
Abstract
Background:
Diabetic foot osteomyelitis affecting the toes is associated with several complications including amputation. Management is variable and include medical therapy alone or coupled with surgery. Removal of infected tissues is a common therapeutic option. However, limited source data are available. This study determines the outcome and complications of percutaneous partial bone excision (PPBE) of infected bone among diabetic patients with toe osteomyelitis.
Methods:
This is an uncontrolled experimental prospective study in diabetic patients who underwent PPBE of infected pieces of bone for toe osteomyelitis in the outpatient setting at a single foot clinic. All participants were followed up until the occurrence of wound healing or amputation.
Results:
Forty-seven patients (mean ± SD age was 62.8 ± 11.6 years) participated. Forty-four patients (93.6%) had complete healing and 3 (6.4%) required toe amputation. The mean (±SD) wound healing time was 11 (±4.6) (range, 7-22) weeks. Diabetes mellitus type 1 and younger age were significantly associated with increased risk for amputation.
Conclusion:
PPBE of infected toes in diabetic patients can be performed successfully and safely in the outpatient clinic. It can also improve healing and avoids inpatient stay.
Level of Evidence:
Level II, prospective cohort study.
Introduction
Foot infections are among the most frequent diabetes-related causes for hospitalization and lower-extremity amputation. 25 About 19% to 34% of diabetic patients develop a foot ulcer at some time during their life, and 40% to 80% of these ulcers become infected.1,4 Approximately 20% of foot infections are associated with bone involvement that usually leads to nonhealing ulcers or amputations. 3 Of note, toes are the most common site for amputation among diabetic patients. 21
The cause of foot ulcers in diabetic patients is multifactorial and includes neuropathy, vasculopathy, immunopathy, and poor glycemic control. Motor neuropathy can lead to structural changes to the foot manifesting as claw toes, hammertoes, prominent metatarsals, and other deformities. 11 The hammer/claw deformity is related to a reduction in the thickness of the fat pad under the metatarsal head leading to increased plantar pressures which can lead to foot ulceration.7,10 Another cause to the development of toe ulcers is the presence of corn. The most common locations for corns are over the dorsal lateral aspect of the fifth toe and in the interdigital space between the fourth and fifth toes. 9 Once developed, those toe ulcers could then easily progress to deep ulcers with osteomyelitis mostly because the interphalangeal joints and phalanges are covered directly by skin.5,36
Removing of infected bones from the toes to treat nonhealing ulcer is common practice in hospitals and wound care centers. However, data on this practice are still limited.32,36 The current study aims to determine the outcome of partial excision of infected pieces of bones in diabetic patients in the outpatient settings.
Patients and Methods
We used an uncontrolled experimental study. It is a type of observational study in which the effect of an intervention in a single group of patients is described without a control group.8,13 The study was performed at the Diabetic Foot Clinic at the National Center for Diabetes, Endocrinology, and Genetics (NCDEG) in Amman, Jordan. The center offers medical services for diabetic patients. It has several specialized clinics including a specialized foot care clinic. The foot clinic is multidisciplinary, with staff consisting of vascular surgeons, general surgeons, infectious disease physician, and certified diabetic foot care nurses. The population of patients attending the center is characterized by the following: diabetic foot ulcer prevalence of 4.7%, amputation of 1.7%, peripheral neuropathy of 39.5%, and peripheral arterial disease of 5.4%.2,22,27 The study was approved by the Institutional Review Board of the NCDEG.
All the patients who attended the diabetic foot clinic and were suffering from toe ulcer with an underlying toe osteomyelitis were included. Enrollment of patients was done by S.M. Diagnostic criteria for toe osteomyelitis were sausage-like toes, foot radiograph showing bone destruction at the site of the ulcer, positive probing test, exposed bone, recurrence of the ulceration, or an ulcer for more than 2 weeks with poor healing response manifesting as failure to decrease in the size of the wound.3,28 Exclusion criteria were severe infection requiring admission or severe peripheral arterial disease according to a clinical criteria that included toe pressure <30 mm Hg, ankle brachial index <0.6, or diagnosis by a physician. 30 Collected data included clinical history, feet examination, plain radiograph of the affected foot, glycated hemoglobin (HbA1c), and wound or bone culture. Bacterial cultures were performed only for patients who did not show signs of improvement after 1 week of treatment.
The procedure was explained to all participants and was performed by 2 of the investigators (N.Y. or S.M.): N.Y. is a surgeon working in the foot clinic for the last 12 years and S.M. is a certified diabetic foot nurse with 12 years of experience. During the procedure, we removed the destructed bone and the necrotic tissue including nail bed and tendon when affected. The tissue was removed and nibbled by sharp debridement through the open ulcer using a bone nipper or a curette. We removed the destructed bone until hard bone was felt. Wound dressing was performed with the use of products containing silver ion, hydro gel, collagen dressing, or iodine patches. Patients would be examined at the third day after the procedure. Wounds were left open and were not sutured. Patients were then followed up in the clinic with appointments as once, twice, or 3 times weekly depending on the level of exudate and the signs of infection. In the following visits, we used a bone curette to feel manually for bone fragments and a radiograph to detect sequestrum in order to decide on further debridement and to detect any bone that was not removed in previous procedure sessions.
