
Abstract
Lower extremity ambulatory assistive devices (LEADs) are important augments that provide mobility and stability when weightbearing is restricted in the setting of injury, surgery, or balance disorders. In order to optimize patient safety and function when prescribing these devices, it is essential for the orthopaedic surgeon to have a firm understanding of their specific indications, proper fitting, energy demand, biomechanical advantages, and potential complications. Comprehension of normal gait cadence, identification of the functional deficit present and knowledge of available options will assist in safely prescribing the proper device. Over the last decade, newer alternatives to traditional LEADs (canes, crutches, walkers) have become available, including the rolling knee scooter and hands-free single crutch. These have been developed to improve mobility and independence; however, it is necessary to appreciate their limitations when prescribing them to patients. This review will provide an update on normal and pathologic gait biomechanics as well as the most common types of LEADs currently available to the orthopaedic surgeon, their indications, important considerations, proper fitting, associated energy expenditure, and complications.
Introduction
Lower extremity ambulatory assistive devices (LEADs) are important augments that provide mobility and stability when weightbearing is restricted in the setting of injury, surgery, or balance disorders. In order to optimize patient safety and function when prescribing these devices, it is essential for orthopaedic surgeons and other providers to have a firm understanding of their specific indications, proper fitting, energy demand, biomechanical advantages, and potential complications. Comprehension of normal gait cadence, identification of the functional deficit present, and knowledge of available options will assist in safely prescribing the proper device. Over the last decade, new alternatives to traditional LEADs have become available, including the rolling knee scooter, hands-free single crutch, dynamic ankle foot orthoses (AFOs), and exoskeletal devices. These have been developed to improve mobility and independence; however, it is necessary to appreciate their limitations when prescribing them to patients. This review will provide an update on the most common types of LEADs currently available, their indications, important considerations, proper fitting, associated energy expenditure, and complications.
Background
Lower extremity assistive devices (LEADs) are important augments to allow safe mobilization in a variety of patient populations. 2 Most commonly, they are prescribed to geriatric patients for gait stabilization due to decreased physical conditioning, vestibular dysfunction, neuromuscular disease, or neuropathy. 30 In 2011 alone, roughly 8.5 million (25%) adults >65 years of age reported using an ambulatory assistive device, with a third of these patients reporting multiple device usage. 15 These statistics have increased substantially because of an aging population. 1 In the orthopaedic population, these devices serve an important role in postoperative patients who have been made partial or nonweightbearing and those who are full weightbearing but have residual weakness after surgery.
The effects of prolonged immobilization are well documented. Musculoskeletal complications include decubitus ulcers, muscular atrophy, contractures, disuse osteopenia, and degenerative joint disease. 10 Perhaps more pressing are the increased cardiovascular risks, which include increased rates of venous thromboembolism (VTE), cardiac deconditioning, and orthostatic hypotension. 10 Orthopaedic procedures, especially those involving the lower extremity, have higher rates of VTE. 11 When possible, early weightbearing and joint mobilization has been shown to decrease the rate of VTE. 22 This highlights the importance of appropriately prescribed LEADs and mobilization in postoperative patients.
The goal of LEADs is to prevent these complications through stabilization of gait. This is accomplished biomechanically through broadening the base of support of the user, improving balance and stability, reducing the load to one of the lower limbs, augmenting muscle action, assisting propulsion, and transmitting somatosensory cues to noninjured extremities, which ultimate lowers energy expenditure for the patient. 12 There are numerous devices that accomplish this goal; however, special consideration must be given to patient factors in order to optimize outcomes.
Choosing optimal LEADs for patients requires an understanding of their gait, cognitive function, physical endurance, living environment, judgment, vision, vestibular function, and upper body strength to prevent further injury or complications. 12 Physical therapy plays an important role in determining proper LEADs for patients and they can provide gait and device training. Referral should be considered for patients who demonstrate improper use due to weakness, need device training, or if there are concerns for improper device selection, which may increase risk for falls.
The purpose of this review is to provide an updated review on the most common types of LEADs currently available to the orthopaedic surgeon. Understanding their indications, important considerations, proper fitting, associated energy expenditure, and complications will allow for proper selection and optimize patient outcomes. Table 1 is an overview of LEADs.
