
Abstract
Background:
Chronic plantar fasciitis (CPF) is a prevalent cause of heel pain, often refractory to conservative treatments. Corticosteroid injections (CSIs) are frequently used for symptom relief but may provide only transient benefits and are associated with potential adverse effects. Platelet-rich plasma (PRP) has gained attention as an alternative because of its regenerative properties. This study compares the effectiveness of PRP injections (n = 75) and CSI (n = 77) in reducing pain and improving function over six months in patients with CPF.
Methods:
A retrospective cohort study was conducted on 152 patients diagnosed with CPF who received ultrasound-guided injection therapy at a tertiary university hospital between September 2021 and September 2024. Patients were divided into CSI (n = 77) and PRP injection (n = 75). Pain intensity was measured using the visual analog scale (VAS), and functional status was assessed with the Foot Function Index (FFI). Evaluations were performed at baseline and 1, 3, and 6 months postinjection.
Results:
At baseline, VAS (P = .449) and FFI (P = .462) scores were comparable between groups. At 1 month, no significant differences were found for VAS (P = .368) and FFI (P = .392). At 3 months, VAS (P = .586) and FFI (P = .578) scores remained similar. At 6 months, PRP showed significantly lower VAS scores (1.98 ± 0.35) compared with corticosteroids (2.79 ± 1.13; P < .001); however, the difference did not exceed the MCID threshold (0.9 cm), suggesting limited clinical significance. Conversely, FFI scores improved more in the PRP group (22.3 ± 4.1) than in the corticosteroid group (29.8 ± 5.5; P < .001), exceeding the MCID threshold (7 points), confirming clinical relevance.
Conclusion:
PRP injections were associated with superior 6-month functional improvement over corticosteroids in CPF, with statistically significant gains that met the MCID threshold. Although both treatments were effective in the short term, only functional improvements reached clinical significance. These findings support PRP’s role in providing a modest functional advantage and highlight the need for future trials to optimize injection protocols and assess long-term outcomes.
This is a visual representation of the abstract.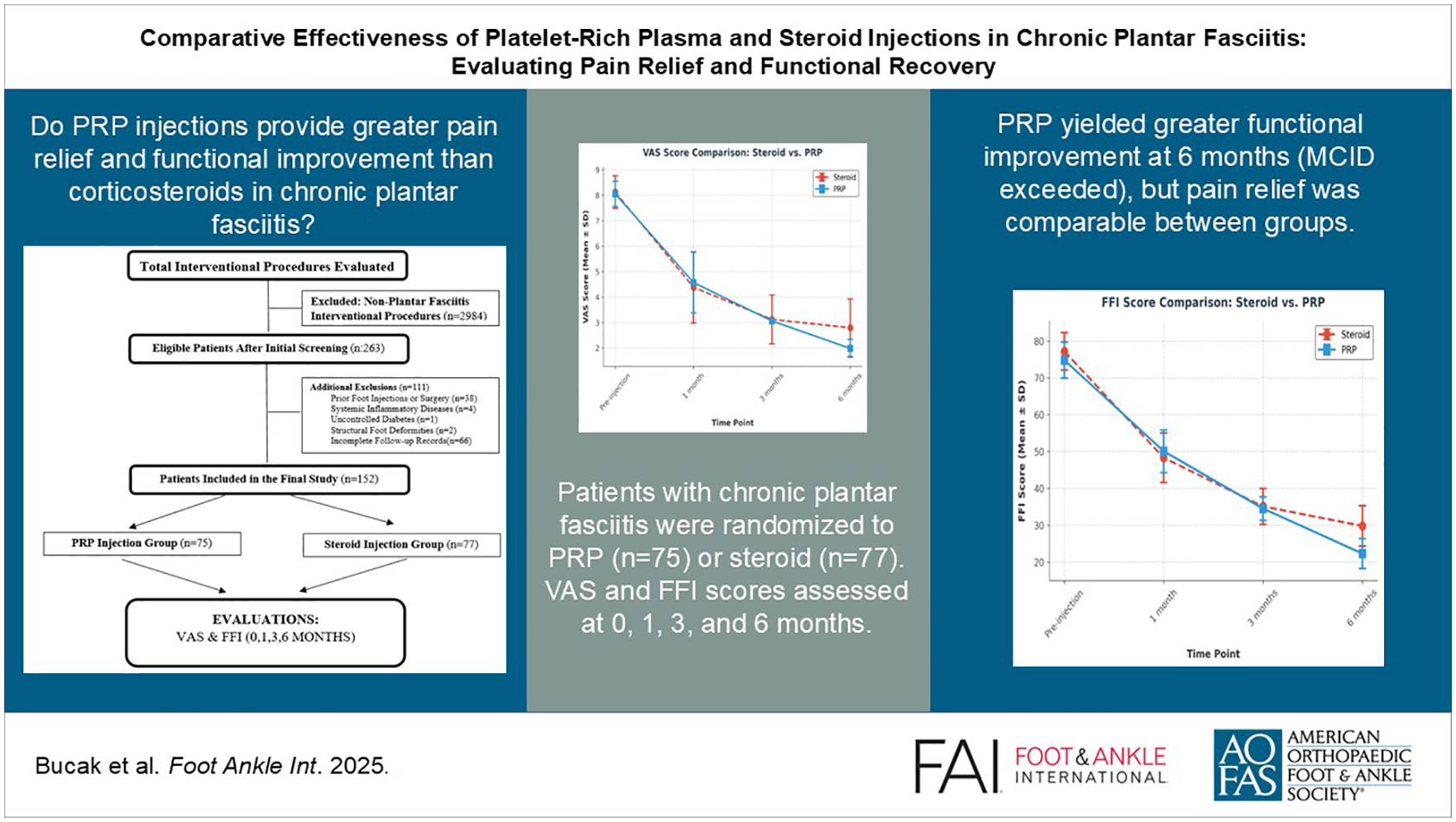
Introduction
Plantar fasciitis (PF) is a common cause of heel pain, affecting up to 10% of individuals in their lifetime.9,38 It is characterized by degeneration and inflammation of the plantar fascia due to anatomical, biomechanical, and chronic conditions. 32 It is more common in women and typically causes medial-inferior heel pain that worsens after inactivity or prolonged weightbearing.20,28 Pain and discomfort associated with plantar fasciitis have been shown to significantly reduce quality of life. 18
Diagnosis is usually based on clinical history and findings of local tenderness. In addition to clinical findings, imaging modalities are frequently used in the diagnosis of plantar fasciitis. Ultrasonographic imaging is not only diagnostic but also valuable in objectively assessing treatment response. 25 It provides a more specific and accurate tool than patient-reported pain scales and potentially aids in treatment adjustments or identification of other sources of pain. 25
Plantar fasciitis is generally considered a self-limiting condition, and approximately 80% to 90% of patients experience significant symptom relief over a period of several months with conservative treatments including nonsteroidal antiinflammatory drugs (NSAIDs), stretching exercises, orthotics, night splints, and physical therapy. 20 However, a proportion of patients may experience persistent symptoms after 6 to 12 months, which may require further interventions. 26 However, previous studies have reported that patients with persistent symptoms lasting 3 months or longer may also benefit from interventional treatments such as corticosteroids (CS) or platelet-rich plasma (PRP) injections, suggesting variability in clinical practice.16,33,35 This highlights the importance of individualized treatment decisions based on symptom severity and patient preference.
Initial management focuses on pain reduction and support of the plantar fascia through antiinflammatory drugs and orthotic support. 20 If symptoms persist for longer than 6 months, minimally invasive procedures such as CS and PRP injections are often considered. 30
