
Abstract
Background:
With the growing popularity of total ankle arthroplasty (TAA), there is an expectation that revision surgeries will increase. However, limited data exist on revision TAA outcomes using a revision-specific implant. The INVISION Total Ankle Revision System is a modular revision implant (Wright Medical Group/Stryker). The purpose of this study was to report implant survivorship, complications, and radiographic and clinical outcomes of revision TAA using the INVISION system at a minimum 2-year follow-up.
Methods:
A retrospective review was conducted of 27 patients that underwent a revision TAA using the INVISION implant at a single institution with minimum 2-year follow-up between 2016 and 2020. Implant survivorship was the primary outcome. Demographics, complications, reoperation, and radiographic and clinical outcomes were recorded.
Results:
Implant survivorship was 81.5% (22/27) at a mean of 3.6 years following revision TAA using the INVISION implant. There was evidence of aseptic loosening in 3 patients and talar subsidence in 4 patients on final radiographs. Reoperation rate at final follow-up was 40.7%, most commonly for aseptic loosening (n = 3), septic TAA (n = 2), or gutter impingement (n = 2). The mean American Orthopaedic Foot & Ankle Society (AOFAS) total score was 54.5, Foot and Ankle Ability Measure (FAAM) activities of daily living (ADL) subscale score was 52.9, and FAAM Sports was 31.0.
Conclusion:
Revision TAA using the INVISION implant demonstrated 81.5% implant retention at a mean of 3.6 years in this complex cohort. Patient-reported outcomes were lower than those reported after primary TAA. Physicians and patients should recognize that revision TAA remains a challenging procedure with a high rate of complications and reoperations.
This is a visual representation of the abstract.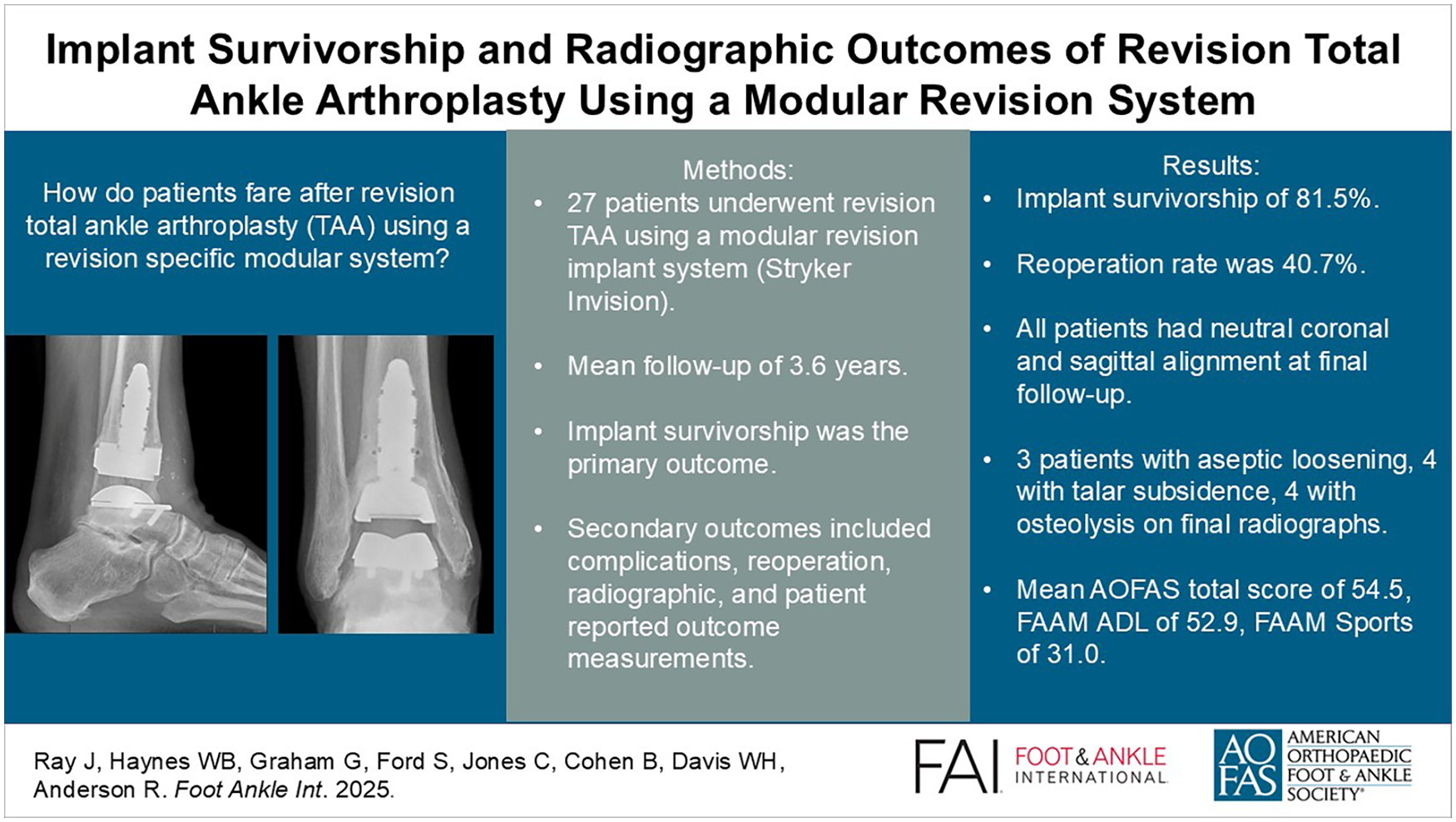
Introduction
