
Abstract
Background:
The main goal of this study was to evaluate postoperative changes in the length of the first metatarsal (M1) and the proximal phalanx of the hallux (P1) after acellular dermal allograft interpositional arthroplasty (ADA-IPA). We hypothesized that there would be a shortening of the first ray at the first metatarsal, the proximal phalanx, or both.
Methods:
In this retrospective study, we assessed patients who underwent ADA-IPA between 2019 and 2022. On standing anteroposterior (AP) foot radiographs, we measured first metatarsal (M1), second metatarsal (M2), proximal phalanx (P1), and the entire hallux (HX) lengths. M1/M2 and P1/HX ratios were calculated. The first metatarsophalangeal joint space was calculated. All measurements were recorded preoperatively, at 6 weeks postoperatively, and at final follow-up.
Results:
The pilot study included 11 patients. At final follow-up, we found shortening of M1 and P1 in comparison to the preoperative length, as evidenced by lower M1/M2 (82.6 ± 2.3 vs 75.4 ± 5.1; P = .001) and P1/HX ratios (53.4 ± 2.3 vs 48.9 ± 7.9; P = .001). Follow-up length was negatively correlated with M1/M2 (r = −0.76, P = .003).
Conclusion:
ADA-IPA might be associated with shortening of both first metatarsal and proximal phalanx, with the former showing progressive shortening.
Introduction
First metatarsophalangeal joint (first MTP) interpositional arthroplasty (IPA) entails resection of the damaged articular surface, osteophytes, joint decompression, and implantation of tissues at the joint interface. 10 It is considered a “bridging” procedure to postpone first metatarsophalangeal joint (MTPJ) fusion. 7 Interpositional arthroplasty using acellular dermal allograft (ADA-IPA) is an appealing option for hallux rigidus (HR) patients who prefer a joint-sparing procedure. 3
In our recent experience, despite observing overall good initial clinical outcomes, progressive shortening of the first metatarsal was observed in patients treated with ADA-IPA, which can lead to reported complications such as cock-up hallux deformity and transfer metatarsalgia. 3 To the authors’ knowledge, direct measurements of first metatarsal length following IPA-ADA have not been reported in the literature. The primary goal of this study was to investigate post–IPA-ADA changes in first metatarsal (M1) and proximal phalanx (P1) lengths. We hypothesized that significant first-ray shortening at the first metatarsal, the proximal phalanx, or both would be observed.
Methods
Study Design and Sample
In this institutional review board–approved retrospective study, patients who underwent IPA-ADA at a single institution between 2019 and 2022 were analyzed. Patients were excluded if they had 1 or more of the following: revision procedures, associated lesser metatarsal procedures, inflammatory arthritis, and incomplete medical records.
Surgical Technique
Dorsal approach to the first MTPJ was used to prepare the articular surface using cup-and-cone reamers (resection was limited to 1-2 mm of each articular surface). The ADA (Arthroflex, Arthrex, Naples, FL) was then prepared with 2 sets of central leading absorbable sutures, as well as corner routing absorbable sutures. The graft was then soaked in a bone marrow aspirate concentrate and introduced into the joint space. The graft was then fixed to the metatarsal under appropriate tension followed by standard layered closure (Figure 1).