An Overview of Traditional and Novel LEADs for Reference. a
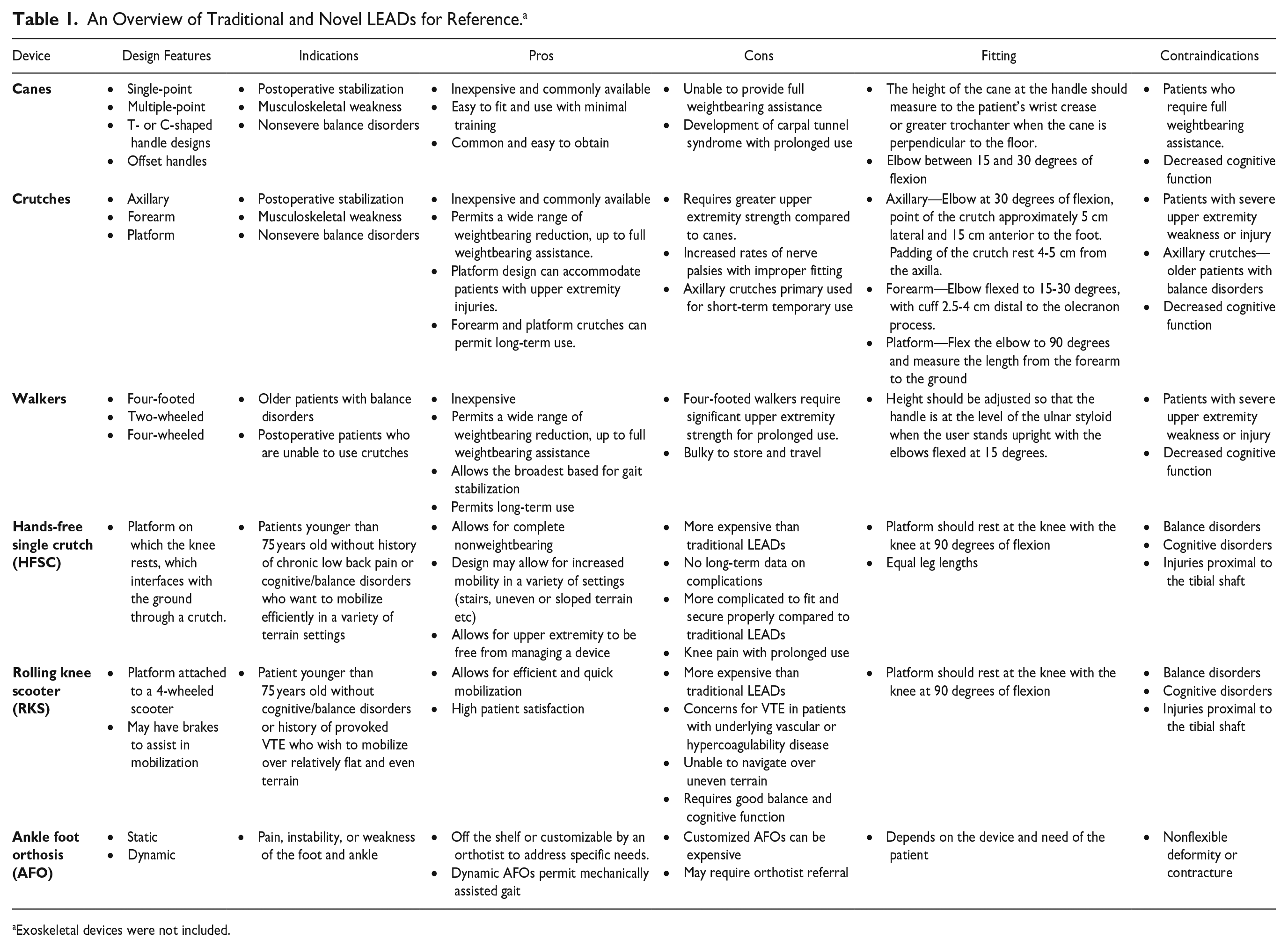
Exoskeletal devices were not included.