Corticosteroid injections (CSIs) provide short-term pain relief by reducing inflammation in refractory plantar fasciitis. Although effective, they can impair tissue repair, leading to complications such as facial rupture, fat pad atrophy, nerve damage, and calcaneal osteomyelitis.2,3,36
PRP, an autologous blood product with a concentrated platelet count, has emerged as a popular treatment for various musculoskeletal conditions, including plantar fasciitis, and is increasingly used for soft tissue injuries like tendinopathies, and degenerative joint diseases such as knee and hip osteoarthritis, either as a primary therapy or postsurgically to augment healing.5,7,8,24,29
Several clinical trials and meta-analyses have demonstrated the potential efficacy of PRP in the treatment of CPF, reporting superior results in pain reduction and functional improvement compared with CSI or placebo.11,14,34
A recent meta-analysis has pointed to the potential superiority of PRP over CSI in pain reduction and functional improvement, while emphasizing the need for standardized treatment protocols and outcome measures.6,11,17 Besides this shortcoming, there is a common belief among clinicians and researchers that statistical significance equals clinical significance. 21 However, statistical significance only refers to the probability that the result of the analysis between 2 treatments is indeed different. Thus, a significant finding only provides us with a degree of confidence that the result is not a chance finding. 31 So in this case, a statistically significant treatment effect does not necessarily indicate an important or clinically meaningful effect for patients. From this perspective, the most effective method of examining the results of a study for clinical significance is to compare them to a prespecified minimal clinically important difference (MCID) for the outcome. 21 The MCID represents the smallest difference in a given area that can be perceived by patients and would justify a change in management in the absence of side effects or excessive costs. 37 Central to clinical research and guideline development, the MCID is often estimated using measures of variability such as standard deviation or standard error.22,27 Well-defined MCID thresholds for visual analog scale (VAS) in chronic pain conditions, including foot and ankle conditions, provide a reference for assessing treatment efficacy. 19 Therefore, direct comparison of PRP and CSI with MCID for CPF is warranted.
This study hypothesizes that ultrasound-guided PRP injections provide longer-lasting pain relief and greater functional improvement, measured respectively by the VAS and the Foot Function Index (FFI), compared with ultrasound-guided CSI in the treatment of CPF. To test this hypothesis, we analyze comprehensive patient data from a specialized foot and ankle clinic at a tertiary university hospital. By assessing the clinical significance of these changes, we aim to interpret the findings not only in terms of statistical significance but also within the context of meaningful clinical improvement.
Materials and Methods
Study Design
This retrospective cohort study was conducted at the Foot and Ankle Outpatient Clinic of tertiary care university hospital, a specialized facility where patients with foot and ankle pathologies have been systematically evaluated and managed since August 2021. As part of a structured clinical registry, all patients undergoing assessment and treatment at this dedicated clinic have been prospectively documented, ensuring comprehensive follow-up and standardized data collection. For this study, eligible patients were identified through a systematic review of outpatient clinical records and electronic hospital database entries. Using a dual-source approach (clinic registry and electronic system cross-referencing) minimized the risk of missed cases and ensured the completeness of patient inclusion.
The medical records of patients diagnosed with CPF were reviewed retrospectively to evaluate treatment outcomes following interventional pain management procedures. The study protocol was reviewed and approved by the local ethics committee in accordance with the Declaration of Helsinki (ethics approval no: 2024-10-30, protocol number: 2024/265).
Patient Selection and Eligibility Criteria
In this retrospective cohort study, the treatment distribution was evaluated based on the data obtained from the patient files kept in detail. Patients included in the study were retrospectively identified from clinical records as individuals who had not responded to first-line conservative treatments and needed further treatment.
