
Abstract
Background:
This study sought to establish normative values for baseline physical and mental health by foot and ankle diagnosis using validated PROMIS scores and to compare the correlation between these 2 outcomes across common diagnoses. Additionally, it investigated the effects associated with chronic vs acute conditions and specific diagnoses on mental health.
Methods:
We reviewed baseline PROMIS Physical Function 10a (PF10a) and PROMIS Global-Mental (PGM) scores of 14,245 patients with one of the 10 most common foot and ankle diagnoses seen at our institution between 2016 and 2021. Pearson correlation coefficients were calculated to assess the relationship between PF10a and PGM by diagnosis. A multivariable regression model including age, sex, language, race, ethnicity, education level, income, and Charlson Comorbidity Index was used to determine the associated effect of diagnosis on PGM score.
Results:
On unadjusted analysis, patients diagnosed with an ankle fracture had the lowest mean physical function, whereas patients with hallux valgus had the highest (PF10a = 33.9 vs 46.7, P < .001). Patients with foot/ankle osteoarthritis had the lowest mean self-reported mental health, whereas patients with hallux rigidus had the highest (PGM = 49.9 vs 53.4, P < .001). PF10a and PGM scores were significantly positively correlated for all diagnoses; the correlation was strongest in patients diagnosed with foot/ankle osteoarthritis or hammertoes (r = 0.511) and weakest in patients with ankle fractures (r = 0.232) or sprains (r = 0.280). Chronic conditions, including hammertoes (β = −5.1, 95% CI [−5.8, −4.3], P < .001), foot/ankle osteoarthritis (β = −5.0, 95% CI [−5.7, −4.3], P < .001), and hallux valgus (β = −4.8, 95% CI [−5.5, −4.1], P < .001) were associated with the largest negative effects on patients’ mental health.
Conclusion:
Self-reported physical function and mental health varied across common foot and ankle diagnoses and were more tightly correlated in chronic conditions. The associations between diagnosis and mental health scores appear larger for more chronic diagnoses, including those that are generally associated with relatively unimpaired physical function.
Introduction
Patient-reported outcome measures (PROMs) are an important component of patient-centered and evidence-based treatments for foot and ankle conditions. 28 With research and health policy placing increasing value on the patient experience, there is a push toward integrating PROMs into routine clinical care. 30 Doing so, however, requires that physicians have a comprehensive understanding of normative values, reference ranges, and predictive thresholds.
Patient-Reported Outcomes Measurement Information System (PROMIS) measures have been forwarded as the choice PROMs for orthopaedic care, in large part because of their straightforward and uniform interpretation.12,17,27 Although legacy foot and ankle measures such as the American Orthopaedic Foot & Ankle Society (AOFAS) scales, Foot and Ankle Ability Measure (FAAM), or Foot Function Index (FFI) remain among the most commonly used in the foot and ankle literature,37,42 research has shown PROMIS measures to be comparable or even superior in terms of validity, reliability, and responsiveness, with the advantage of a reduced questionnaire burden.1,6,24 Accordingly, PROMIS scores are increasingly used in the foot and ankle literature.
There are no published reports comprehensively summarizing the baseline PROM scores of a large patient cohort using a single valid metric for common foot and ankle diagnoses. Although prior studies have used PROMIS to assess outcomes of foot and ankle surgery generally,2,20 by anatomic region, 22 and for specific interventions,5,13,14,18 many of these reports do not offer insight into, or facilitate interpretation of, patient-reported conditions at initial presentation. Furthermore, prior literature suggests there is a bidirectional relationship between mental health and physical function3,4,10,15,20,32,33,38; however, the extent of that relationship and how it varies between specific foot and ankle diagnoses remains unknown. With the prevalence of mental health disorders reported to be approximately 30% among foot and ankle patients,32,33 we sought to gain a deeper understanding of which patients, on the basis of diagnosis, may benefit from additional mental health screening or support during their orthopaedic treatment in order to optimize their recovery process and overall treatment outcomes.
The goal of this investigation was to (1) establish normative values for baseline physical and mental health by foot and ankle diagnosis using validated PROMIS scores, (2) describe and compare the correlation between self-reported physical function and mental health across common foot and ankle diagnoses, and (3) determine the associated effects of acute vs chronic and specific foot and ankle diagnoses on self-reported mental health to identify diagnoses for which mental health might be a particularly important consideration.
Methods
Institutional review board approval was obtained for this retrospective, cross-sectional study.
Study Cohort
Our institutional PROM database was queried for patients ≥18 years old who completed the PROMIS Physical Function Short Form 10a (PF10a) and PROMIS Global-Mental (PGM) instruments at a foot and ankle clinic visit between June 2016 and November 2021. Sites included 1 large urban academic center, 1 associated community hospital, and several surrounding suburban outpatient clinics. The initial query identified 44,564 encounters at which the PF10a and PGM had been completed. Data were processed to include only the first case of those with duplicate MRN and primary diagnosis. Cases with missing zip code or census income data were excluded. The remaining 36,527 cases were then grouped by diagnosis, and only cases associated with one of the top 10 most common diagnoses in the data set were included in final analyses (N = 14,245) (Figure 1). The included International Classification of Diseases, Tenth Revision (ICD-10), codes are listed in Supplemental Table 1.