Traditional Leads
Cane
The cane is the most commonly used ambulatory assistive device, and it is reported that up to 67% of patients obtain them from nonmedical professionals.15,29 There are various types of cane designs based on the material of construction, handle, offset, and base design. In terms of handle design, there are C- and T-shaped handles. Data supports that the T-shaped handle disperses forces across the hand more evenly, which may lead to lower rates of carpal tunnel syndrome. 2 Offset in cane design refers to a bend in the shaft of the cane near the handle which positions the axis of weight distribution in-line down the shaft of the cane. In nonoffset designs, the axis of weight distribution is often a few centimeters behind or in front of the shaft of the cane. Optimizing the axis of weight distribution in line with the shaft of the cane is more effective in offloading the affected extremity. 27 The base design differs on the amount of contact points that engage the ground. The most commonly seen are the single-point, 3-point, and 4-point designs. Increasing contact points and the distance between these contact points increases stability for the user. 28 Figure 1 demonstrates different cane types and characteristics.
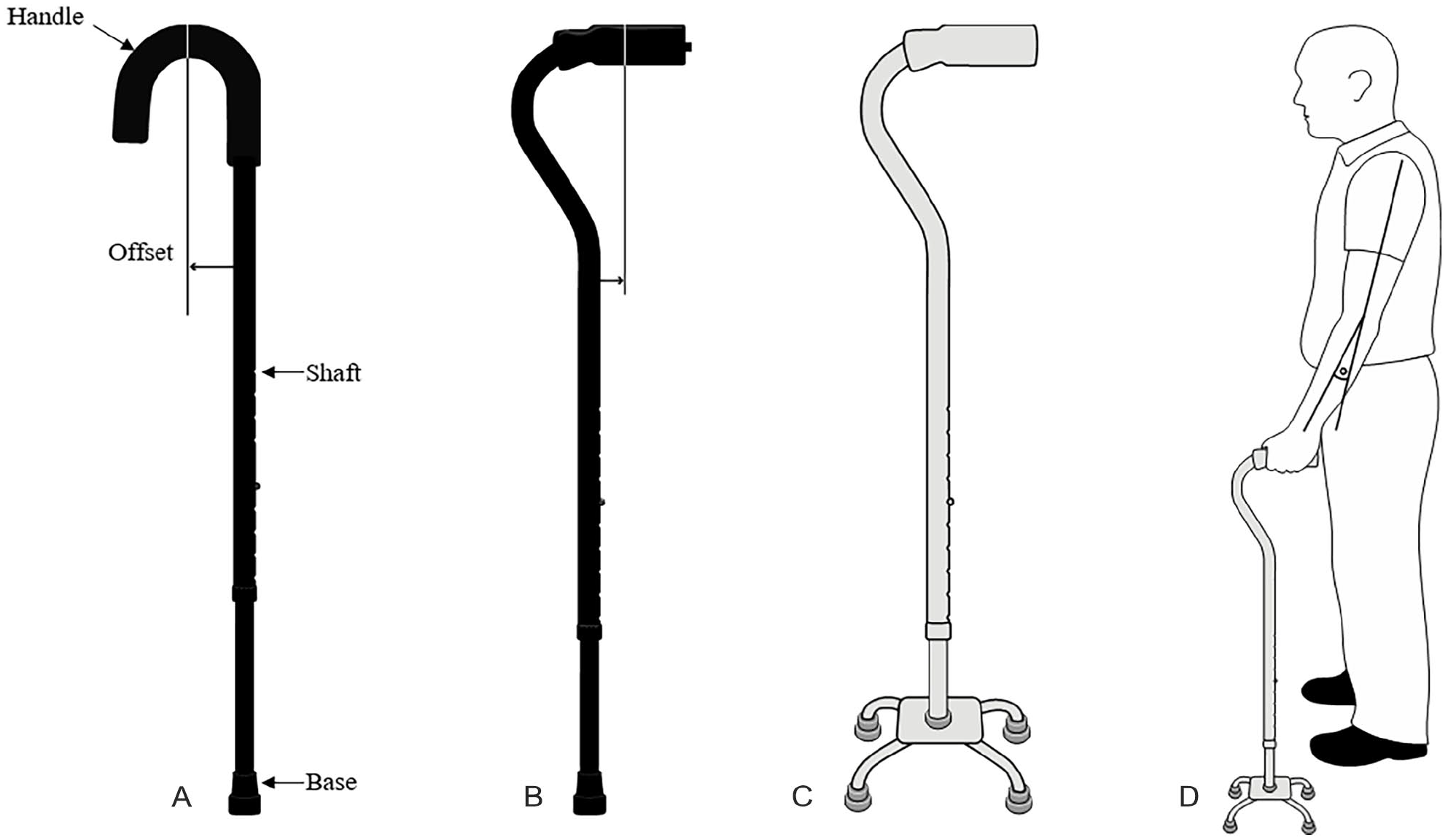
Different cane designs. (A) A simple C-shaped handle design with labeled cane components. Note the increased offset of the handle compared. (B). A T-shaped handle with a bend in the shaft near the handle to decrease offset and better align the patient’s weight down the axis of the shaft. (C) T-shaped handle with a 4-point base that increases the stability for the user and allows the cane to remain upright when left unattended. (D) Appropriate placement of the cane with 15 to 30 degrees of elbow flexion.