Analysis of the patient files showed that treatment decisions were based on evidence-based clinical protocols for CPF management, encompassing standardized ultrasound-guided injection techniques and first-line conservative strategies, and were finalized through patient-physician shared decision-making. It was confirmed from the recorded patient data that patients were informed about the mechanisms of action, expected outcomes, and possible side effects of CS and PRP injections prior to treatment in line with current evidence-based guidelines. The final choice of treatment was based on a combination of patient preference and the clinical judgment of the physician, as demonstrated by retrospective patient file reviews.
A total of 387 patients who underwent interventional pain management procedures for foot and ankle disorders during the designated study period were initially screened. Following a thorough evaluation based on predefined inclusion and exclusion criteria, a final cohort of 152 patients with a confirmed diagnosis of CPF was identified and included in the analysis, as illustrated in Figure 1. These patients had received ultrasound-guided injection therapy as part of their treatment regimen. Of these patients, 77 were assigned to the CS injection group, whereas 75 were included in the PRP injection group.
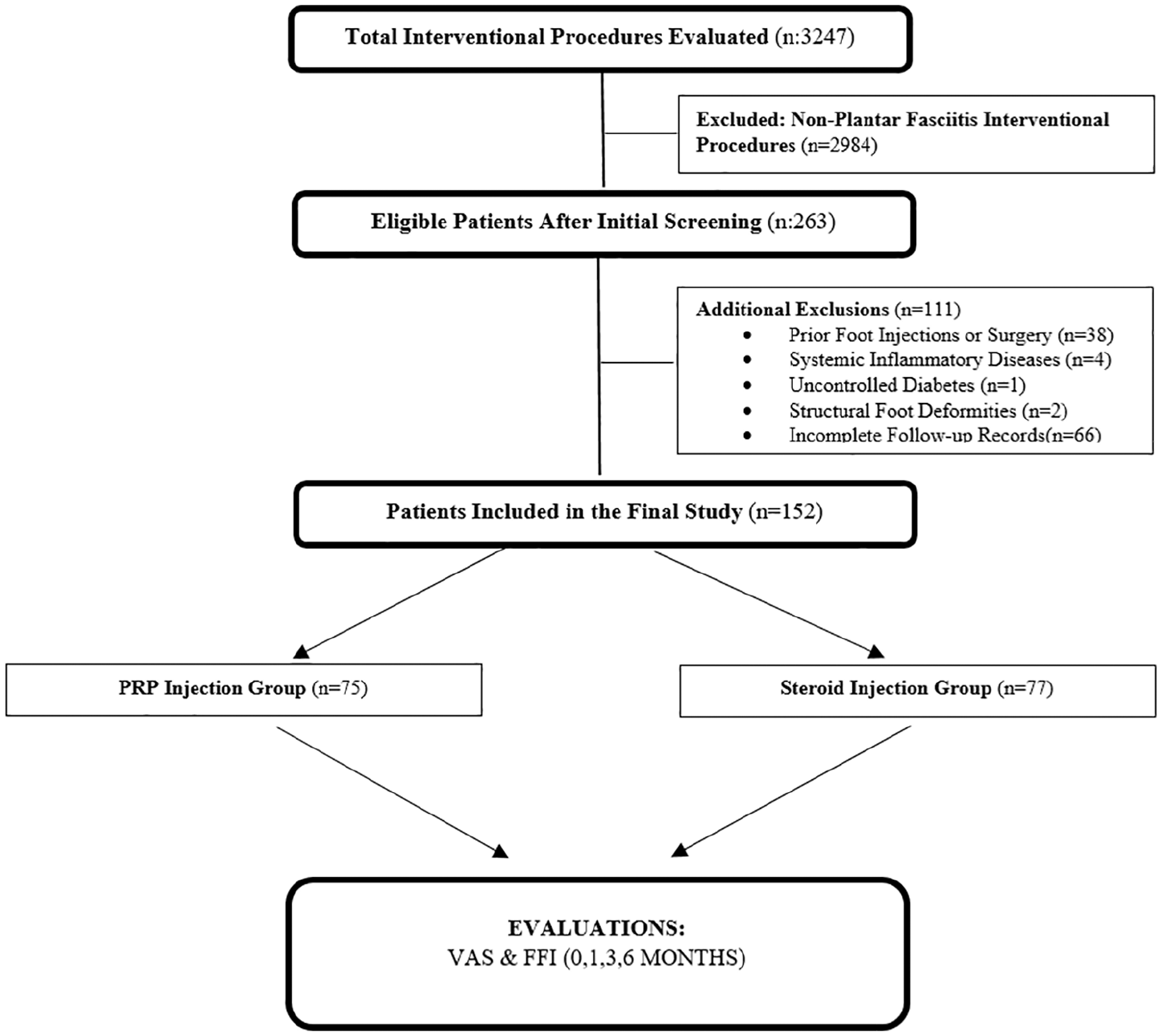
Flowchart of the study. This flowchart illustrates the patient selection process for the study. A total of 3247 patients who underwent interventional pain management procedures during the designated study period were screened. Of these, 152 patients with a confirmed diagnosis of chronic plantar fasciitis, who received ultrasound-guided injection therapy (either steroid or PRP), were included in the final analysis and assigned to groups based on the type of injection procedure administered.
Patients aged 18 years or older with a clinical diagnosis of CPF and persistent symptoms for at least 3 months, despite conservative management such as NSAIDs, physiotherapy, orthotic support, or stretching exercises, were eligible for inclusion. Only patients with no previous history of CS or PRP injections in the affected foot were considered. Exclusion criteria included a history of prior foot injections or foot surgery, the presence of systemic inflammatory diseases (such as rheumatoid arthritis, psoriatic arthritis, or ankylosing spondylitis), uncontrolled diabetes mellitus with associated peripheral neuropathy, structural foot deformities affecting gait biomechanics (including conditions such as severe pes planus, pes cavus, and hallux valgus), and incomplete medical records or loss to follow-up.