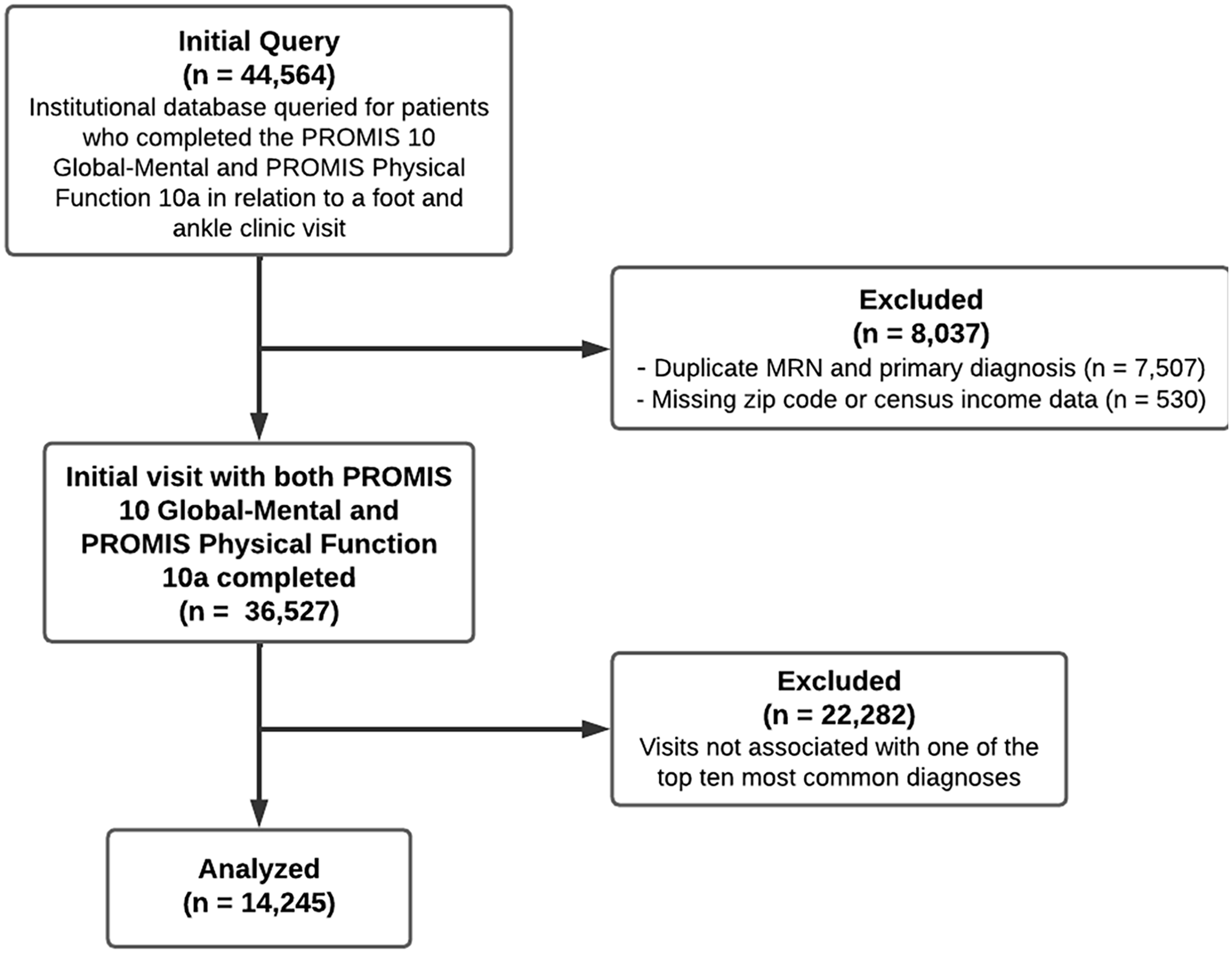
Data processing and exclusion to yield final study cohort.
Data Collection
Patients completed PROM questionnaires prior to clinic visits through an online portal or during clinic check-in. Surveys were administered in English only, and an interpreter may or may not have assisted patients with completion.
The PF10a contains 10 questions to assess overall self-reported physical function. The PGM is a subscore of the PROMIS Global-10 measure and is composed of items on quality of life, mental health, social satisfaction, and emotional problems. The raw scores on PROMIS questionnaires are converted to T scores normalized for the general US population with a mean and SD of 50 ± 10 using tables provided by PROMIS on healthmeasures.net. 34 A higher T score represents better function or mental health.
Age, sex, zip code, self-reported race and ethnicity, primary language spoken, education level, and Charlson Comorbidity Index (CCI) were abstracted from our institutional database. US Census Bureau American Community Survey data (5-year estimates in 2019 inflation-adjusted dollars) were queried to estimate a median household income (MHI) for each patient using their zip code. 39
Statistical Analysis
Data were aggregated using SPSS (version 27; IBM). Continuous predictor variables were transformed into categorical variables for analysis. Patients were categorized into 3 groups based on their CCI: no comorbidities, mild to moderate CCI (1-4), and severe CCI (≥5). 23 We computed quartiles for MHI to create the following categories: ≤$87985 = lowest quartile, $87986-$108046 = second quartile, $108047-$128824 = third quartile, and ≥$128825 = highest quartile. The chronicity of the diagnoses was defined as acute (traumatic injuries for which patients tend to present with less than 6 weeks of symptoms), chronic (conditions for which patients tend to present with greater than 6 weeks of symptoms), or indeterminate (all other included diagnoses for which patients tend to present with variable symptom duration).
To establish normative physical and mental health PROMIS scores at baseline, descriptive analyses were conducted for PROM scores by diagnosis, with further stratification by sex and age group. Sex was binary and age was categorized into 3 groups—<40 years old, 40-64.9 years old, and >65 years old—per prior literature and to facilitate point of care interpretations.19,26,41 To assess for differences in PROM scores by sex and age, respectively, within diagnoses, t tests and ANOVA were utilized. Pearson correlation coefficients (r’s) were calculated to assess the relationship between PF10a and PGM by diagnosis and interpreted as follows: 0.00-0.29, no correlation; 0.30-0.49, weak correlation; 0.50-0.69, moderate correlation; 0.70-0.89, strong correlation; and 0.90-1.00, very strong correlation.
PROM scores were interpreted using MCIDs calculated for each diagnosis using the one-half-SD method and score ranges provided by our institution. Other approaches for determining MCIDs have been described in the foot and ankle literature,2,17,25 with results for PROMIS measures varying widely depending on calculation method, diagnosis, and timing of data collection. Previously reported MCID values in the foot and ankle literature range from about 3 to 4.5 for PF10a17,25 and 4.2 to 4.7 for PGM,11,29 respectively. The PF10a score range descriptions provided by our institution are as follows: 14-30 = severe, 30-40 = moderate, 40-45 = mild, 45-62 = within normal limits, and PGM score range descriptions include 21-29 = poor, 29-40 = fair, 40-48 = good, 48-56 = very good, and 56-68 = excellent.
