
Abstract
Background:
This study aimed to compare the complications and outcomes of lateral and central Achilles tendon–splitting approaches for the treatment of Haglund syndrome.
Methods:
Patients who underwent surgery for Haglund syndrome between June 2012 and June 2022 were included in the study. Patients undergoing lateral approach surgery were included in group 1, whereas patients undergoing central Achilles tendon-splitting approach surgery were included in group 2. Surgical outcomes of the patients were evaluated using the American Orthopaedic Foot & Ankle Society (AOFAS) ankle hindfoot scale, visual analog pain scale (VAS), and Victorian Institute of Sport Assessment–Achilles (VISAA) scores. In addition, preoperative and final follow-up scores were compared.
Results:
The study included 66 patients: 32 (14 females, 18 males) underwent surgery using the lateral approach in group 1, whereas in group 2, 34 patients (18 females, 16 males) underwent surgery using the central Achilles tendon–splitting approach. There was a significant statistical difference in the AOFAS, VISAA, and VAS scores between preoperative and final follow-up for both group 1 and group 2 (P < .001, P < .001, P < .001, P < .001, respectively). Group 1 had a small (0.76) relative increase in VAS score compared with group 2 (P = .033). There was no significant difference between the complication rates of group 1 and group 2.
Conclusion:
In our study, we found the lateral approach and central Achilles tendon–splitting approaches to be safe and effective in the surgical treatment of Haglund syndrome without clinically meaningful differences in outcomes or complication rates.
Introduction
Posterior heel pain is a common cause of orthopaedic outpatient clinic presentation. First, Patrick Haglund described Haglund deformity as a posterior heel pain caused by a prominent posterosuperior corner of the calcaneus in combination with wearing a rigid low-back shoe in 1927. 18 Enlargement of the posterosuperior prominence of the calcaneus causes retrocalcaneal bursitis and insertional Achilles tendinitis. Haglund triad consists of the simultaneous presentation of Achilles tendinosis, Haglund deformity, and retrocalcaneal bursitis. 11
The treatment of Haglund syndrome is mainly conservative, such as shoe wear modification, heel lift, stretching of the gastrocnemius-soleus complex, anti-inflammatory medication, steroid injection, activity modification, and shockwave therapy. 12 Surgical treatment is recommended for patients who cannot achieve satisfactory results with 6 months of conservative treatment. 12 Surgical treatment includes Achilles tendon debridement, excision of bursal tissue, and resection of Haglund deformity. 10
Various surgical approaches have been identified for treatment, including the vertical J-shaped medial incision, endoscopic techniques, lateral incision, double incision, transverse Cincinnati incision, and central Achilles tendon–splitting incision.2,13,15 The medial J-shaped incision, in particular, allows for greater exposure to the lateral corner of the Achilles tendon insertion and ensures complete debridement.16,19 Two of the most commonly used approaches are the lateral approach and the central Achilles tendon-splitting approach. Good results have been reported with the lateral approach in the treatment of Haglund syndrome. 17 One of the advantages of the lateral approach is that the medial insertion of the Achilles tendon is wider. 20 With the lateral approach, the risk of postoperative avulsion is less. However, the risk of sural nerve injury is higher. 3 The central Achilles tendon-splitting approach was first described in 2002 with good clinical outcomes.9,13 The advantage of the central tendon-splitting approach is that all pathologies can be accessed with a single incision, and the risk of sural nerve injury is lower. 15 The disadvantages of the central tendon-splitting approach are wound healing problems, painful scar, and wound infections.
For surgical treatment, there are different approaches. There is no consensus on the choice of surgical approach. This study compares the complications and outcomes of lateral and central Achilles tendon–splitting approaches.
Materials and Methods
This study evaluated patients with Haglund syndrome who were admitted to our outpatient clinic between January 2015 and January 2022 retrospectively. After approval of the Institutional Ethics Committee (E1-23-3950), patient databases were reviewed. All researchers who participated in the study signed the most recent version of the Helsinki Declaration. Informed consent forms were obtained from all of the patients in the study.