A detailed analysis of the patient selection process and exclusion criteria is shown in Figure 1.
Ultrasound-Guided Injection Protocol
All injections were performed by the same experienced physiatrist under real-time ultrasound guidance using a Hitachi Aloka Arietta 65 (Hitachi Medical Systems, Tokyo, Japan) ultrasound device equipped with a high frequency (6-18 MHz) linear transducer. Patients were positioned in the prone position with the foot adequately supported to ensure optimal precision during injection. The ultrasound probe was placed longitudinally along the medial aspect of the heel to ensure clear visualization of the medial calcaneal tuberosity and the plantar fascia insertion site.
For patients in the steroid group, a mixture of 40 mg of triamcinolone acetonide and 1 mL of 2% lidocaine was prepared in a sterile syringe and injected using a 22-gauge needle with an in-plane approach under real-time ultrasound guidance. The injection targeted the medial calcaneal tuberosity and the plantar fascia insertion site in a single bolus without multiple punctures, following standard clinical practice for CS administration.
For patients in the PRP group, 30 mL of venous blood was extracted from the antecubital vein into citrate-containing tubes using a sterile vacutainer system. The blood was then processed with an Elektro-Mag M815 A2 CGF and PRP/PRF centrifuge at 3200 rpm for 10 minutes to achieve optimal platelet concentration. The resulting PRP product was characterized by a 4- to 6-fold increase in platelet concentration compared to baseline whole blood levels, minimal leukocyte content with reduced neutrophil proportions, and negligible erythrocyte contamination, corresponding to a leukocyte-poor PRP profile. Subsequently, the top 3-mL layer of PRP was extracted and injected under real-time ultrasound guidance using a 22-gauge needle with an in-plane approach, precisely targeting the medial calcaneal tuberosity and plantar fascia insertion site, with a peppering technique applied, involving multiple small injections around the plantar fascia to enhance biological stimulation.
Postprocedure Protocol
After injection, patients were monitored for 20-30 minutes for immediate adverse reactions. All patients were systematically instructed in a standardized home-based exercise program emphasizing plantar fascia and Achilles tendon stretching. In addition, patients were advised to apply cold therapy to the heel area and to limit high-impact activities for at least 1 week. Paracetamol was allowed for pain, but NSAIDs were discouraged in the PRP group because of potential interference with platelet activity and healing.
Outcome Measures
The primary outcome measure includes pain intensity assessed using the VAS, and the secondary outcome measure includes functional status assessed by the FFI. The VAS is a validated 10-point numeric rating scale used to assess pain intensity, with 0 representing no pain and 10 representing the worst possible pain.17,39 The VAS was chosen for its ability to detect changes in pain levels over time. The FFI is a validated tool designed to measure the impact of foot pathology on daily activities. 4 The Turkish version of the FFI, which has established validity and reliability, was used in this study. 2 The FFI consists of 3 subscales: The first subscale, the pain subscale, assesses foot-related pain in different activities. The second subscale, the disability subscale, assesses difficulty in performing functional tasks. The third subscale, activity limitation subscale, measures limitations in daily activities due to foot pain. Each subscale is scored from 0 to 100, with higher scores indicating more pain, disability, and activity limitation. 4
In order to ensure that the results of the study were clinically meaningful, the MCID thresholds were integrated into the study design. These thresholds, which were derived from established literature, describe the smallest improvement in outcome measures that patients perceive as beneficial. The MCID for the VAS is 9 mm (0.9 cm), which indicates the minimum pain reduction required for meaningful symptom relief. For the FFI, the MCID is 7 points for total FFI, indicating that the observed functional improvements are clinically meaningful. 19
VAS and FFI scores were recorded at before injection (baseline) and during scheduled follow-up visits at 1, 3, and 6 months postinjection. All patients were systematically followed up through the hospital’s clinical record system. Approximately 1 week before each scheduled follow-up, patients were contacted by phone to confirm their appointment status. For patients who had not yet made an appointment, new follow-up appointments were scheduled to ensure complete data collection. Minor scheduling variations (±7 days) were tolerated around the planned 1-, 3-, and 6-month follow-up visits.
Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics 22.0 (IBM Corp, Armonk, NY). The Shapiro-Wilk test assessed data normality. Descriptive statistics were reported as mean ± SD for continuous variables and frequencies (%) for categorical variables. Between-group comparisons used independent t tests for normally distributed data and Mann-Whitney U tests for non-normal data. Within-group comparisons employed repeated measures analysis of variance with Bonferroni correction for parametric data and Friedman tests with Wilcoxon post hoc analysis for nonparametric data. Effect sizes were calculated using Cohen d and partial η². Statistical significance was set at P <.05.
Results
A total of 152 patients were included in the study, with 77 patients in the CS group and 75 patients in the PRP group (Figure 1).
The mean age was 46.75 ± 11.05 years in the CS group and 47.28 ± 10.12 years in the PRP group. The proportion of female patients was higher in both groups, with 59 females (76.6%) and 18 males (23.4%) in the CS group and 61 females (81.3%) and 14 males (18.7%) in the PRP group. Other baseline demographic and clinical characteristics, including body mass index (BMI), duration of pain, and affected side, were comparable between the groups (Table 1).
Baseline Characteristics of the Study Population.