A multivariable regression model was used to determine the effects associated with diagnosis on self-reported mental health when accounting for variation in physical function as well as demographic factors and comorbidity burden, which have been previously shown to impact PROM scores. 11 Predictors included MHI, education level, primary language spoken, CCI, sex, age, and PF10a score. The same multivariable model was run to determine the association between chronic vs acute conditions and PGM scores.
Results
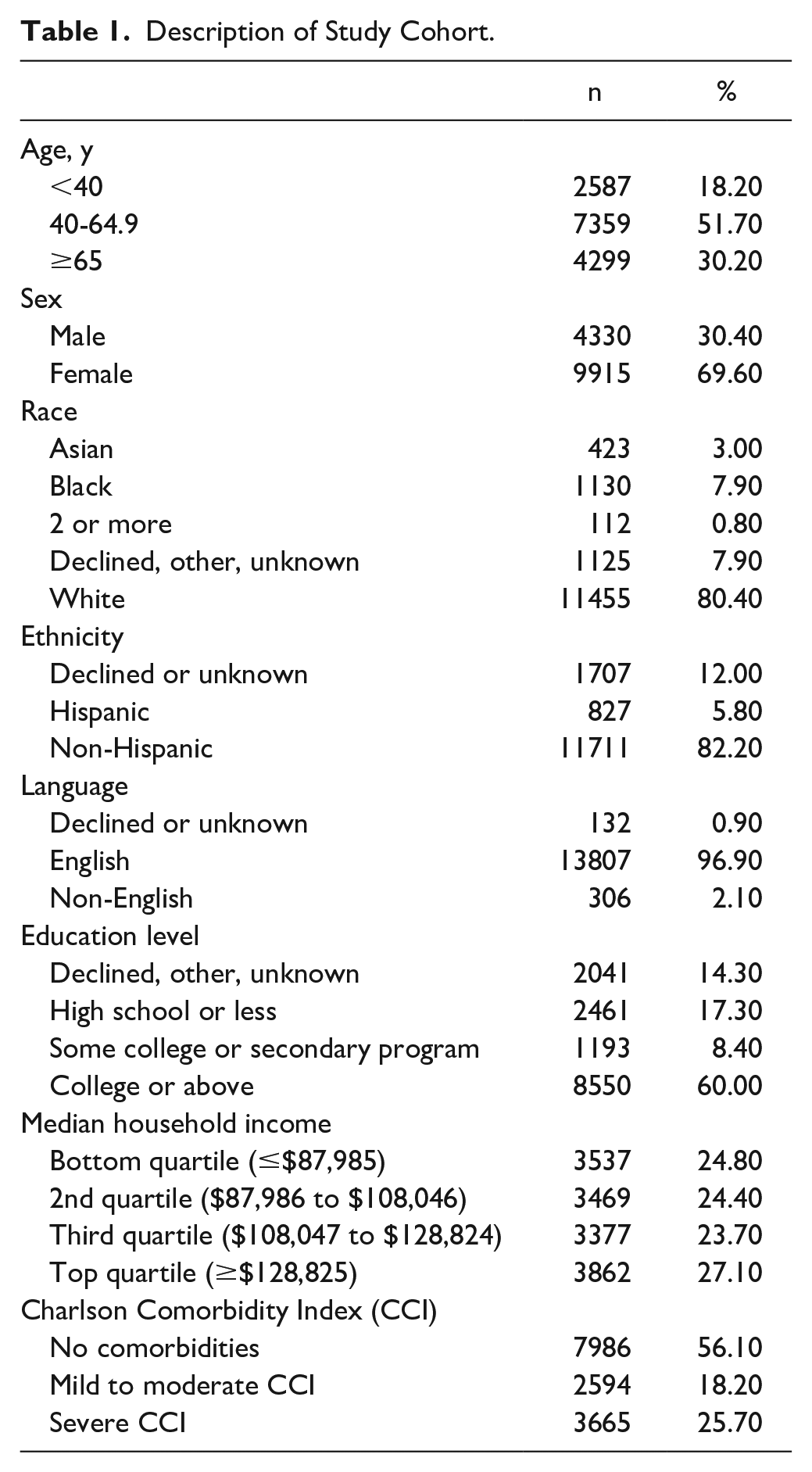
There were 14,245 patients included in the final analyses (Figure 1, Table 1). The top 10 most common diagnoses presenting to our clinic were plantar fasciitis (n = 2,345), hallux valgus (n = 2007), foot or ankle osteoarthritis (OA) (n = 1915), hammertoes (n = 1597), Achilles tendinopathy (n = 1237), ankle sprain (n = 1140), posterior tibial tendinitis (n = 1203), hallux rigidus (n = 1075), peroneal tendinopathy (n = 948), and ankle fracture (n = 778). Compared with the overall US population, 40 our cohort was older, included more female patients, was more educated and wealthier, and had fewer Black, Hispanic, Asian, and non-English-speaking patients (Supplemental Table 2).
Description of Study Cohort.
On unadjusted analysis, patients diagnosed with an ankle fracture had the lowest mean physical function, whereas patients with hallux valgus had the highest mean physical function (PF10a = 33.9 vs 46.7, P < .001). Patients diagnosed with foot/ankle OA had the lowest mean self-reported mental health, whereas patients with hallux rigidus had the best mean mental health (PGM = 49.9 vs 53.4, P < .001) (Figure 2).
