
Abstract
Background:
Metatarsophalangeal (MTP) arthrodesis is the gold standard for treatment of end-stage degeneration or severe hallux valgus deformities. Traditional fixation uses stainless steel or titanium plates, often with a crossing screw. Nitinol, a superelastic nickel-titanium alloy, offers dynamic compression. Nevertheless, it is unknown how nitinol implantation in the context of first-MTP arthrodesis performs biomechanically. We hypothesized that nitinol constructs would demonstrate biomechanical performance comparable or superior to a traditional plate-and-screw construct.
Methods:
Twelve pairs of cadaveric metatarsophalangeal joints were organized into 3 groups according to a balanced incomplete block design: (1) a traditional titanium plate and cross-screw (PS) construct, (2) a nitinol staple and cross screw (NSS) construct, and (3) a proprietary nitinol hybrid screw (NHS) construct. The PS construct consisted of a plate with a compression cross screw; the NSS construct consisted of a nitinol staple with a compression cross screw; and the NHS construct consisted of a hybrid nitinol staple with a compression cross screw. Each specimen was cyclically loaded over 100 cycles at 1 Hz from 20 to 90 N followed by failure testing. A high-definition camera recorded gapping. Failure load, deflection, and stiffness were recorded.
Results:
Compared with the PS construct, both nitinol constructs (NSS and NHS) demonstrated significantly higher failure loads (NSS: 196 ± 101 N, P = .011; NHS: 161 ± 45 N, P = .045), greater stiffness (NSS: 33 ± 15 N/mm, P = .012; NHS: 29 ± 12 N/mm, P = .042), reduced deflection after cyclic loading (NSS: 6 ± 3 mm, P = .047; NHS: 7 ± 3 mm, P = .048), and decreased gapping at failure (NSS: 1 ± 1 mm, P = .003; NHS: 2 ± 1 mm, P = .008). No significant differences were observed between NSS and NHS.
Conclusion:
Nitinol constructs for MTP arthrodesis demonstrated superior mechanical performance compared with a traditional plate-and-screw construct, with higher failure load and stiffness.
Clinical Relevance:
These results support the growing use of nitinol for joint fusion, highlighting its potential to improve load to failure and reduce displacement under cyclic loading.
Introduction
The first metatarsophalangeal (MTP) joint is a common source of debilitating pain for patients and can markedly restrict comfortable ambulation.3,9,11 There are several etiologies for this problem, including hallux rigidus or failed motion-sparing procedures.6,8,9,11,12,16,17 In these situations, MTP arthrodesis is the gold standard, offering relief from pain and restoration of proper ambulation.3,7,9 Over the past several decades, multiple fixation techniques have been thoroughly investigated, both from a clinical perspective and through biomechanical studies, all of which have consistently demonstrated union rates exceeding 90%.3,6-9,11-13,17,18
Traditionally, surgeons have instrumented an MTP arthrodesis with screws and/or plates made of stainless steel or a titanium alloy Ti6Al4V.11,20 These devices function by providing static compression at the arthrodesis site, with the highest level of compression being achieved at the time of implant insertion. 11 This is a critical clinical concern, as stress relaxation in bone or bone resorption at the arthrodesis site can result in loss of compression and an increased risk of nonunion.15,21