With the growing popularity of total ankle arthroplasty (TAA), revision surgeries are expected to significantly increase.1,2,9 Revision TAA remains challenging with high complication rates.1,11 Limited data exist on revision TAA using a revision-specific implant. The INVISION Total Ankle Revision System is a modular revision system with theoretical benefits of improved fixation, restoration of joint height, coverage of bone loss, and maximal talar coverage (Wright Medical Group/Stryker). A recent study of the INVISION TAA noted excellent short-term survivorship at 3.5 years with no failures. 8 The purpose of this study was to describe implant survivorship and clinical and radiographic outcomes of revision TAA at a single institution using the INVISION implant at minimum 2-year follow-up.
Methods
This retrospective chart review examined patients at a single institution who underwent revision TAA using an INVISION talus and/or tibial component between 2016 and 2020 with minimum 2-year follow-up. All patients who underwent revision TAA using the INVISION system were included (Figure 1). Patients with less than 2-year follow-up and unwilling to return to clinic were excluded. A prospectively maintained TAA registry was queried, identifying 27 eligible patients. Two patients were deceased at final follow-up.

Anteroposterior (AP) and lateral weightbearing radiographs of a patient 18 months postoperative revision total ankle arthroplasty using the INVISION tibial and talar components.
Four fellowship-trained foot and ankle orthopaedic surgeons with extensive TAA experience performed the revision procedures. The revision TAA was performed with an intramedullary-referencing tibial implant and flat-cut talus. The previous components were assessed for loosening. Revision was performed with either an INBONE II (n = 11) or INVISION (n = 16) tibial component and either an INBONE II (n = 7) or INVISION (n = 20) talar component (Table 1). Component cementation was performed at the discretion of the operating surgeon in cases with poor bone stock or extensive bone loss.
Summary of Patients Included in the Case Series.
