
Abstract
The spring ligament is one of the main stabilizers of the medial arch of the foot and the primary static supporter of the talonavicular joint. Attenuation or rupture of this ligament is thought to play a central role in the pathophysiology of progressive collapsing foot deformity. Traditional correction of flexible flatfoot consists of posterior tibial tendon augmentation along with various osteotomies or hindfoot fusions. Repair or reconstruction of the spring ligament has not been as widely pursued. In recent years, newer techniques have been explored and may improve outcomes of traditional procedures, or possibly entirely replace some osteotomies. Combined spring-deltoid ligament reconstruction is also gaining traction as a viable technique, particularly as the ankle begins to deform into valgus. This review summarizes the variety of nonanatomic and anatomic reconstruction techniques that have been described, including autologous tendon transfers, allografts, and synthetic augmentation. Although many have only been characterized in biomechanical cadaver studies, this article reviews preliminary clinical studies that have shown promising results. There is a need for more high-quality studies evaluating the clinical, radiographic, and patient-reported outcomes following spring ligament reconstruction.
Introduction
Adult acquired flatfoot deformity (AAFD), 34 more recently termed progressive collapsing foot deformity (PCFD), 47 is an acquired deformity in 3 dimensions, with hindfoot valgus in the coronal plane, midfoot/forefoot abduction in the axial plane, and loss of the medial longitudinal arch in the sagittal plane. In addition to or independent from posterior tibial tendon (PTT) dysfunction, PCFD occurs with loss of ligamentous support across the hindfoot and midfoot.22,41
Surgery for PCFD usually includes a combination of osseous realignment and soft tissue reconstruction, predominantly of the PTT via tendon transfers. Realignment may be through osteotomy or fusion, and each procedure has its own risks and benefits. However, none of these procedures primarily corrects one of the key underlying pathologies, which is loss of ligamentous restraint of the hindfoot and midfoot joints.19,39,45,49
For most collapsing arch deformities, the primary subluxation is around the talus. This component of the deformity has been termed dorsolateral peritalar subluxation, which occurs through the talonavicular and subtalar joints and involves dorsolateral translation of the calcaneus and navicular relative to the talus. 64 Under weightbearing conditions, the main ligamentous support for these joints is the spring ligament. Attenuation or rupture of this ligament is intrinsic to flatfoot deformity in many, if not most, cases.21,29
Although isolated direct repair of this ligament has not proven successful, there is renewed interest in reconstruction of this ligament to support other bony and soft tissue procedures. The aim of this review is to provide an updated overview of the current indications and technique advancements for spring ligament reconstruction in the setting of PCFD with a focus on clinical studies.
Background
Spring Ligament Anatomy and Function
The calcaneonavicular, or spring, ligament runs from the sustentaculum tali of the calcaneus to the navicular. Three discrete components of the ligament have been described: the superomedial, inferior longitudinal, and medioplantar oblique bands. The spring ligament contains the head of the talus within the navicular and calcaneus, acting as a sling to orient the talus (Figure 1).17,66 With attenuation or rupture, the head of the talus can plantarflex, while the navicular and calcaneus rotate away, with resultant hindfoot valgus and abduction of the foot relative to the talus in the axial plane. The spring ligament is therefore the major restraint to talonavicular deformity, and is considered the primary static stabilizer of the medial longitudinal arch of the foot.34,66
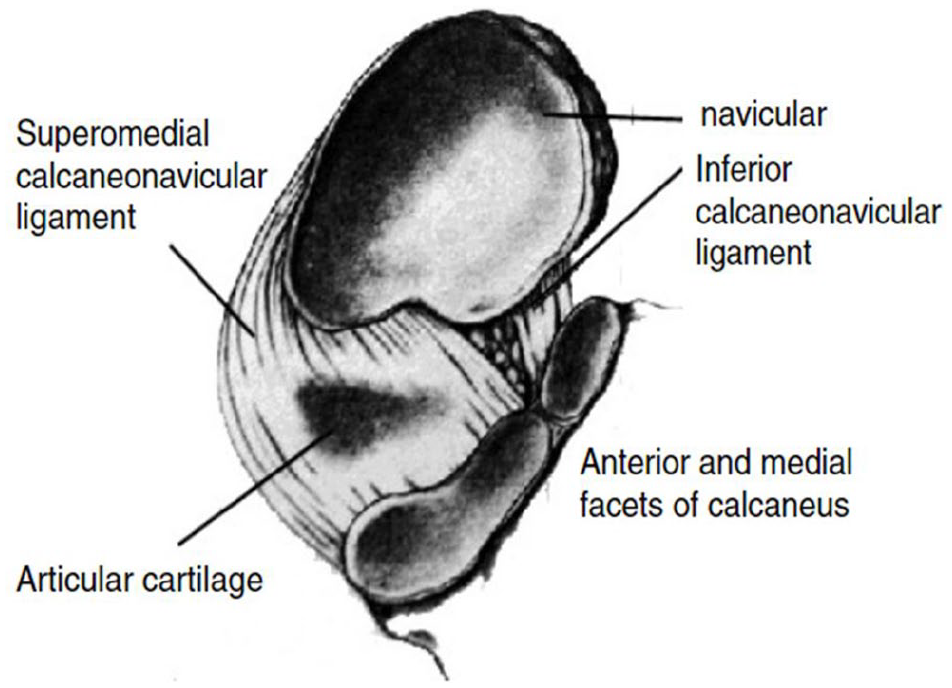
The spring ligament acts as a sling to orient the talus. Dorsal view of subtalar joint with talus removed demonstrating orientation and components of the spring (calcaneonavicular) ligament. Reprinted with permission from Davis et al. 17
In addition to the spring ligament, other static soft tissue structures that stabilize the medial arch include the deltoid ligament, plantar fascia, interosseous plantar and talocalcaneal (ITCL) ligaments, cervical ligament (CL), and the capsule of the talonavicular and naviculocuneiform joints.48,56 Interest has been also turned toward the ITCL and CL in particular, as the spring ligament might not be the only important medial arch ligament that fails in the setting of PCFD.45,60 The CL and ITCLs provide subtalar joint stability and have even been regarded as the “cruciate ligaments of the subtalar joint.” 35 The CL attaches proximally to the superolateral surface of the calcaneus and distally attaches to the talar neck, running diagonally through the sinus tarsi. 54 The ITCL runs just posterior to the CL in the sinus tarsi and is formed partially by the fusion of the capsules of the talocalcaneonavicular and subtalar joints.42,54 It emerges from the talar sulcus and inserts into the calcaneus just anteromedial to the posterior talocalcaneal joint capsule. 42
