
Abstract
Background:
Three-dimensional weightbearing CT (WBCT) has been widely used to assess foot and ankle alignment. However, most current measurement methods are based on 2-dimensional concepts—distance, long axis, angulation, etc—and are sensitive to changes in orientation of the WBCT images. This study demonstrated how changes in positioning of the image can significantly influence the evaluation of hindfoot alignment.
Methods:
WBCT scans of 10 feet without deformities were used. In the horizontal view, the long axis of the foot image was aligned to a neutral position and then rotated 5, 10, 15, and 20 degrees both internally and externally to simulate malposition. The Calcaneal Moment Arm (CMA) was measured by 2 investigators independently in the above positions. An intraclass correlation coefficient (ICC) model was used to assess the intra- and interobserver reliabilities. The correlation between the CMA and the rotation angle of the foot images was analyzed using linear regression.
Results:
The CMA measurements demonstrated that internal rotation of the image changed the neutral hindfoot into valgus, whereas external rotation led to varus. A 1-degree internal or external rotation of the image correlated with 0.48 (±0.03) mm increase or decrease in the modified WBCT-CMA value (P < .0001, R2 = 0.6406).
Conclusion:
This study demonstrated that although 3D WBCT provides the ability to observe the foot from different perspectives, current alignment evaluation tools are limited to 2 dimensions. Therefore, positioning the WBCT images in a consistent orientation is important to generate correct data.
Introduction
The hindfoot alignment is routinely evaluated in many foot and ankle disorders.8,18 In 1976, Cobey 7 introduced the posterior XR of the foot, a 2D radiographic method of imaging the leg and heel to assess the hindfoot alignment in the coronal plane. In 1995, Saltzman and El-Khoury 16 introduced the Apparent Moment Arm (AMA), a radiographic metric for quantitative assessments of the hindfoot alignment3,6 (XR-AMA). Several studies have pointed out the importance of foot positioning on the hindfoot alignment when using conventional 2-dimensional radiographic techniques.4,12 Buck et al 5 found that XR measurements as described by Cobey were not reliable and showed considerable divergence with rotation. Measurements using the XR-AMA manifested an almost linear relationship with progressive foot rotation during image acquisition. 5
Weightbearing computed tomography (WBCT) has been widely used for assessing the alignment of the foot and ankle.2,9,10,14 Compared with conventional 2-dimensional XR, WBCT can provide more information about the anatomic structures with greater precision and accuracy. 15 However, the hindfoot alignment evaluation tools that we use currently are based on 2-dimensional (2D) concepts: axis, distance, angulation, and translation. After loading the WBCT scans, positioning the image of the foot consistently for analysis remains important, and this has not been sufficiently studied. This study used the hindfoot alignment measurement on WBCT scans to demonstrate that changing the orientation of the foot images could significantly affect the hindfoot alignment.
Material and Methods
Subjects
This was a retrospective study with institutional review board approval for using existing WBCT scans captured as part of routine clinical care. WBCT scans of 10 feet without any foot and ankle deformities were included. Eight feet were from males and 2 feet were from females, and the age of the subjects averaged 35 years (range, 22-51 years, SD 11.18 years).
Measurement Methods and Data Collection
The hindfoot alignment evaluation method used in this study was modified from the Calcaneal Moment Arm (CMA) method introduced by Arena et al 1 (WBCT-CMA) and was therefore called the Modified WBCT-CMA. CubeVue software (version 3.9.195; CurveBeam AI LLC, 2024) was used for the Modified WBCT-CMA analysis. According to the WBCT-CMA, 1 a coronal cut was chosen based on the widest tibial diaphyseal distance at the most proximal edge of the image to place the proximal circle, with a clear distal tibial plafond presented in the same cut for creating the distal circle. However, the authors of this study have found that this image often cannot be ensured in one coronal cut to include both the widest tibial diaphysis and the distal tibial plafond. (Figure 1). Therefore, the Modified WBCT-CMA used a 3D reconstructed full tibia including all slices in the coronal plane to provide the widest proximal tibial diaphysis and the intact tibial plafond. The proximal and distal circles were then placed.