Radiographic evaluation was performed 1 week after the procedure to ensure that no bone sequestrum was left in the wound. Offloading devices such as wedge shoes and felted foam was used to relieve pressure from the affected area depending on the patient situation and the site of the wound. Healing was defined as complete epithelialization of the wound with absence of any discharge. We followed the patients for 12 weeks after healing to observe for the development of new ulcer or recurrent infection. The follow-up was scheduled once every 2 weeks in the first month and then once a month in the following 2 months.
All patients received empiric antibiotics after debridement. Antibiotic regimen for the initial 5-7 days included intramuscular ceftriaxone, oral ciprofloxacin, and oral metronidazole. If the infection responded, this was followed by oral clindamycin or ciprofloxacin for at least another 2 weeks. If the infection did not respond within 1 week of antibiotic, a bone culture was performed and antibiotics were changed accordingly. Antibiotic therapy was discontinued when the bone became covered by soft tissue and had no signs of infection, or the wound became clean and had no signs of infection for a minimum period of 2 weeks.
Statistical Analysis
Sample size was calculated for proportions and was found to be 54 patients assuming a significance level of .05, a power of 0.90, an intervention demonstrating 50% reduction in infection, and a response rate of 60% for treating osteomyelitis with antibiotics alone.3,8 Data analysis was performed using Statistical Package for Social Sciences IBM SPSS, version 21 (IBM Corp, Armonk, NY). Data were described using mean and SD for continuous variables and frequency and percentage for categorized variables. Chi-square test was used to determine the associations between healing and other variables. Sample t test was used to find the differences among the tested groups. The P value of <.05 was chosen as statistically significant.
Results
The study was performed from November 1, 2011, until March 30, 2019. Among patients who were interviewed for the study purposes, 48 agreed to participate and signed the informed consent. One patient was lost to follow-up, and thus a total of 47 patients were included in the final analysis. Among the participants, there were 66% males, the mean (±SD) age was 62.8 (± 11.6) years, 44 (93.6%) patients had type 2 diabetes, and the mean (±SD) duration of diabetes was 16.7 (± 8.59) years (Table 1).
Participant Demographics and Clinical Characteristics.
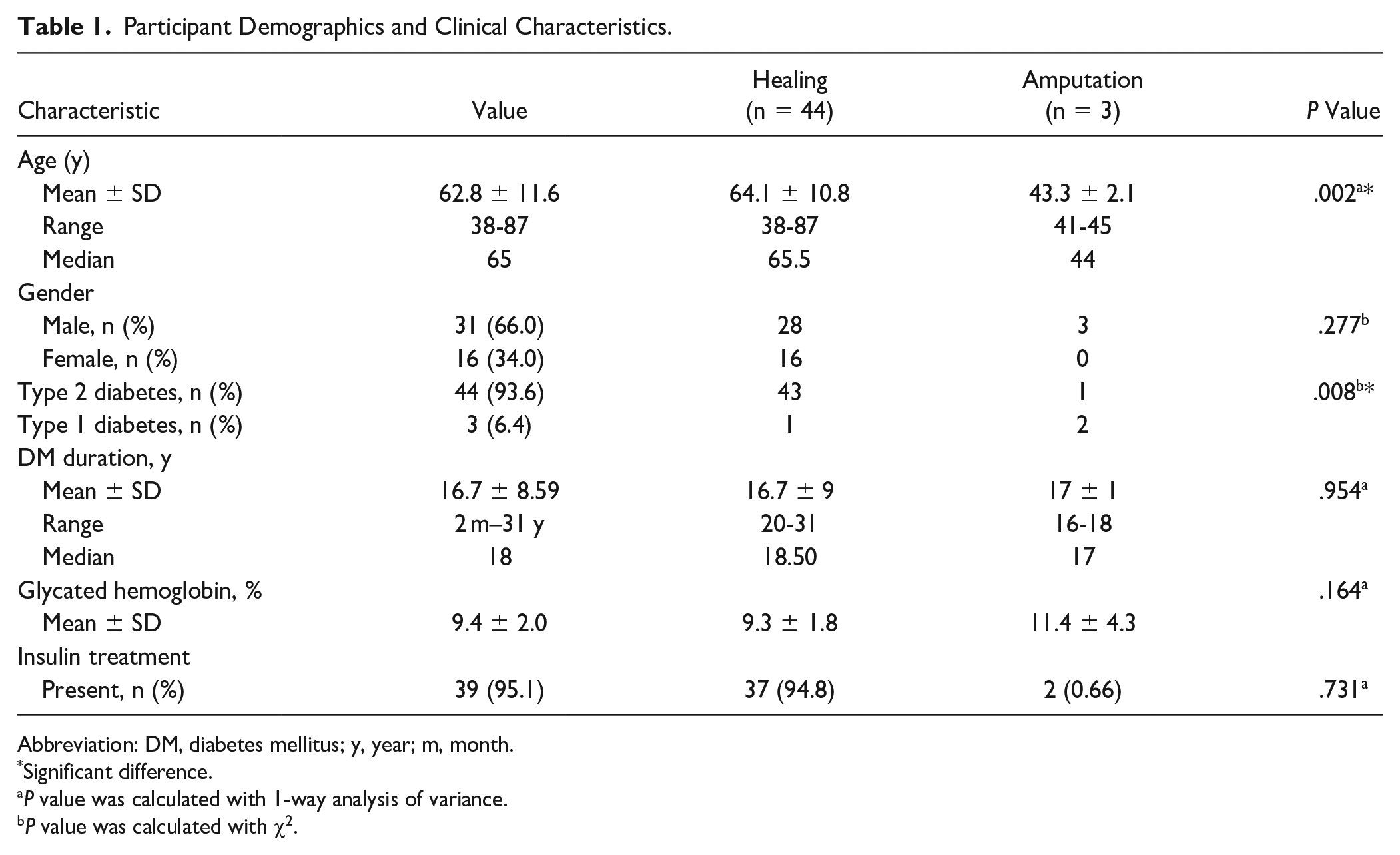
Abbreviation: DM, diabetes mellitus; y, year; m, month.