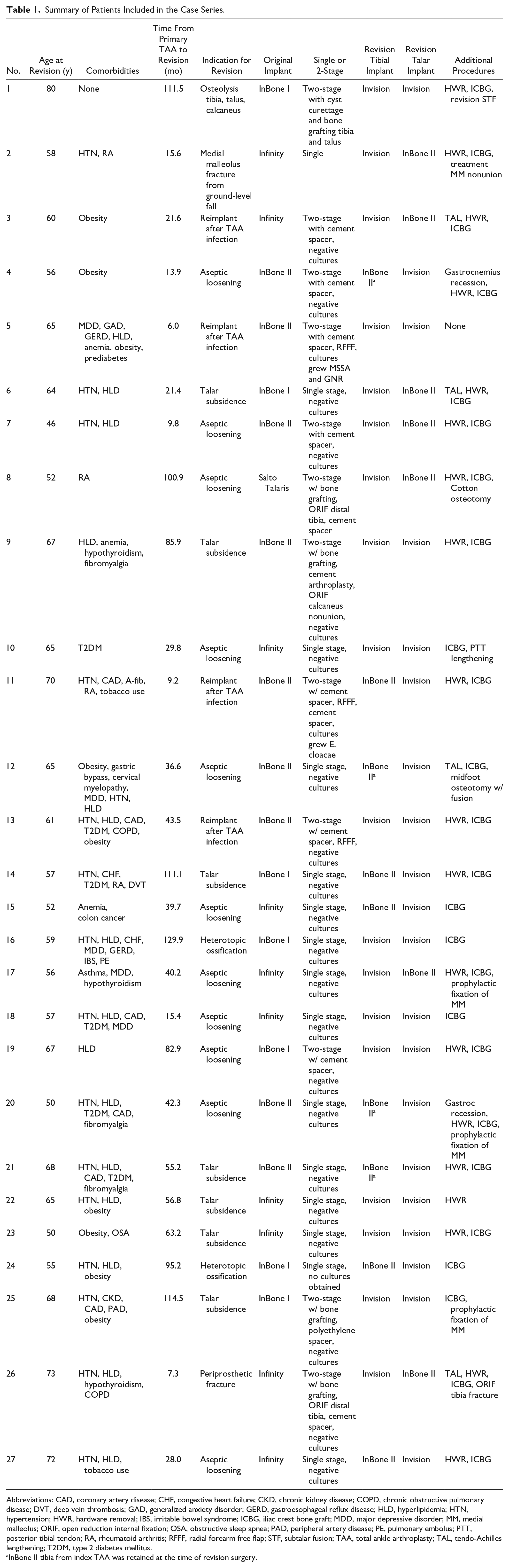
Abbreviations: CAD, coronary artery disease; CHF, congestive heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DVT, deep vein thrombosis; GAD, generalized anxiety disorder; GERD, gastroesophageal reflux disease; HLD, hyperlipidemia; HTN, hypertension; HWR, hardware removal; IBS, irritable bowel syndrome; ICBG, iliac crest bone graft; MDD, major depressive disorder; MM, medial malleolus; ORIF, open reduction internal fixation; OSA, obstructive sleep apnea; PAD, peripheral artery disease; PE, pulmonary embolus; PTT, posterior tibial tendon; RA, rheumatoid arthritis; RFFF, radial forearm free flap; STF, subtalar fusion; TAA, total ankle arthroplasty; TAL, tendo-Achilles lengthening; T2DM, type 2 diabetes mellitus.
InBone II tibia from index TAA was retained at the time of revision surgery.
Indications for revision TAA included aseptic loosening (n = 11), talar subsidence (n = 7), reimplant after infection (n = 4), periprosthetic fracture (n = 2), heterotopic ossification (n = 2), and osteolysis (n = 1). All patients underwent concomitant procedures at time of revision TAA (Table 1). The tibial component was cemented in 14.8% of patients (4/27), and the talus was cemented in 44.4% of patients (12/27).
The primary outcome was implant survivorship defined as retention of metal components at final follow-up. Additional procedures, complications, and reoperation were recorded. Clinical outcomes included Foot and Ankle Ability Measure (FAAM) activities of daily living and sports subscales, along with total American Orthopaedic Foot & Ankle Society (AOFAS) scores. Weightbearing radiographs were assessed for osteolysis, loosening, subsidence, and component alignment. Aseptic loosening was determined by progressive lucency greater than 2 mm at follow-up and confirmed intraoperatively by manually testing the implants for stability. Osteolysis was defined as a cyst greater than or equal to 5 mm. This is usually observed without subsidence initially (Figure 2).

