
Abstract
Background:
To our knowledge, no study is available comparing the change in ankle mechanics during gait after total ankle arthroplasty (TAA) based on the origin of the osteoarthritis. As the nature of trauma is different in patients sustaining post-fracture ankle osteoarthritis (PFOA) from those sustaining post-sprain ankle osteoarthritis (PSOA), it could be expected that the outcomes of TAA, in terms of ankle mechanics during gait, would be different in the 2 groups. A prospective matched comparative study was therefore performed to investigate whether patients sustaining PFOA had different outcomes in terms of changes to ankle mechanics during gait (before surgery vs 1 year after surgery), compared with patients sustaining PSOA.
Methods:
Fifteen patients with PFOA and 15 patients with PSOA scheduled for primary TAA for pain relief were recruited and peer-matched based on their demographic and spatiotemporal data. All patients underwent a 3D gait analysis before and after surgery, during which a kinematic and kinetic multi-segment foot model was used to quantify inter-segmental joint kinematics and kinetics.
Results:
The PFOA group exhibited significantly lesser pre- vs postoperative increases in ankle (Shank-Calcaneus) joint peak power, and ankle (Shank-Calcaneus) joint work after TAA compared with the PSOA group. Furthermore, the results demonstrated a trend toward greater increases in peak ankle (Shank-Calcaneus) joint plantarflexion moment and in negative ankle (Shank-Calcaneus) joint work for the PSOA group compared with the PFOA group.
Conclusion:
This study suggests that patients sustaining PFOA have smaller pre- to postoperative gains in ankle (Shank-Calcaneus) joint power and ankle (Shank-Calcaneus) joint work during gait after TAA compared with patients sustaining PSOA, with modest between-group effects. Although evidence in TAA is lacking, insights from knee replacement suggest prehabilitation and nutritional support may mitigate deficits, representing a potentially essential strategy for PFOA patients requiring further validation.
This is a visual representation of the abstract.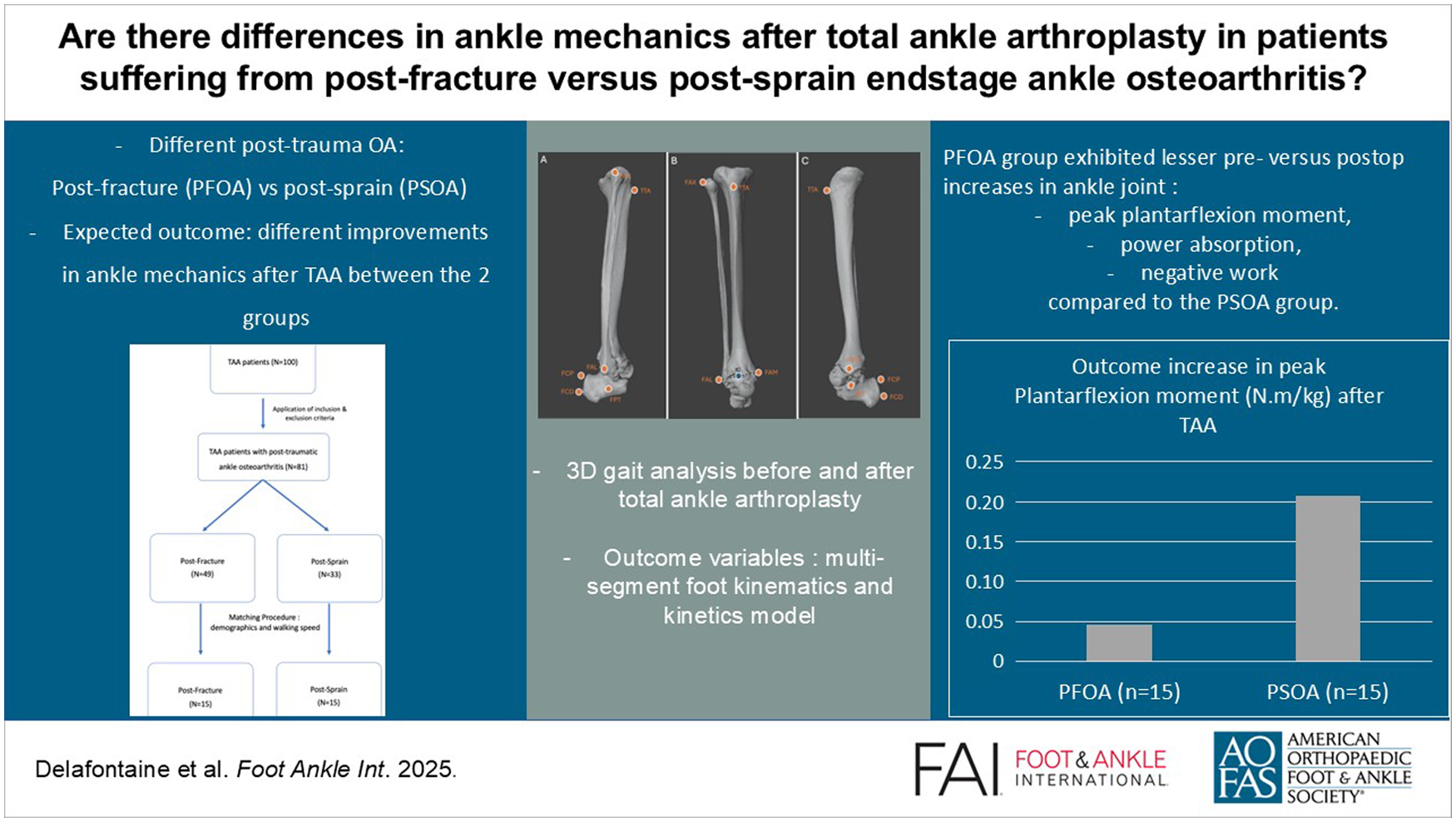
Keywords
Introduction
End-stage ankle osteoarthritis (OA) is a painful and debilitating condition characterized by loss of cartilage, joint space narrowing, and osteophyte formation.1,34 Most cases of OA in the ankle are associated with previous joint trauma, with incidence reaching up to 79.5% of symptomatic ankle OA cases.3,33,38 Posttraumatic ankle OA most frequently occurs secondary to an intra-articular fracture involving the ankle joint and to damage to the stabilizing ligaments of the ankle joint that leads to chronic ankle instability. 33 Evidence suggests that post-fracture OA (PFOA) results either from cartilage breakdown that occurs at the time of the fracture or from chronic cumulative mechanical overload of the cartilage that occurs as a result of incongruities of the post-fracture articular surface.6,26 The evidence also suggests that post-sprain OA (PSOA) results either from cartilage damage sustained at the time of the ankle sprain, or from damage to supporting ligaments of the ankle leading to altered kinematics, increasing stress at the articular surface, and eventually degeneration of the ankle joint cartilage.6,26