Significant difference.
P value was calculated with 1-way analysis of variance.
P value was calculated with χ2.
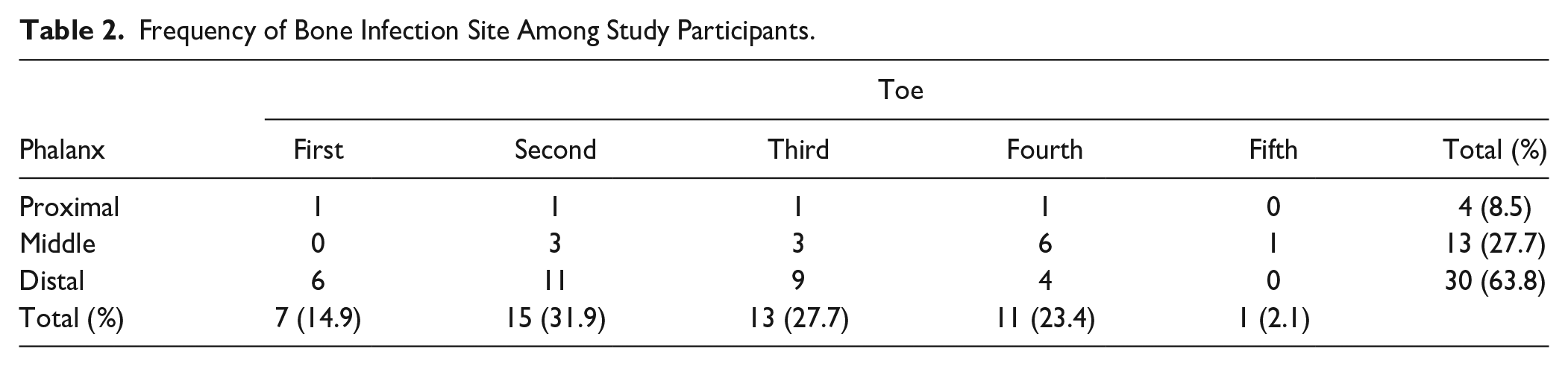
The most affected toe was the second toe and the most affected phalanx was the distal phalanx (Table 2). Representative cases of percutaneous partial bone excision (PPBE) at 3 different toe sites are shown in Figures 1 to 3. All patients were fully ambulant after the procedure. Of participants, 44 healed (93.6%) (Table 2). Healing time ranged between 7 and 22 weeks (mean: 11 [±SD 4.6] weeks; median: 9 weeks). Toe osteomyelitis affected the right foot in 28 patients (59.6%), the left in 19 (40.4%). No bilateral affection was observed. In 16 patients (34%), we removed the infected bone from more than 1 phalanx. Of patients, 12 (25.5%) had persistent clinical infection and underwent deep tissue culture (Table 3). The duration of antibiotic therapy ranged between 2 and 8 weeks.
Frequency of Bone Infection Site Among Study Participants.