An alternative approach involves the use of nitinol, a nickel-titanium alloy, in the form of nitinol staples, compressive discs, and plate fixation constructs (Figure 1B). Nitinol offers dynamic compression because of its unique material properties, particularly superelasticity and shape memory.1,10 These properties allow nitinol implants to recover lost compression secondary to gap formation due to bone resorption, which is not possible with conventional static fixation constructs such as plates and screws.1,10 Furthermore, nitinol staples, when used in isolation, uniquely compress arthrodesis surfaces without traversing the fusion interface, thereby maximizing the total contact area.1,10 Nitinol implants are characterized by their ease of insertion (reducing surgical time) and their compact size compared with commonly used dorsal compression plates, potentially decreasing the risk of symptomatic hardware.5,14 Despite the potential advantages associated with nitinol implants, comprehensive biomechanical data to support its use in MTP arthrodesis remain limited.5,19
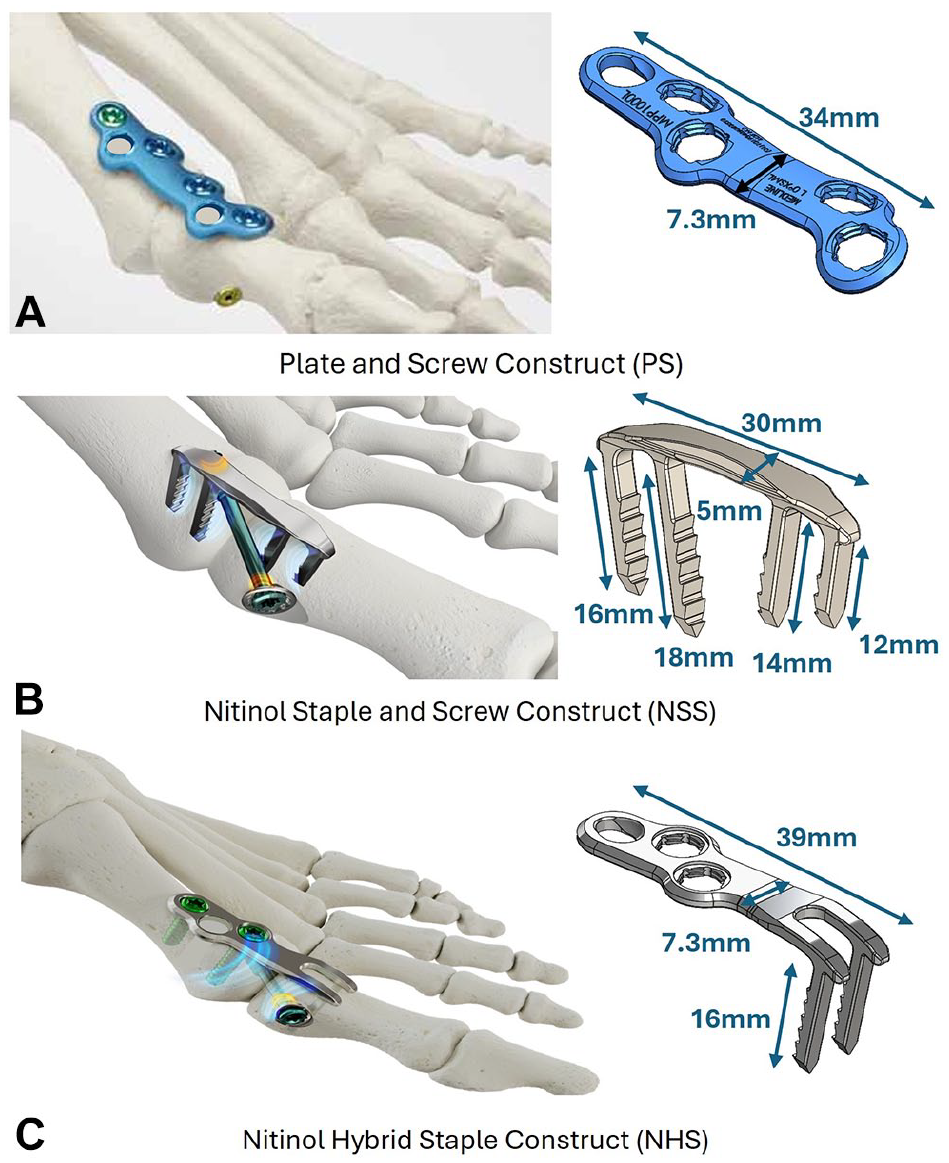
Surgical techniques and dimensions: (A) Plate-and-screw (PS) construct, (B) nitinol staple and screw (NSS) construct, and (C) nitinol hybrid staple (NHS) construct.
A prior 2022 biomechanical cadaveric study investigated 2 nitinol staple constructs: 2 orthogonal nitinol staples and a singular dorsal nitinol staple with cross screws. 20 Both constructs in this study used 2-prong nitinol staples. The study found that both constructs permitted significant motion at the first MTP joint during simulated weightbearing, which the authors extrapolated could lead to clinical failure with early postoperative weightbearing. Because of this, the authors of the current study opted to use a 4-prong staple construct. The prior study also showed that the orthogonal staple construct failed with significantly fewer cycles of load with respect to the staple with cross-screw construct. Therefore, the authors of the current study opted to use a cross-screw in all constructs, aiming to elucidate the strongest biomechanical combination.
The objective of this study is to compare the failure load, stiffness, deflection at failure, deflection after cyclic loading, and gapping at failure between 3 MTP arthrodesis constructs: (1) a traditional PS construct (Figure 1A), (2) a 4-prong NSS construct (Figure 1B), and (3) a proprietary NHS construct (Figure 1C). It was hypothesized that failure load, stiffness, deflection at failure, deflection after cyclic loading, and gapping at failure of the nitinol construct implants will not be significantly different from a traditional plate-and-screw construct when subjected to cantilever loading.
Materials and Methods
Specimen Preparation
Twelve matched pairs of fresh frozen cadaveric human feet (mean donor age: 55.6 years; range 42-65; 10 males and 2 females) were acquired for the study. Institutional review board approval was unnecessary because the tissues were donated for research use, and no genetic information was used. Specimens were excluded based on age <18 years or >65 years, body mass index <18 or >35, and a history of degenerative joint disease, osteoarthritis, other joint pathology, osteoporosis, prior MTP surgery, or metastatic cancer. The specimens were thawed for 24 hours before dissection and testing. Each specimen was exposed using a standard dorsomedial approach, and a fellowship-trained foot and ankle orthopaedic surgeon performed either a PS construct, a NSS construct, or a NHS construct. Following surgical intervention, the first ray was dissected away from all soft tissue attachments, leaving only the skeletal aspects of the MTP joint. Specimens were then potted 3 cm proximal to the MTP joint along its longitudinal axis into a cylindrical mold that was filled with polymethylmethacrylate (PMMA), and 2 pins mounted with black spheres were placed into the phalanx and first metatarsal such that the pin-to-pin axis was parallel to the longitudinal axis of the bone.