The deltoid ligament complex offers restraint to hindfoot valgus and talar external rotation. Anatomic studies have consistently demonstrated the blending of the superficial deltoid ligament with the superomedial spring ligament (Figure 2).10,16 This confluence has been described as a single entity, the tibiocalcaneonavicular ligament (TCNL). It has been suggested that further division of the TCNL is not anatomically or functionally useful because of the close relationship of these structures, and these anatomic considerations have affected how treatment for flatfoot is approached.9,16,41,48
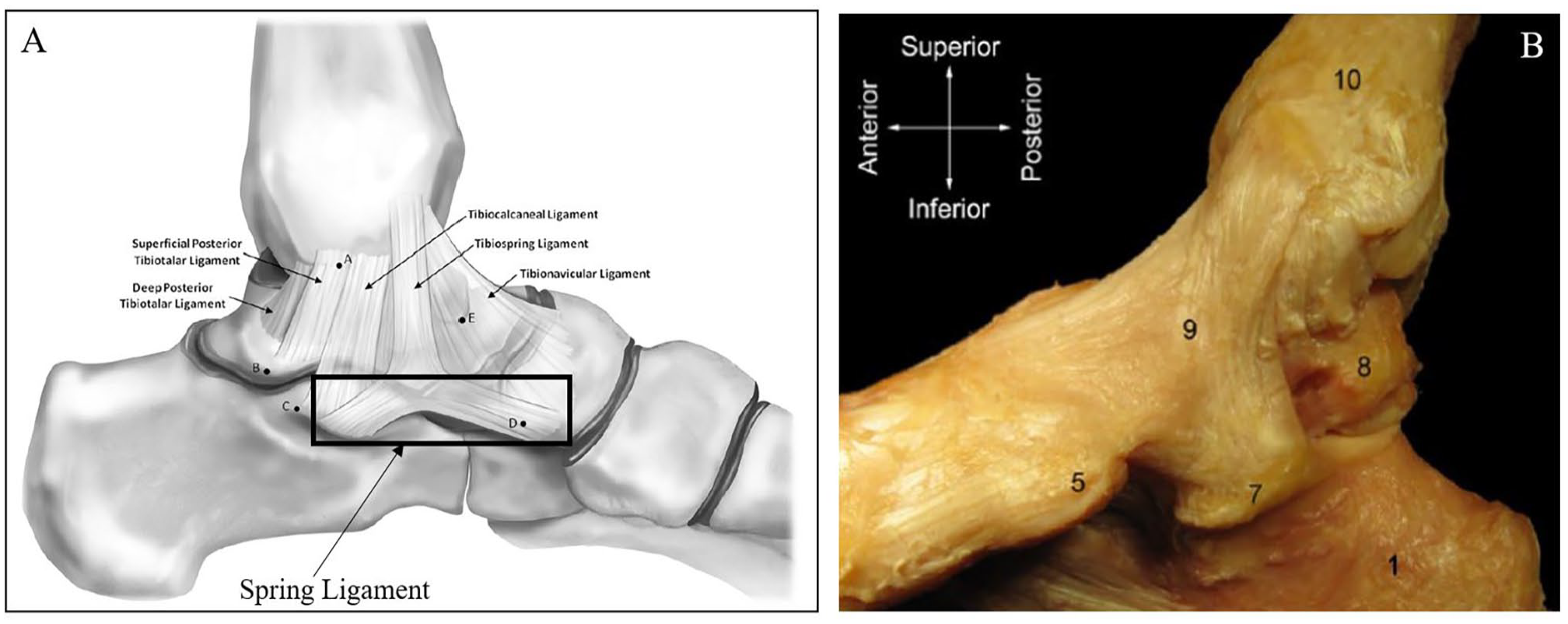
Medial ankle ligamentous complex anatomy. (A) Illustration of medial ligament complex demonstrating blending of spring ligament with superficial deltoid: point A, distal center of the intercollicular groove; point B, posteromedial talar tubercle; point C, posterior point of the sustenaculum tali; point D, tuberosity of the navicular; and point E, anteromedial corner of the trochlea. Reprinted with permission from Campbell et al. 10 Copyright 2014 by The Journal of Bone and Joint Surgery, Incorporated. (B) Cadaver image of medial ankle demonstrating tibiocalcaneonavicular ligament confluence: point 1, calcaneus; point 5, navicular; point 7, sustentaculum tali; point 8, talus; point 9, tibiocalcaneonavicular ligament; and point 10, tibia. Reprinted with permission from Cromeens et al. 16
Role of the Spring Ligament in Progressive Collapsing Foot Deformity
Traditionally, PCFD has been attributed to dysfunction of the PTT as it is the main dynamic supporter of the medial longitudinal arch.24,28,53 The PTT is important for effective gait, facilitating hindfoot inversion by locking the transverse tarsal joints.24,28,49,53 Just prior to heel rise in the gait cycle, the PTT fires to pull the hindfoot into slight varus. Thus, when the Achilles tendon activates to initiate heel rise, the calcaneal tuberosity will be more medial, as the force vector already favors that direction to support the arch. If the PTT does not fire sufficiently, the heel remains in more valgus, which is exacerbated by the lateralized vector of the Achilles, further flattening the arch and breaking down the spring ligament over time. 59 Alternate models propose the primary pathology is loss of the arch ligaments such as the spring ligament. Over time, the PTT may fail by repeatedly trying to overcome this arch collapse. Valgus orientation of the posterior facet of the subtalar joint may also predispose the calcaneus to translate laterally and place chronic pressure on the spring and other ligaments, resulting in flatfoot.3,13,55 Regardless of whether PTT dysfunction or spring ligament attenuation is a primary or secondary problem, loss of spring ligament integrity plays a central role in arch collapse pathogenesis.21,29,39,49
Clinically, spring ligament insufficiency has been implicated in the development of PCFD. Magnetic resonance imaging (MRI) studies have reported a high incidence of spring ligament attenuation in cases of PCFD. 21 Although rare, there have been reports of isolated spring ligament injury with an intact and healthy PTT that resulted in flatfoot deformity.8,46,51,65 The mechanism of injury is often due to a low-energy twisting mechanism, during sporting activity or walking.46,65 These patients are generally between the ages of 30 and 50 years.
It has also been demonstrated that PTT insufficiency alone does not result in PCFD. 49 Additionally, in the presence of spring ligament sectioning or the elongation of medial ligamentous complex structures, solely restoring the PTT may not be sufficient to alter or correct the deformity.39,49 Overall, these findings support the spring ligament’s crucial role in the development of flatfoot deformity. As the deltoid ligament forms a part of this medial ligamentous complex, it may be implicated earlier in disease progression than previously thought.
Presentation
Typically, patients present with progressive pes planus deformity and hindfoot valgus, often accompanied by medial-sided foot pain from PTT inflammation and/or degeneration. To facilitate a plantigrade foot in the setting of hindfoot eversion and valgus, there can be compensatory forefoot supination and abduction, sometimes fixed or rigid, as indicated by the “too many toes” sign. In the later stages, lateral-sided foot pain can occur from gradual subfibular and/or sinus tarsi impingement.1,38
Inability to perform a single-leg heel rise and weakened inversion are signs of a dysfunctional PTT. A characteristic finding of isolated spring ligament insufficiency is the ability to perform a single-leg heel rise with correction of the medial longitudinal arch and preserved inversion strength, but persistent forefoot abduction and heel valgus.46,65 Given the proximity of these structures, it is often difficult to distinguish causes of medial arch pain, but tenderness may be present more anteriorly to the medial malleolus if the spring ligament is involved. In contrast, more posteromedial pain along the course of the tendon may be attributed to the PTT.