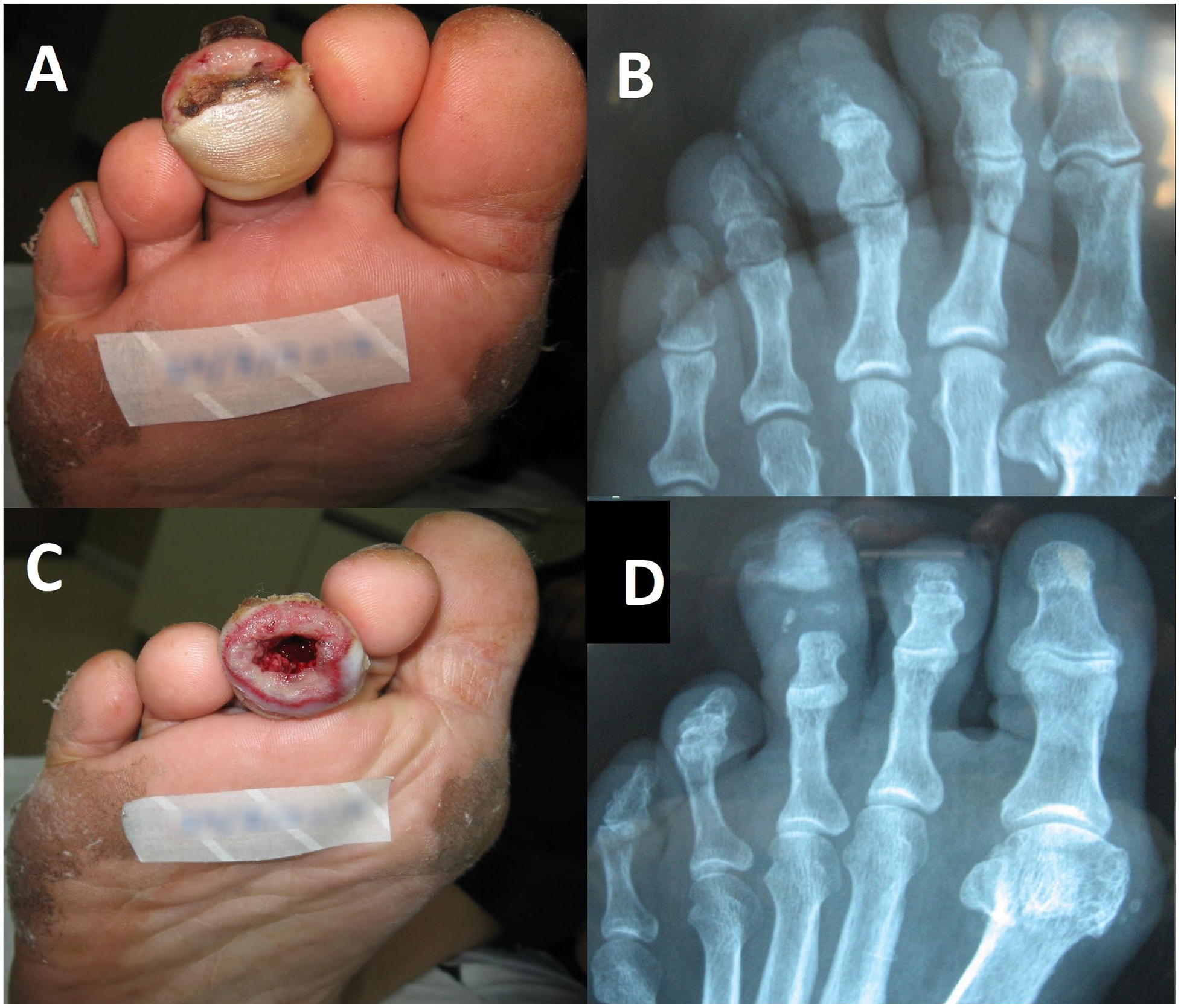
(A) An infected distal phalanx of the third toe before percutaneous partial bone excision (PPBE), (B) radiograph before PPBE, (C) the third toe after PPBE, and (D) radiograph after PPBE.
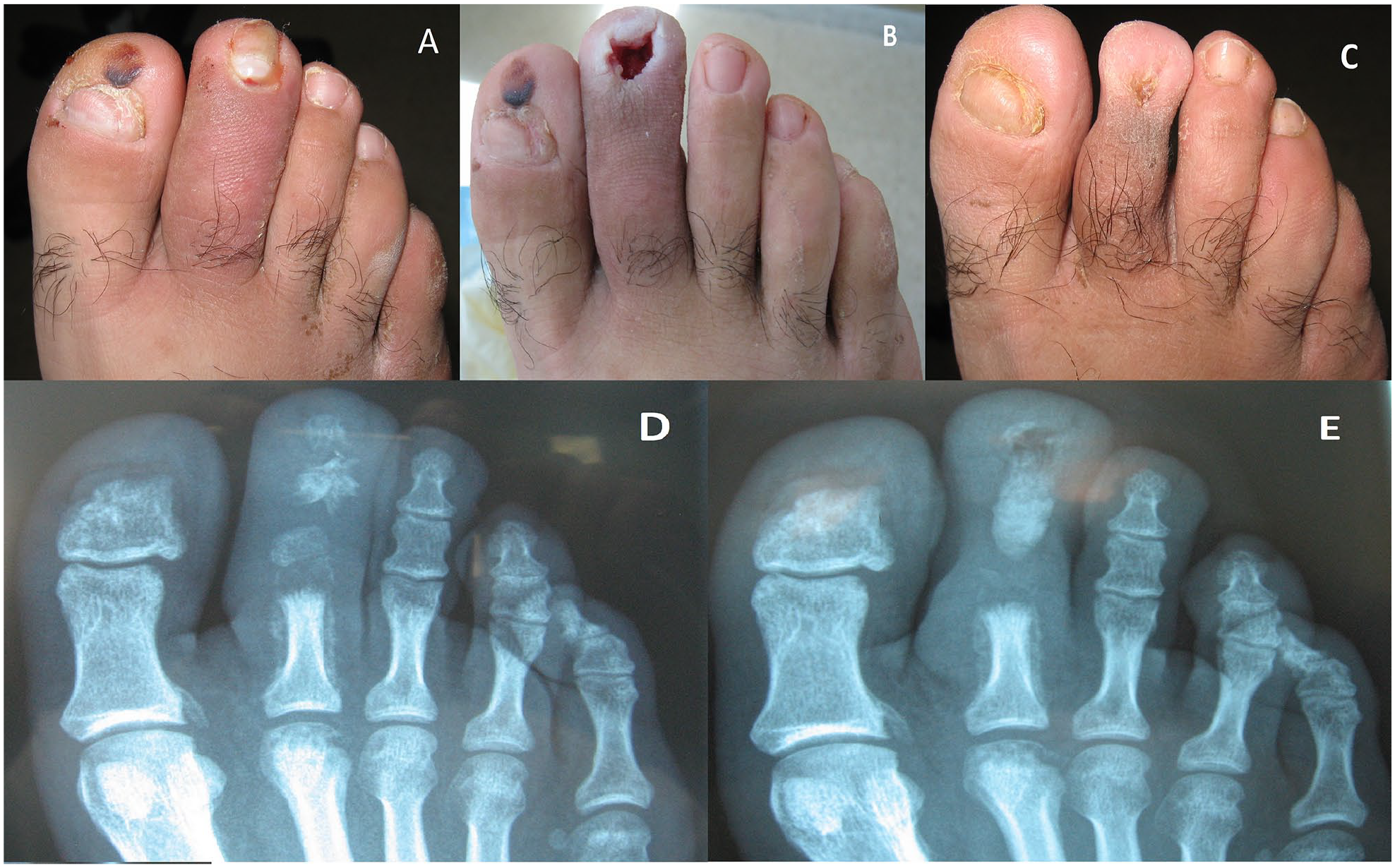
(A) An infected second toe before percutaneous partial bone excision (PPBE), (B) after PPBE, (C) after healing, (D) radiograph before PPBE, and (E) radiograph after PPBE.