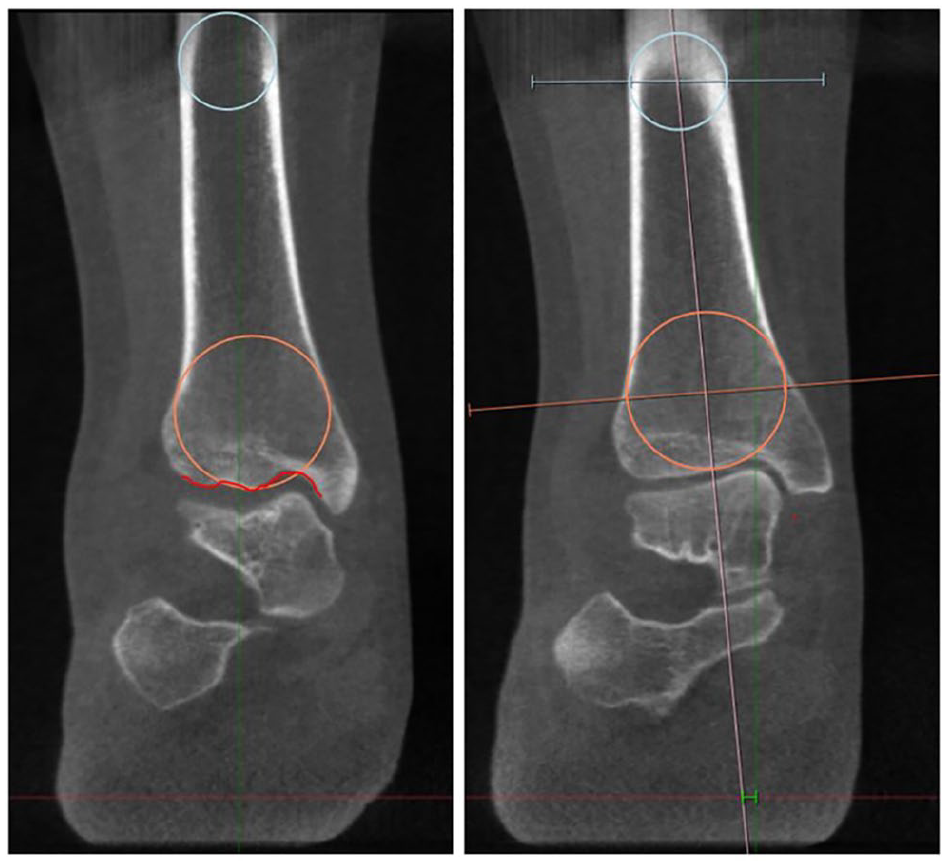
In using the WBCT-CMA method, the image on the left can include the widest tibial diaphysis proximally, but not the tibia plafond, whereas the image on the right includes the tibia plafond but not the widest tibial diaphysis. CMA, Calcaneal Moment Arm; WBCT, weightbearing computed tomography.
The remaining steps were similar to the WBCT-CMA. A line was extended across the centers of both the proximal and distal circles to the most inferior portion of the image to represent the tibial axis. The most inferior aspect of the calcaneus was identified on the axial cut visualized in the transverse plane and was relocated to the coronal cut using the intersection of axial lines. A line parallel to the ground was drawn between the calcaneus weightbearing point and the extension of the tibial axis to measure the Modified WBCT-CMA (Figure 2A).