Once the resultant pain is no longer responsive to conservative treatment, the surgical management of end-stage ankle OA involves either total ankle arthroplasty (TAA) or ankle arthrodesis, with TAA becoming increasingly the preferred option.10,31,32,36 TAA has the potential to remove the pain, to preserve the preoperative range of motion (RoM), and to reduce the preoperative mechanical compensations occurring in the Chopart and hip joints.2,7,8,20,35 A recent meta-analysis reporting the change in gait mechanics TAA with a fixed-bearing prosthesis found moderate evidence of improved spatio-temporal parameters (ie, mean 0.19-m/s increase in walking speed) and ankle kinematics (ie, mean 3-degree dorsi-/plantarflexion RoM increase) compared with the preoperative condition. 10 To our knowledge, no studies have directly compared the changes in ankle mechanics during gait after TAA based on the origin of the OA. 10 As the nature of trauma is different in patients sustaining PFOA from those sustaining PSOA, it could be expected that the outcomes of TAA, in terms of ankle mechanics during gait, would be different in the 2 groups. A prospective and comparative study was therefore performed to investigate whether patients sustaining PFOA had different outcomes in terms of changes to ankle mechanics during gait (before surgery vs 1 year after surgery), compared to patients sustaining PSOA. It was hypothesized that patients sustaining PFOA would have lesser pre- vs postoperative changes in ankle mechanics during gait after TAA compared with patients sustaining PSOA. This hypothesis was underpinned by the findings of previous studies which highlighted that TAA in patients sustaining PFOA has lesser clinical and radiographic results than in other patient groups. 16 Furthermore, PFOA patients may exhibit greater functional impairments due to soft tissue contracture as a result of previous osteosynthesis surgeries or contracture of muscle-tendon units after scarring of tendons in their sheaths or fibrosis of their muscles. 18
Patients and Methods
Patients
Patients were selected from an ongoing prospective multi-centre study approved by the local research ethical committee (B200-2017-061), all participants having given informed consent. Between January 2017 and June 2021, electronic medical records of 100 eligible patients presenting with end-stage ankle OA scheduled for primary TAA were reviewed for possible inclusion in this study (Figure 1). A total of 81 patients had end-stage posttraumatic ankle OA (48 PFOA subjects and 33 PSOA subjects). Patients who did not complete their 1-year follow-up or explicitly stated in their electronic medical records that their data could not be used for research purposes were excluded from this study. The inclusion criteria were (1) diagnosis of posttraumatic end-stage ankle OA (Giannini stage 3; 3 being subtotal or complete obliteration or deformation of the joint space) with an indication for TAA established by 2 senior orthopaedic surgeons, (2) implantation of a fixed-bearing ankle prosthesis (CADENCE prosthesis; Smith & Nephew, London, United Kingdom), (3) age older than 18 years of age, (4) absence of systemic or neurologic diseases, and (5) capacity of walking at least 100 m without needing any walking aids. Exclusion criteria were (1) any orthopaedic reconstruction or replacement procedures at the foot or at a more proximal level, (2) pain in more than 1 lower-extremity joint in either limb, and (3) neurologic or systemic diseases that could possibly affect gait.