Study Design
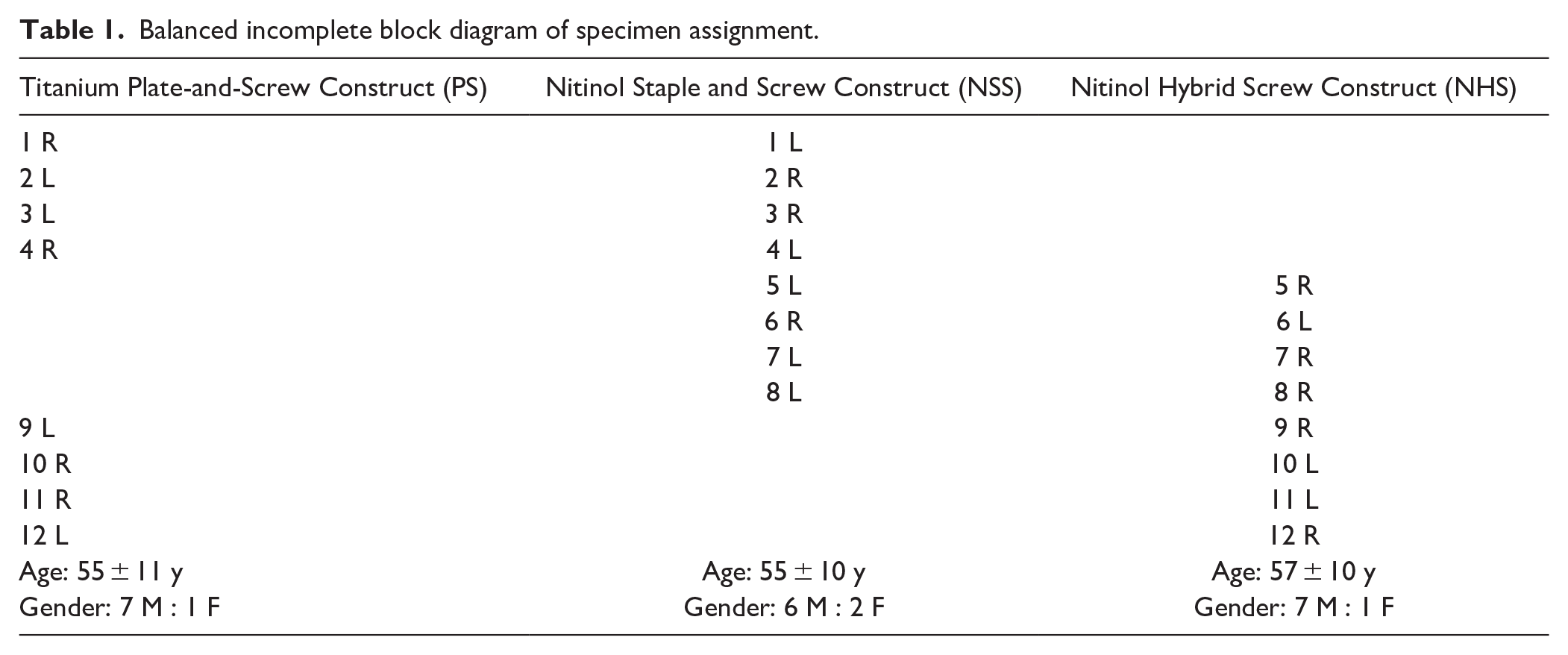
The specimens were organized into 3 testing groups (PS, NSS, and NHS constructs) according to a balanced incomplete block design (BIBD) as shown in Table 1. A BIBD design minimizes interspecimen variability by leveraging paired specimen similarity. Additionally, BIBD is an optimal efficiency design in the case of 3 treatments distributed across matched pairs.
Balanced incomplete block diagram of specimen assignment.
Surgical Techniques
Each cadaver was prepared and instrumented by a team consisting of a fellowship-trained foot and ankle orthopaedic surgeon and an assisting fellow. The joint was exposed through a standard dorsal capsulotomy, preserving the plantar attachments of the collateral ligaments and plantar plate. A 1.6-mm Kirschner (K)-wire was placed through the center of the metatarsal shaft and proximal phalanx with fluoroscopic guidance. Cannulated, powered hemispherical reamers were used to remove cartilage from the metatarsal head and base of the proximal phalanx. Each specimen was then held reduced in a simulated position for first MTP arthrodesis at approximately 15 degrees of dorsiflexion and 10 degrees of valgus. This position was then stabilized with an oblique K-wire.
Plate-and-Screw Construct
A 1.4 mm K-wire was placed from distal medial to proximal lateral across the first MTP joint, and appropriate position was confirmed with fluoroscopy. The wire was measured and overdrilled, and an appropriately sized 4-mm partially threaded cannulated headed compression screw with a washer was placed, compressing the joint in an oblique fashion. A precontoured extra-small 0-degree first MTP plate (Medline UNITE, Northfield, IL) was placed on the dorsal joint. It was fixed with a 3.5-mm nonlocking cortical screw (Medline UNITE, Northfield IL) in the proximal phalanx followed by an adjacent locking screw. In the proximal part of the plate, a 3.5-mm nonlocking cortical screw (Medline UNITE) was placed in the slot hole in compression mode. An additional adjacent locking screw was placed. Screw placement and plate size was intentionally chosen to match the size and prong spacing of a 4-prong nitinol staple. Fluoroscopic images were taken to ensure that the hardware matched acceptable clinical fixation constructs.
Nitinol Staple and Screw Construct
A nitinol staple guide (Medline UNITE) was positioned by fluoroscopy and drilled, using temporary pins to ensure that all holes were parallel. Using the manufacturer instrumentation, a guidewire for a 4-mm cross screw was placed. Then a 4-prong nitinol staple (Medline UNITE) was impacted onto the dorsal joint. Following this, the cross-screw guidewire was measured, overdrilled, and an appropriately sized 4-mm partially threaded cannulated headed compression screw with a precontoured nitinol compressive disc (Medline UNITE) was placed.