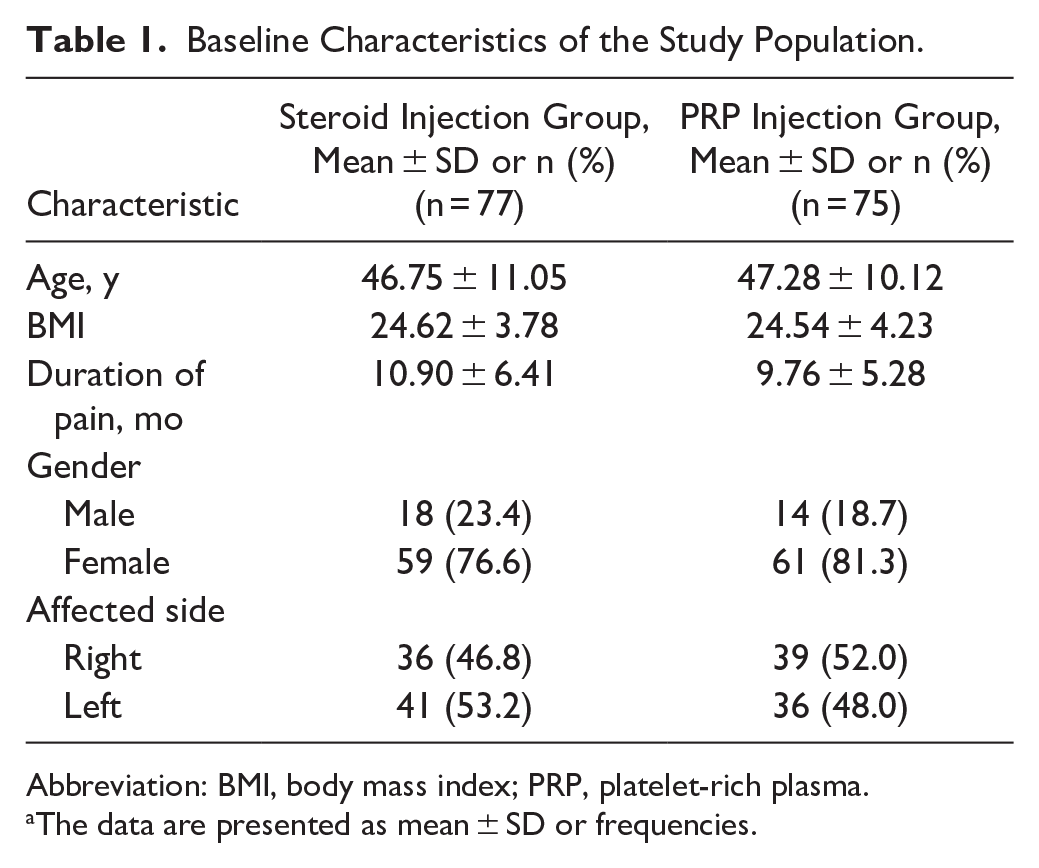
Abbreviation: BMI, body mass index; PRP, platelet-rich plasma.
The data are presented as mean ± SD or frequencies.
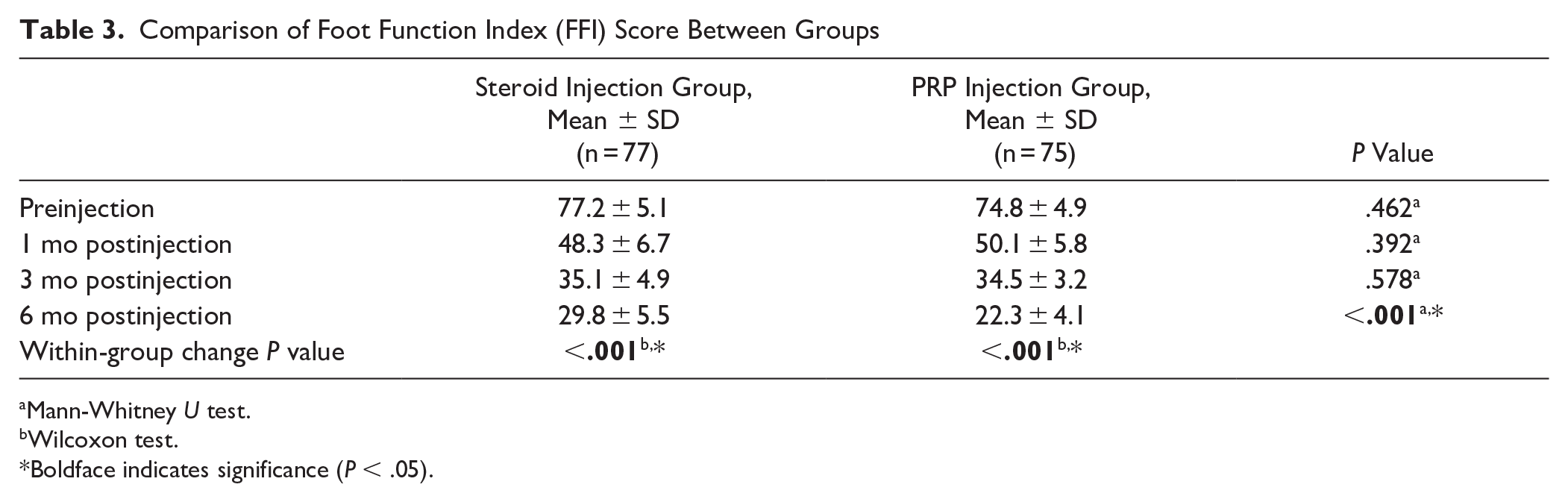
The severity of pain was measured using the VAS, which revealed a decrease in both groups over time (Table 2 and Figure 2). At baseline, the VAS scores were similar between the CS group (8.13 ± 0.64) and the PRP group (8.06 ± 0.49) (P = .449). At 1 month, VAS scores were 4.38 ± 1.4 in the CS group and 4.57 ± 1.19 in the PRP group, with no statistically significant difference between the groups (P = .368). At 3 months, VAS scores further decreased to 3.12 ± 0.96 and 3.06 ± 0.09 in the CS and PRP groups, respectively, again without significant difference (P = .586). At 6 months, the PRP group showed significantly lower VAS scores (1.98 ± 0.35) compared with the steroid group (2.79 ± 1.13) (P < .001). Within-group improvements in VAS scores were statistically significant for both groups (P < .001 for both). FFI, a measure of functional outcomes, exhibited a comparable trend (Table 3 and Figure 3). At baseline, the FFI scores were 77.2 ± 5.1 and 74.8 ± 4.9 in the CS and PRP groups, respectively (P = .462), indicating no significant difference at the study’s inception. There was a progressive functional improvement in both groups, with no significant differences observed at 1 month (P = .392) and 3 months (P = .578). However, at 6 months, the PRP group exhibited significantly greater functional improvement (FFI: 22.3 ± 4.1) compared with the steroid group (FFI: 29.8 ± 5.5) (P < .001).