An example of osteolysis of the talus.
Statistical Analysis
Descriptive statistics with means and SDs for continuous variables, and ratios and percentages for categorical variables. Analysis was conducted using SAS (SAS Institute, Cary, NC) with P value <.05 considered significant. Comparisons between cemented and uncemented groups were performed using Fisher exact test.
This study was approved by the Wake Forest University Institutional Review Board (IRB) with a protocol number of IRB00090483.
Results
The study included 27 patients with a mean age of 61.4 ± 8.1 years, 63.0% male (17/27), who underwent revision TAA using INVISION tibia and/or talus implant (7 tibia only, 9 talus only, 11 combined). Implant survivorship was 81.5% (22/27) at a mean of 3.6 years. The average time from index TAA to revision using INVISION was 4.3 years (range 7 months to 10.8 years). Only 4 patients had a cemented tibial component with 1 implant failure noted, making it difficult to draw conclusions given the small sample size. To our knowledge, this is the first study to examine cementing of the tibial and/or talar component in revision TAA using the INVISION implant.
Radiographic Outcomes
All patients had neutral coronal and sagittal alignment on final radiographs. The median coronal tibiotalar angle (TTA) was 89.5 degrees (interquartile range 88, 90.9). The mean coronal distal tibia component angle (DTCA) and sagittal DTCA were 89.6 ± 1.7 degrees and 87.6 ± 1.6 degrees, respectively, at final follow-up. On final radiographs, aseptic loosening was noted in 3 patients (11.1%), talar subsidence in 4 patients (14.4%), and tibial and talar osteolysis in 4 patients (14.4%).