Our study had a retrospective design. Patients who were operated for Haglund syndrome between June 2015 and June 2022 were included in the study. These patients were diagnosed with Haglund triad, which consists of the simultaneous presentation of Achilles tendinosis, Haglund deformity, and retrocalcaneal bursitis. Preoperative physical examinations of the patients were performed, and anterior-posterior and lateral foot radiographs and MRI were evaluated. Haglund triad was confirmed by physical examination and imaging studies. The same conservative treatment protocol was applied to all patients. Surgical treatment was recommended for patients who did not respond to conservative treatment for more than 6 months. All patients were operated with lateral or central Achilles tendon–splitting approaches (Figure 1).
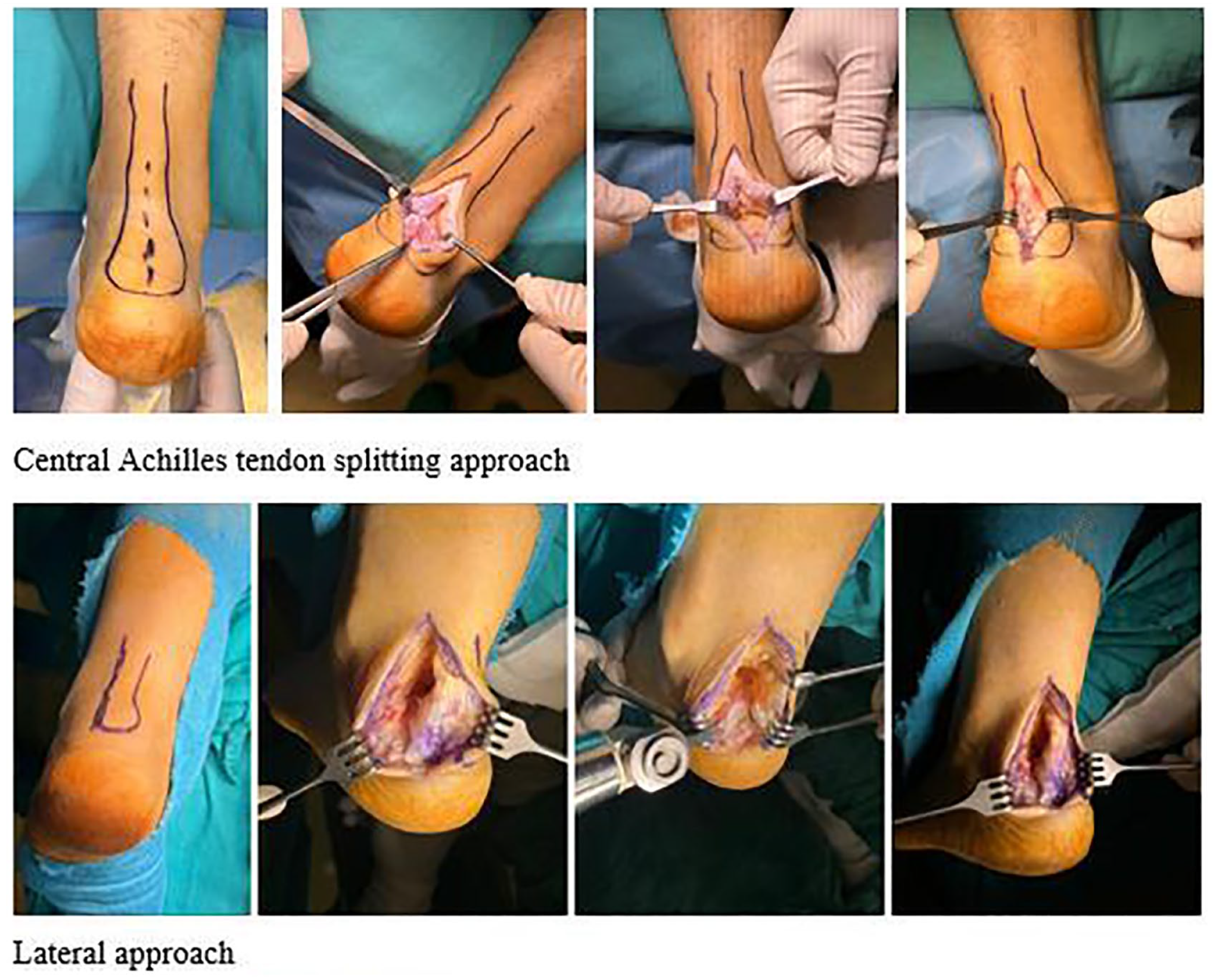
Lateral and central Achilles tendon–splitting approaches for Haglund deformity.