A number of radiographic parameters are used to assess flatfoot deformity. Increased talonavicular uncoverage percentage and talo–first metatarsal angle, indicative of forefoot abduction, are seen on AP radiographs. On lateral x-ray, a decreased calcaneal pitch, increased talo–first metatarsal angle (Meary angle), and decreased medial cuneiform height all indicate loss of arch height. Ankle radiographs can reveal valgus tilt due to deltoid insufficiency and ankle arthritis.
Although MRI is not necessary for the diagnosis of PCFD, it can be used to evaluate the degree of damage to soft tissue structures, and bone marrow edema visualized on MRI can identify sites of impingement. Ultrasonography and tendoscopy have also been used to evaluate the soft tissue structures implicated in progressing flatfoot.4,30,33 Weightbearing computed tomography (WBCT), although not widely available, has emerged as a valuable tool in assessing PCFD. Unlike conventional radiographs, WBCT is not subject to variability caused by ankle rotation and allows for improved characterization of hindfoot deformity, peritalar subluxation, and lateral extra-articular impingement. 43 Discrepancies in measurement values of WBCT compared to clinical and radiographic examination have been observed, suggesting that conventional diagnostic tools may underestimate the degree of deformity.20,58 Implications of WBCT on treatment decisions and outcomes still need to be elucidated.
Treatment
Rationale for Treatment Considerations in PCFD
Operative intervention for PCFD is generally indicated once patients fail conservative treatment, experiencing persistent pain and deformity progression. Although the general risk factors for developing PCFD include a congenital flat foot, obesity, hypertension, diabetes, female sex, and injury to the medial arch ligaments and/or PTT, it is yet to be determined who is at higher risk of rapid deformity progression or failing conservative treatment. 67 Joint-sacrificing arthrodesis is typically reserved for patients with fixed or severe deformity or preexisting arthritis in affected joints. The surgical treatment of patients with flexible flatfoot is highly variable and depends on patient and deformity characteristics.
Traditional correction of flexible flatfoot consists of PTT augmentation along with various osteotomies or hindfoot fusions. The flexor digitorum longus (FDL) tendon is typically the tendon of choice for transfer, as it is immediately adjacent and has a similar line of pull as the PTT.1,28 Gastrocnemius or Achilles tightness may play a role as indicated before in exacerbating the deformity, and lengthening of the muscle or tendon is often included.
Medial displacement calcaneal osteotomy (MDCO) is a critical procedure in addressing collapsing foot deformity. Direct correlation between the amount of heel slide and hindfoot valgus correction has been established, and although this often does not fully realign peritalar deformity, correction of hindfoot valgus is a strong predictor of favorable clinical outcomes.11,15 Another main benefit is in medializing the Achilles insertion on the tuberosity, which can augment, rather than antagonize, the inversion force from the reconstructed PTT and FDL transfer. 59
Other osseous procedures are often used to enhance and balance foot realignment, such as midfoot osteotomies (Cotton), lateral column lengthening (LCL), and selective midfoot or hindfoot fusions. Each of these procedures has limitations, including insufficient correction or undesired stiffness. For example, LCL increases lateral plantar pressure and may induce lateral-sided foot pain.7,23,26,37,50 Overcorrection with LCL has also been associated with worse clinical outcomes, stress fractures, and high rates of nonunion.14,18,31 However, perhaps the biggest drawback to any of these procedures is that they do not address the primary problem in most deformities, which is loss of spring ligament support.
Spring ligament reconstruction has been increasingly pursued to directly address an underlying driver of deformity and minimize complications associated with osteotomies or fusions. Nevertheless, the current indications reported for spring ligament reconstruction are not consistent in the literature. Some authors use spring ligament reconstruction to avoid the use of LCL or bony procedures,2,62 whereas others have used it to correct residual deformity following LCL.22,68
Spring Ligament Repair
Direct, isolated spring ligament repair has not been widely pursued for flatfoot correction because it is likely inadequate. However, it may be considered in the rare case of an isolated acute spring ligament rupture or in those with an adequate amount of healthy tissue (Tables 1 and 2).8,46,51,65
Clinical Studies Characteristics.
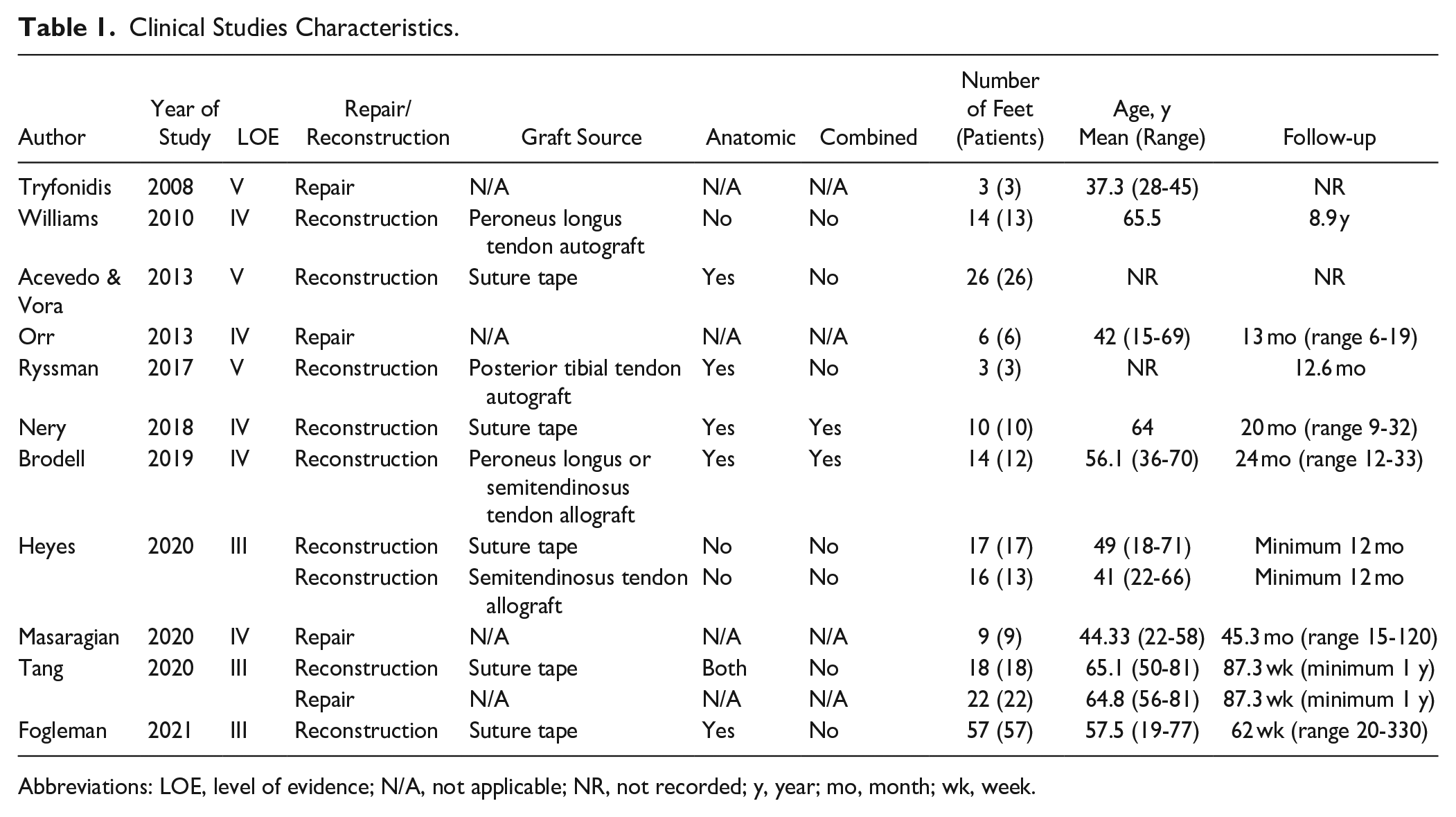
Abbreviations: LOE, level of evidence; N/A, not applicable; NR, not recorded; y, year; mo, month; wk, week.
