tightness could not be included for multivariate logistic regression analysis. Fourth, as we did not perform MRI for all patients, we could not evaluate the precise status of Achilles tendon. So, patients with asymptomatic Achilles tendinosis could have been in the control group. However, the diagnosis of IAT was based on images and patients’ symptoms. Even if some patients in the control group had MRI findings of Achilles tendinosis, if they had no heel pain, they would be included in the control group. Fifth, our method of measuring Haglund deformity size is 2-dimensional and is both subject to rotation protectional artifact and cannot quantify volume. Despite these limitations, our study has several strengths. To our knowledge, it is the first age/sex-matched case control study to investigate the effect of Haglund deformity size on IAT providing valuable information. We introduce a new measurement system for Haglund deformity with good to excellent intraobserver and interobserver reliability, which may be useful for clinical patient evaluation and future research.
Conclusion
Based on our results, the actual size of Haglund deformity is not associated with IAT, suggesting that a routine Haglund deformity resection may be unnecessary in the surgical treatment of IAT. Patients with Haglund deformity and posterior heel spur, intra–Achilles tendon calcification, or increased calcaneal pitch angle, are associated with a higher likelihood of having IAT, and these issues may need to be addressed in the surgical treatment of IAT.
Supplemental Material
sj-docx-2-fai-10.1177_10711007231168625 – Supplemental material for Association of Haglund Deformity Size and Insertional Achilles Tendinopathy
Supplemental material, sj-docx-2-fai-10.1177_10711007231168625 for Association of Haglund Deformity Size and Insertional Achilles Tendinopathy by Wonyong Lee, Margaret Elizabeth Giro and Colt Crymes in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231168625 – Supplemental material for Association of Haglund Deformity Size and Insertional Achilles Tendinopathy
Supplemental material, sj-pdf-1-fai-10.1177_10711007231168625 for Association of Haglund Deformity Size and Insertional Achilles Tendinopathy by Wonyong Lee, Margaret Elizabeth Giro and Colt Crymes in Foot & Ankle International
Footnotes
Ethical Approval
Ethical approval for this study was obtained from Institutional review board of the Guthrie Clinic (IRB# 2111-67).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.