Nitinol Hybrid Screw Construct
A 1.4-mm K-wire was placed to provisionally position the MTP joint. A template guide for the implant was appropriately sized, positioned under fluoroscopy, and secured using temporary fixation pins. A 2.8-mm drill bit was used to drill holes through the staple portion of the template and a 2.8-mm locator pin was placed in each hole. The template was removed. The nitinol staple (Medline UNITE) was stretched following manufacturer guidelines with the supplied instrumentation. The implant staple tines were then impacted into the proximal phalanx. Subsequently, a nonlocking screw was placed in the slot hole of the nitinol staple in compression mode. An adjacent locking screw was placed in the proximal aspect of the staple. Following this, an appropriately sized 4-mm partially threaded cannulated headed compression screw was placed with a precontoured nitinol disc (Figure 1).
Biomechanical Testing Protocol
The specimens were mounted to the base of a dynamic tensile system (Instron ElectroPuls E10000; Instron, Norwood, MA) such that the specimen was oriented in 10 degrees of plantar flexion with the plantar surface facing up 7 (Figure 2). A high-definition video camera (ILCE-6300; Sony Corporation, Tokyo, Japan) was positioned perpendicular to the specimen to track the relative position of the pins in the sagittal plane during testing. A 20-N compression preload was applied to the specimen, and the initial position of the end effector was recorded. To evaluate cyclic mechanical behavior and failure behavior of each technique, each specimen was subjected to a limited cyclic loading protocol that simulated load magnitudes experienced during physiologic walking in a short leg walking cast, with the ventral phalanx cyclically loaded from 20 to 90 N at 1 Hz for 100 cycles.2,4,11,22 The applied load was then decreased to 20 N, and the position of the end effector of the materials testing machine was recorded. After cyclic loading, the specimens were pushed to failure at 1 mm/s. Failure was defined as an acute reduction in load under this continual axial displacement or ventral joint gapping over 7 mm. 7 The resulting force-displacement curve was recorded.
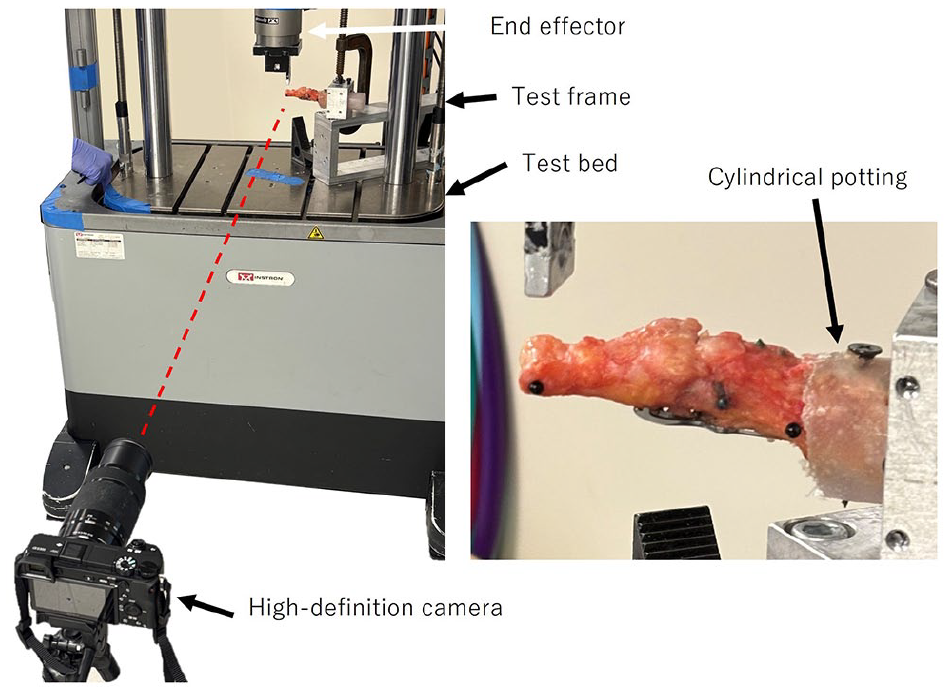
Biomechanical testing setup with representative specimen repaired with nitinol hybrid screw construct.
Ultimate failure load and mode of failure were recorded. Deflection after cyclic loading was calculated as the difference in the end effector’s initial position and its position after 100 cycles. Deflection at failure was calculated as the difference in the end effector’s initial position and its position at the point of failure. Construct stiffness was determined as the slope of the linear region of the force-displacement data. Joint gapping at failure was the difference in distance in the sagittal plane between a fiducial on the ventral side of the phalanx to a point on the ventral side of the metatarsal from the initial loading point to the time of failure. The locations of the pins relative to the ventral side of the MTP joint were measured with calipers, and a custom image recognition script (MATLAB, version R2023, The MathWorks Inc, Natick, MA) calculated the distance between the 2 ventral points from the locations of the pins. (Deflection values represent the total displacement measured at the fixture level and include both joint movement and system compliance.)
Statistical Analysis
Statistical power was considered based on our fixed sample size and the BIBD. Analysis of variance (ANOVA) for a BIBD achieves a statistical efficiency between that of a randomized complete block design and an independent samples ANOVA. Based on preliminary testing and assuming 8 specimens per group (12 pairs, 24 specimens in total), 2-tailed hypothesis testing, and an alpha level of .05, the sample size was sufficient to detect a minimum detectable difference in failure load of 29 N (d = 1.1) and a minimum detectable difference in stiffness of 5 N/mm between groups with 80% statistical power.