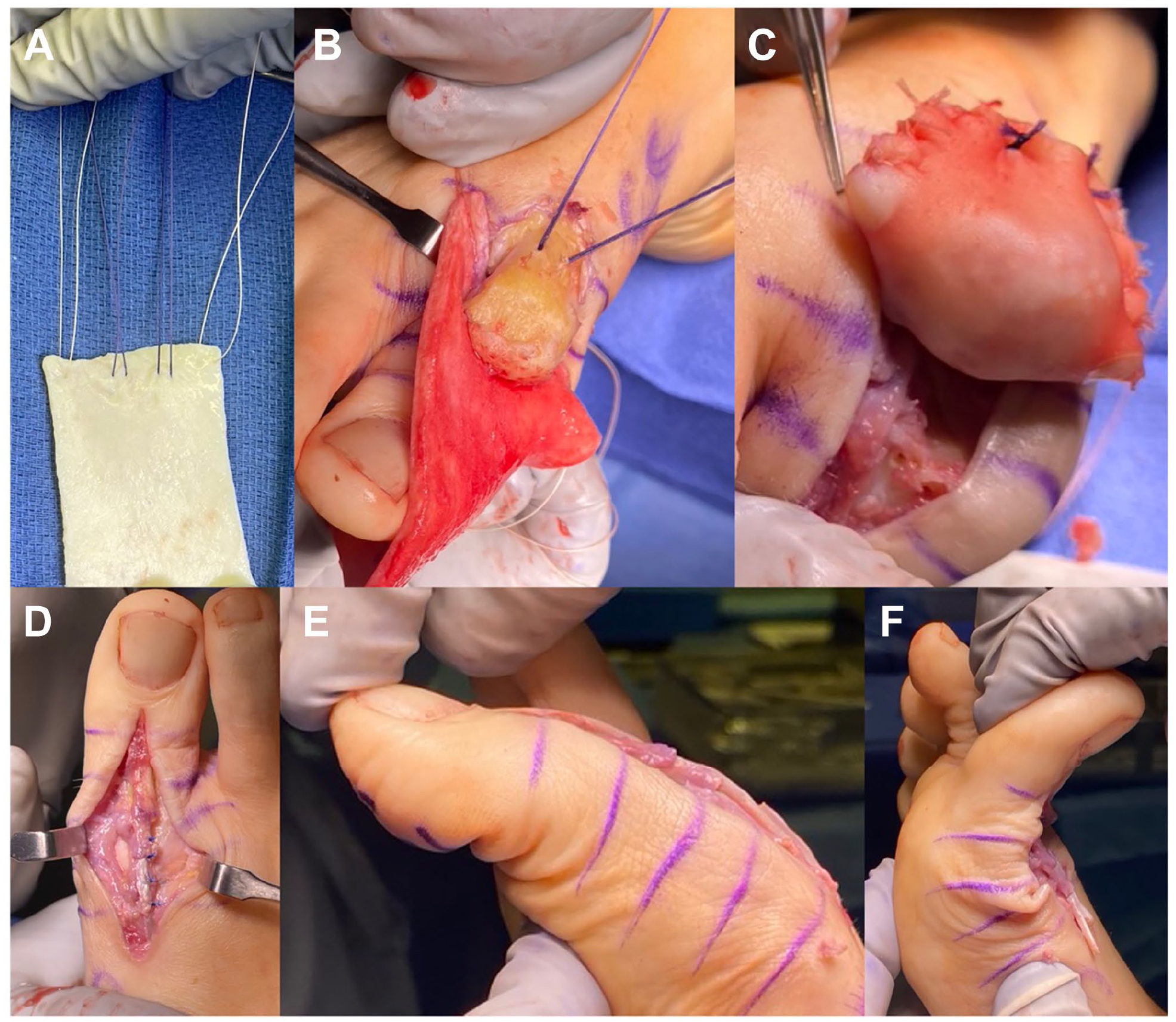
Surgical technique of ADA-IPA: (A) The dermal allograft is prepared on the backtable, where 2 corner routing sutures are placed in addition to 2 central leading sutures. (B) Leading sutures are retrieved through tunnels in the first metatarsal to apply the graft to the bone while routing sutures help tension the graft on the plantar aspect. (C) The graft is trimmed appropriately then corners are sutured with absorbable sutures. (D) The joint capsule is reapproximated. (E and F) Intraoperative assessment of range of motion of the first MTPJ. ADA-IPA, acellular dermal allograft interpositional arthroplasty.
Assessment
Weightbearing radiographs were performed before surgery, at 6 weeks after the procedure, and at final follow-up. The following measurements were carried out on standing anteroposterior (AP) foot radiographs:
First metatarsal (M1) length (mm): M1 length was measured between two points connecting the center of the proximal and distal articular surfaces of the first metatarsal (Figure 2A).
Second metatarsal (M2) length (mm): centers of the proximal and distal articular surfaces of the second metatarsal were identified. M2 was recorded as the distance between the two centers (Figure 2A).
Hallux proximal phalanx (P1) length (mm): P1 was measured as the distance between the centers of the proximal and distal articular surfaces of the hallux proximal phalanx (Figure 2C)
Hallux (Hx) length (mm): This was recorded as the distance from the center proximal articular surface of the hallux proximal phalanx to the tip of the hallux distal phalanx (Figure 2C).