Indications for cane use are broad, and they may be used to treat both musculoskeletal and neurogenic gait abnormalities, with a maximum reduction of weightbearing of 50%. 24 If single-point canes are used, they are indicated to reduce 25% of the weightbearing load. 56 Contraindications for use include ipsilateral upper extremity injury. An advantage of the cane is its versatility for both permanent long-term and temporary short-term use. Individuals with musculoskeletal disease place more weightbearing load through the cane compared to those with neurologic disease. 2 Proper fitting and use is paramount for efficient utilization and reduction of metabolic demands. The most important factor is setting the appropriate height. 8 The height of the cane at the handle should measure to the patient’s wrist crease or greater trochanter when the cane is perpendicular to the floor. This will place the elbow between 15 and 30 degrees of flexion. 26 The cane should be placed in the opposite hand of the injured extremity to properly offload the affected extremity and maintain a 2- or 3-point gait pattern.
Improper fitting can lead to falls and altered biomechanics, which may increase metabolic expenditure and abandonment of use. It is reported that between 30% and 50% of geriatric patients will discontinue use soon after receiving a device because of difficulty of use. 47 Other reported complications include upper extremity pain, especially in those individuals who have or develop upper extremity tendonitis, osteoarthritis, and carpal tunnel syndrome. 2
Crutches
Crutches are commonly used in the orthopaedic setting. In general, they are utilized in a younger and healthier population when compared to the cane, owing to increased metabolic costs. They are used when increased weightbearing reduction is needed compared to the cane. There are 3 types of crutch design: axillary, forearm (Canadian, Lofstrand), and platform. 48 Figure 2 demonstrates the different types of crutch design. A single axillary crutch (SAC) may permit 80% load sharing of full weightbearing, while 2 crutches allow full reduction of weightbearing. 19

Various crutch designs. (A) Standard axillary crutches; newer models may have spring-assisted axillary pads and larger bases for ease of use. (B) Forearm crutches that are more commonly used in Canada and Europe. (C) Platform crutches used for patients with additional forearm, wrist, or hand injuries. It allows weight to be placed through the elbow to maintain balance and forward gait.
Because crutches can be used to treat both musculoskeletal and neurogenic sources of gait abnormalities, choosing the proper type depends on the expected time of use and upper extremity strength of the user. Axillary crutches require the most upper body strength compared with other crutch designs. They are more commonly used in healthy postoperative patients and are the most commonly prescribed crutch in the United States. 51 The forearm crutch is indicated for patients who have upper extremity weakness and are most commonly used in pediatric and older patients with neurogenic causes of gait abnormalities. It is also more commonly preferred in Canada and Europe in place of the axillary crutch for postoperative mobilization. Platform crutches act in a similar way to forearm crutches; however, they allow isolated weightbearing through the forearm. This is advantageous in patients with elbow contractures and in patients with weak or painful hands or wrists, including polytrauma patients with upper and lower extremity injuries. 44 In general, axillary crutches are indicated for temporary short-term use whereas the forearm and platform crutches are used for both permanent long-term and temporary short-term use depending on the patient’s needs.