Patient-Reported Outcome Measures
At final follow-up, the mean FAAM activities of daily living was 52.9 ± 22.2 and mean FAAM sports was 31.0 ± 20.9. Average AOFAS total score was 54.5 ± 25.7.
Reoperation
The reoperation rate at final follow-up was 40.7% (Table 2), most commonly for aseptic loosening (n = 3), septic TAA (n = 2), gutter impingement (n = 2), instability (n = 1), medial malleolus stress fracture (n = 1), talar subsidence (n = 1), and wound dehiscence (n = 1). There were no intraoperative complications noted. Implant survivorship at final follow-up was 81.5% (22/27). Postoperative complications as described by Glazebrook et al 3 are described in Table 3.
Reoperation Numbers, Indication, and Reoperation Procedures Following Revision TAA.
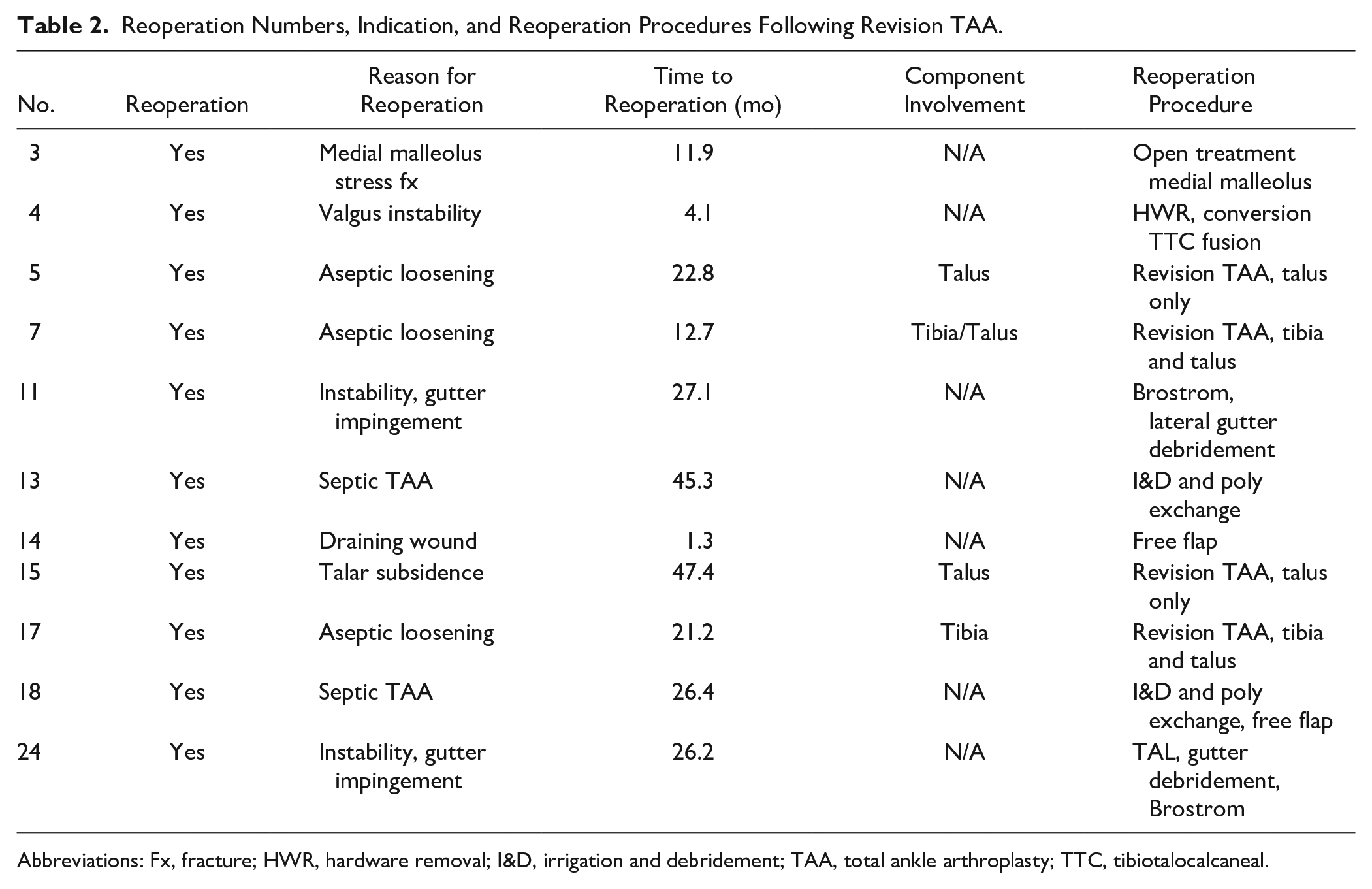
Abbreviations: Fx, fracture; HWR, hardware removal; I&D, irrigation and debridement; TAA, total ankle arthroplasty; TTC, tibiotalocalcaneal.
Postoperative Complications as described by Glazebrook et al. 3
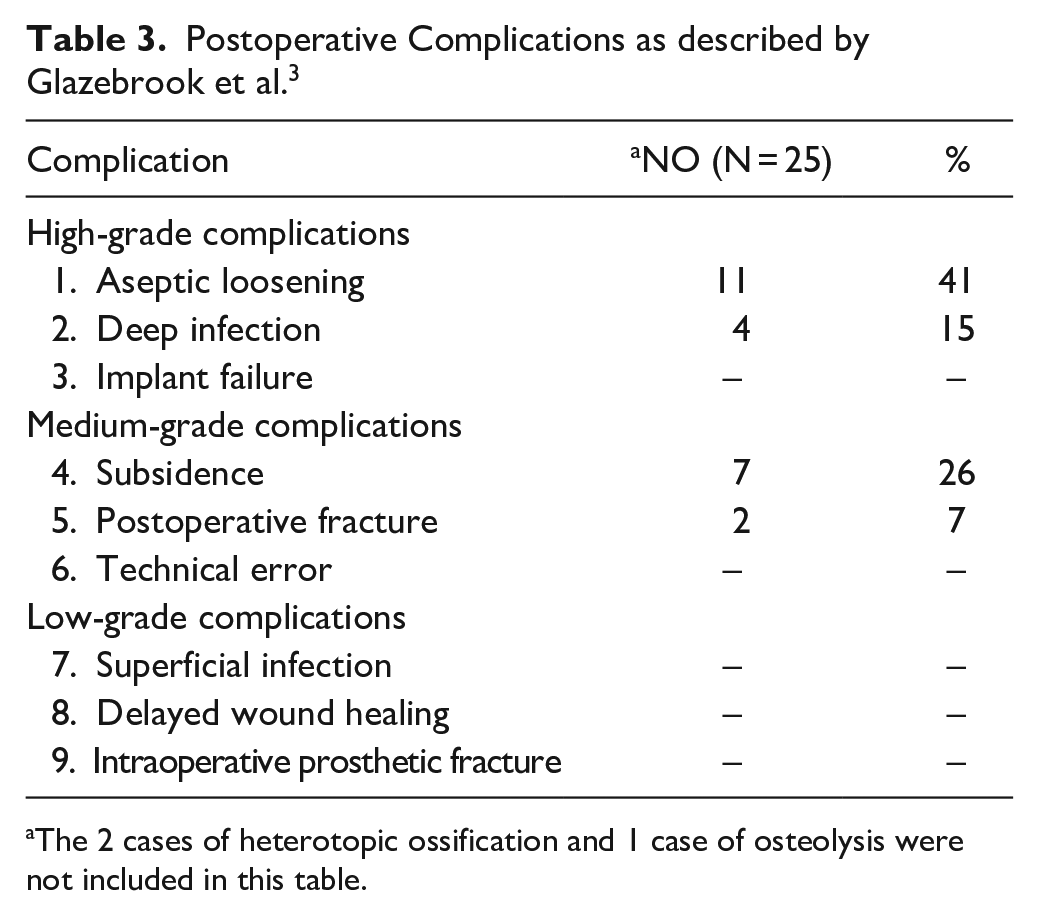
The 2 cases of heterotopic ossification and 1 case of osteolysis were not included in this table.
Discussion
With the growing popularity of TAA, understanding the challenges, survivorship, and complications of revision TAA is essential. Historically, failed TAA was treated with conversion to fusion, often associated with poor outcomes and high nonunion rates.4,5 The introduction of modular revision-specific TAA implants has provided additional surgical options for these complex cases.