Patient Outcomes Following Spring Ligament Repair/Reconstruction.
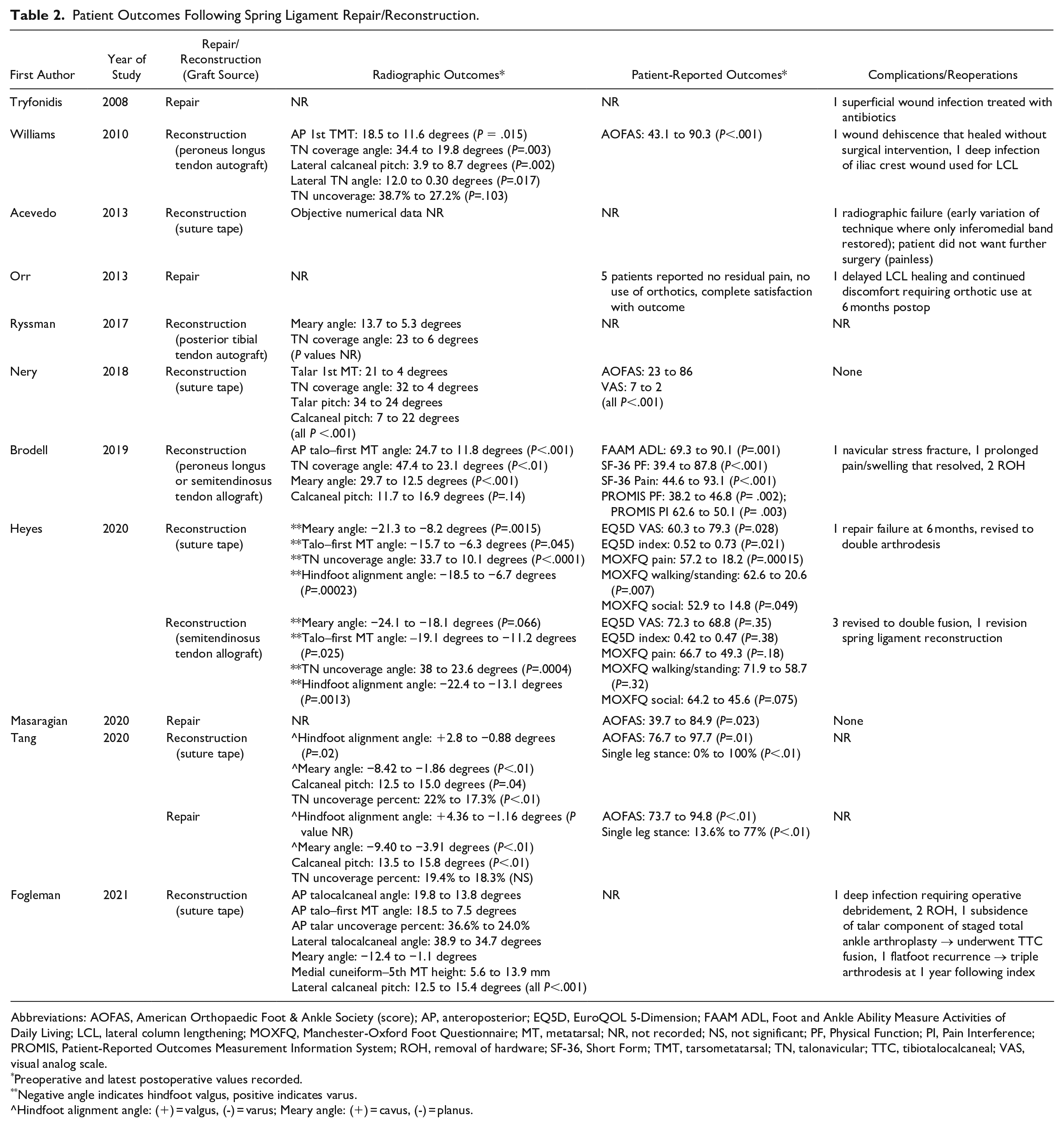
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society (score); AP, anteroposterior; EQ5D, EuroQOL 5-Dimension; FAAM ADL, Foot and Ankle Ability Measure Activities of Daily Living; LCL, lateral column lengthening; MOXFQ, Manchester-Oxford Foot Questionnaire; MT, metatarsal; NR, not recorded; NS, not significant; PF, Physical Function; PI, Pain Interference; PROMIS, Patient-Reported Outcomes Measurement Information System; ROH, removal of hardware; SF-36, Short Form; TMT, tarsometatarsal; TN, talonavicular; TTC, tibiotalocalcaneal; VAS, visual analog scale.
Preoperative and latest postoperative values recorded.
Negative angle indicates hindfoot valgus, positive indicates varus.
^Hindfoot alignment angle: (+) = valgus, (-) = varus; Meary angle: (+) = cavus, (-) = planus.
Biomechanical studies assessing spring ligament repair have not produced promising results (Table 3). In one study, 8 of the 8 repairs failed after cyclic loading of the construct. 5 In a different study, lateral translation of the foot following spring ligament sectioning (39.2 ± 10.9 mm) did not improve with repair (34.2 ± 9.5 mm, P = 0.472). Lateral translation was restored to the level of the intact condition only following synthetic suture anchor reconstruction. 52
Biomechanical Studies Characteristics.