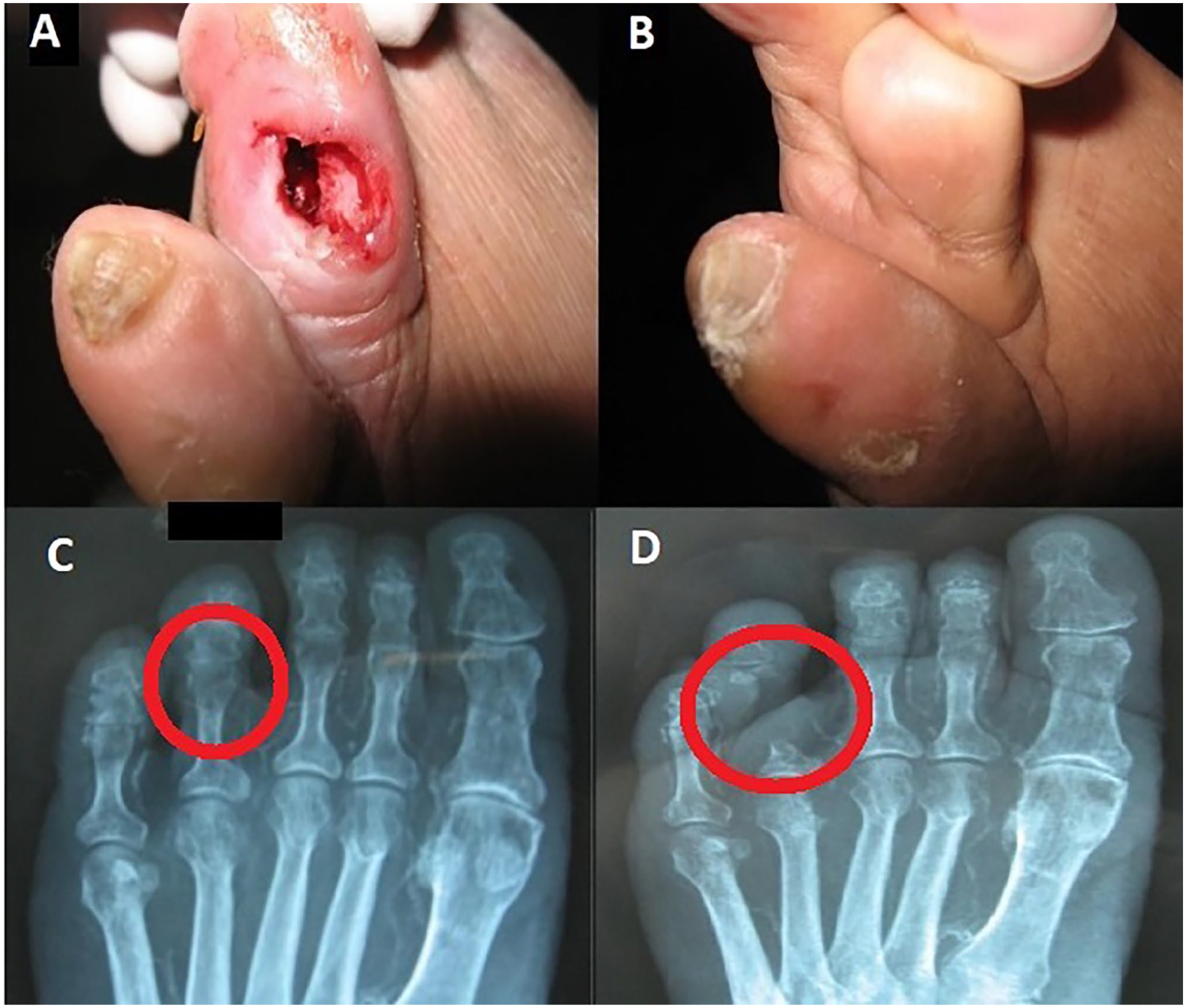
(A) An infected fourth toe after percutaneous partial bone excision (PPBE), (B) after healing, (C) radiograph before PPBE with the circle showing destructed bone of middle and proximal phalanx and proximal interphalangeal joint, and (D) radiograph after PPBE with the circle showing the phalanges after PPBE.