Comparison of Visual Analog Scale (VAS) Score Between Groups.
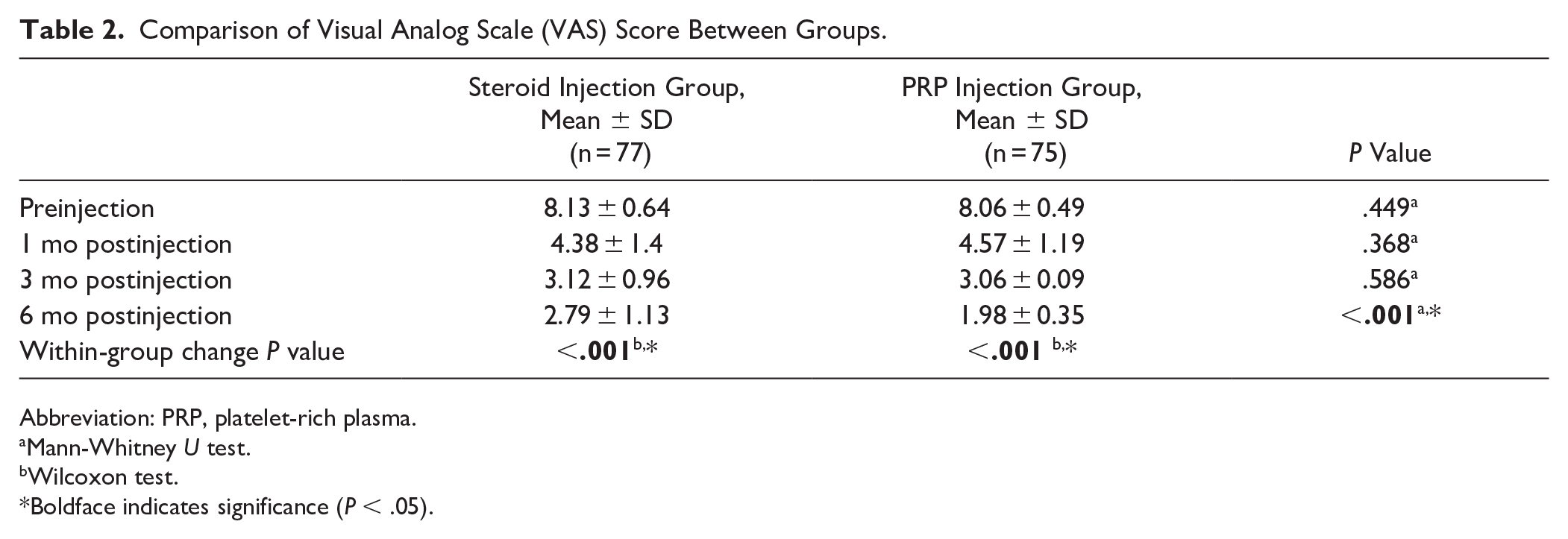
Abbreviation: PRP, platelet-rich plasma.
Mann-Whitney U test.
Wilcoxon test.
Boldface indicates significance (P < .05).
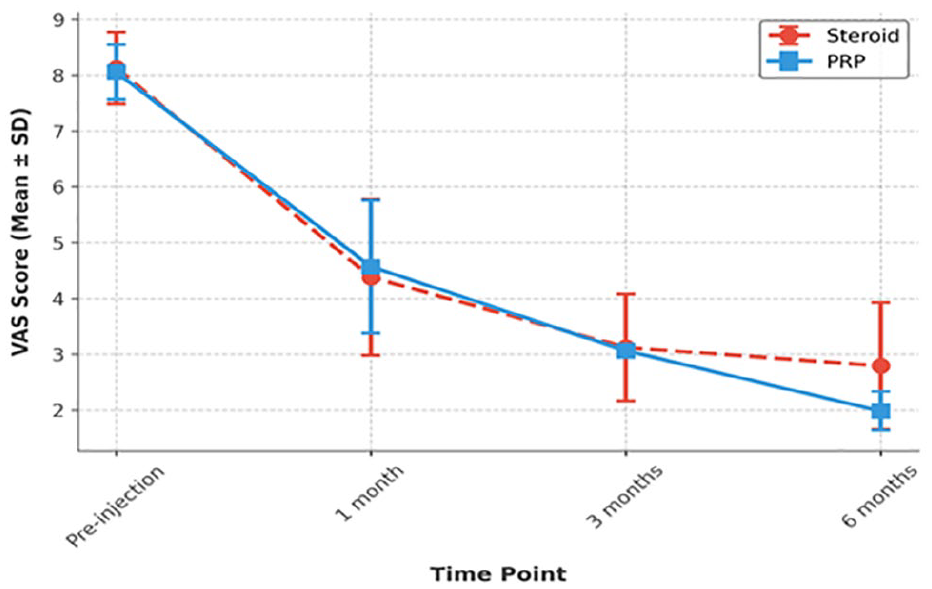
Comparison of VAS score between steroid and PRP groups over time. PRP showed a significant advantage at 6 months. PRP, platelet-rich plasma; VAS, visual analog scale.