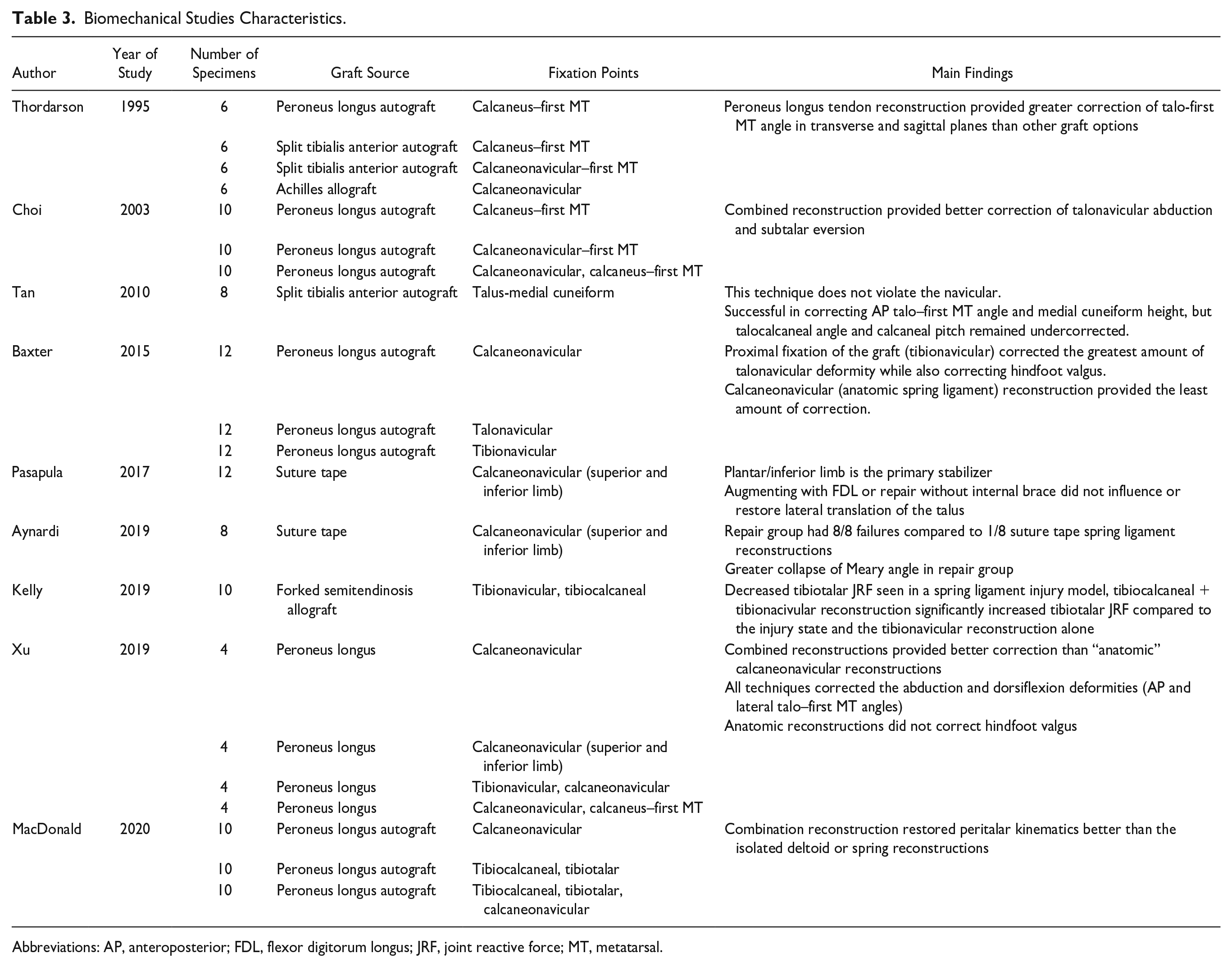
Abbreviations: AP, anteroposterior; FDL, flexor digitorum longus; JRF, joint reactive force; MT, metatarsal.
On the other hand, there have been reports of successful repair in a few small case series. In one series of patients with isolated spring ligament injury and resultant flatfoot who failed 3-4 months of nonoperative treatment, 6 of the 9 patients had a history of minor trauma to the involved foot and were initially treated for a medial ankle sprain. 46 Four patients already presented with forefoot abduction and/or hindfoot valgus, whereas the remaining 5 were treated before these deformities developed. Patients underwent adjunct MDCO and/or LCL as necessary for deformity correction. For all but 1 patient treated with an open repair, endoscopic repair with a suture passer and a sliding knot was performed. 46 At 1 year postoperatively, AOFAS scores improved without any complications. There was no difference in AOFAS improvement in those who underwent additional procedures, and difference in outcomes depending on initial deformity was not reported.
In a series of patients with a more insidious onset of medial arch pain (mean 27 months, range 5-30), 51 all but 1 (5/6) underwent concomitant procedures in addition to primary spring ligament repair, with 4 undergoing LCL. Direct repair in an “interrupted manner” was carried out with absorbable or nonabsorbable suture, without the use of suture anchors, allograft, or tendon augmentation. 51 At a mean follow-up of 13 months, none had residual deformity and all but 1 were pain free without orthotics. 51
Finally, a recent clinical study comparing direct repair to repair with synthetic augmentation in patients with flexible flatfoot showed improved talonavicular coverage and an increased number of patients able to complete single-leg heel rise in the synthetic group at a minimum follow-up of 1 year. 62 It is important to note that no patient in the synthetic group underwent a concomitant bony procedure, whereas all patients who underwent repair had an MDCO. 62 These studies suggest that direct repair is inadequate on its own, and some of the reported positive outcomes may be confounded by the supplementary procedures performed.