Inclusion criteria:
Patients with Haglund syndrome
>6 months of conservative treatment with unsatisfactory results
Age >18 years
>12 months’ follow-up
Surgical treatment with lateral or central Achilles tendon–splitting approach
Exclusion criteria:
History of foot trauma or surgery
Neuromuscular pathology
Patients with inflammatory arthritis
<6 months’ conservative treatment
All patients were operated in the prone position with a tourniquet. Depending on the surgeon’s decision, a lateral or central Achilles tendon–splitting approach was preferred for all patients. Two of the surgeons in the surgical team used the central Achilles splitting approach in all their cases, whereas the other 2 surgeons used the lateral approach in all their cases. The surgeons chose the approach based on their preferences. Patients who were operated with a lateral approach were included in group 1, and those who were operated with the central Achilles splitting approach were included in group 2. Excision of the retrocalcaneal bursa, debridement of the Achilles tendon, and resection of Haglund prominence were performed for all patients. The Achilles tendon was reattached to the calcaneus with a single-row suture anchor technique.
The lateral approach was located 3 mm anterior to the lateral border of the Achilles tendon. And the lateral incision was started 3 cm proximal of the calcaneus superior crest and extended distally to the insertion of the Achilles tendon on the calcaneus. The Achilles tendon was lifted from lateral to medial of the calcaneus as a full thickness flap. Next, the retrocalcaneal bursa was removed and calcaneal osteotomy was performed with an oscillating bone saw to excise the Haglund deformity. Excision of the Haglund deformity was confirmed with intraoperative fluoroscopy and Achilles tendon insertion debridement was performed. It was difficult to evaluate the medial part of the calcaneus with the lateral approach. However, if necessary, the Achilles could be completely stripped from the calcaneus and visualization of the medial calcaneus could be achieved, although it was difficult. Finally, the Achilles tendon was reattached with a single-row suture anchor technique.
The central Achilles splitting approach was described by McGarvey et al. 13 First, a midline skin incision was made proximal to the Achilles tendon insertion, extending distally for about 8 cm. The paratenon was centrally incised and the Achilles tendon was split centrally, starting from the attachment point of the bone tendon and moving proximally. Nest, the Haglund deformity was revealed on stripping the Achilles tendon from the calcaneus bilaterally. The retrocalcaneal bursa was then removed and calcaneal osteotomy was performed from distal to proximal with an oscillating bone saw to excise the Haglund deformity. Excision of the Haglund deformity was confirmed with intraoperative fluoroscopy. Then, Achilles tendon was reattached with a single-row suture anchor technique. Finally, the split tendon and paratenon were repaired with sutures.
A short leg cast was applied with 10-degree plantar flexion for the first 2 weeks. After 2 weeks, the skin sutures and short leg cast were removed and the patients started to use the walking boot. Also, partial weightbearing and rehabilitation exercises were started. The walking boot was used for 6 weeks. After 6 weeks, weightbearing was allowed and the walking boot was removed. After 3 months, patients were allowed to resume normal daily activities. The same physiothearpy protocol was applied in all patients.
The American Orthopaedic Foot & Ankle Society (AOFAS) ankle hindfoot scale, visual analog pain scale (VAS), and the Victorian Institute of Sport Assessment–Achilles (VISAA) scores were used to evaluate the surgical outcomes of the patients. Preoperative and final follow-up scores were compared. Additionally, complication rates of patients treated with different approaches were compared. And patients were asked whether they would choose to undergo the same surgical treatment again if they needed it again at the 12-month follow-up.