All statistical analysis was performed by a designated team member who was not involved in the surgical procedures with the statistical package R version 4.0.0 (R Development Core Team, Vienna, Austria, with the additional packages ibd and emmeans). Differences in mean ultimate failure load, deflection after cyclic loading, deflection at failure, stiffness, and gapping at failure between the PS, NSS, and NHS constructs were analyzed with an ANOVA corresponding to the BIBD (Table 1). To address the primary hypotheses of the study and to account for multiple comparisons, pairwise group comparisons were made among the estimated marginal means (EM Means) with the Tukey method. A P value <.05 was considered statistically significant. The study was not powered for formal equivalence testing between nitinol groups, and such interpretations should be limited accordingly. All statistical analysis was performed by staff scientists and only revealed to the treating surgeon on completion.
Results
Ultimate Failure Load and Failure Mode
Representations of the loading protocol can be found in Figure 3. Graphical display of the ultimate failure load data can be found in Figure 4. All specimens failed because of an acute reduction in load under continual axial displacement. No specimens failed because of ventral joint gapping exceeding 7 mm. The NSS construct (196 ± 101 N) and the NHS construct (161 ± 45 N) exhibited significantly higher ultimate failure load (NSS: P = .011; NHS: P = .045) than the standard PS construct (PS: 113 ± 61 N). NSS and NHS constructs showed no significant difference in failure load.

Loading protocol, including the cyclic loading and load-to-failure steps, for representative specimens of each repair construct.
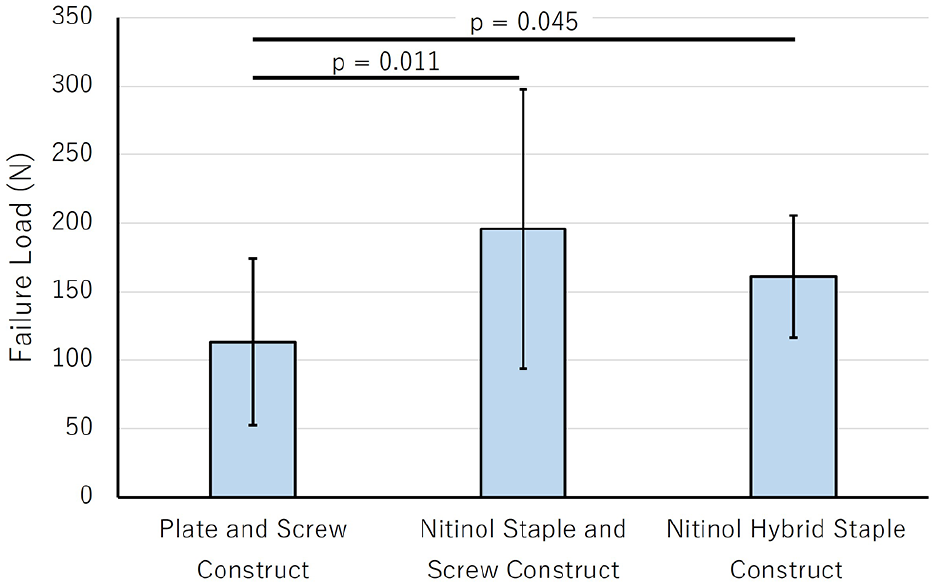
Ultimate failure load for the PS (plate-and-screw) construct, the NSS (nitinol staple and screw) construct, and the NHS (nitinol hybrid screw construct).
Stiffness
Graphical display of the stiffness data can be found in Figure 5. The NSS (33 ± 15 N/mm) and NHS (29 ± 12 N/mm) constructs exhibited significantly higher stiffness (NSS: P = .012; NHS: P = .042) than the PS construct (15 ± 8 N/mm). Stiffness of the NSS and NHS construct showed no statistically significant difference, although the study was not powered for formal equivalence testing.
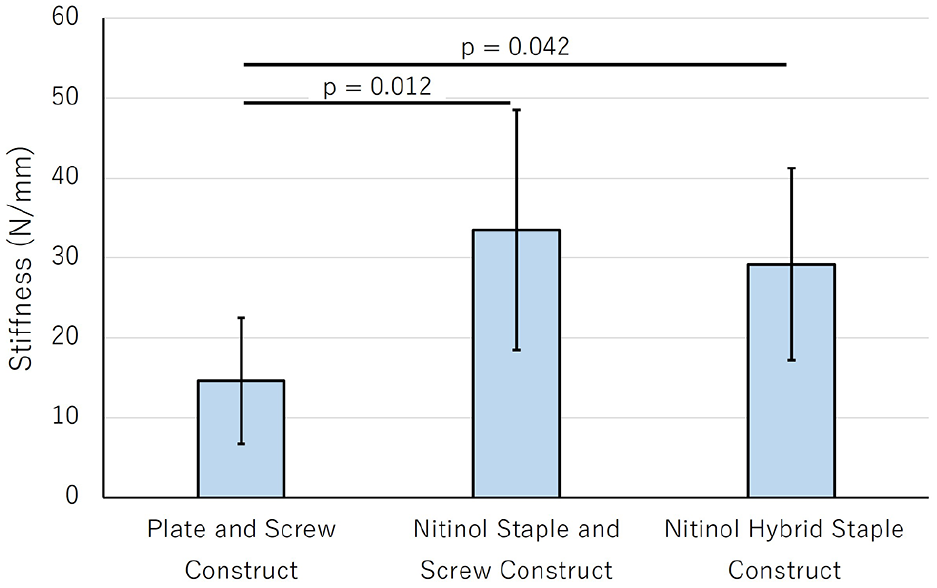
Stiffness for the plate-and-screw construct (PS), the nitinol staple and screw construct (NSS), and the nitinol hybrid staple construct (NHS).