Spring Ligament Reconstruction: Nonanatomic Tendon Transfers and Allografts
For reconstruction of the spring ligament, anatomic (reconstructing the ligament with fixation points in the calcaneus and navicular) and nonanatomic approaches using a variety of tendon transfers and allografts have been described. One of the more commonly reported techniques in the literature is the use of peroneus longus (PL) autograft, preserving its distal insertion and rerouting the tendon through a proximal bone tunnel. For the proximal fixation point, the PL has been secured directly to the calcaneus, passed through the navicular before being anchored to the calcaneus or vice versa, or even passed through the tibia and secured to fibular screw posts.12,63,68
In one biomechanical study, PL autograft that was passed directly medial to lateral through the calcaneus provided the most robust correction compared to 3 other reconstruction techniques with different graft sources (Supplemental Figure 1A). 63 Another biomechanical study tested a combined, “anatomic” spring ligament reconstruction that first rerouted the PL through both anterior and posterior calcaneal drill holes, and then finally from dorsal to plantar through a navicular tunnel (Supplemental Figure 1B). 12 When compared to isolated plantar and superomedial reconstructions, this combination approach provided a significantly greater deformity correction. 12
Nonanatomic PL autograft spring ligament reconstruction has been tested clinically in a case series where LCL did not fully correct talonavicular deformity. 68 Again, the PL was left at its insertion on the first metatarsal, and was passed from dorsal to plantar through a navicular bone tunnel. If only residual abduction was observed at the talonavicular joint, the proximal fixation point for the graft was the tibia (Supplemental Figure 1C). If significant residual plantar sag was observed at the talonavicular joint, the proximal fixation point was in the calcaneus instead, to create the slinglike effect of the spring ligament under the talar head (Supplemental Figure 1D). The authors postulated that inserting the graft into the calcaneus would better support collapse in the sagittal plane, whereas inserting the graft into the tibia would better support abduction through the talonavicular joint. Successful correction from both methods was observed in this study at a mean follow up of 8.9 ± 1.8 years. 68
Split tibialis anterior (TA) autograft has been tested biomechanically with questionable results. Thordarson and colleagues tested 2 TA approaches that did not provide as strong of a correction compared to their PL autograft. 63 Leaving the TA distal insertion intact, the medial third of the tendon was passed from dorsal to plantar through the navicular and from medial to lateral through the calcaneus (Supplemental Figure 1E). The second TA technique did not violate the navicular, and the graft was passed directly through the calcaneal bone tunnel (Supplemental Figure 1F). Another biomechanical study only tested their TA graft at static loads and found that talocalcaneal angle and calcaneal pitch remained significantly undercorrected. 61 For this technique, the graft was secured in bone tunnels in the inferomedial talus, passing from plantar to dorsal through the medial cuneiform. To our knowledge, the TA autograft approach has not been applied in a clinical setting.
Finally, an Achilles tendon allograft technique has been described and applied clinically. 25 The graft was passed from dorsal to plantar through the navicular, into the medial malleolus through a tibial bone tunnel, and then secured to fibular screw posts. The graft was passed so the calcaneal bone block end was secured in the dorsal aspect of the navicular (Supplemental Figure 1G). The authors felt that an anatomic calcaneonavicular reconstruction where the tendon is fixed proximally through a calcaneal bone tunnel provides less consistent results. 25 Anecdotally, securing the graft through the medial malleolus and tibia more strongly supported the medial arch, emphasizing the confluence of the anterior deltoid with the spring ligament that provides support for the talonavicular joint. If sag persisted at the talonavicular joint despite adequate reduction of abduction using a single allograft, a second graft was placed from the navicular through the calcaneus, essentially performing a TCNL reconstruction. 25
Spring Ligament Reconstruction: Anatomic Tendon Transfers/Allografts
Truly anatomic autograft and allograft reconstructions are less common. One of the 4 methods described by Thordarson and colleagues used an Achilles tendon allograft to create a calcaneonavicular reconstruction (Supplemental Figure 2A). 63 Unlike the previously described Achilles tendon technique, the bone plug was secured in the medial aspect of the calcaneal bone tunnel, and then the remainder of the graft was passed from plantar to dorsal through the navicular and sewn to itself. Again, this did not perform as well as the PL tendon transfer, where the tendon’s distal insertion was left intact and the proximal end was rerouted through the calcaneus. 63
In a finite element model assessing 4 different PL reconstructions, anatomic spring ligament reconstructions (sustentaculum tali to navicular with 1 or 2 limbs) (Supplemental Figure 2B) were tested against 2 “nonanatomic” reconstructions (Supplemental Figure 2C). 69 Using the CT and MRI of a healthy male volunteer, 28 bones, sesamoids, plantar fascia, 24 ligaments, cartilage, and soft tissues were included in the finite element model. The “nonanatomic” reconstructions were superior, and interestingly, the one that provided the most robust construction had fixation points in the tibia, calcaneus, and navicular, simulating the native TCNL. 69 Limitations of this model include it was based on a healthy foot, the loading model was representative of standing rather than walking, and several simplifications were introduced in the modeling process, such as using material properties for soft tissues from the literature instead of actual measurements. 69
One case series even used the PTT to reconstruct the spring ligament, preserving the PTT distal insertion and releasing it proximally. 57 The proximal stump was then passed through a single bone tunnel in the sustentaculum tali to re-create the calcaneonavicular ligament attachment (Supplemental Figure 2D). One major limitation to this technique is using a torn or degenerated PTT, which is highly likely in the setting of flatfoot, and can compromise the reconstruction.
Altogether, these studies highlight the complexity of the medial ligamentous complex anatomy and the ongoing discrepancies in the definitions of its components. The distinction between anatomic vs nonanatomic likely bears less importance than the graft source and specific fixation points that support the arch as much as possible across the entire medial column from the ankle to the midfoot. Overall, there are a variety of options for reconstructing the spring ligament with auto- or allograft, none of which have been extensively studied in a clinical setting. Favorable results have been reported regarding maintaining deformity correction in the few clinical studies that have been published (Tables 1 and 2).57,68
Spring Ligament Reconstruction - Synthetic Augmentation
Limitations to autologous tendon transfers include donor site morbidity, nonanatomic reconstructions, and potentially limited availability due to the altered state of a native tendon. Allografts can eliminate the risk of donor site morbidity although they may take longer to incorporate into the recipient. Especially in the setting of an attenuated spring ligament, augmentation with synthetic material, such as collagen-coated suture tape, can reinforce the spring ligament and stabilize the talar head. This method has shown promise in biomechanical studies (Table 3),5,52 and the typical approach involves anchoring suture tape in the sustentaculum tali. Then, 2 limbs of suture tape are passed distally through the navicular, medial cuneiform, or 1 in each bone (Figure 3).