Statistical Analysis
Statistical data analyses were performed using SPSS 22.0 software (SPSS Inc, Chicago, IL, USA). Categorical variables were compared between groups using the χ2 test. The suitability of continuous variables to normal distribution was examined by calculating skewness and kurtosis values. Continuous variables with normal distribution were compared using the independent samples t test, and continuous variables with non-normal distribution were compared using the Mann-Whitney U test. Measurements taken before and after the surgery were analyzed using the dependent sample t test. The results were evaluated within 95% CIs, and P <.05 was considered significant.
Results
Sixty-six patients were included in the study. In group 1, 32 patients (14 female, 18 male) were operated with a lateral approach. The mean age in group 1 was 45.5 ± 11.3 years. Twenty-one right (65.6%) and 11 left (34.4%) Haglund deformities were operated on. In group 2, 34 patients (18 female, 16 male) were operated on using a central Achilles tendon–splitting approach. The mean age of group 2 was 46.3 ± 11.5 years. Thirteen right (38.2%) and twenty-one left (61.8%) Haglund deformities were operated on. The mean follow-up duration was 20 months (12-72 months) for group 1 and 19.5 months (13-30 months) for group 2. There was no significant difference between group 1 and group 2 in gender, age, and the following time (P = .45, P = .78, and P = .95, respectively) (Table 1).
Demographic Characteristics of the Patients.
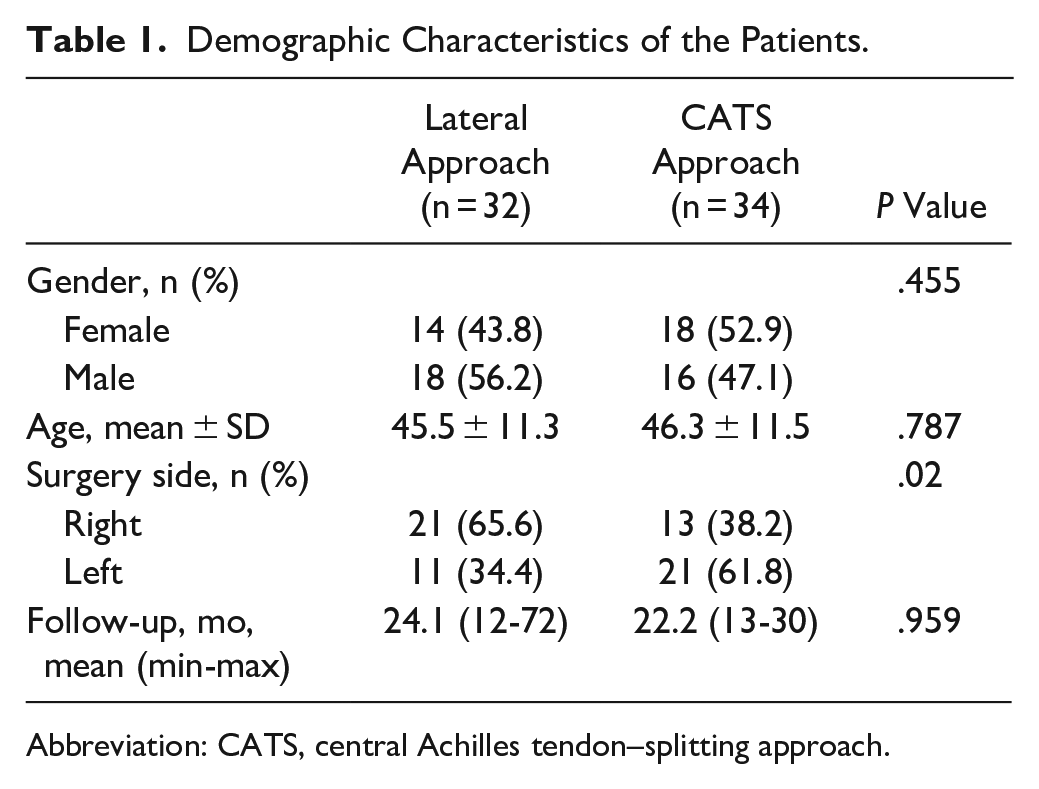
Abbreviation: CATS, central Achilles tendon–splitting approach.