Microbiological Culture Results for Patients With Persistent Infection.
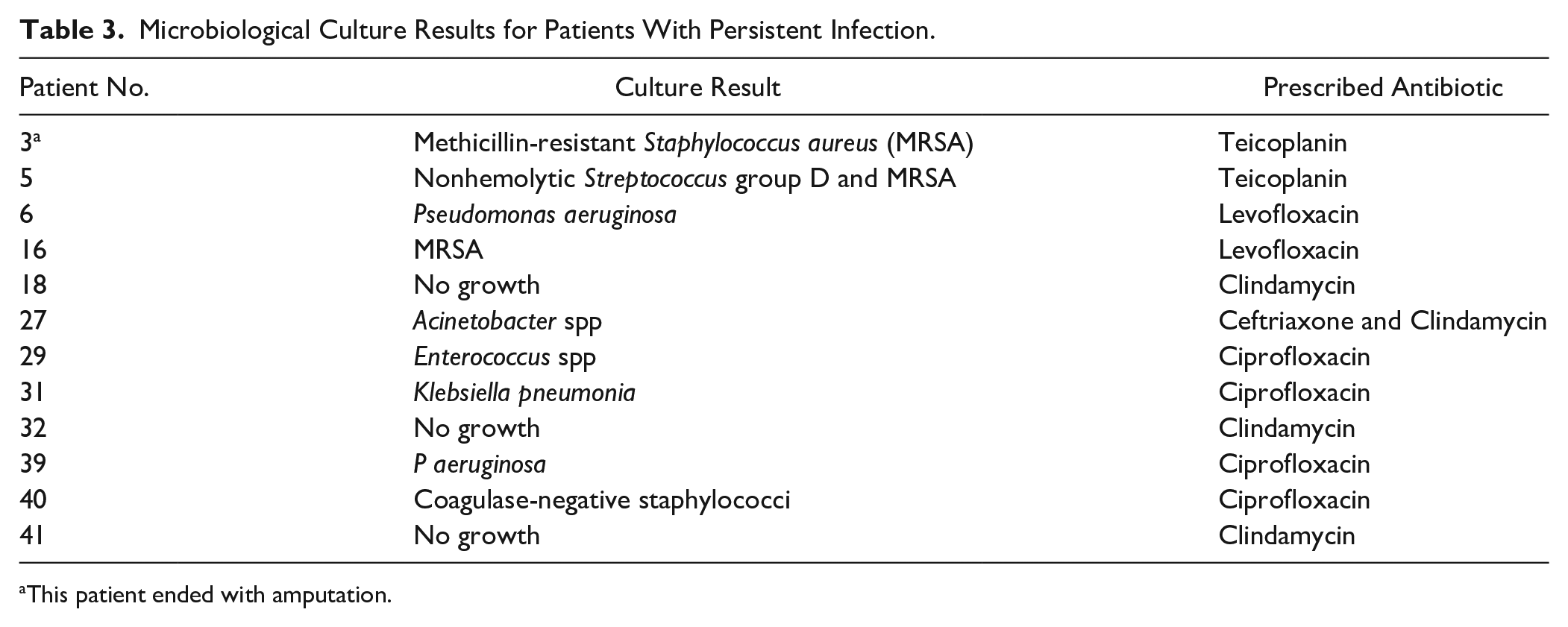
This patient ended with amputation.
Three (6.4%) patients developed severe infection that did not respond to our management (mean (±SD) age was 43.3 (± 2.1) years; all were males; and 2 had type 1 diabetes) (Table 2). All these patients developed systemic symptoms of infection, including 1 who developed necrotic toe. They were admitted to the hospital where toe amputations were performed.
Discussion
Here, we determined the outcome of PPBE in 47 diabetic patients. We showed that 44 (93.6%) patients healed without complications and 3 (6.4%) ended up with toe amputation. Our results support the use of PPBE in diabetic patients with toe ulcers and underlying osteomyelitis. The procedure may lead to reduction in minor toe amputation and preserve the toes. Preserving the toes and the arch structures is critical to gait because of the large range of motion displayed by the ankle. 16 In a recent review by Senneville and Robineau, 33 the authors concluded that the combination of bone resection limited to the most advanced bone lesions and antibiotic therapy directed to bone samples culture appear to be an interesting option. They also proposed that the growing problem of resistant bacteria is likely to reduce the part of the medical approach.