Recent studies on early implant survivorship of revision TAA using the INVISION implant have reported excellent survivorship with low complication and reoperation rates.7,8 Purnell et al 8 reported 100% implant survivorship rate in 19 patients at mean follow-up of 3.5 years with no reoperations. Similar results were reported by Martin et al 7 in 17 patients at mean follow-up of 3.4 years noting 100% implant retention with 1 patient undergoing reoperation. A study of 28 patients undergoing revision TAA using the INVISION talus noted a 10.7% rate of reoperation and 10.7% implant failure at 1.3 years. 10 Implant survivorship in our study was 81.5% at a mean of 3.6 years, still good given the complex nature of revision TAA but lower than previous reports. Our higher complication rate is likely multifactorial in nature. This group of patients was treated with the Invision system, which is generally used for more complex revisions with more bone loss and fixation challenges, therefore excluding easier revision cases. Moreover, alternative surgical options for these patients remains limited and typically include either a complex fusion/reconstruction or amputation. The small sample sizes of our study and other similar studies should also be taken into account as a different outcome for 1 or 2 patients can drastically skew the results of the study.
Reoperation rates at final follow-up in our study were 40.7% for revision TAA using the INVISION system, higher than previously reported.5-7 Martin et al 7 did note an overall complication rate of 39.3% at 1.3 years using INVISION talus, despite the lower 10.7% rate of reoperation. The most common complications after revision TAA in our study were due to aseptic loosening (11.1%), septic TAA (7.4%), and gutter impingement (7.4%).