For group 1, preoperative and final follow-up mean AOFAS scores were 60.59 ± 6.19 and 91.43 ± 6.59, respectively. Preoperative and final follow-up mean VISAA scores were 54.65 ± 7.9 and 83.65 ± 6.27, respectively. Moreover, VAS scores improved from 8.0 ± 0.96 to 2.2 ± 0.993. A statistically significant difference was found between the preoperative and final follow-up AOFAS, VISAA, and VAS scores of group 1 (P < .001, P < .001, and P < .001, respectively) (Table 2).
Comparison of Preoperative and Final Follow-up Scores. a
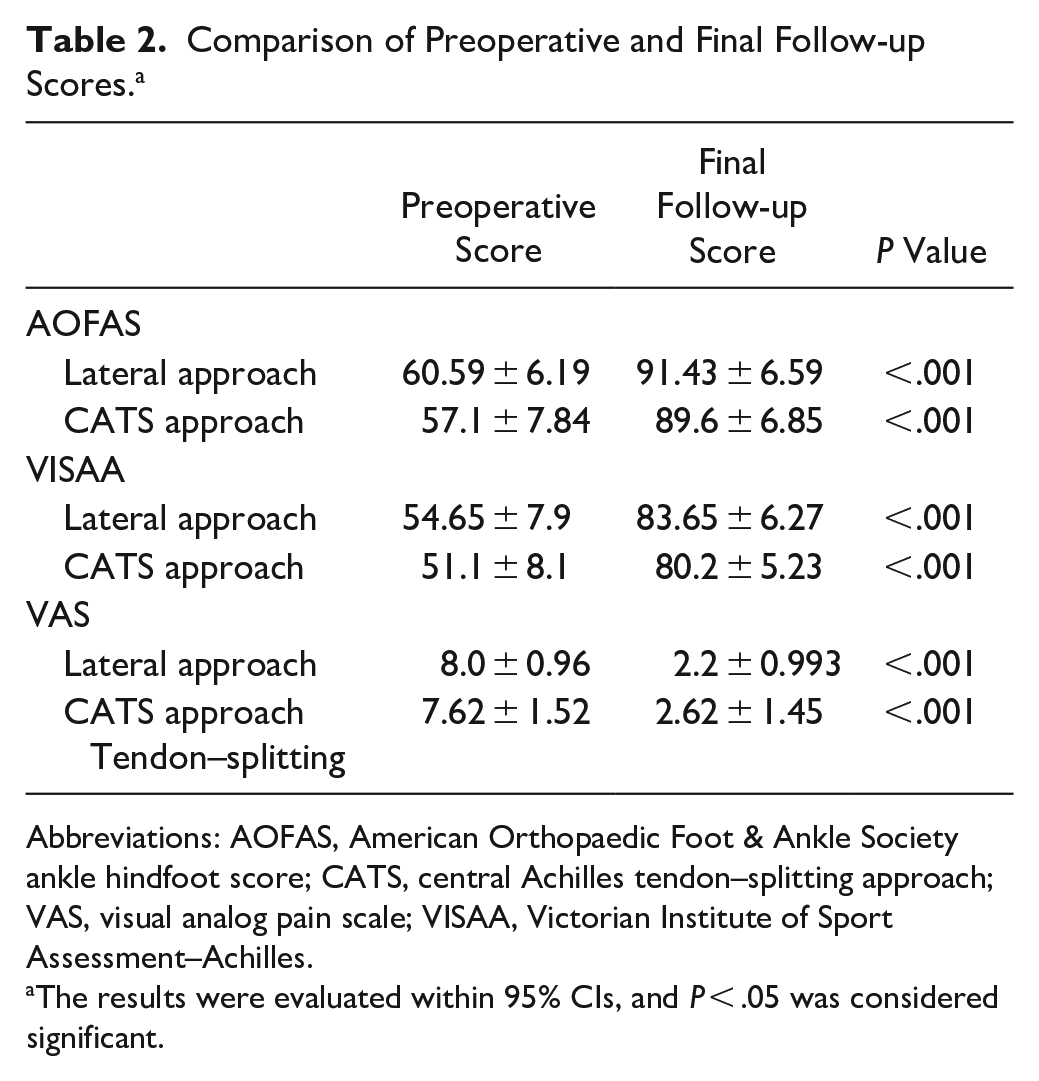
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society ankle hindfoot score; CATS, central Achilles tendon–splitting approach; VAS, visual analog pain scale; VISAA, Victorian Institute of Sport Assessment–Achilles.