Deflection After Cyclic Loading
Graphical display of the deflection after cyclic loading data can be found in Figure 6. The NSS construct (6 ± 3 mm) and the NHS construct (7 ± 3 mm) exhibited significantly reduced deflection after cyclic loading (NSS: P = .047; NHS: P = .048) than the PS construct (10 ± 6 mm). Deflection after cyclic loading of the NSS construct and the NHS construct were not significantly different from each other although the study was not powered for formal equivalence testing. (Deflection values represent total displacement measured at the fixture level and include both joint movement and system compliance.)
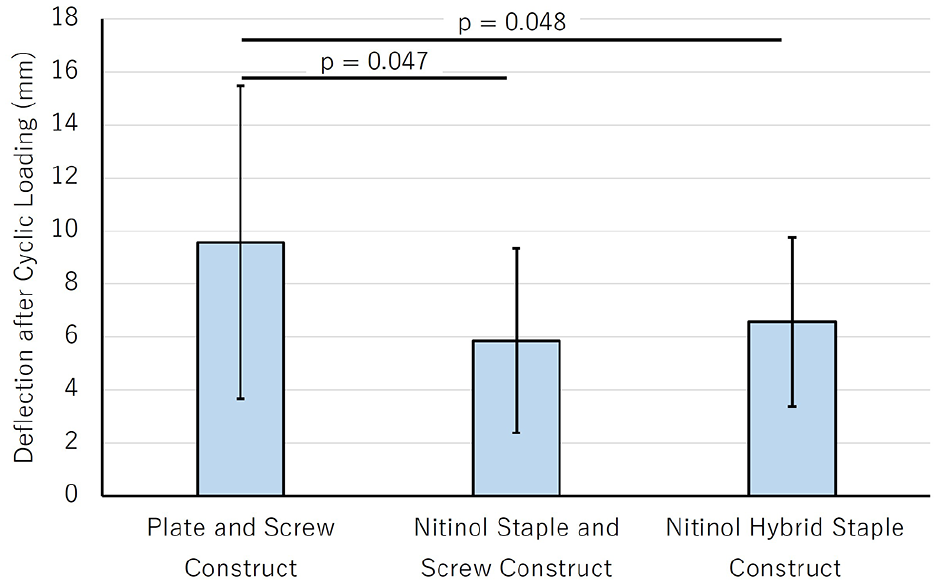
Deflection after cyclic loading for the plate-and-screw construct (PS), the nitinol staple and screw construct (NSS), and the nitinol hybrid staple construct (NHS).
Deflection at Failure
Graphical display of the deflection at failure can be found in Figure 7. There was no difference in deflection at failure between the PS construct (17 ± 7 mm) and the NSS construct (15 ± 5 mm, P = .71), the PS construct and the NHS construct (12 ± 3 mm, P = .81), and the NSS construct and the NHS construct (P = .90).
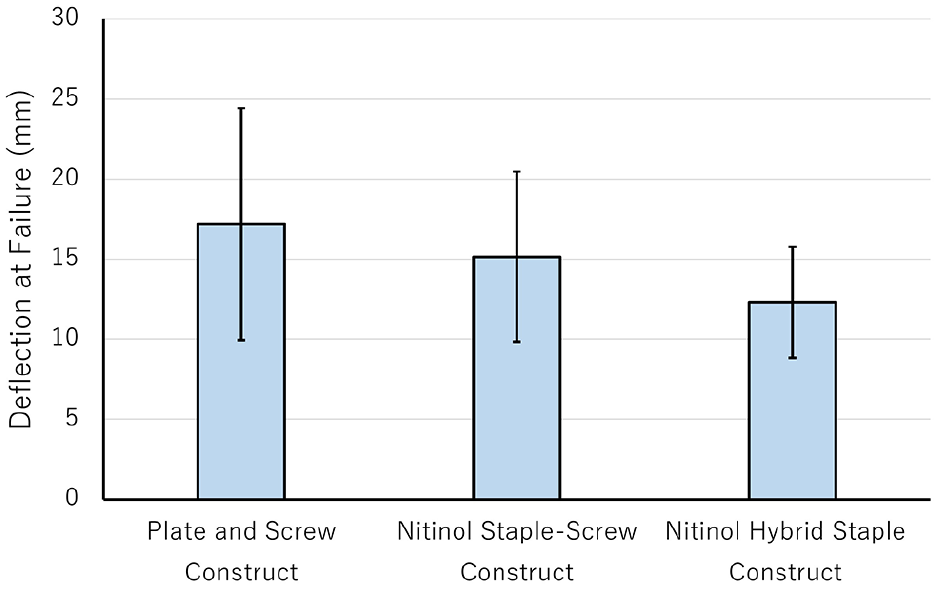
Deflection at failure for the plate-and-screw construct (PS), the nitinol staple and screw construct (NSS), and the nitinol hybrid staple construct (NHS). There was no significant difference in deflection at failure between repairs.
Modes of Failure
No construct failed during cyclic loading. A list of modes of failure for all specimens can be found in Table 2. Bone failure occurred in all specimens. The most common modes of failure in the PS construct group were metatarsal fracture at proximal plate in 3 specimens (38%) and metatarsal fracture at the cannulated headed compression cross screw in 2 specimens (25%). The most common modes of failure in the NSS construct group were cross screw pull-through in 5 specimens (63%), defined as axial displacement of the cross screw through the bone, and metatarsal fracture at proximal staple in 2 specimens (25%). The most common modes of failure in the NHS construct group were metatarsal fracture at the cross screw in 3 specimens (38%), phalanx fracture at the cross screw insertion site in 2 specimens (25%), and fracture at the interface of the metatarsal and the PMMA in 2 specimens (25%).