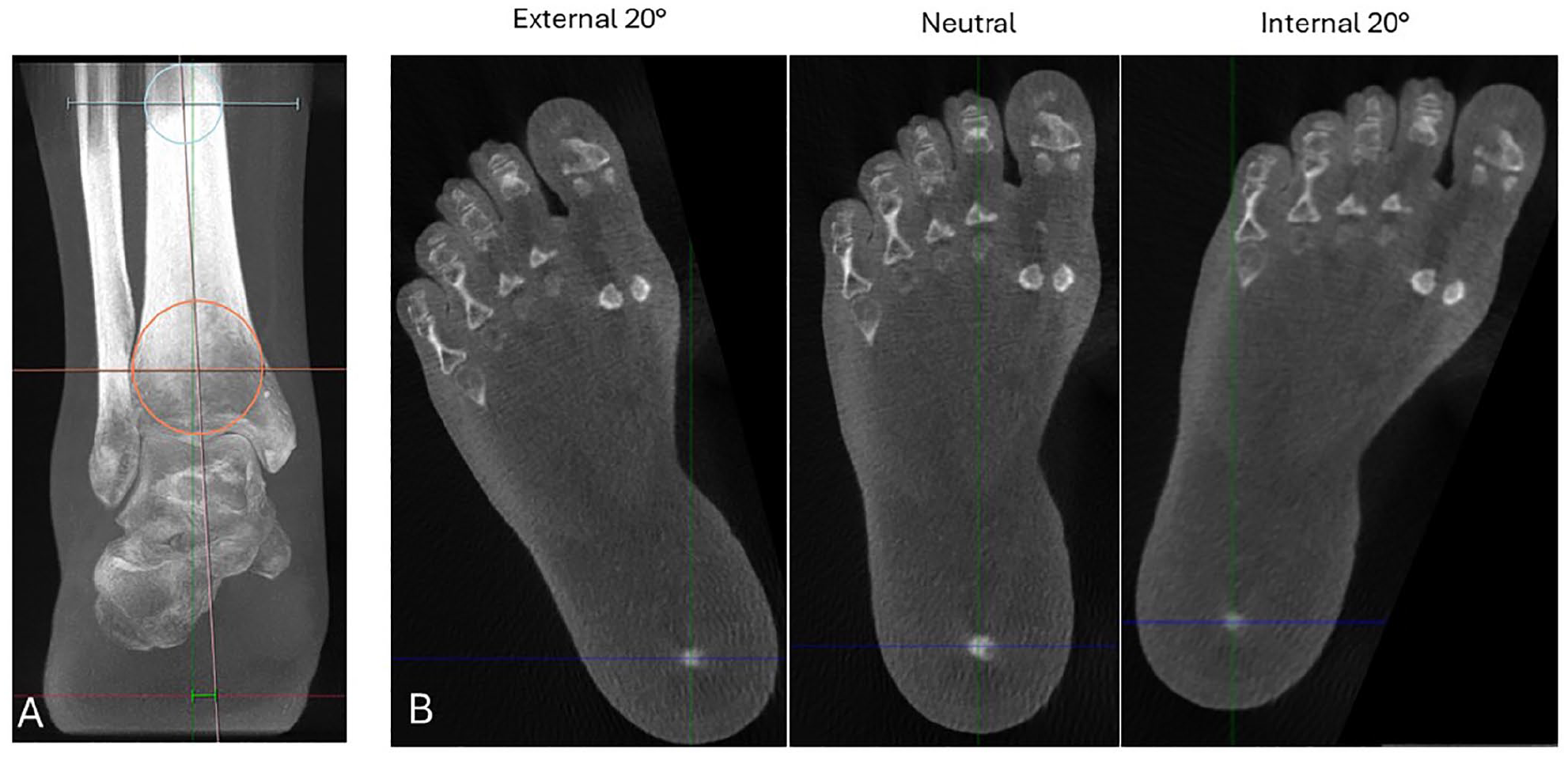
(A) How is the Calcaneal Moment Arm (CMA) value measured in the neutral position using the Modified WBCT-CMA method. (B) The foot is aligned to neutral, then rotated to 20 degrees externally and internally. WBCT, weightbearing computed tomography.
To simulate malposition of the WBCT image, the transverse scans were first used to create a 3D reconstructed foot. A straight line connecting the center of the second metatarsal head and the center of the heel was used to define the neutral orientation of the foot. The foot was then rotated in the transverse plane 5, 10, 15, and 20 degrees both externally and internally (Figure 2B) and the Modified WBCT-CMA was measured in each rotated position. Measurements were recorded in millimeters, rounded to 2 decimal places. A varus alignment was recorded as a negative value, and a valgus alignment was recorded as a positive value. The CMA for each image position was measured twice by 2 independent experienced foot and ankle surgeons.
Statistical Analysis
An intraclass correlation coefficient (ICC) model was used to assess the intraobserver and interobserver reliability of CMA values. ICC reliability values were interpreted as follows: <0.50, poor; 0.5 to 0.75, moderate; 0.75 to 0.9, good; and >0.90, excellent. 11 A linear regression model was used to analyze the relationship between the CMA values and the rotation angles. A simple linear regression analysis was performed with the rotation angle as the independent variable, and CMA value as the dependent outcome. The correlation coefficient between rotation angles and CMA values was evaluated based on the R2 value. R2 of 0.5 to 0.7 indicated a moderate correlation, and R2 >0.7 indicated a strong correlation. 13 We also compared the average difference between the WBCT-CMA and the Modified WBCT-CMA in the neutral (0 degrees) position. 17 Statistical analysis was completed using Microsoft Excel (Microsoft, 2024) and SAS Studio (SAS Institute Inc, Cary, NC). A P value <.05 was considered to indicate statistical significance.