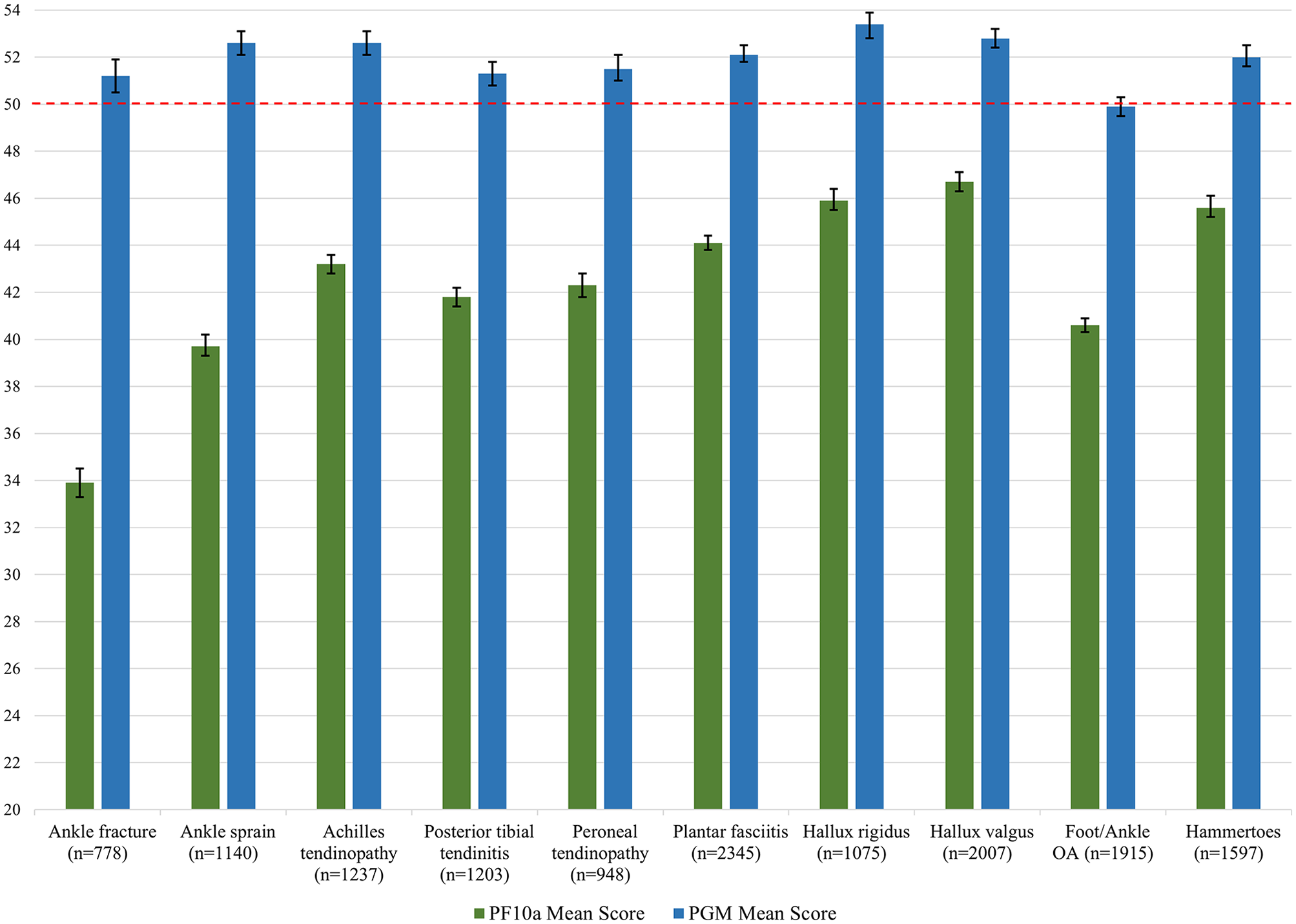
Comparison of mean unadjusted PROMIS Physical Function 10a and PROMIS Global-Mental scores by diagnosis. The mean and SD of the general (nonclinical) US population is 50 ± 10 and is indicated by the red dashed line. [See online article for color figure.]
PF10a and PGM scores were significantly positively correlated for all diagnoses (Table 2). Self-reported physical function and mental health had the strongest correlation in patients diagnosed with foot/ankle OA or hammertoes (r = 0.511, moderate correlation) and the weakest correlation in patients with ankle fractures (r = 0.232, no correlation) or ankle sprains (r = 0.287, no correlation) (Table 2).