Metatarsal and hallux ratios (M1/M2, P1/HX, %): The ratio of M1 length to M2 length was analyzed as a marker of potential shortening of the first metatarsal. Similarly, to study potential P1 shortening, the ratio P1/HX was calculated (Figure 2).
First metatarsophalangeal joint space measurements: The most medial aspect of the articular surface of the proximal phalanx and the first metatarsal were defined. The distance between these 2 points were measured to represent the width of the medial first MTPJ space. The lateral MTPJ space width was analogously measured (Figure 2D). The average first MTPJ space was calculated using this formula 4 :

7. Metatarsal head osteonecrosis: Osteonecrotic changes of the first metatarsal head was evaluated according to the Meier and Kenzora criteria. 8
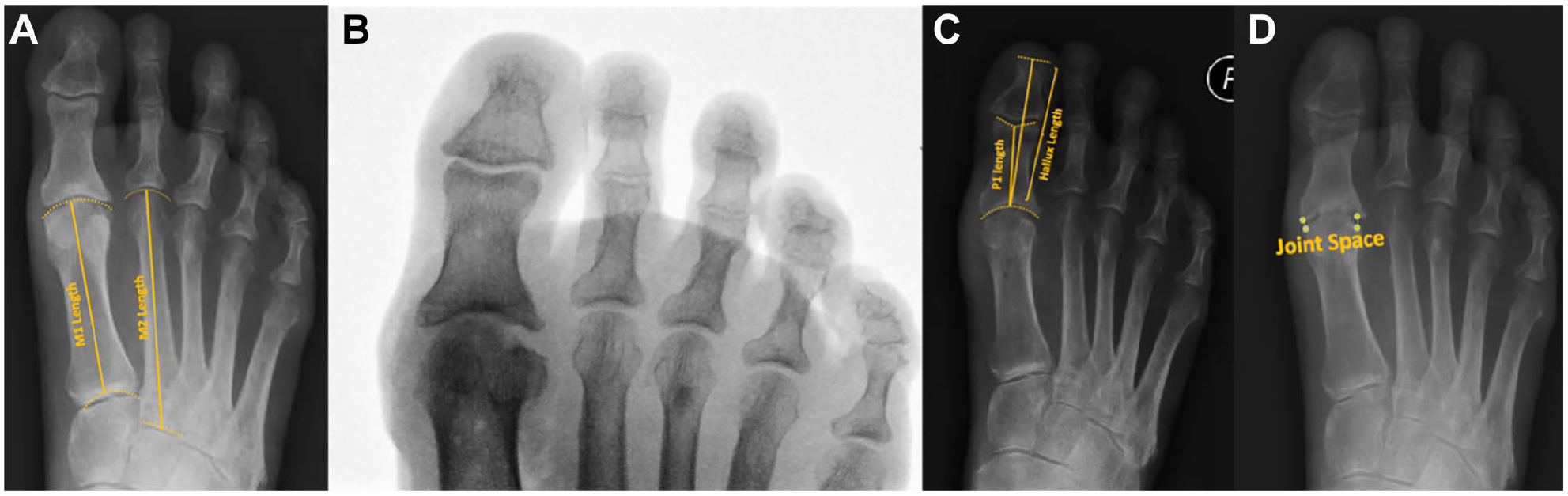
(A) Preoperative foot radiographs. M1 length: the length of the first metatarsal, defined as the distance between the center of the distal and proximal articular surfaces of the first metatarsal bone. M2 length: the length of the second metatarsal, measured as the distance between the center of the proximal and distal second metatarsal bone. (B) Intraoperative fluroscopic image after ADA-IPA. (C) Six-week postoperative radiographs. P1 length: the length of the proximal phalanx of the hallux, measured between the centers of the disal and proximal articular surfaces. HX length: measurement of the full length of the hallux from the center of the proximal articular surface of the proximal phalanx to the distal tip of the distal phalanx. (D) Nine-month postoperative radiographs. Measurement of the first MTPJ space between the most medial and lateral corresponding points on the articular surfaces of the first metatarsal and proximal phalanx. ADA-IPA, acellular dermal allograft interpositional arthroplasty; MTPJ, metatarsophalangeal joint.