Results
The Modified WBCT-CMA measurements had excellent intraobserver (ICC = 0.97) and interobserver reliabilities (ICC = 0.94) (Tables 1 and 2). External rotation changed a neutral hindfoot into varus, and internal rotation changed a neutral hindfoot into valgus (Figure 3). A linear correlation was detected between the Modified WBCT-CMA values and the rotation angles. A 1-degree internal or external rotation of the image correlated with a 0.48-mm (±0.03) increase or decrease in the Modified WBCT-CMA value (P < .0001, R2 = 0.6406) (Figure 4). The average difference between the WBCT-CMA and the Modified WBCT-CMA in the neutral (0 degrees) position was 0.003 mm, statistically insignificant (P = .99).17,18
Modified WBCT-CMA Values as Measured by 2 Independent Observers. a

Abbreviations: CMA, Calcaneal Moment Arm; OB, observer; WBCT, weightbearing computed tomography.
All measurement units were recorded in millimeters.
In the neutral position, the measurement was repeated twice by each measurer to calculate the intraobserver reliability.
Intraobserver and Interobserver Reliabilities of the Modified WBCT-CMA.

Abbreviations: CMA, Calcaneal Moment Arm; ICC, intraclass correlation coefficient; OB, observer; WBCT, weightbearing computed tomography.
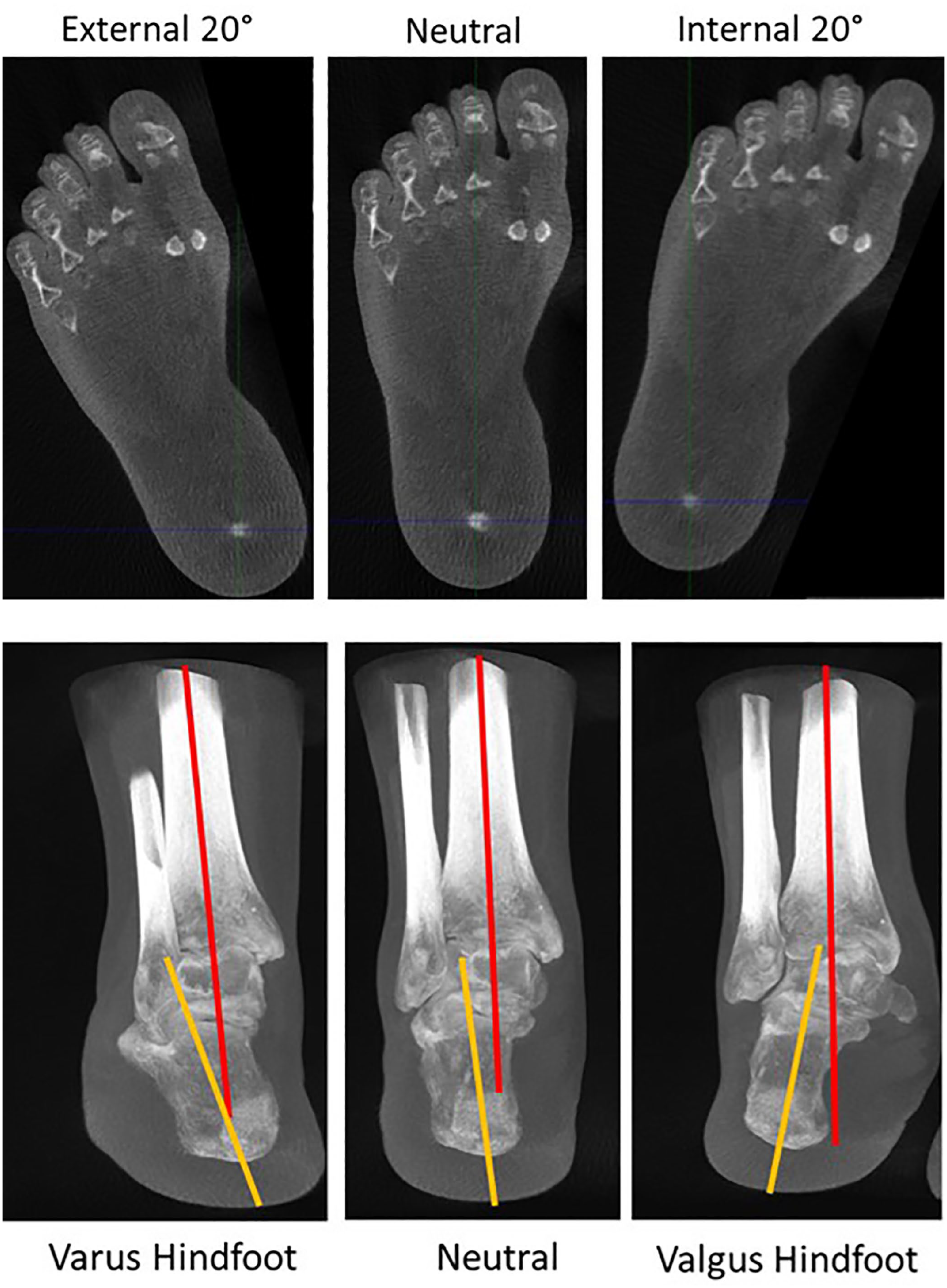
After 20 degrees of external rotation, a neutral hindfoot turns into a varus hindfoot, whereas after 20 degrees of internal rotation, a neutral hindfoot turns into a valgus hindfoot.
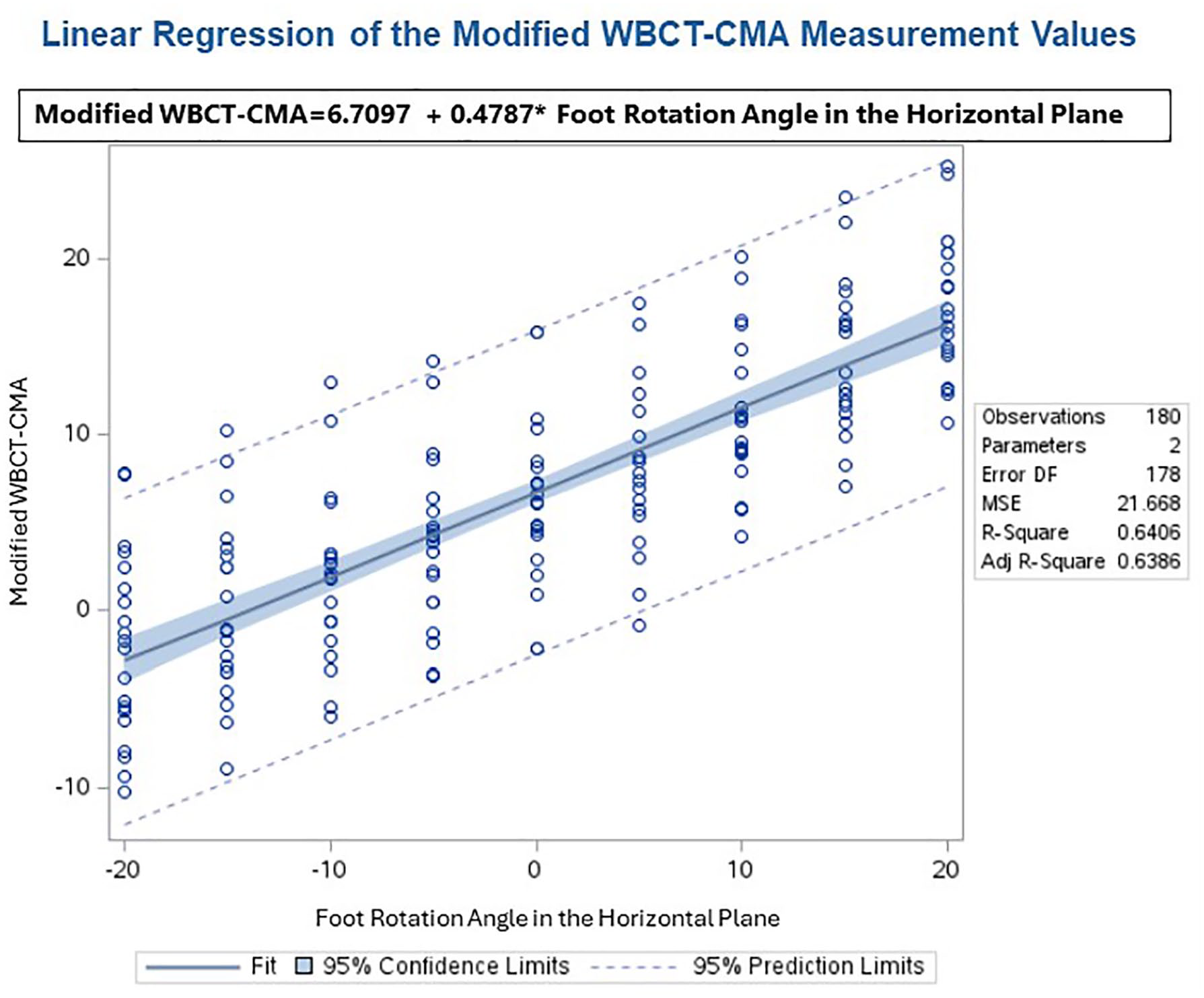
The linear correlation between the Modified WBCT-CMA value and the degree of the rotation of the WBCT image. CMA, Calcaneal Moment Arm; WBCT, weightbearing computed tomography.
Discussion