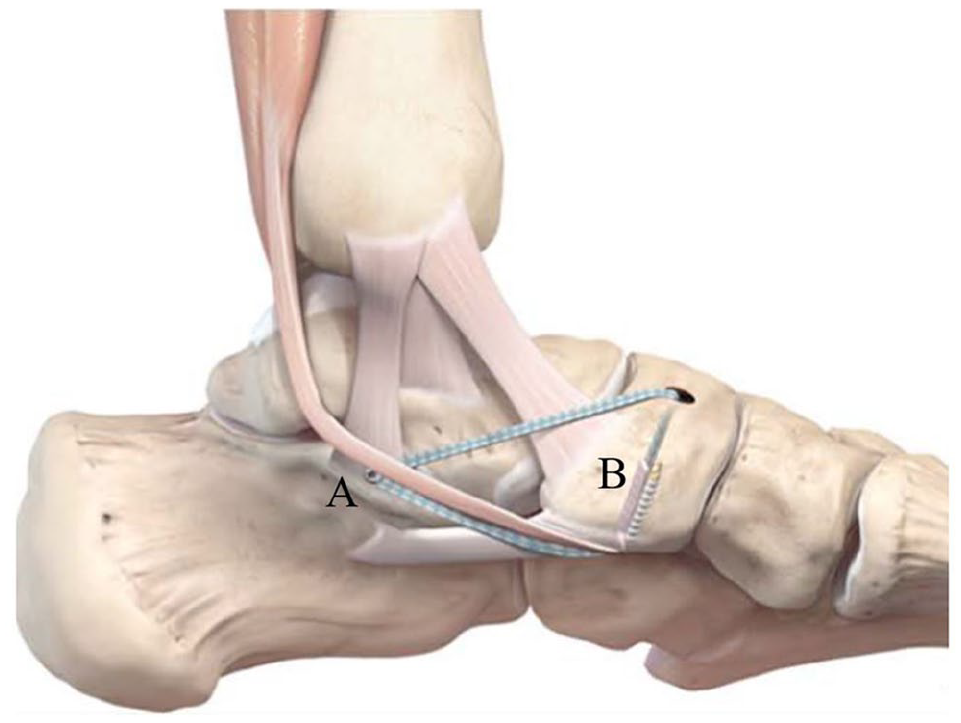
Synthetic spring ligament reconstruction/augmentation with suture tape. Medial ankle image of suture tape anchored in the sustentaculum tali (point A) and 2 limbs of suture tape passed dorsal to plantar and plantar to dorsal, respectively, through navicular bone tunnel and secured with an interference screw (point B). Reprinted with permission from Acevedo and Vora. 2
Acevedo and Vora were the first to report synthetic augmentation in a series of 26 patients, reporting nonspecific but favorable radiographic outcomes. 2 For this technique, the 2 limbs of suture tape were anchored in the sustentaculum tali. One limb was passed dorsal to plantar through the navicular to replicate the superomedial band of the spring ligament, and the other limb was passed plantar to dorsal to create the inferior band. The FDL tendon was passed with the inferior band to complete the FDL transfer, and the native spring ligament was tensioned and repaired after the synthetic augmentation was secured. 2
A larger retrospective review of 57 patients who underwent the same reconstruction corroborated the success of this method, reporting significant improvements in all measured radiographic parameters (AP talocalcaneal angle, talo–first MT angle, talar uncoverage percentage; lateral talocalcaneal angle, talo–first MT angle, medial cuneiform–fifth MT height, calcaneal pitch) at an average follow-up of 62 ± 46.5 weeks (range 20-330 weeks) (Table 2). 27 Five patients had subsequent operations for symptomatic hardware removal (x2), debridement of deep infection, recurrence of flatfoot, and subsidence of the talar component in a case of flatfoot reconstruction with a staged total ankle arthroplasty. All patients underwent concomitant procedures as part of their flatfoot reconstruction, and it was found that reconstruction that included either a subtalar fusion or MDCO led to statistically significant postoperative radiographic changes. These findings highlight how it is difficult to assess the isolated contribution of spring ligament reconstruction in the setting of concomitant procedures. Concomitant procedures performed in clinical studies are presented in Table 4.
Concomitant Procedures Performed in Addition to Spring Ligament Reconstruction or Repair.
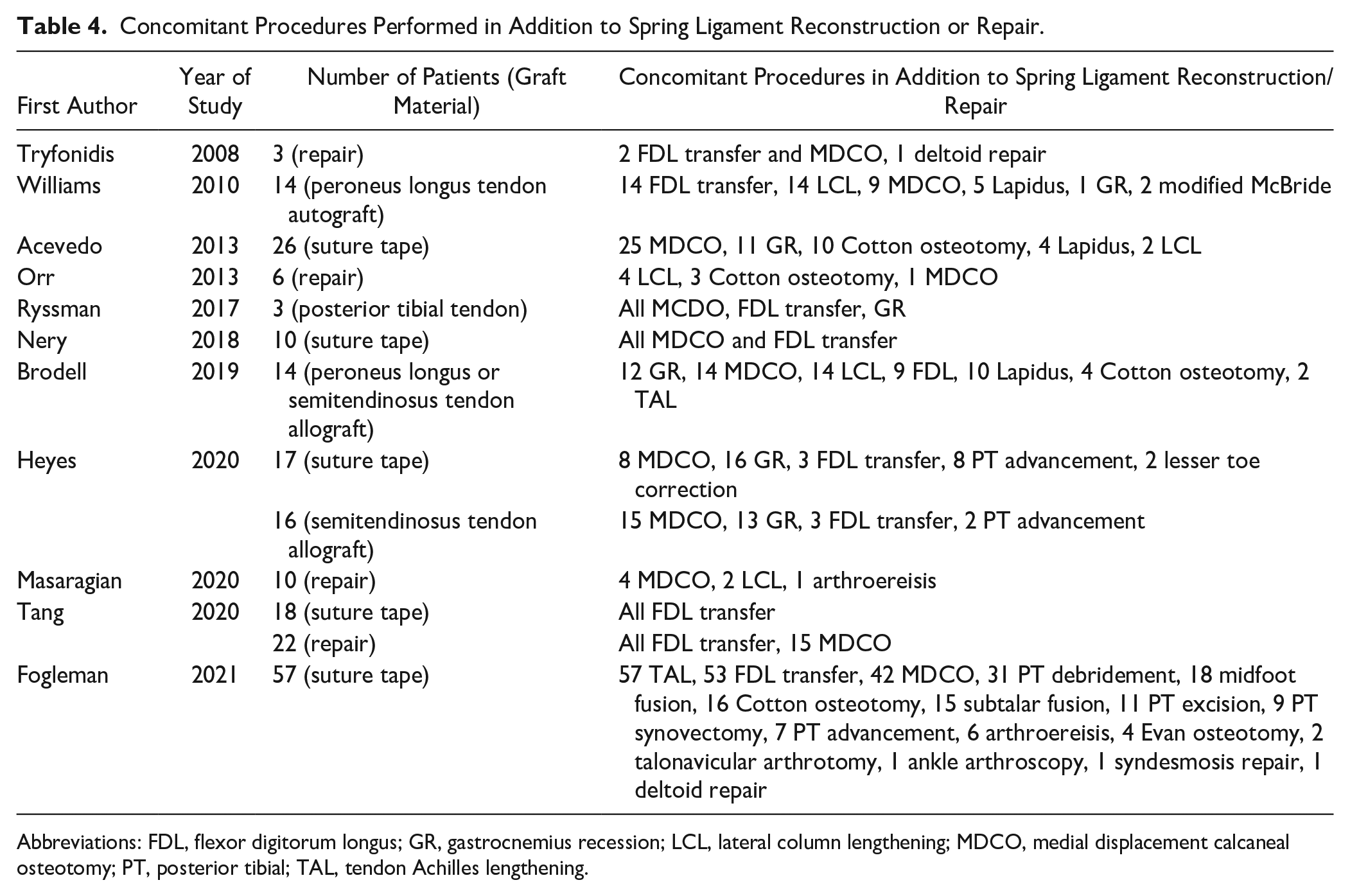
Abbreviations: FDL, flexor digitorum longus; GR, gastrocnemius recession; LCL, lateral column lengthening; MDCO, medial displacement calcaneal osteotomy; PT, posterior tibial; TAL, tendon Achilles lengthening.