Mode of Failure of Every Specimen.
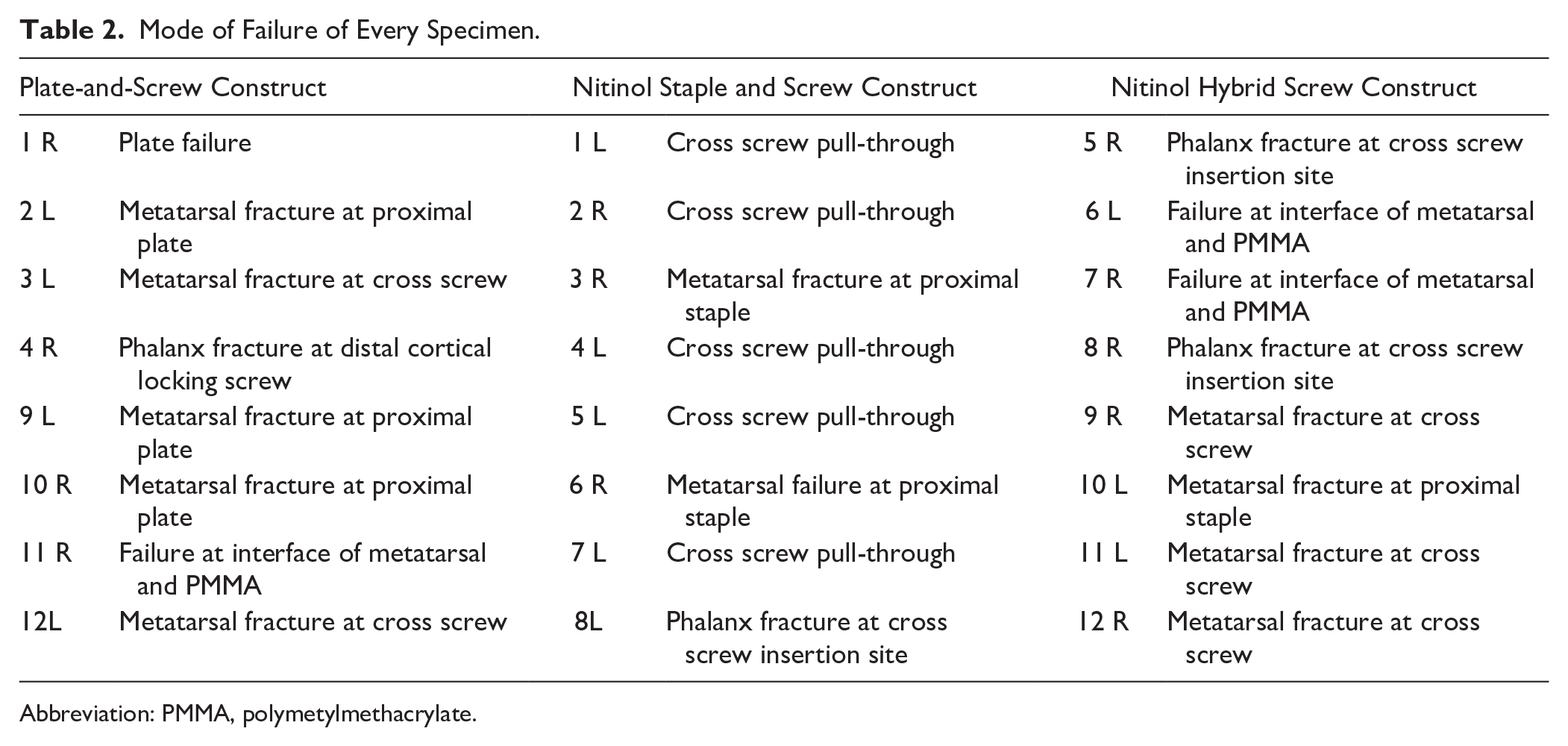
Abbreviation: PMMA, polymetylmethacrylate.
Gapping at Failure
Graphical display of the joint plantar gapping at failure can be found in Figure 8. The NSS construct (NSS: 1 ± 1 mm) and the NHS construct (NHS: 2 ± 1 mm) exhibited significantly reduced gapping at failure (NSS: P = .003; NHS: P = .008) compared with the PS construct (3 ± 1 mm). Plantar gapping at failure of the nitinol staple-screw NSS construct and the NHS construct showed no statistically significant difference, although the study was not powered for formal equivalence testing.
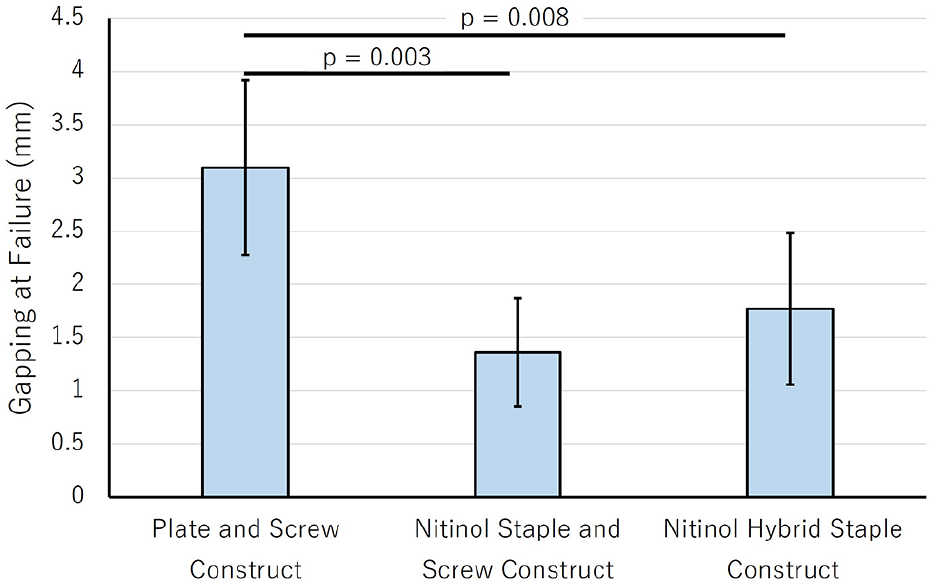
Gapping at failure for the plate-and-screw construct (PS), the nitinol staple and screw construct (NSS), and the nitinol hybrid staple construct (NHS).