Buck et al 5 proved that foot rotation had a significant impact on the radiographic hindfoot alignment, and this current study demonstrated a similar issue with WBCT. Although WBCT scans provide 3D information, current methods of hindfoot alignment evaluation are based on 2D concepts. With the limitations of 2D measurement, one needs to ensure that when evaluating the WBCT the image of the foot is positioned consistently. Currently, when taking WBCT, patients are instructed to position the long axis of the foot along reference lines on the weightbearing plate of the scanner. However, if there is a rigid deformity in either the foot or the ankle, the patient will not be able to position the foot in this standardized position and the WBCT images need to be adjusted to determine the hindfoot alignment. However, this consistent orientation of the WBCT image may not exist, because it needs to be defined differently in different conditions including the rigidity of the foot, the alignment of the hip and knee, and abduction/adduction of the midfoot.
This study demonstrated the necessity for correct spatial orientation of the images in analyzing WBCT scans and noted a linear correlation to predict the change in CMA when the image is malpositioned.17,18 The Modified WBCT-CMA demonstrated excellent inter- and intraobserver reliability, similar to the original WBCT-CMA.
It should be noted that rotating a 3D WBCT image is a completely different concept than rotation of the foot during the WBCT acquisition. The latter was not the goal of this study. However, an in vivo pilot study has demonstrated differences in the hindfoot alignment when changing the foot from the position requested by the radiography technician to a natural standing position 19