The results were evaluated within 95% CIs, and P < .05 was considered significant.
For group 2, preoperative and final follow-up mean AOFAS scores were 57.1 ± 7.84 and 89.6 ± 6.85. Preoperative and final follow-up mean VISAA scores were 51.1 ± 8.1 and 80.2 ± 5.23. Furthermore, VAS scores were improved from 7.62 ± 1.52 to 2.62 ± 1.45. A statistically significant difference was determined between the preoperative and final follow-up AOFAS, VISAA, and VAS scores of group 2 (P < .001, P < .001, P < .001, respectively) (Table 2).
When the changes in AOFAS and VISAA scores in group 1 and group 2 were compared, there was no significant difference (P = .368, P = .960, respectively). However, a statistically significant difference was determined between VAS score changes in group 1 and group 2 (P = .033). VAS score improvement was greater in the lateral approach group (Table 3). The preoperative and postoperative VAS score change between group 1 and group 2 is 0.8. Although this creates a statistically significant difference, it was not create a clinically significant one. The effect size, as measured by Cohen d, was 0.53, indicating a medium effect.
Comparison of Preoperative and Postoperative Scores for Lateral and Central Achilles Tendon–splitting Approaches. a
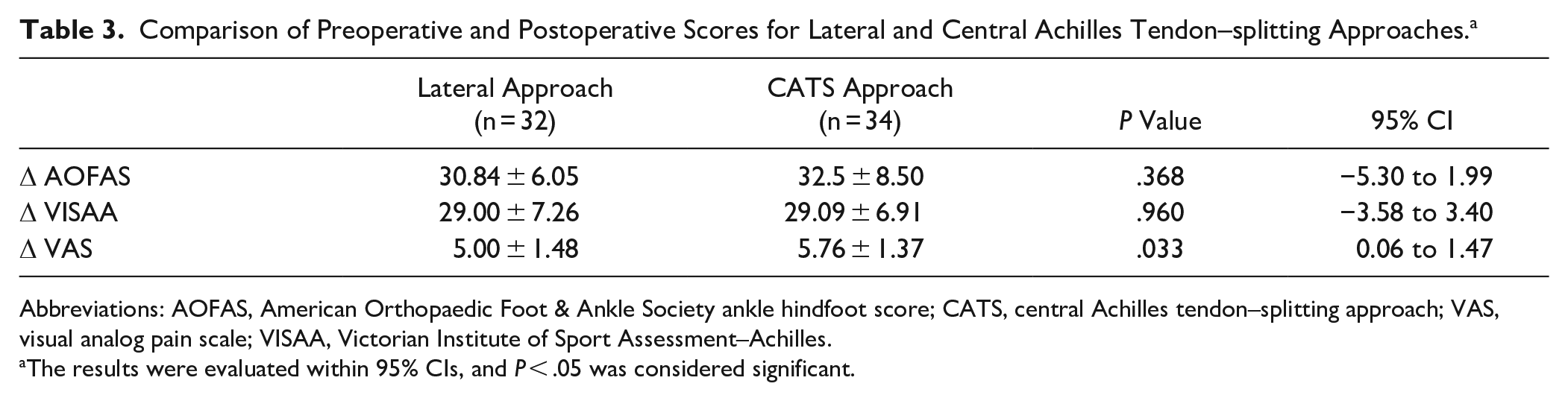
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society ankle hindfoot score; CATS, central Achilles tendon–splitting approach; VAS, visual analog pain scale; VISAA, Victorian Institute of Sport Assessment–Achilles.
The results were evaluated within 95% CIs, and P < .05 was considered significant.