Proper fitting of crutches is paramount for complication prevention and ease of use. Numerous studies have reported on the proper fitting of axillary crutches. Fitting should ideally place the elbow at 30 degrees of flexion, which corresponds to the point of the crutch being approximately 5 cm lateral and 15 cm anterior to the foot. 3 It is important that the padding of the crutch rest 4-5 cm from the axilla. Other methods include subtracting 40 cm from the patient’s height or selecting a crutch that is 77% of the patient’s height. 34 Axillary crutches that are too long risk compression injuries, with reports including the suprascapular nerve, axillary artery, radial nerve, ulnar nerve, long thoracic nerve, and the brachial plexus. 12 Crutches that are too short cause the patient to lean forward, increasing pressure on the shoulders, elbow, hand, and wrist. No differences in metabolic expenditure or perceived exertion have been identified with crutch length within 2.5 cm of the standard 5 cm from the axilla. 45
Axillary crutches have the highest energy consumption compared to Lofstrand and platform crutches when 2-pt, 3-pt, or nonweightbearing gait is utilized. 33 This equates to crutch-assisted gait being 50% less efficient than normal gait, with energy consumption becoming more equivalent to faster walking speeds. 50
Fitting for forearm and platform crutches is similar in that the crutch point should be lateral and anterior to the foot with the elbow flexed to 15 to 30 degrees. Forearm crutches utilize a cuff that should be positioned on the proximal third of the forearm approximately 2.5 to 4 cm distal to the olecranon process. 16 Platform crutches utilize a platform piece that is measured by flexing the elbow to 90 degrees and measuring the length from the forearm to the ground. 16
Walkers
It is estimated that 2 million Americans use a walker for gait assistance and stabilization, of whom more than 75% are of advanced age. 18 There are 3 commonly encountered walkers, which include the 4-wheeled (4W) walker, 2-wheeled (2W) walker, and 4-footed (4F) walker. All have options for folding and bench support. Walkers provide increased stability at the cost of metabolic expenditure and maneuverability. They are primarily indicated in patients of advanced age with neurogenic causes of gait instability; however, appropriately selected walkers, especially the 4W walker, may benefit younger, healthier patients.
Walkers are indicated for both permanent long-term and temporary short-term use. They may benefit those who are full weightbearing and nonweightbearing. It is important to note that those patients made nonweightbearing should be prescribed the 4F or 2W walker as these have more stability to support the patient’s full weight. Figure 3 shows the different walker types available for use.

Various walker designs. (A) A standard 4-footed (4F) walker. (B) A 2-wheeled (2W) walker. (C) A 4-wheeled (4W) walker with brake attachments and bench. This offers the greatest mobility with least metabolic demand, albeit least stability.
Hall et al 18 suggested guidelines for proper fitting regardless of walker type. These authors propose that the height should be adjusted so that the handle is at the level of the ulnar styloid when the user stands upright with the elbows flexed at 15 degrees. 18 Biomechanically, the 4F walker is the most stable walker; however, it requires the greatest energy demand. Studies cite an increase in the oxygen exchange rate (a surrogate for metabolic demand) by 200%.14,20 This is due to upper extremity metabolic demands to lift the walker and utilization of a 3-point step-to-gait pattern. 40 The utilization of 2W and 4W devices are much less metabolically expensive, this is due to decreased activation of the upper extremity and ability to perform a 2-point bipedal gait. 40 Overall, the metabolic demands of 4W and 2W walkers are only slightly greater than normal bipedal gait at the same speed. 40 These walkers are best suited for patients with gait patterns that are too fast for a 4F walker or those patients who are too frail to lift a standard 4F walker. 46 Additionally, wheeled walkers provide a large base for balance in those that can tolerate ambulation of substantial distances who do not require substantial weightbearing support. 31
The incidence of falls associated with walker use is not well defined with high-quality evidence. van Riel et al 52 performed an epidemiologic database study on the complication rates of 4W walkers and found that the overall injury risk was 3.1 per 100 users. Injury risk was the highest in women aged 85 years and older. The majority of injuries were fractures (60%), with hip fractures (25%) being the most common. In another study of emergency department admissions for unintentional falls, Stevens et al reported similar findings. They found that in a national safety database there were 47,312 fall injuries that were associated with walking aids, and that 87% of cases were specifically associated with walker use. 49 Approximately one-third of subjects in this study were hospitalized for their injuries. 49
The sequela of falls is well understood and include increased rates of fractures, head trauma, and hospital admission. 46 The greatest predictor of falls while using walkers is reported to be the lateral spontaneous sway amplitude of the user. 31 Greater attention and concentration is required for walker ambulation compared to cane use, which may increase risk for falls. 54
Novel LEADs
Hands-Free Single Crutch (HFSC)
The HFSC is a newer device that provides the support and benefits of crutches without reliance on the upper extremity. The device is composed of a platform, on which the injured extremity rests and is secured, and a crutch, which interfaces with the ground. Figure 4B demonstrates a modern HFSC. Advantages cited include maintaining a 2-point alternating gait, which is more energy efficient, and the ability to maintain gait without upper extremity assistance.