Discussion
This study demonstrates that both an construct and a proprietary NHS construct have a higher ultimate failure load and higher stiffness when compared to a standard PS construct. These findings are consistent with our hypothesis and add to a growing body of literature that supports clinical applications of nitinol’s unique material properties of superelasticity and shape memory.1,10
Interestingly, the most common mode of failure differed in each construct group. Both the PS and the NHS constructs demonstrated metatarsal failure at the cross screw, whereas the NSS construct failed via cross screw pull-through. One explanation for this is that the combination of the metatarsal screws and the cross screws in the PS and NHS constructs create metatarsal stress risers. The NSS construct, on the other hand, only includes the cross screw, not the metatarsal screws. Thus, the weakest location of the NSS construct is not the metatarsal bone but rather the bone around the cross screw, resulting in a higher prevalence of cross screw pull-through failure.
Furthermore, the superelasticity of the nitinol implant may explain different load-sharing behavior of the implant and the cross screw between the PS and NHS construct groups. Prior biomechanical literature has emphasized a potential concern in trading off stiffness for flexibility and superelasticity when using nitinol implants. Schafer et al 20 compared 2 orthogonal 2-prong nitinol staples with a 2-prong nitinol staple and screw construct for first MTP arthrodesis, reporting significantly earlier failure in the orthogonal staple group. Ten specimens in the study failed because of excessive gap formation. In the current study, every construct failed not due to excessive gapping but due to bone or implant failure, and the nitinol constructs demonstrated lower gapping when these failures occurred than the PS construct group. In contrast, all constructs in our study failed because of mechanical or bony failure, and the nitinol constructs exhibited significantly less gapping at failure.
This suggests that the superelasticity of the nitinol implants may be transmitting axial load to the cross screw, which, in an NSS construct, results in cross screw pullout, and, in the NHS construct, results in metatarsal fracture. In the PS group, the less elastic plate may allow greater joint gapping prior to failure. It is important to note that nitinol implants come in various shapes and sizes, and many factors affect the biomechanical properties, including thickness, staple bridge width, number of prongs, and prong length. These factors may contribute to how our constructs behaved differently than those in previous biomechanical studies.
Our study has several limitations. First, this was a cadaveric study where a limited cyclic loading protocol was applied to replicate the load magnitudes experienced while walking in a short leg cast. However, use of a walking cast is rare in modern rehabilitation protocols, and 100 cycles of loading represents time-zero cyclic loading and not a full rehabilitation protocol. This was done intentionally to obtain accurate failure load data. Second, this study does not account for any potential biologic healing that would aid in stabilizing the MTP arthrodesis over time. Thirdly, the cyclic loading in this study occurred in 1 plane of motion. We recognize that true motion across this joint is more complex and occurs in multiple planes. Further, although the cross screw and nitinol implant may provide multidirectional stability, rotational stability was not tested in this study. Moreover, the position of the end effector was used to measure cantilever displacement of the construct and includes displacement inherent to the mechanical testing system. This systemic displacement may add uncertainty to the deflection and stiffness outcomes. Finally, this study was highly dependent on the bone quality of the cadaveric specimens. The effects of the variation in specimens were minimized by using matched pairs with a balanced incomplete block design.
Conclusion
This study demonstrates that the 2 distinct nitinol constructs for first MTP arthrodesis had higher ultimate failure load and greater stiffness compared with a traditional plate and cross screw construct. These biomechanical advantages highlight nitinol’s potential role in enhancing joint stability during the early postoperative period.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007251341886 – Supplemental material for Biomechanical Comparison Between Fixation Techniques for First-Metatarsophalangeal Joint Arthrodesis
Supplemental material, sj-pdf-1-fai-10.1177_10711007251341886 for Biomechanical Comparison Between Fixation Techniques for First-Metatarsophalangeal Joint Arthrodesis by Chase M. Romere, Jason P. Sidrak, Justin F. M. Hollenbeck, Kevin A. Schafer, Craig T. Haytmanek and Jonathon D. Backus in Foot & Ankle International
Footnotes
Ethical Approval
Ethical approval was not sought for the present study as cadaveric studies do not fall under the regulatory definition of human subject research and the cadavers were obtained from a company that consents for use in research in the donor application process.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Craig T. Haytmanek Jr, MD, reports general disclosures of consultant and research support from Arthrex and research support from Stryker. Jonathon D. Backus, MD, reports disclosures related to manuscript of $45,000, surgical supplies, and cadavers provided by Medline UNITE for this project; being a consultant and receiving royalties from Medline UNITE; and general disclosures of the scientific advisory board and stock options in Sparta Medical. Disclosure forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Medline Industries (USA-000138).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.