This study has limitations: the neutral alignment used in the study was defined by the center of the second metatarsal head and the heel, which did not take into consideration the influence of midfoot abduction or adduction. However, this has never been previously studied, and there is no reference for hindfoot alignment when midfoot abduction or adduction is present. This study was performed on WBCT images of normal feet but may have clinical relevance when applied to deformities.
Conclusions
Using the current 2-dimensional methodology to evaluate hindfoot alignment on WBCT, positioning the image in the correct orientation is important. Improper image positioning can change a neutral hindfoot into valgus or varus on the hindfoot measurements and may bias clinical decision-making. This study continues our increasing understanding of the challenges with measuring 3D hindfoot alignment by 2D measurements, even if done with WBCT rather than standard radiographs.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007241286889 – Supplemental material for Different Positions of Weightbearing CT Images Can Influence the Hindfoot Alignment Evaluation Using 2-Dimensional Methodology
Supplemental material, sj-pdf-1-fai-10.1177_10711007241286889 for Different Positions of Weightbearing CT Images Can Influence the Hindfoot Alignment Evaluation Using 2-Dimensional Methodology by Mingjie Zhu, Wanjun Gu, Chao Wang, Songmin Sun, Sera Sempson, Mingzhu Zhang, Kenneth J. Hunt, Mark S. Myerson and Shuyuan Li in Foot & Ankle International
Footnotes
Ethical Approval
Ethical approval for this study was waived by Colorado Multiple Institutional Review Board (21-4067) under category 4.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.