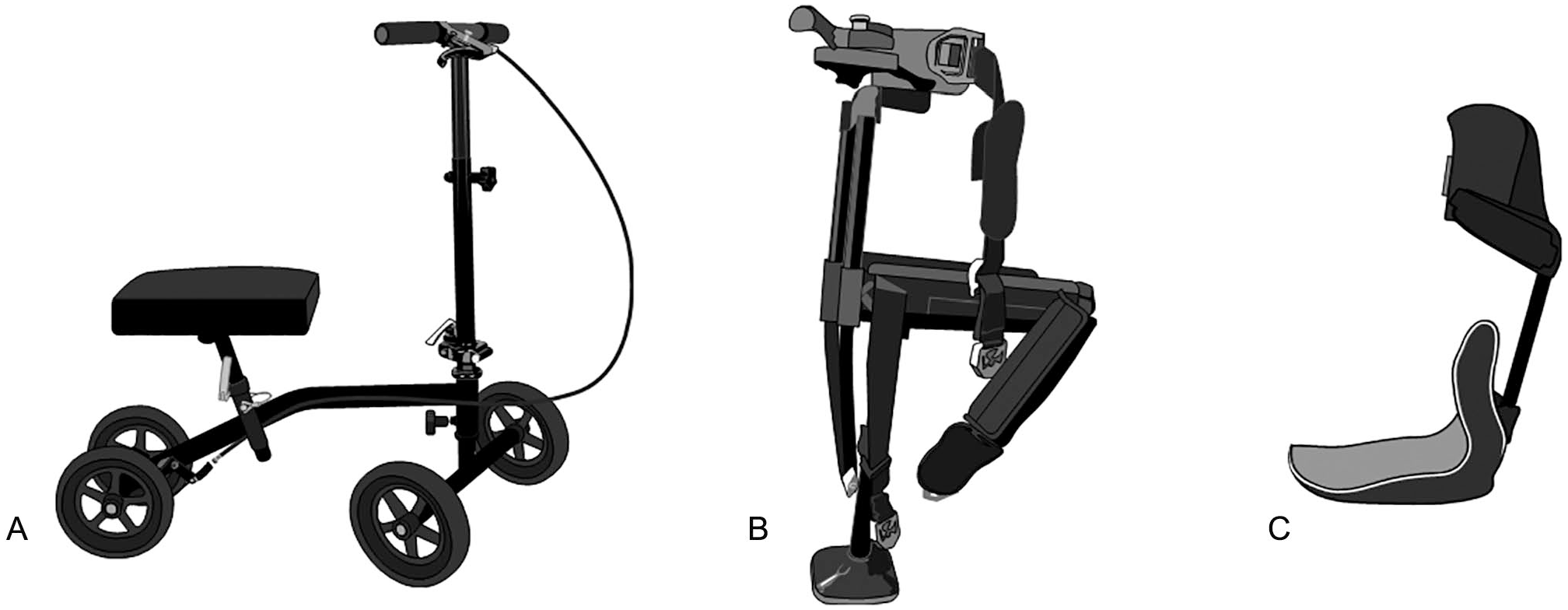
Novel devices. (A) An example of a rolling knee scooter with brake attachment. (B) A hands-free single crutch. (C) An example of a dynamic ankle foot orthosis (IDEO brace).
Compared to the traditional LEADs, there is a lack of published data supporting the use, indications, and complications of the HFSC. The one study that evaluated for potential complications was in healthy adult patients with an average age of 32 years. No falls were reported, although there was 7% rate of proximal leg strap irritation in the HFSC group. 32 This rate was much lower than the 86% of SAC users who reported axillary or hand pain after crutch use in this series. 32 This lends early support to the use of the HFSC as a potential alternative to traditional LEADs in appropriately selected patients. 36 Sizing, restrictions, and pricing vary based on manufacture.