Unadjusted PROM Scores and Correlation Coefficients by Diagnosis. a
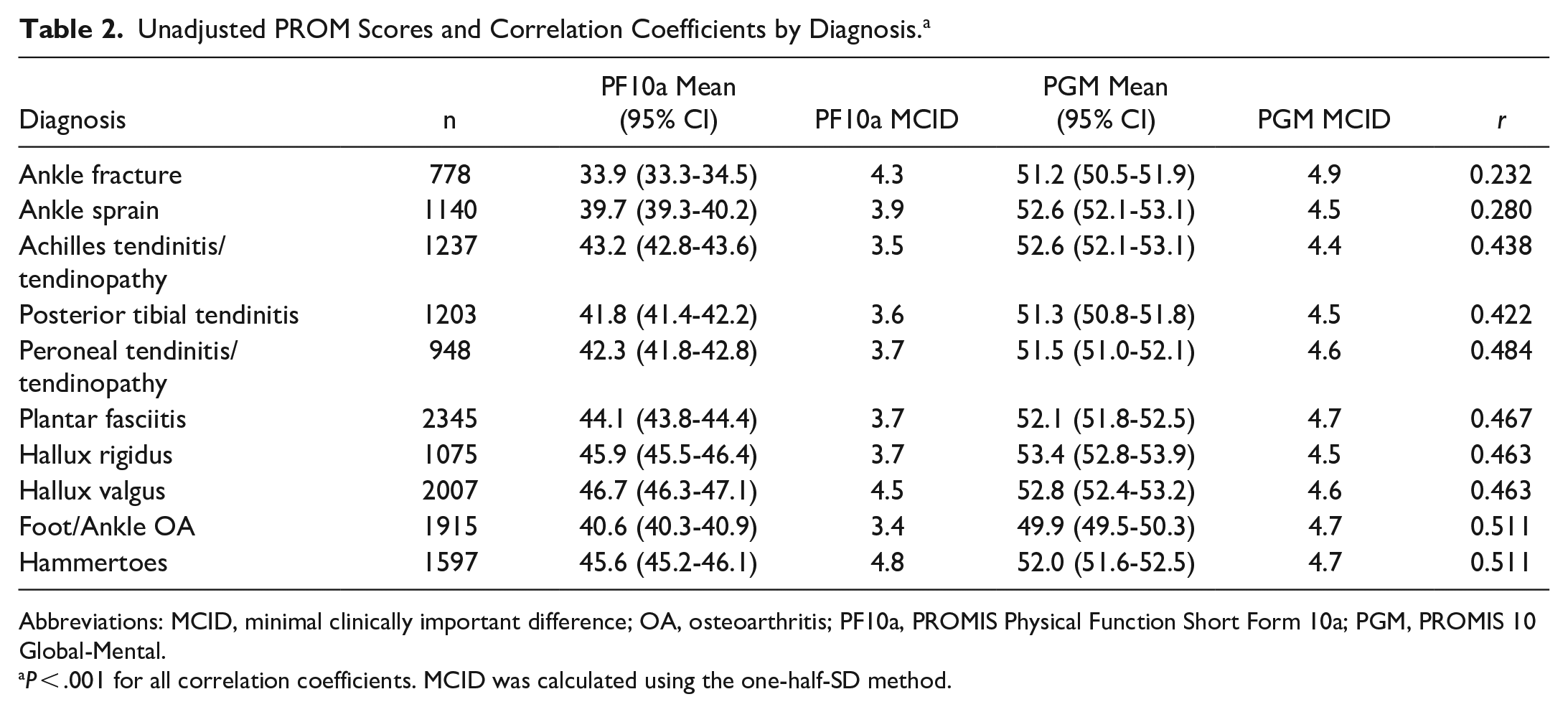
Abbreviations: MCID, minimal clinically important difference; OA, osteoarthritis; PF10a, PROMIS Physical Function Short Form 10a; PGM, PROMIS 10 Global-Mental.
P < .001 for all correlation coefficients. MCID was calculated using the one-half-SD method.
Baseline PF10a and PGM scores varied by sex and age group for some, but not all diagnoses (Table 3). For diagnoses with significant score variation by sex (plantar fasciitis, posterior tibial tendinitis, Achilles tendinopathy, hallux rigidus, peroneal tendinopathy, and ankle sprain), males scored higher than females for both PF10a and PGM. For diagnoses with significant score variation by age group (foot/ankle OA, hallux valgus, hammertoes, posterior tibial tendinitis, Achilles tendinopathy, plantar fasciitis, and peroneal tendinopathy), PF10a scores generally declined with age whereas PGM scores improved with age.
Normative Baseline PROM Scores by Sex and Age for Common Foot and Ankle Diagnoses.
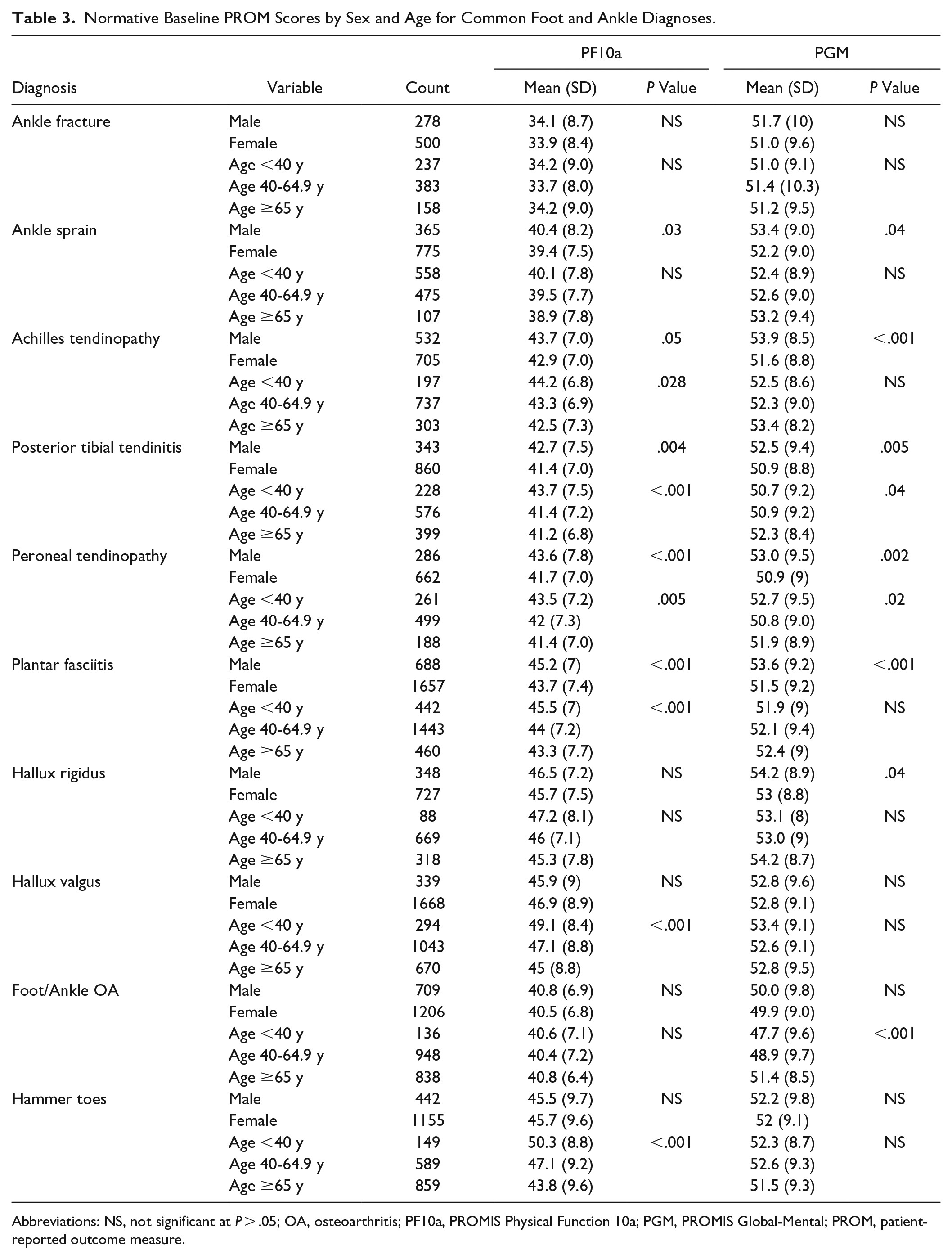
Abbreviations: NS, not significant at P > .05; OA, osteoarthritis; PF10a, PROMIS Physical Function 10a; PGM, PROMIS Global-Mental; PROM, patient-reported outcome measure.