Comparison of Foot Function Index (FFI) Score Between Groups
Mann-Whitney U test.
Wilcoxon test.
Boldface indicates significance (P < .05).
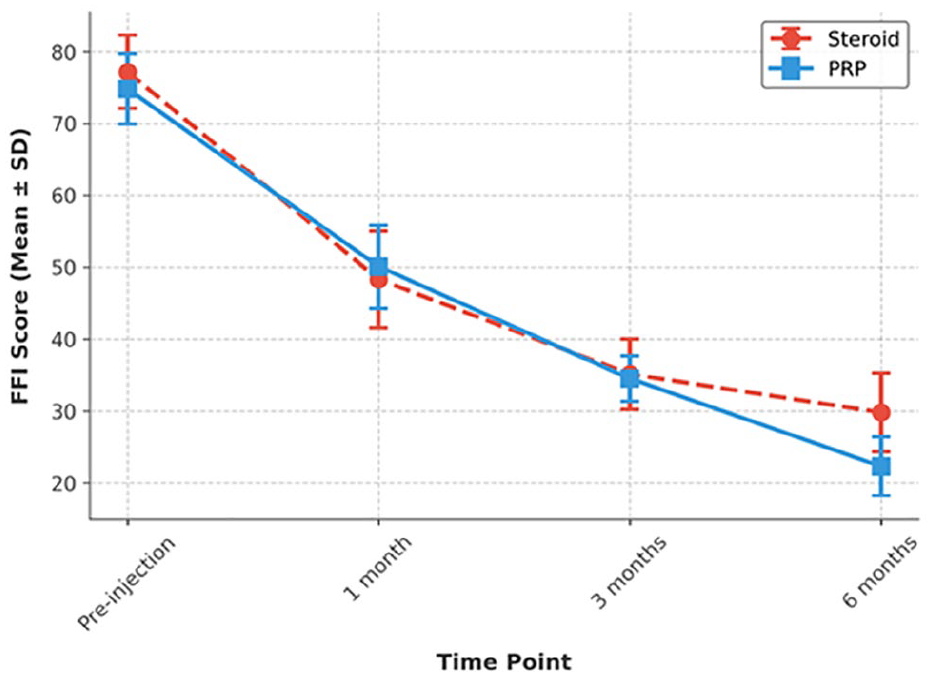
Comparison of FFI score between the Steroid and PRP groups over time. PRP showed a significant advantage at 6 months. FFI, Foot Function Index; PRP, platelet-rich plasma.
At 1 month, FFI scores were 48.3 ± 6.7 in the CS group and 50.1 ± 5.8 in the PRP group (P = .392). At 3 months, scores were 35.1 ± 4.9 for the CS group and 34.5 ± 3.2 for the PRP group (P = .578). At 6 months, the PRP group demonstrated significantly greater functional improvement, with FFI scores of 22.3 ± 4.1 compared with 29.8 ± 5.5 in the steroid group (P < .001).
Importantly, both the PRP and CS groups demonstrated clinically meaningful improvements from baseline in both pain (VAS) and functional (FFI) scores, exceeding the established MCID thresholds.
Despite this statistical significance, the VAS reduction was 5.34 cm in the steroid group and 6.08 cm in the PRP group, resulting in a between-group difference of 0.81 cm. Given that the MCID threshold for VAS is 0.9 cm, the observed between-group difference did not meet the threshold for clinical significance.
Importantly, within-group reductions in FFI were 47.4 points for the steroid group and 52.5 points for the PRP group, resulting in a between-group difference of 7.5 points.
Transient pain exacerbation occurred in 1 patient (1.3%) in the PRP group and in 2 patients (2.6%) in the CS group. Symptoms in all affected patients resolved spontaneously within maximum 5 days under routine follow-up without requiring additional treatment. No other adverse events were reported in either group throughout the study period.
Discussion
This study robustly compares CS and PRP efficacy in CPF treatment, showing that both improve short-term pain and function, although PRP offers superior benefits, sustaining VAS and FFI improvements at 6 months. Although PRP showed statistical superiority in functional outcomes at 6 months, both groups improved significantly from baseline. The clinical significance of between-group differences remains modest. These findings align with recent systematic reviews, meta-analyses, and randomized controlled trials (RCTs) that have consistently reported PRP’s superiority over CS in CPF management.1,10-13,34,40
Pain reduction was observed in both groups; however, PRP demonstrated a sustained analgesic effect, with significantly lower VAS scores at 6 months compared with CS. These results are consistent with those reported in a meta-analysis by Hurley et al, 13 which found that PRP outperformed CS beyond 3 months, with an effect size favoring PRP for long-term pain relief. Similarly, a multicenter and randomized controlled trial (RCT) by Shetty et al 34 showed that PRP-treated patients experienced superior pain reduction lasting up to 12 months, whereas CS effects diminished after 3 months. In another double-blind RCT, Jain et al 14 confirmed PRP’s significantly lower VAS scores at 6 and 12 months compared with CS, reinforcing PRP’s sustained analgesic properties.