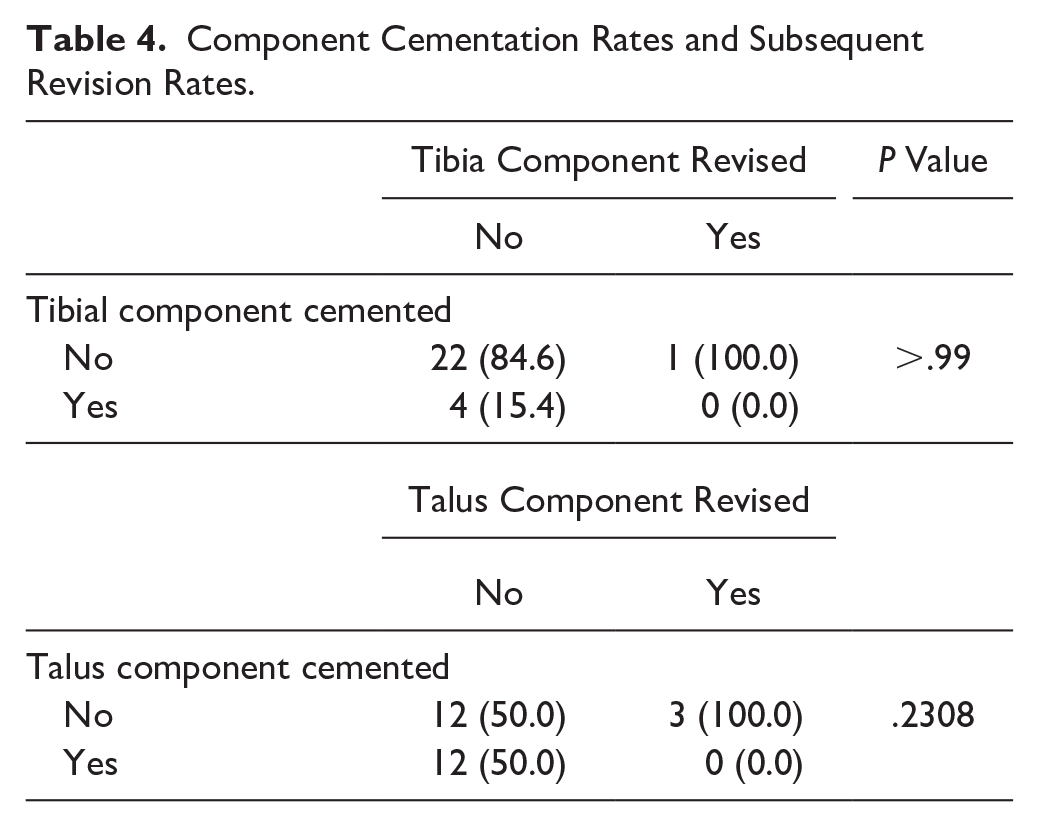
Among patients with a cemented talar component, implant survivorship at final follow-up was 91.7%, compared with 73.3% in the uncemented group. The use of cement should be considered in patients undergoing revision TAA, with many of these patients having significant bone loss and poor overall bone stock. Revision rates for the patients with cement compared to the noncement group can be found in Table 4.
Component Cementation Rates and Subsequent Revision Rates.
The mean FAAM Activities of Daily Living, FAAM Sports, and average AOFAS total scores were acceptable, but lower than previously reported literature in patients who underwent primary TAA (Table 5). Lachman et al 6 noted similar findings in their series of 29 revision TAA, noting that improvements in PROMs were higher after primary TAA than after revision TAA. The lower PROMs observed in our study are likely due to the revision nature of the surgery as well as complexity with implant failure.
Patient-Reported Outcome Measures.