Outcomes
Statistical analysis
Comparison of preoperative and postoperative measurements and outcomes was performed using analysis of variance or the Kruskal-Wallis test according to data normality. The Dunn-Bonferroni test was then performed for pairwise group comparisons. Reliability of measurements was assessed using the intraclass correlation coefficient. Significant differences were established for P values under .05.
Results
The study included 11 eligible patients; patients demographics and characteristics are illustrated in Table 1. Intraclass correlation coefficient for M1/M2 was 0.97 (95% CI 90.6-99.3, P < .001), P1/Hx was 0.95 (95% CI 84.9-98.9, P < .001), and joint space measurement was 0.9 (95% CI 64.2-97.4, P < .001). At final follow-up, there was shortening of the first ray in comparison to preoperative length at both the first metatarsal and proximal phalanx, as evidenced by differences in mean M1/M2 (82.6, SD ± 2.3 preoperatively, vs 75.4, SD ± 5.1 postoperatively; P = .001) and P1/HX ratios (53.4, SD ± 2.3 preoperatively, vs 48.9, SD ± 7.92 postoperatively; P = .01). A significant negative correlation between follow-up length and M1/M2 (r = –0.76, P = .003) was present. No metatarsal head osteonecrosis was observed using the proposed criteria. The average follow-up duration was 21 months (range 6-39).
Criteria and Demographics of Included Patients.

Abbreviation: BMI, body mass index.
Revision procedure after failed Cartiva implants.
Discussion
The most important finding of this study was shortening at both the first metatarsal (82.6 ± 2.3% preoperatively vs 75.4 ± 5.1% at final follow-up, P = .001) and proximal phalanx (53.4 ± 2.3% preoperatively vs 48.9 ± 7.9% at final follow-up, P = .01) after ADA. The average shortening of the first metatarsal at the final follow-up was 4.8 mm.
Shortening of the first metatarsal could jeopardize the procedural outcome in the short or long term with possible complications such as transfer metatarsalgia, cock-up hallux deformities and more challenging arthrodesis in the future.1,3,5,7 Although several prior reports tried to minimize bone resection to avoid complications (including the current work), there was a negative correlation between the length of the first metatarsal and the length of follow-up, suggesting progressive resorption at the interposition interface with subsequent shortening.3,5 Hirahara et al 6 studied postoperative ADA vascularity and thickness after shoulder superior capsular reconstruction (SCR). They found formation of pulsatile vessels and thickening of the graft at bone attachment (greater tuberosity). 6 Plachel et al 9 studied the histology of explanted ADA after SCR and found fibrocartilaginous changes induced by mechanical stresses. Local hyperemia, thickening of the graft, and stress-induced changes in the graft could play a role in bone resorption at the graft interface. Although avascular necrosis could affect the first metatarsal head especially after aggressive soft tissue stripping, it does not explain the shortening at the proximal phalanx. Aggressive intraoperative bone resection with violation of the strong subchondral bone could also lead to bone shortening. 2
The current work has several limitations. Small sample size and short follow-up limit the evaluation of the shortening extent and other potential complications. Although first metatarsal head osteonecrosis was not detected using radiographs, it is possible that some cases were missed. The study represents patients of a single surgeon, limiting the generalizability of the results.
Conclusion
ADA-IPA in the treatment of hallux rigidus was associated with possible risk of progressive shortening of the first metatarsal. Future studies to evaluate the biology at the graft-bone interface are needed. Patients with an existing short first metatarsal or lesser toes metatarsalgia may not be ideal candidates for the procedure. Patients probably should also be advised that they might need a bone block to restore first metatarsal length if fusion is indicated in the future.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007241281729 – Supplemental material for Progressive First Metatarsal Shortening Is Observed Following Dermal Allograft Interpositional Arthroplasty in Hallux Rigidus: Short Report
Supplemental material, sj-pdf-1-fai-10.1177_10711007241281729 for Progressive First Metatarsal Shortening Is Observed Following Dermal Allograft Interpositional Arthroplasty in Hallux Rigidus: Short Report by Aly Maher Fayed, Matthew Jones, Kepler Alencar Mendes de Carvalho, Emily Luo, Antoine Acker, Nacime Salomão Barbachan Mansur and Cesar de Cesar Netto in Foot & Ankle International
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the institutional review board at the University of Iowa Health Care (IRB 201904825).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.