Martin et al 32 performed a randomized prospective comparative study and found that healthy patients with foot and ankle disorders preferred the HFSC over the SAC. They demonstrated that overall, the HFSC had lower metabolic demands as determined by lower dyspnea scores as well as pre- and postactivity heart rate elevations. Upper extremity pain was also lower compared to the SAC. The authors concluded that in patients with foot and ankle disorders, the HFSC may be a viable option for mobilizing patients and protecting against ipsilateral muscular atrophy and disuse osteopenia from stress shielding.
Electromyographic testing has demonstrated increased lower extremity muscular recruitment in HFSC compared to the SAC and rolling knee scooter. 9 Those patients with vestibular or neuropathic conditions likely would not be suitable candidates for HFSC use. Utilizing a 2-point alternating gait pattern requires better balance as the patient must coordinate lower extremity proprioception through an end bearing device and moving an ambulatory assistive device with the contralateral lower extremity. 35
Orishimo et al 36 performed 3D motion analysis and compared hip and lumbar spine biomechanics between the HFSC, SAC, and normal gait. They found no difference in hip reactive forces between HFSC or SAC compared to normal gait. However, HFSC had lower hip range of motion compared to SAC with slightly increased lumbar spine motion to compensate. 36 They suggest that HFSC, when indicated properly, may be a viable alternative to SAC; however, in patients with underlying lumbar spine disease, this may lead to increased pain or discomfort.
Rambani et al 42 attempted to quantify the HFSC advantage over the SAC in patients with foot and ankle trauma with ipsilateral upper extremity injuries through randomization of HFSC or SAC. They found that the HFSC group displayed a shorter hospitalization (2.3 vs 6.7 days) compared to the SAC, with increased function and 36-Item Short Form Health Survey scores. 42 The authors concluded that the HFSC is likely a useful adjunct for mobilization in a polytrauma patient. Their results, although promising, have not been duplicated in other studies. There also exists a possible selection bias as the study groups are not well defined. Further studies are needed to confirm these results and HFSC usefulness for mobilization in polytrauma patients.
Given the available literature, the HFSC is likely best indicated for younger patients without a history of chronic low back pain or cognitive/balance disorders who want to mobilize efficiently in a variety of terrain settings.
Rolling Knee Scooter
The RKS (Figure 4A) has many names such as the “orthopaedic scooter,” “knee scooter,” and “wheeled knee walker.” The use of the RKS in foot and ankle surgery is likely increasing; however, the exact rate is currently not defined. The RKS provides a method for mobilization that requires less metabolic exertion to maintain faster gait speeds, less muscular recruitment, and higher patient satisfaction scores compared to traditional LEADs. 25 Similar to the HFSC, there is a paucity of literature supporting its exact indications, clinical outcomes, and complications.
Rahman et al performed a survey study querying 333 foot and ankle surgeons about complications and indications for RKS use. They found that the majority of foot and ankle surgeons were using the RKS for patients who were made nonweightbearing after arthrodesis and fracture fixation. 41 Roughly 50% of the surgeons had prescribed an RKS with a mean reported complication rate of 2.5%. 41 This is substantially lower than the 43% fall rate cited by Yeoh et al. 55 The high complication rate of 43% in the series by Yeoh et al may be attributable to 67% of their patients not receiving training or education on the RKS prior to use and the inherent reporting bias of survey studies. 55 Risk factors identified by Rahman et al 41 were female gender, age >44 years, obesity, and sedentary lifestyle.
In another survey to assess patient complications with the RKS, Workman et al 53 found that 25 of 101 patients (24.7%) experienced some form of a fall, with 5 patients seeking medical attention due to injury (4.9%). The study cohort had an average age of 54 years, with an average body mass index of 28.5. Interestingly, 96% of this population preferred the RKS over the SAC. Identified factors that contributed to falling included hitting an obstacle, making a sharp turn, moving too fast, and moving downhill. There was no correlation between falls and patient comorbidities. 53
In addition to falls, another major complication cited is the development of deep vein thrombosis (DVT) due to prolonged knee flexion. This is a concern among those providers who prescribe the RKS as there are no formal studies that quantify the DVT rates in this population. Duplex blood flow studies have demonstrated decreased volumetric flow rate through the popliteal vein with the knee flexed on a RKS. 7 However, recent data suggest that this decreased flow can be mitigated through the activation of the musculovenous pump through toe flexion and extension in healthy patients. 43 Further prospective trials are needed to elicit any difference in the rates of DVT in healthy and vascular-deficient patients with use of an RKS.