Furthermore, comparative studies have demonstrated favorable outcomes following repair with synthetic augmentation compared to other techniques (Table 2).36,62 One of these used the technique described by Acevedo and Vora, but if lateral weightbearing preoperative radiographs showed the medial cuneiform sagging relative to the navicular, then only one of the limbs of suture tape was anchored to the navicular, and the other was anchored to the medial cuneiform. 62 As previously mentioned, synthetic augmentation reconstruction with suture tape generated better clinical and radiographic outcomes compared to direct repair, without the need for bony procedures. 62
Heyes et al 36 compared synthetic augmentation to semitendinosus allograft. Their synthetic technique involved proximal fixation to the sustentaculum tali but distal fixation to the medial cuneiform instead of the navicular to additionally reconstruct the naviculocuneiform ligament.36,60 The semitendinosus allograft was secured proximally at the junction of the talar neck and body, passed through the navicular, and secured back onto itself on the plantar medial side of the navicular to correct any residual forefoot abduction. Synthetic reconstruction provided greater correction of all radiographic parameters (Meary angle, talo–first MT angle, TN uncoverage angle, hindfoot alignment angle) at 6 and 12 months postoperatively, but the most notable differences between these 2 techniques were seen in patient-reported outcomes (PROs) (Table 2). 36 From baseline to 12 months following operation, all PROs (EQ5D VAS and index; MOXFQ pain, walking or standing, and social) improved in the synthetic group, whereas there was no improvement from baseline in the hamstring group (Table 2). Three patients had synthetic ligament reconstruction in one foot and hamstring allograft in the other. Interestingly, all 3 subjectively preferred the synthetic reconstruction side. 36 This highlights the importance of comparative clinical studies and collection of PROs. Even though the hamstring allograft was able to objectively correct deformity, it did not produce the same improvement in PROs. Because the reconstruction anchoring points and other aspects of the surgical technique differed notably between the study groups, it is difficult to determine which factors contributed most to the difference in outcomes.
Combined Spring and Deltoid Ligament Reconstruction
Combined spring and deltoid ligament reconstruction is also gaining traction as a viable technique, as the anatomy of the medial ankle ligaments is more thoroughly understood.10,16 Grunfeld et al 32 was the first to describe a combined approach, inserting a folded portion of either a forked semitendinosus or PL allograft into a vertically oriented medial malleolar bone tunnel. Then, one limb was passed dorsal to plantar through the navicular, and the other medial to lateral through the calcaneus. The FDL tendon was sutured to the PTT distal stump and also passed through the navicular tunnel and tensioned together with the navicular limb of the allograft. 32
Biomechanical studies have supported the efficacy of this technique (Table 3).6,40,44 One study demonstrated that spring ligament injury diminishes the tibiotalar joint reactive force, contributing to ankle joint instability. 40 Using a reconstruction similar to that described by Grunfeld et al, 40 enhanced restoration of joint reactive force was seen with this combined tibiocalcaneonavicular approach (Supplemental Figure 3A). Furthermore, a study using native PL tendon showed that a combined TCNL reconstruction was superior to isolated spring or deltoid reconstructions in restoring peritalar kinematics (Supplemental Figure 3B). 44 Although increased size of the spring ligament tear correlated with increased valgus alignment of the subtalar joint, isolated spring ligament reconstruction was not able to fully correct subtalar and tibiotalar valgus deformity. TCNL reconstruction, however, was able to correct both. 44 Another study compared 3 different reconstruction configurations using a PL autograft: tibionavicular, talonavicular, and anatomic spring ligament (calcaneonavicular) (Supplemental Figure 3C). 6 The tibionavicular reconstruction corrected the abduction, talonavicular eversion, and hindfoot valgus deformities significantly more than the other techniques. 6 Of note, all 3 of these studies looked at ligament reconstructions in isolation, and no concomitant procedures were performed.
Two clinical case series support the promise of the combined technique (Tables 1 and 2).9,48 At an average follow-up of 24 months (range 12-33) following combined reconstruction, improved radiographic parameters and PROs were observed. 9 In this series, 6 patients were treated with the technique as described by Grunfeld et al, whereas 8 underwent a modified technique where after passing the graft through the navicular, it was then rerouted back to the sustentaculum tali in a figure-of-8 fashion (Supplemental Figure 3D). This allowed for an inferior limb reconstruction in addition to the superomedial reconstruction. However, this construct seemed to increase stress at the navicular tunnel, potentially contributing to the development of a navicular stress fracture in 1 patient. 9 Of note, neither outcomes between the 2 graft techniques nor the 2 patient groups (stage IIB and stage IV; PCFD A1B1 and E1) were compared.
Combined reconstruction of the spring and deltoid ligaments with suture tape has also been tested clinically. 48 Following native deltoid and spring ligament repair with an imbrication suture, 2 limbs of suture tape were anchored in the medial malleolus, and passed to the sustentaculum tali and talar neck, respectively. Then, using a second anchor, 2 additional limbs of suture tape were passed from the sustentaculum tali through a navicular bone tunnel (Supplemental Figure 3E). Improved radiographic parameters and PROs were seen at an average follow-up of 20 months (range 9-32). 48 The rationale for pursuing combined reconstruction is the concern that isolated reconstructions might not fully restore combined tibiotalar, tibionavicular, and subtalar joint stability. 9
Conclusion
The role of the spring ligament and other static medial soft tissue structures in PCFD have been increasingly recognized, leading to the pursuit of medial soft tissue reconstructive techniques. Spring ligament reconstruction is likely a viable technique for reducing talonavicular abduction and potentially the degree of correction needed from certain osteotomies or fusions. The recognition of the close relationship between the spring and deltoid ligaments has prompted the development of combined reconstructive techniques, with promising initial results that suggest a combined approach may be superior. Future work should also focus on assessing the contribution of other medial/plantar arch ligaments to pathogenesis, and continued elucidation of proper indications for the wide variety of surgical options is needed. Furthermore, there is a lack of prospective randomized clinical studies with larger cohorts, longer follow-up periods, and patient-reported outcome scores.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231178538 – Supplemental material for Spring Ligament Reconstruction for Progressive Collapsing Foot Deformity: Contemporary Review
Supplemental material, sj-pdf-1-fai-10.1177_10711007231178538 for Spring Ligament Reconstruction for Progressive Collapsing Foot Deformity: Contemporary Review by Bonnie Y. Chien, Justin K. Greisberg and Emily Arciero in Foot & Ankle International
Supplemental Material
sj-pdf-2-fai-10.1177_10711007231178538 – Supplemental material for Spring Ligament Reconstruction for Progressive Collapsing Foot Deformity: Contemporary Review
Supplemental material, sj-pdf-2-fai-10.1177_10711007231178538 for Spring Ligament Reconstruction for Progressive Collapsing Foot Deformity: Contemporary Review by Bonnie Y. Chien, Justin K. Greisberg and Emily Arciero in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.