Four of the patients (2 patients in group 1 and 2 in group 2) had paresthesia around the wound. Four of the patients (1 patient in group 1 and 3 in group 2) had superficial infections. Three patients were treated with medical therapy. Debridement was performed on 1 patient. One of the patients (group 2) had delayed wound healing. One of the patients (group 2) had a hypertrophic scar. Scar revision was recommended to the patient, but the patient did not accept it (Table 4). There was a significant difference between the complication rate of group 1 (9.37%) and group 2 (20.58%) (P = .034). The effect size, as measured by Cohen d, was 0.61, indicating a medium effect. In our study, early period complications were paresthesia around the wound, superficial infection, hypertrophic scar, and delayed wound healing. However, superficial infection and delayed wound healing problems were resolved in the first 3 months. At the final follow-up, the patients’ complaints due to paresthesia around the wound were decreased but continued. And there was no significant difference between the complication rates of group 1 and group 2 after 3 months (P = .69).
Complications of Lateral and Central Achilles Tendon–splitting Approaches.
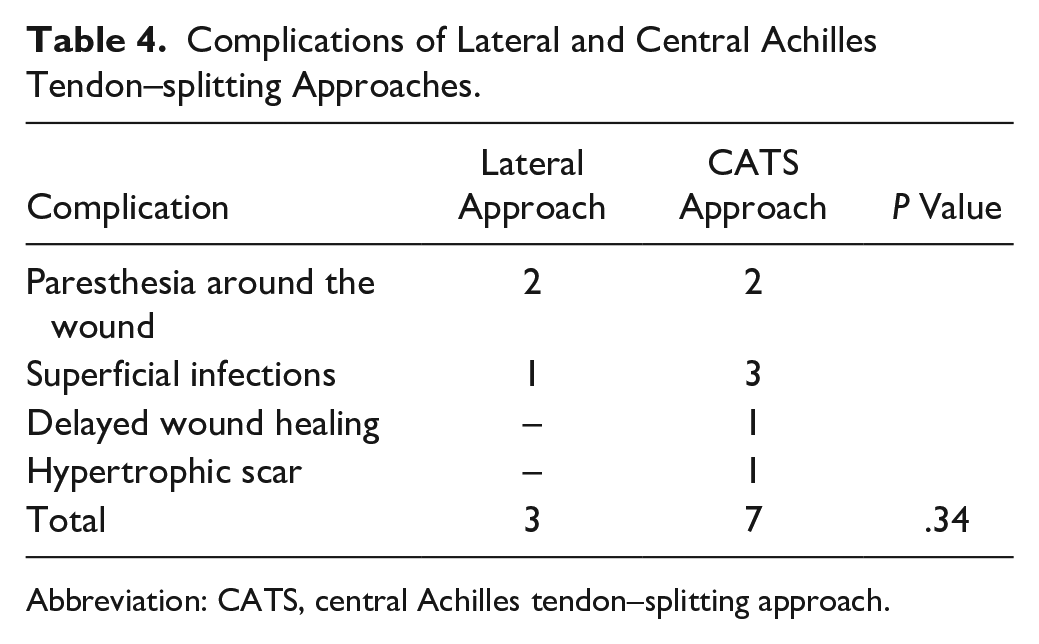
Abbreviation: CATS, central Achilles tendon–splitting approach.
When asked if they would make the same decision to undergo surgery, 30 patients (93.8%) in group 1 and 30 patients (88.2%) in group 2 reaffirmed their initial decision for operative intervention. There was no significant difference between the groups (P = .436).
Discussion
In the current study, when the results of Haglund syndrome surgery performed with lateral and central Achilles tendon–splitting approaches were compared, the complication rates are similar. For patient-reported outcomes, we found the AOFAS and VISAA scores to be similar, but improvement in VAS score was slightly greater (0.76) in patients who underwent a lateral approach. Whether this is clinically meaningful is unknown as this magnitude is below most estimates of a clinically meaningful change in a 0-10 VAS scale.