Given the available literature, the RKS is best indicated in younger patients without cognitive/balance disorders or history of provoked VTE who wish to mobilize over relatively flat and even terrain. In contrast to the HFSC, the RKS is not indicated in patients with upper extremity injuries or weakness as it requires both upper extremities to steer.
Ankle Foot Orthosis
Traditional AFOs are static devices used to restrict ankle plantarflexion and keep the talocrual joint in a neutral position. This facilitates gait swing and prevents equinus contractures in patients with foot drop. 6 The most common indication for an AFO is neuromuscular in etiology following a cerebrovascular accident or stroke. 13
Dynamic (energy storing) AFOs, often constructed of carbon fiber, are similar to traditional AFOs. However, they are also able to store potential energy from heel strike to midstance and return this as kinetic energy at the push-off phase of gait, helping to facilitate forward progression. 17 The delivery of kinetic energy in areas of deficiency in the gait cycle has expanded the indications for AFOs beyond that of foot drop. These now include any foot and ankle condition in which pain or weakness associated with plantarflexion or joint instability are present. 37 This is commonly seen in foot and ankle arthrodesis, arthritis, limb salvage, and partial foot amputations. 37 It is important to note that there are a wide range of available AFOs, ranging from off-the-shelf varieties to custom fabricated devices that require referral to an experienced orthotist.
One relatively new AFO with promising clinical outcomes is the Intrepid Dynamic Exoskeletal Orthosis (IDEO). This device (Figure 4C) incorporates 2 posteriorly mounted carbon fiber struts that extend from a proximal ground reaction leg cuff to a plantar-flexed supramalleolar solid ankle AFO and footplate. 39 Clinical outcomes are favorable in the reported literature, with improved functional scores in all parameters compared to other brace types. 38 Clinical results of its use and a return to run program have demonstrated promising results in military populations with a 4-fold likelihood to return to duty and decrease desire for delayed amputations in limb salvage cases.4,5
In a recent retrospective review of outcomes, Hoyt et al 21 evaluated 185 individuals who reported IDEO use. Interestingly, those patients diagnosed with footdrop or ankle weakness were more likely to continue use (odds ratio 2.33, P = .04), compared to patients with a previous fusion (odds ratio 0.45, P = .049). 21 Overall, 16 patients (7.5%) underwent delayed lower extremity amputations following IDEO treatment, whereas only 27.2% of patients who initially desired amputation eventually underwent the procedure. 21 These findings are supported by the work of Ikeda et al, 23 who reported that IDEO use resulted in improved visual analog scale (VAS) scores (5.2 ± 2.9 to 1.7 ± 1.6 points). Additionally, Lower Extremity Functional Scale scores increased from 29.7 ± 16.6 to 59.5 ± 13.6 after brace initiation. 23 It seems most important that the brace be used in conjunction with individualized physical therapy to maximize patient-reported outcome measures.
Conclusion
Lower extremity ambulatory assistive devices are important augments that provide patients mobility in various settings. There are numerous devices on the market and in development, all of which have different designs, indications, complication profiles, and limitations. It is important that providers who prescribe these devices are aware of these factors and incorporate specific patient factors into determining the appropriate device for their patient. This will ultimately improve patient mobility and satisfaction while maximizing safety.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007231207637 – Supplemental material for Lower Extremity Assistive Devices (LEADs): A Contemporary Literature Review
Supplemental material, sj-pdf-1-fai-10.1177_10711007231207637 for Lower Extremity Assistive Devices (LEADs): A Contemporary Literature Review by Erik M. Hegeman and Jeannie Huh in Foot & Ankle International
Footnotes
Disclaimer
The views expressed in this article are those of the authors and do not reflect the official policy of the Department of Army, Defense Health Agency, Department of Defense, or US Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.