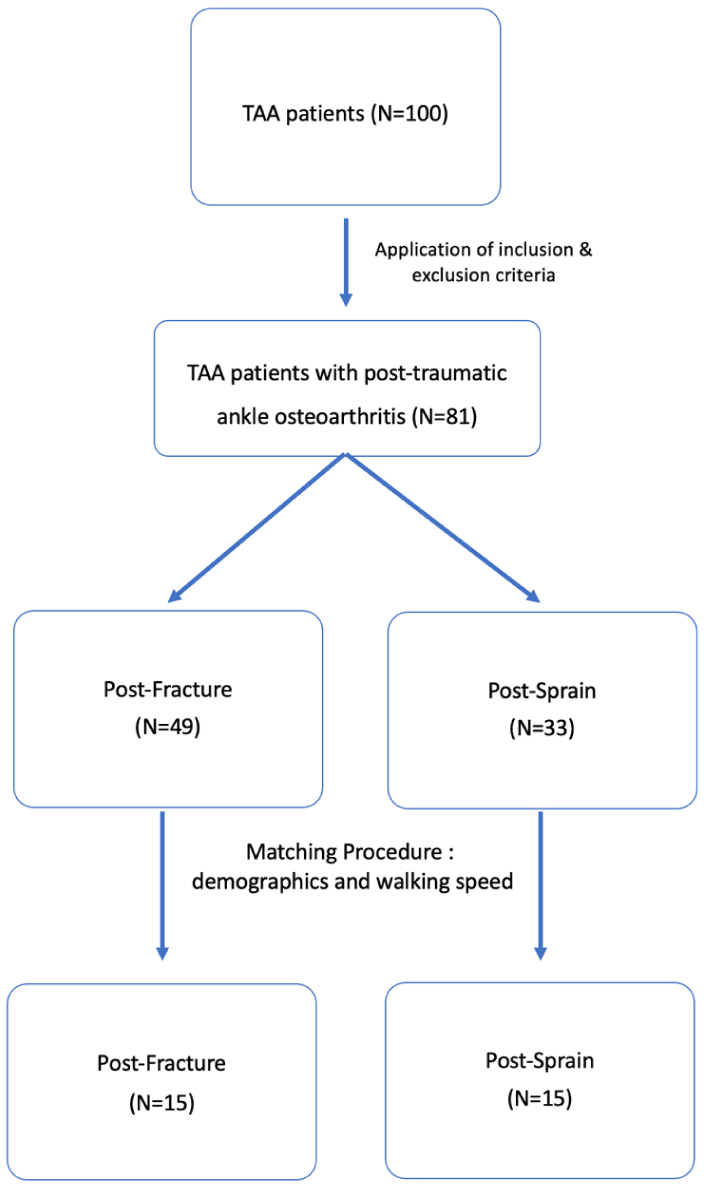
Study flow diagram.
Matching Procedure
Patients were grouped based on their subtype of posttraumatic end-stage ankle OA. Subsequently, pairs were created by matching patients who had PFOA with patients in the PSOA group on the basis of demographic data (age, weight, height, BMI) and spatio-temporal variables. Control of these confounding variables are of primary importance as they may have affected the kinematic and kinetic outcome variables. 4 After the matching procedure, 30 subjects were included in this study. Participants’ demographics, radiographic data, and concomitant ancillary procedures with the implantation of the ankle prosthesis were reported in Table 1. These procedures were performed to restore and maintain the foot and/or hindfoot alignment and ligamentary balance, both factors determining the sustainability of TAA.
Participant’s Demographic Data.