Different approaches can be used in the surgical treatment of Haglund syndrome. In this study, lateral and central Achilles tendon–splitting approaches are compared. The advantage of the central Achilles tendon–splitting approach is that it provides easy access to all pathologies. The advantage of the lateral approach is that the medial part of the Achilles tendon insertion can be preserved, and the risk of postoperative avulsion is less. 20 Good clinical results have been reported with the lateral and central Achilles tendon–splitting approach in the surgical treatment of Haglund syndrome.14,21 The central Achilles splitting approach is purported to be more appropriate for patients with Haglund syndrome who have medial-side calcaneus pathology. 1 However, in this study, the surgeons had no difficulty in reaching medial-part Achilles tendon pathologies with a lateral approach. Patients were randomly selected. Two of the surgeons in the surgical team used the central Achilles splitting approach in all their cases, whereas the other 2 surgeons used the lateral approach in all their cases. And good clinical results were obtained with both approaches. Moreover, there was no notable difference in clinical scores.
For all patients, excision of the retrocalcaneal bursa, debridement of the Achilles tendon, and resection of Haglund prominence were performed. Ettinger et al 4 treated 40 patients with a central Achilles tendon–splitting approach, and the average AOFAS and VAS scores improved from 59.4 to 86.5 and 8.5 to 2.6, respectively. Jiang et al 8 treated 14 patients with a lateral approach, and the average AOFAS and VAS scores improved from 67 to 90 and 4.82 to 1.21, respectively. In this study, AOFAS and VAS scores showed improvements consistent with the literature. The difference in preoperative and postoperative VAS score changes between the lateral approach group and the central Achilles tendon–splitting approach group was 0.76. Although this was found to be a statistically significant difference, it does not create a clinically significant difference.
Haglund syndrome is more commonly seen in women. However, in our study, the number of male patients was higher. The treatment of Haglund syndrome is primarily conservative. And all patients in this study were operated after 6 months of conservative treatment. The complication rates for open surgery were about 12.3%. 22 In the current study, the complication rate was 15.15%. The complication rate of the central Achilles tendon–splitting approach was 20.58% and for the lateral approach with 9.37%, but this difference is not statistically significant (P = .34). Complications for a lateral approach were paresthesia around the wound and superficial infection. Complications for the central Achilles tendon–splitting approach were paresthesia around the wound, superficial infection, hypertrophic scar, and delayed wound healing. Yuen et al 22 reported that for open Haglund surgery, the complication rates of paresthesia around the wound and superficial infection were 4.3% and 3%, respectively. In our study, the complication rate of paresthesia around the wound and superficial infection were 6% and 6%, respectively. In the central Achilles tendon–splitting approach, shoe-related problems are more common because of scar irritation. 7 Xia et al 21 reported that the lateral approach provided better short-term pain relief and reduced delayed wound healing compared with the central Achilles tendon–splitting approach. In our study, there was no scar irritation or delayed wound healing in patients treated with the lateral approach. One of the patients treated with the central Achilles splitting approach had scar irritation, and one had delayed wound healing. In previous studies when the endoscopic approach has been compared with other approaches including the central splitting and lateral, there has been shown to be less risk of scar irritation, wound infection, and sural nerve injury. However, in the current study, the endoscopic approach was not used.
In the lateral approach, all medial Achilles lesions can be reached after the detachment of lateral Achilles insertion. 8 In the current study, the lateral approach could access almost all pathologies. Although some studies have shown concern for sural nerve injury in the lateral approach, 6 a number of cadaver studies have shown a safe approach to the Achilles without injury to the sural nerve. 5 In our study, there was no difference between the 2 approaches for sural nerve injury.
There are several limitations to our study. First, our study had a retrospective design. Second, only a limited number of patients were evaluated in the study.
Conclusion
The lateral approach and central Achilles tendon–splitting approach are equally safe and effective in the surgical treatment of Haglund syndrome.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007241250003 – Supplemental material for Comparison of Lateral and Central Achilles Tendon–Splitting Approaches in the Treatment of Haglund Deformity
Supplemental material, sj-pdf-1-fai-10.1177_10711007241250003 for Comparison of Lateral and Central Achilles Tendon–Splitting Approaches in the Treatment of Haglund Deformity by Enver Kilic, Olgun Bingol, Guzelali Ozdemir, Alper Deveci, Atahan Durgal and Taha Esref Karahan in Foot & Ankle International
Footnotes
Ethical Approval
Ethical approval for this study was obtained from Ankara City Hospital Ethical Committee (E1-22-2376, approval date: February 23, 2022),
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.