When comparing patients with acute conditions (ankle sprains and ankle fractures) to those with chronic conditions (foot/ankle OA, hallux valgus, hallux rigidus, and hammertoes), we found that patients with acute conditions had significantly lower PF10a scores (mean difference = −7.1 points, P < .001) (Table 4). Patients whose condition was indeterminate also had lower mean PF10a scores than patients with chronic conditions (−1.4 points, P < .001). With regard to PGM, on unadjusted analysis, patients with chronic vs acute conditions did not differ. When accounting for differences in sociodemographic factors, comorbidity burden, and PF10a scores, patients with chronic conditions had significantly lower PGM scores compared to patients with acute conditions (mean difference = −4.1points, P < .001).
Comparison of Unadjusted PROM Scores by Chronicity.
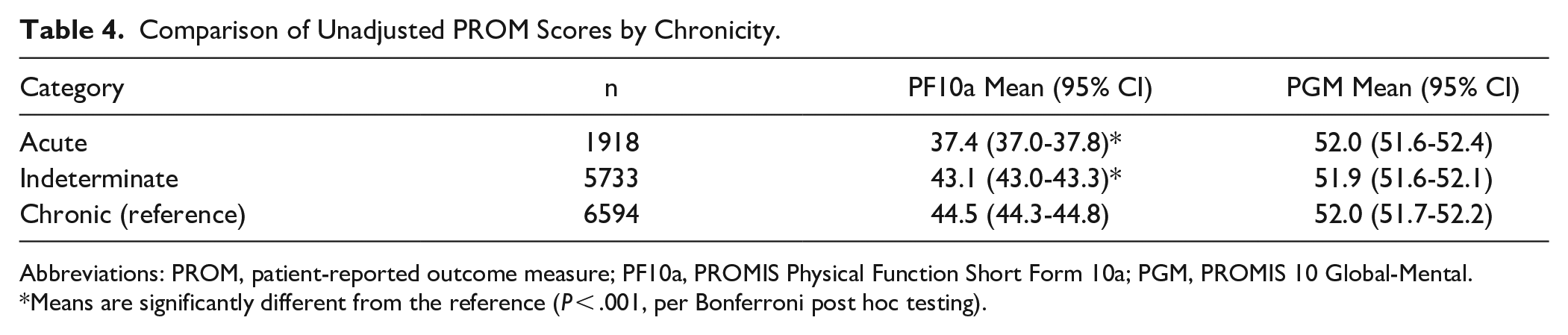
Abbreviations: PROM, patient-reported outcome measure; PF10a, PROMIS Physical Function Short Form 10a; PGM, PROMIS 10 Global-Mental.
Means are significantly different from the reference (P < .001, per Bonferroni post hoc testing).
In the multivariable regression model for PGM scores, diagnosis was the strongest predictor (Supplemental Table 3). A high-school-or-less education, Black race, and lowest quartile MHI were associated with the next largest negative effects on mental health. When examining the associations between diagnoses and PGM scores after controlling for differences in physical function, we found that the diagnoses of foot/ankle OA (β = −5.0, 95% CI −5.7, −4.3; P < .001), hammertoes (β = −5.1, 95% CI −5.8, −4.3; P < .001), and hallux valgus (β = −4.8, 95% CI −5.5, −4.1; P < .001), all chronic conditions, were associated with the largest negative effects on patients’ self-reported mental health (reference=ankle fracture) (Figure 3). In other words, in patients with equally limited physical function, those with hammertoes, foot/ankle OA, and bunions are expected to report the worst mental health.