Functional improvement, measured using FFI scores, followed a similar trajectory. Although both groups exhibited a significant reduction in disability, PRP yielded greater improvements at 6 months, suggesting superior functional restoration. Moreover, both treatment groups demonstrated clinically meaningful improvements from baseline in pain and function, as both VAS and FFI scores exceeded their respective MCID thresholds at 6 months. This aligns with a large systematic review by Herber et al 11 which concluded that PRP-treated patients showed significantly better functional recovery than those receiving CS, particularly in high-demand individuals. Similarly, Khandaker et al 15 found that ultrasound-guided, intrafascial PRP injections significantly enhanced both pain relief and functional capacity, as reflected in improved FFI scores over time. Furthermore, Peerbooms et al 29 reinforced PRP’s long-term therapeutic benefits in a double-blind multicenter RCT, demonstrating that PRP yielded greater improvements in foot function and disability scores compared with CS, with sustained effects beyond six months. Although many trials extend follow-up to 12 months to evaluate sustained treatment efficacy, a 6-month time frame is commonly adopted in musculoskeletal rehabilitation studies to facilitate early clinical decision making and minimize confounding effects of long-term compliance and cointerventions.6,11,33 Moreover, the choice of a leukocyte-poor PRP preparation and triamcinolone-based CSI aligns with current clinical standards and was selected to enhance safety, minimize variability, and maintain methodologic consistency with recent comparative studies.29,30,35
As a result, at 6-month follow-up, VAS and FFI scores were significantly lower both within and between groups. When we evaluated the clinical reflection of these 2 outcome measures, the MCID value was found to be high for both VAS and FFI within the group. This shows that both pain and functional improvement were significantly reflected in the clinic. However, in the intergroup evaluation, the MCID value was found to be low in VAS and high in FFI. This showed that, although PRP and CS caused a significantly greater decrease in VAS at 6 months, this was not reflected in the patient’s clinic. There was no clinically significant difference between the groups. On the other hand, the data showed that functional improvement was significantly more reflected in the clinic in the PRP group compared with the CS group.
Despite the growing body of evidence favoring PRP, the lack of standardization in PRP preparation protocols remains a major limitation in the literature. Factors such as centrifugation speed, platelet concentration, leukocyte content, and activation methods significantly influence clinical outcomes. 29 In this study, a standardized PRP preparation protocol was employed, including a fixed centrifugation speed (1800 rpm, 10 minutes) and an ultrasound-guided peppering injection technique to enhance treatment reproducibility. However, future studies should incorporate platelet concentration quantification and compare leukocyte-rich vs leukocyte-poor PRP formulations to determine optimal PRP characteristics for CPF treatment.8,29
A significant strength of this study is its emphasis on a specialized foot and ankle outpatient clinic, where patients with foot-specific pathologies, including plantar fasciitis, are routinely evaluated and managed using standardized protocols. This clinical setting enables the creation of a more homogeneous patient population, thereby reducing variability in treatment response and postinjection rehabilitation adherence. In contrast, Montes-Salas et al 23 emphasized limitations in prior studies related to patient heterogeneity, differences in previous treatments, and variability in procedural techniques, which may confound treatment outcomes. By selecting a well-defined cohort with systematically recorded clinical data, our study minimizes these confounding factors, ensuring a more reliable comparison of PRP and CS efficacy.
Study Limitations
The retrospective design of the study raises the possibility of selection bias, thus limiting the ability to establish causality between treatment and outcomes. Although baseline demographic and clinical characteristics were statistically comparable between the PRP and CS groups, treatment allocation was influenced by a shared decision-making process between physician and patient, potentially resulting in preference-based selection bias. Additionally, the use of MCID values based on previously published minimal important difference estimates introduces a degree of interpretative uncertainty, especially as these values may not be validated for this population. Furthermore, despite efforts to minimize inhibitory factors, differences in patients’ adherence to postinjection rehabilitation protocols, including stretching exercises and activity modifications, may have influenced outcomes. The six-month follow-up period limits the assessment of the long-term sustainability of improvements observed beyond this time period. It should also be noted that although we refer to the study by Landorf et al for MCID estimation, Landorf et al directly reported the minimal important difference values for the original domains of the FFI. Therefore, our use of these values is methodologically appropriate. However, this distinction is transparently stated as a limitation, recognizing that minimal important difference and MCID represent related but distinct constructs.
Conclusions
This study found that PRP was associated with modest superiority at 6 months in functional recovery compared with CS. Importantly, the improvement in FFI scores with PRP exceeded the threshold for clinical relevance, underscoring its potential as a preferred midterm intervention. In contrast, the modest between-group difference in pain reduction, although statistically significant, did not translate into clinically meaningful superiority. These findings emphasize the value of integrating functional outcome measures with clinical significance frameworks and support the use of PRP as a viable, evidence-based option in patients unresponsive to conservative care. Although pain was a primary outcome, the between-group difference in VAS scores at 6 months—although statistically significant—did not exceed the MCID, and thus was not clinically meaningful. Further studies are needed to evaluate whether these findings persist or diverge with longer follow-up.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007251346784 – Supplemental material for Comparative Effectiveness of Platelet-Rich Plasma and Steroid Injections in Chronic Plantar Fasciitis: Evaluating Pain Relief and Functional Recovery
Supplemental material, sj-pdf-1-fai-10.1177_10711007251346784 for Comparative Effectiveness of Platelet-Rich Plasma and Steroid Injections in Chronic Plantar Fasciitis: Evaluating Pain Relief and Functional Recovery by Ömer Faruk Bucak, Eser Kalaoglu, Mucahit Atasoy and Evrim Coskun in Foot & Ankle International
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to Çiğdem Çınar for her invaluable contributions and support in the development of this study.
Ethical Approval
Ethical approval for the study was obtained from the Ethics Committee of Başakşehir Çam and Sakura City Hospital (approval no. 2024-265, dated October 30, 2024). The study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The data supporting this study’s findings are available on request from the corresponding author. The data are not publicly available because of privacy or ethical restrictions.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.