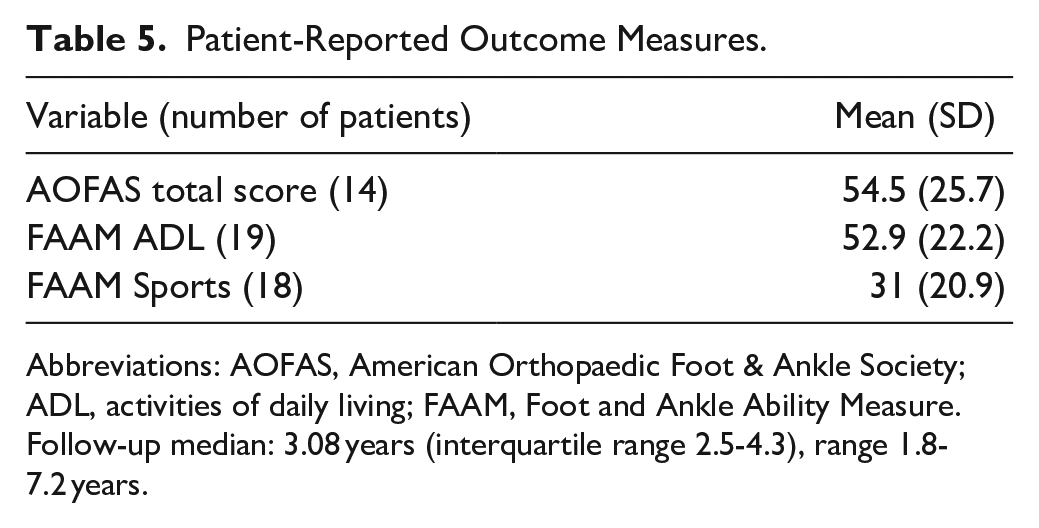
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; ADL, activities of daily living; FAAM, Foot and Ankle Ability Measure.
Follow-up median: 3.08 years (interquartile range 2.5-4.3), range 1.8-7.2 years.
This study has several limitations. The retrospective nature is subject to recall bias. Despite the small sample size and relatively short follow-up, reporting the high complication rates in this complex cohort is important. Small sample size potentially limits the generalizability of our results. Short follow-up could also underestimate the rate of failure in the long term. The surgeons at our institution have extensive experience with TAA and helped design the INVISION system, making generalizability difficult. Preoperative PROMs were not available for review, making it difficult to assess clinical improvements after revision TAA. Finally, patient retention was an issue given our institution is a tertiary referral center, with several patients traveling long distances making selection bias a concern.
Conclusion
Revision TAA with the INVISION system resulted in 81.5% implant retention at early follow-up in a complex cohort. Although this approach offers an alternative to fusion or amputation, patients and physicians should be aware of the associated high complication and reoperation rates. Further studies with larger cohorts and longer follow-up are needed to clarify the durability and comparative effectiveness of this system.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007251352529 – Supplemental material for Implant Survivorship and Radiographic Outcomes of Revision Total Ankle Arthroplasty Using a Modular Revision System
Supplemental material, sj-pdf-1-fai-10.1177_10711007251352529 for Implant Survivorship and Radiographic Outcomes of Revision Total Ankle Arthroplasty Using a Modular Revision System by Justin J. Ray, William B. Haynes, G. Dillon Graham, Samuel E. Ford, Carroll P. Jones, Bruce E. Cohen, W. Hodges Davis and Robert B. Anderson in Foot & Ankle International
Footnotes
Ethical Approval
Ethical approval for this study was obtained from Wake Forest School of Medicine IRB (IRB00090483).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Justin J. Ray, MD, reports disclosures relevant to manuscript from Stryker: support for attending meetings and/or travel. Samuel E. Ford, MD, reports disclosures relevant to manuscript from Stryker: consulting and general disclosures from 2022-22215-S AOFAS Grant $15,300. Carroll P. Jones, MD, reports disclosures relevant to manuscript from Stryker: royalties, consulting fees and general disclosures. Bruce E. Cohen, MD, reports disclosures relevant to manuscript from Stryker: royalties, consulting, support for attending meetings and general disclosures. W. Hodges Davis, MD, reports disclosures relevant to manuscript from Stryker: royalties, consulting, support for attending meetings, stock. Robert B. Anderson, MD, reports disclosures relevant to manuscript from Stryker: royalties, consulting and general disclosures. Disclosure forms for all authors are available online.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.