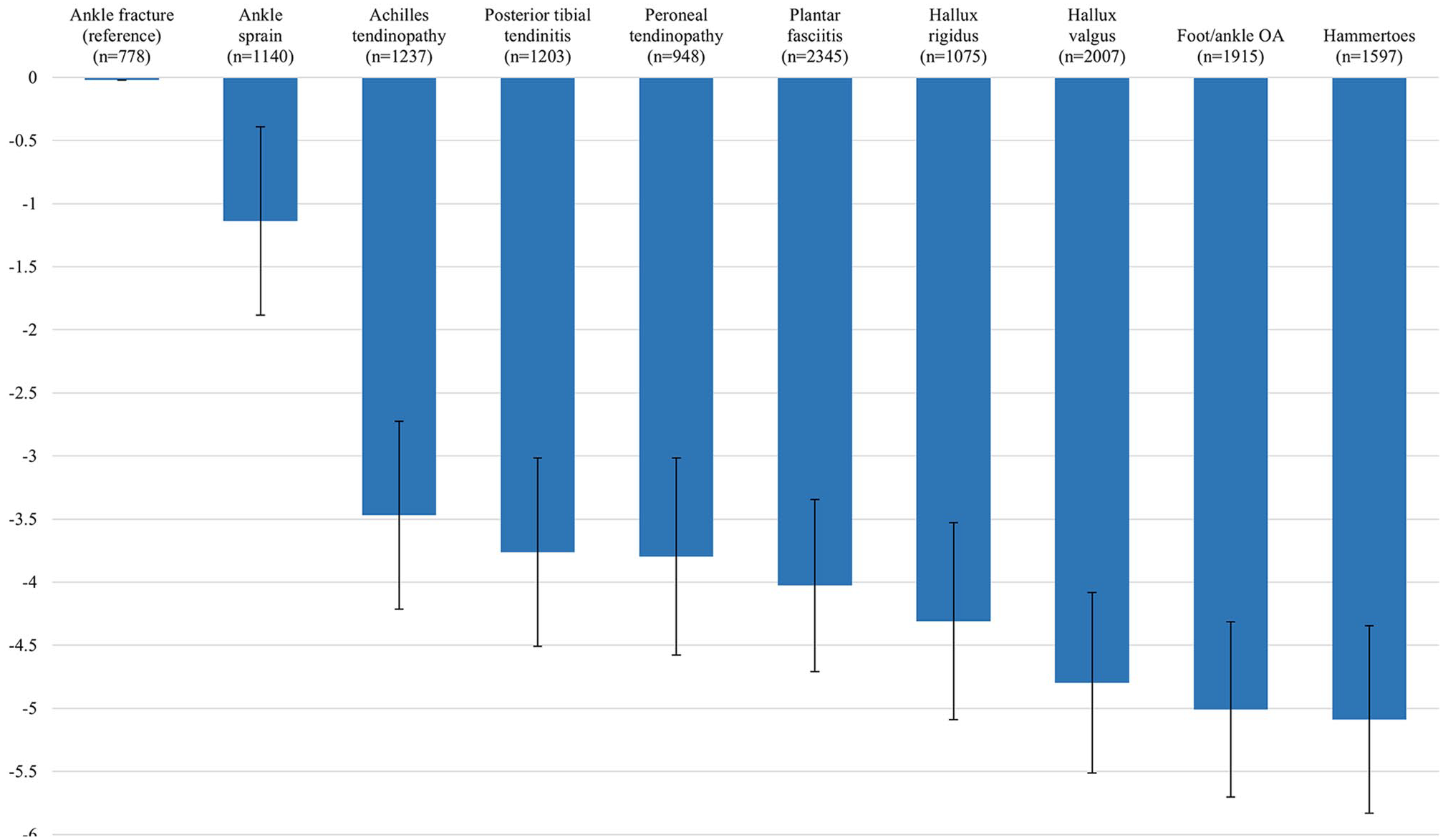
Effect of diagnosis on PROMIS Global-Mental scores after adjusting for differences in physical function and sociodemographic factors. This graph demonstrates the differences in mean mental health scores if you compare patients across diagnoses experiencing the same level of physical disability. For example, patients with osteoarthritis who are experiencing the same level of physical function as patients suffering from an ankle sprain will, on average, report mental health scores 3.9 points worse than the patients with ankle sprains. The β, 95% CIs, and P values for each diagnosis and all other predictors are reported in Supplemental Table 3.
Discussion
In this study, we establish normative self-reported physical and mental health benchmarks using validated PROMIS measures for common foot and ankle diagnoses. We found that there is considerable variation in self-reported physical function and mental health across common foot and ankle diagnoses; however, on unadjusted analysis, only PF10a scores differed more than the MCID. Additionally, we found that the correlation between mental health and physical function varies by diagnosis, with a stronger correlation in more chronic conditions. When stratifying PROM scores by sex and age within diagnoses, only a subset of diagnoses showed appreciable differences across categories. Finally, we identified that diagnoses of hammertoes, foot/ankle OA, and hallux valgus were associated with the largest negative effects on mental health—all exceeding the diagnosis-specific MCIDs—when controlling for physical function, comorbidity burden, and sociodemographic factors.
Establishing normative baseline patient-reported physical and mental health status for patients with specific foot and ankle diagnoses using a PROMIS measure has utility for improving patient care and advancing research efforts. The data we present can be helpful to physicians and patients alike by serving as a benchmark that aids in shared decision making, counseling, and formulating treatment plans. In particular, establishing baseline scores stratified by sex and age allows for more accurate point-of-care interpretation and a deeper understanding of the diagnoses for which sex and age may importantly influence outcomes. These data can also be of use to researchers by facilitating cross-study comparisons, the measurement of treatment effectiveness, and enabling future investigations within comparable patient cohorts.
Prior studies evaluating patient-reported outcomes in foot and ankle patients have used PROMIS measures. Hu et al 22 compared postoperative improvement in PROMIS Physical Function and Pain Interference scores within patients undergoing forefoot, midfoot, hindfoot, and Achilles procedures and found no differences between operative groups. Given the variation in scores we identified between those with osteoarthritis and hallux valgus (both forefoot pathologies), we believe there is utility in studying these outcomes at the diagnosis or procedural level. Ho et al 20 found that foot and ankle patients with low PROMIS Depression scores (<41.5) were unlikely to achieve improvements in depression postoperatively. Nixon et al 33 found that patients with high preoperative PROMIS Anxiety scores undergoing foot and ankle surgery experienced meaningful improvements in pain; however, patients with higher preoperative anxiety had more residual pain postoperatively. Our study builds on prior work by further emphasizing mental health as an important consideration and by offering more specific data as to how individual diagnoses may be associated with trends in mental health outcomes.
In line with previous research,3,15,32,33,35 our study reveals a positive correlation between physical and mental health, regardless of diagnosis. When comparing across diagnoses, we found a stronger correlation between physical and mental health in the context of chronic conditions. Although worse physical function is generally associated with worse mental health, our results suggest that the chronicity of a condition may have a more significant impact on mental health than the degree of physical disability. That said, the cross-sectional nature of our study restricts our ability to comment on the directionality of the relationship between mental health and physical function.