The main goal for treating osteomyelitis is to prevent the recurrence of active infections, reduce the chance of amputation, and prevent deformities. The ability of treating osteomyelitis without removing the bone is still under discussion. 33 Osteomyelitis may be treated either with antibiotics alone or coupled with removal of the infected bone or amputation of the toe. 20 One complication of toe amputation is the displacement of the adjacent toes into the space that resulted from the amputation, which might lead to a new deformity that will eventually lead to new ulcers. 23 Furthermore, it is known that diabetes can cause depression. Thus, informing the patient of his need for an amputation, even if it is a simple amputation, can exacerbate patient’s depression. 14
Data on resection of infected bone in the toes of diabetic foot is scarce. The only meta-analysis about this subject had found 7 related studies. 36 These studies included a total of 290 patients who underwent one of 3 types of conservative surgical procedures: (1) resection arthroplasty of the interphalangeal joint, (2) toe-sparing bone excision (internal pedal amputation), and (3) distal Symes amputation. The meta-analysis demonstrated a healing rate of 98.3%, mean (±SD) healing time of 6.8 ( ± 3.9 )weeks, recurrence rate of 2.3%, wound dehiscence/recurrent infection rate of 6.4%, skin necrosis rate of 2.8%, and revision surgery rate of 7.4%.
A study by Tiwari et al 34 that included 7 diabetic patients with toe osteomyelitis and who underwent excision of the first metatarsophalangeal joint to preserve the toe found that all wounds healed with no new ulcerations and minimal complications and the mean wound healing time was 9.5 weeks (range 5-16 weeks). A study by Feldman et al 15 that compared the outcome of primary nonoperative antibiotic treatment (39 patients) vs digital amputation (21 patients) found that the involved digit was eventually amputated in 13 of the 39 (33%) nonoperatively treated patients. The rate of major amputation was 4 of 39 (10.3%) and 3 of 21 (14.3%), respectively (P = .69). The authors concluded that in patients with mild and limited digital foot osteomyelitis in the absence of sepsis, it may be reasonable to offer a primary nonoperative treatment for digital osteomyelitis of the foot. A study by Treadwell, 35 in a retrospective case series of 45 patients with distal toe ulcers and osteomyelitis of the distal phalanx who underwent excision of the ulcer and removal of the infected distal phalanx using local anesthesia, found that patients with ulcers of the distal toe with osteomyelitis could be safely and effectively treated conservatively in the wound clinic by removing the infected bone followed by a course of oral antibiotics.
In our study, the healing rate was 93.6% and the healing time ranged between 7 and 22 weeks with a mean (±SD) duration of 11 (± 4.6) weeks, which is consistent with the previous studies and is considered to be a high healing rate. Moreover, the patients had no complications after 3 months of follow-up. It should be noted, however, that accurate comparison between this study and previous studies is difficult because of the variable definition of “conservative management” as some studies had done minor amputation as part of their management.
We observed that the second toe is the most affected toe with a rate of 31.9% followed by the third (27.7%) and the fourth (23.4%) toes. Also, the most affected phalanges were the distal phalanges (63.8%) followed by the middle phalanges (27.7%) and the proximal phalanges (8.5%). This might be explained by 2 reasons:
1. The central toes (second, third, and fourth toes) have unique anatomy, function, and deformity; the central toes have minimal subcutaneous tissue covering the prominent bone and joint structures at the tip of the toe and around interphalangeal joints. This predisposes to bone infection when the soft tissue is compromised by wounds.
2. The second toe might be the longest toe in some patients, which makes it more vulnerable to trauma and friction and thus has higher risk of ulceration. 5 Of note, the observation of a short first metatarsal bone behind the big toe compared to the second metatarsal is known as Morton syndrome 31 (Figure 4).