Although the relationship between chronicity and mental health may be expected, we found a counterintuitive trend wherein diagnoses with better mean physical function scores were associated with larger negative effects on mental health (with the exception of foot/ankle OA). Our findings suggest that patients with chronic conditions, who may not appear functionally restricted, may be suffering mentally more than might be expected based on their functional status. For example, although a hallux valgus diagnosis is typically associated with relatively unimpaired physical function, we found this diagnosis to be associated with one of the largest negative effects on mental health. Cosmesis could play a role in this, although given the study design we cannot definitively comment on causation. Of note, although more female patients presented with hallux valgus (1668 vs 339), we found no sex differences in PF10a or PGM scores.
As expected, compared to the mean of the general (ie, nonclinical) US population, the mean PF10a scores across all diagnoses in our sample were lower. Interestingly, the mean PF10a scores for patients with hallux valgus, hallux rigidus, and hammertoes were all considered “within normal limits” (45-62), albeit on the lower end of this range. This calls for further investigation into what is motivating these patients to seek care. Indeed, this finding dovetails with that of Bernstein who found that one-fourth of new orthopaedic patients reported their symptoms to be acceptable at presentation. 8 A potential explanation is that these patients have degraded physically from their own personal “normal” and feel they may benefit from some intervention. Although this may be true in many cases, there may also be situations where this change in status may be the result of normal, nonmodifiable factors (eg, aging), which may not be initially suitable to intervention.
The effects on mental health associated with diagnoses of hallux valgus, foot/ankle OA, and hammertoes all exceeded the diagnosis specific MCIDs calculated for PGM. Remarkably, mental health for patients with foot/ankle OA was found to improve with age; this may be due to patients becoming more accepting of their declining physical condition, or perhaps reflective of the established trend of improved mental health with age.21,31 Except for foot/ankle osteoarthritis, all diagnoses had mean PGM scores slightly higher than the general US population (>50), and all diagnoses had on average “very good” (48-56) mental health. This is somewhat surprising given prior reports of poor mental health among foot and ankle patients, especially those with chronic conditions.15,16,36 This discordance may represent the decline in mental health associated with worsening physical condition between the time of initial presentation, when we collected our data, compared to later in the disease process when other studies collected their data (primarily preoperatively). Alternatively, the relatively high mental health scores of our cohort may be related to the overall higher educational attainment and household income, as such factors are known to correlate with mental health outcomes.9,11 That said, we believe that patients who are presenting to the clinic—spending time and money—are doing so because their experience has compelled them to seek care, and any potential improvement is worth working toward. Although orthopaedic surgeons are not trained mental health counselors, they can still play a role in alleviating patient anxiety and by helping facilitate access to mental health resources if necessary.
This study has several limitations. First, data were gathered at a single institution and thus may have limited generalizability to other domestic or international regions; however, our cohort was very large and likely similar to other major US metropolitan populations. Second, our data may not accurately reflect all patients presenting to our clinic. It is unclear whether patients who did not complete the PROMs declined or were unable to participate because of other barriers. 7 Third, we were unable to further discriminate between diagnoses labeled “Foot/ankle OA” as this categorization reflected the ICD-10 code used and we were limited by what was entered into the EMR. Fourth, although CCI was included in our multivariable regression model exploring the associated effects of diagnosis on mental health, we were unable to control for other musculoskeletal concerns that may confound these relationships. Lastly, our categorization of acute vs chronic is imperfect in that we do not know how long patients had symptoms at the time of presentation. Prospective studies are needed to assess the temporal association between mental health and physical function by foot and ankle diagnosis.
In summary, there is considerable variation in self-reported physical function and mental health across common foot and ankle diagnoses. Physical function and mental health appear to be more tightly correlated in chronic than in acute conditions. More chronic conditions were associated with larger negative effects on mental health, including diagnoses that are generally associated with relatively unimpaired physical function. Future studies may examine interventions to mitigate the negative effects of chronic foot and ankle conditions on mental health and whether such interventions are also associated with improvements in self-reported pain and functional status.
Supplemental Material
sj-docx-2-fai-10.1177_10711007241231974 – Supplemental material for Differences in Baseline Physical Function and Mental Health PROM Scores in Patients With Foot and Ankle Conditions
Supplemental material, sj-docx-2-fai-10.1177_10711007241231974 for Differences in Baseline Physical Function and Mental Health PROM Scores in Patients With Foot and Ankle Conditions by Jeremy T. Smith, Emily B. Parker, Eric M. Bluman, Elizabeth A. Martin and Christopher P. Chiodo in Foot & Ankle International
Supplemental Material
sj-docx-3-fai-10.1177_10711007241231974 – Supplemental material for Differences in Baseline Physical Function and Mental Health PROM Scores in Patients With Foot and Ankle Conditions
Supplemental material, sj-docx-3-fai-10.1177_10711007241231974 for Differences in Baseline Physical Function and Mental Health PROM Scores in Patients With Foot and Ankle Conditions by Jeremy T. Smith, Emily B. Parker, Eric M. Bluman, Elizabeth A. Martin and Christopher P. Chiodo in Foot & Ankle International
Supplemental Material
sj-docx-4-fai-10.1177_10711007241231974 – Supplemental material for Differences in Baseline Physical Function and Mental Health PROM Scores in Patients With Foot and Ankle Conditions
Supplemental material, sj-docx-4-fai-10.1177_10711007241231974 for Differences in Baseline Physical Function and Mental Health PROM Scores in Patients With Foot and Ankle Conditions by Jeremy T. Smith, Emily B. Parker, Eric M. Bluman, Elizabeth A. Martin and Christopher P. Chiodo in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_10711007241231974 – Supplemental material for Differences in Baseline Physical Function and Mental Health PROM Scores in Patients With Foot and Ankle Conditions
Supplemental material, sj-pdf-1-fai-10.1177_10711007241231974 for Differences in Baseline Physical Function and Mental Health PROM Scores in Patients With Foot and Ankle Conditions by Jeremy T. Smith, Emily B. Parker, Eric M. Bluman, Elizabeth A. Martin and Christopher P. Chiodo in Foot & Ankle International
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the Mass General Brigham IRB (Protocol #: 2021P002691).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.