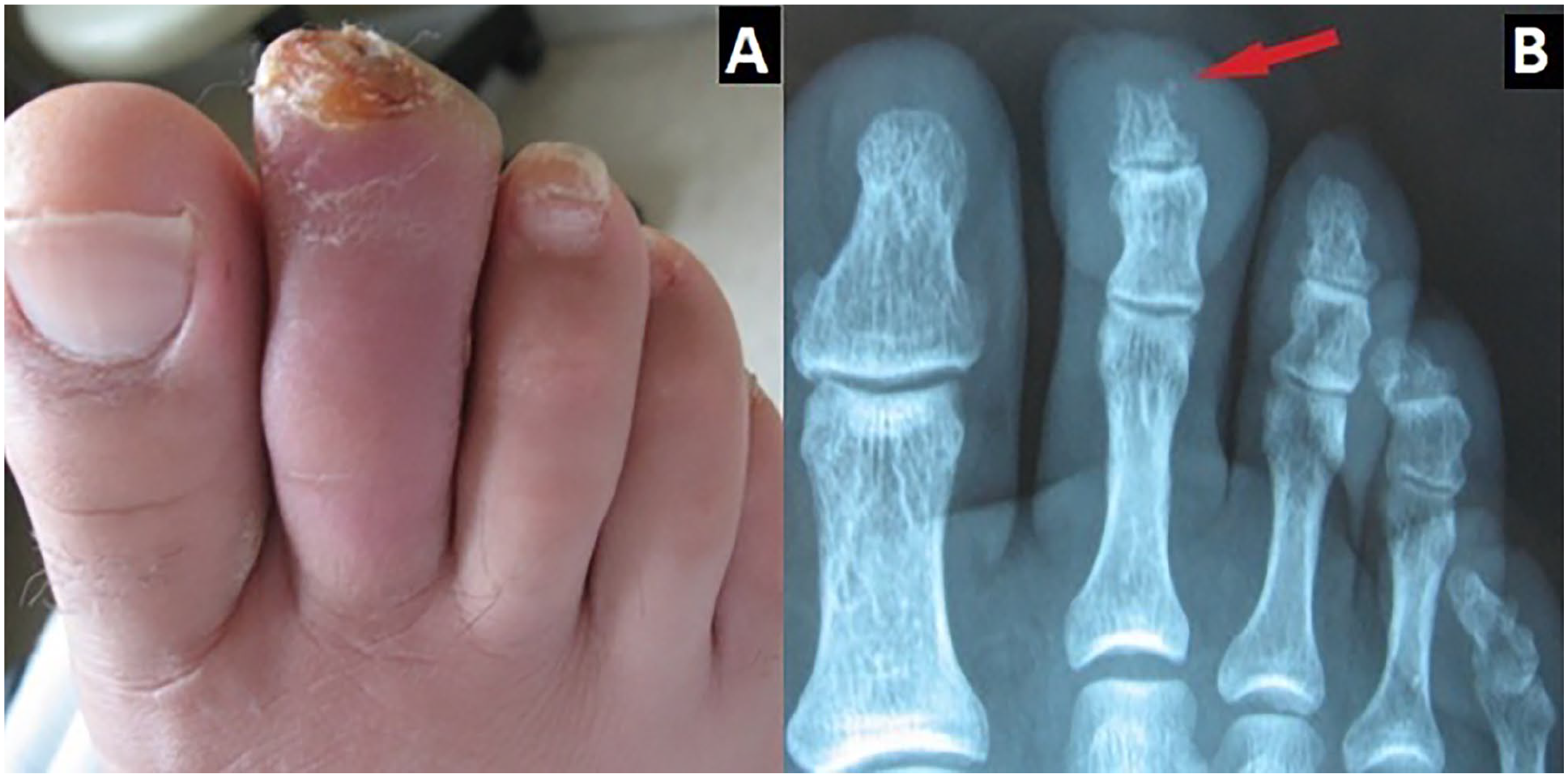
A foot with Morton toe: showing (A) a swelling and an ulcer of the second toe, and (B) a radiograph with bony erosion in the distal phalanx (arrow).
We also found that diabetes type 1 and younger age were significantly associated with increased risk for toe amputation. However, although a recent meta-analysis found no association between amputation and type of diabetes or age, similar findings to ours have been reported. 24 Diabetes type 1 can increase amputation because of more advanced disease severity, and younger age can increase amputation because of death being a competing risk factor in the older age group or as a result of older patients being more conservatively managed because of multiple factors.6,12,19
In our study, empirical antibiotics were administered without doing wound cultures because we did not have a microbiology laboratory in our center at the time and sending bacterial cultures to outside laboratories would have been inconvenient and expensive to the patients. Therefore, we had opted to perform cultures only for patients who had no response to empirical antibiotics. Antibiotics were given after debridement because we could not exclude residual bone infection after PPBE. Here, the duration of antibiotic ranged from 2 to 8 weeks according to wound status. Current guidelines in diabetic foot osteomyelitis recommend using antibiotics for 6 weeks. 26 It should be noted that although several studies had treated diabetic foot osteomyelitis with antibiotic alone without surgery, antibiotics are still widely used in association with surgery.17,26 Of interest, we found resistant organisms in bone cultures for patients with persistent infection such as methicillin-resistant Staphylococcus aureus, Pseudomonas aeruginosa, and Acinetobacter spp (Table 3). Infection with resistant organisms might result in worse outcome.18,29 Indeed, 1 patient who had methicillin-resistant S aureus had ended up with amputation.
Limitations of this study include a small sample, the use of clinical and radiographic criteria to diagnose osteomyelitis rather than bone biopsy or magnetic resonance imaging, which are considered the definitive diagnostic tests, and the need to use antibiotics, which might have acted as a confounder for the findings. We also could not prove that PPBE would avoid amputation because of the inherent limitation of the study design since it did not include a control group.
In conclusion, we have measured the outcome of PPBE in infected toe ulcers with underlying osteomyelitis among diabetic patients. We showed that PPBE could improve healing and would avoid inpatient stay. Health care teams should consider this procedure when faced with such cases.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231178530 – Supplemental material for Percutaneous Partial Bone Excision in the Management of Diabetic Toe Osteomyelitis
Supplemental material, sj-pdf-1-fai-10.1177_10711007231178530 for Percutaneous Partial Bone Excision in the Management of Diabetic Toe Osteomyelitis by Sameh R. Moosa, Ali H. Allan, Amr N. Younes, Faris G. Bakri and Nidal A. Younes in Foot & Ankle International
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the National Institute for Diabetes Endocrinology and Genetics ethical committee (approval number 1/2015).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.