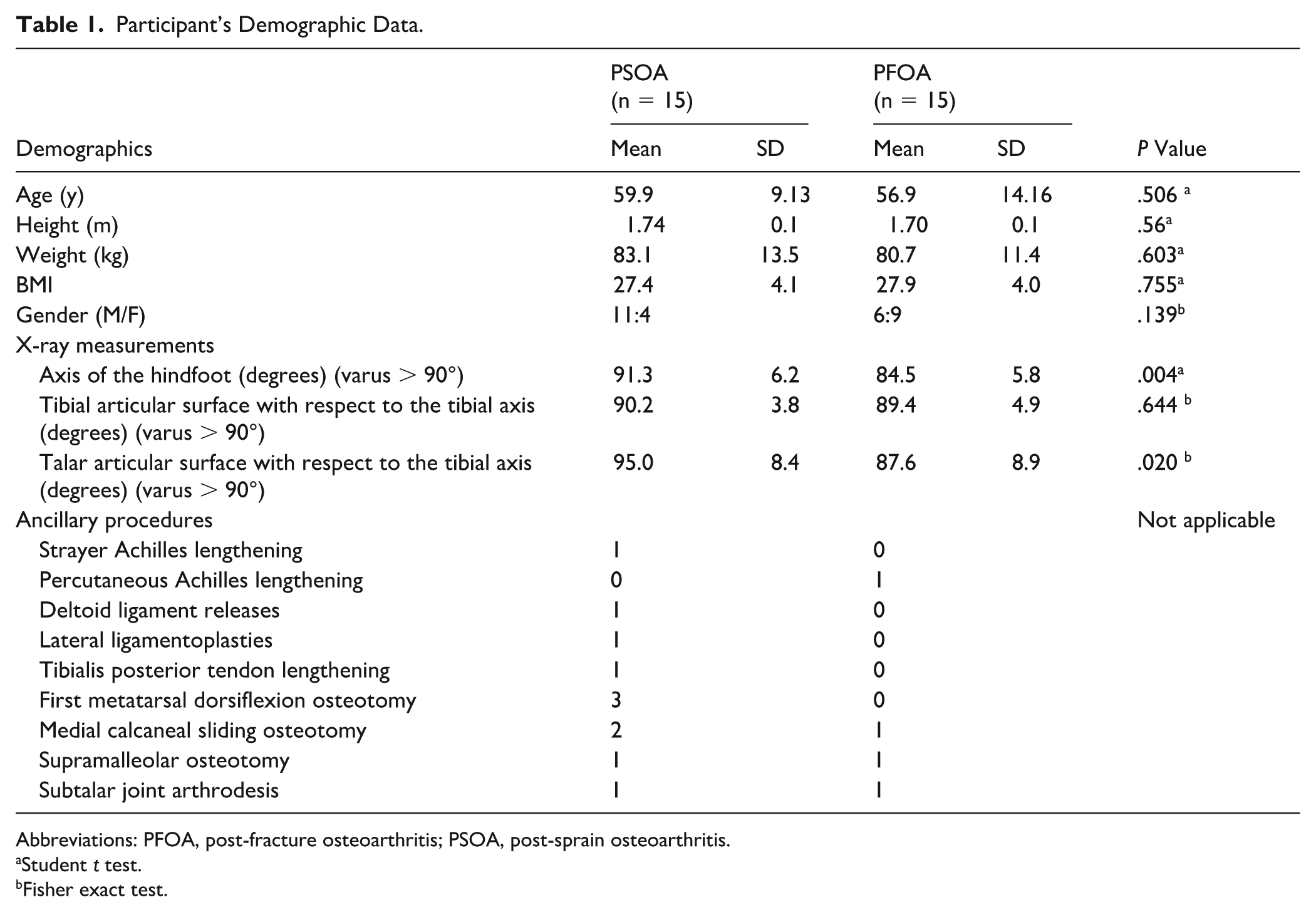
Abbreviations: PFOA, post-fracture osteoarthritis; PSOA, post-sprain osteoarthritis.
Student t test.
Fisher exact test.
Data Collection and Analysis
A motion capture system composed of 10 Miqus optoelectronic motion cameras sampling at 200 Hz was used to track the trajectories of markers (Qualysis, Göteborg, Sweden). The cameras were set up around a 10-m walkway that integrated a Footscan pressure plate (4096 sensors, 2.8 sensors per cm2; RSscan International, Paal, Belgium) mounted on the top of a AMTI-force plate (Advanced Mechanical Technology, Inc, Watertown, MA). Both plates had the same dimensions, measuring 0.5 m by 0.4 m. An RsScan 3D box (RSscan International, Paal, Belgium) provided continuous calibration of the pressure plate with respect to the force plate. Both plates’ data were sampled at 200 Hz.
A senior clinical investigator placed sixteen 8-mm retro-reflective skin markers on the foot and shank of each subject in accordance with the Rizzoli multi-segment foot model marker placement protocol (Figure 2). 22 Patients were asked to walk barefoot at a self-selected, comfortable speed along the walkway. Before the actual data collection, each patient was given enough time to familiarize himself with this walking procedure. Data were collected from subsequent foot and ankle dynamic trials until a minimum of 5 representative trials were recorded per patient. A trial was considered representative when the foot of interest made complete contact with the pressure plate, and there were no obvious changes in the patient’s gait.8,11
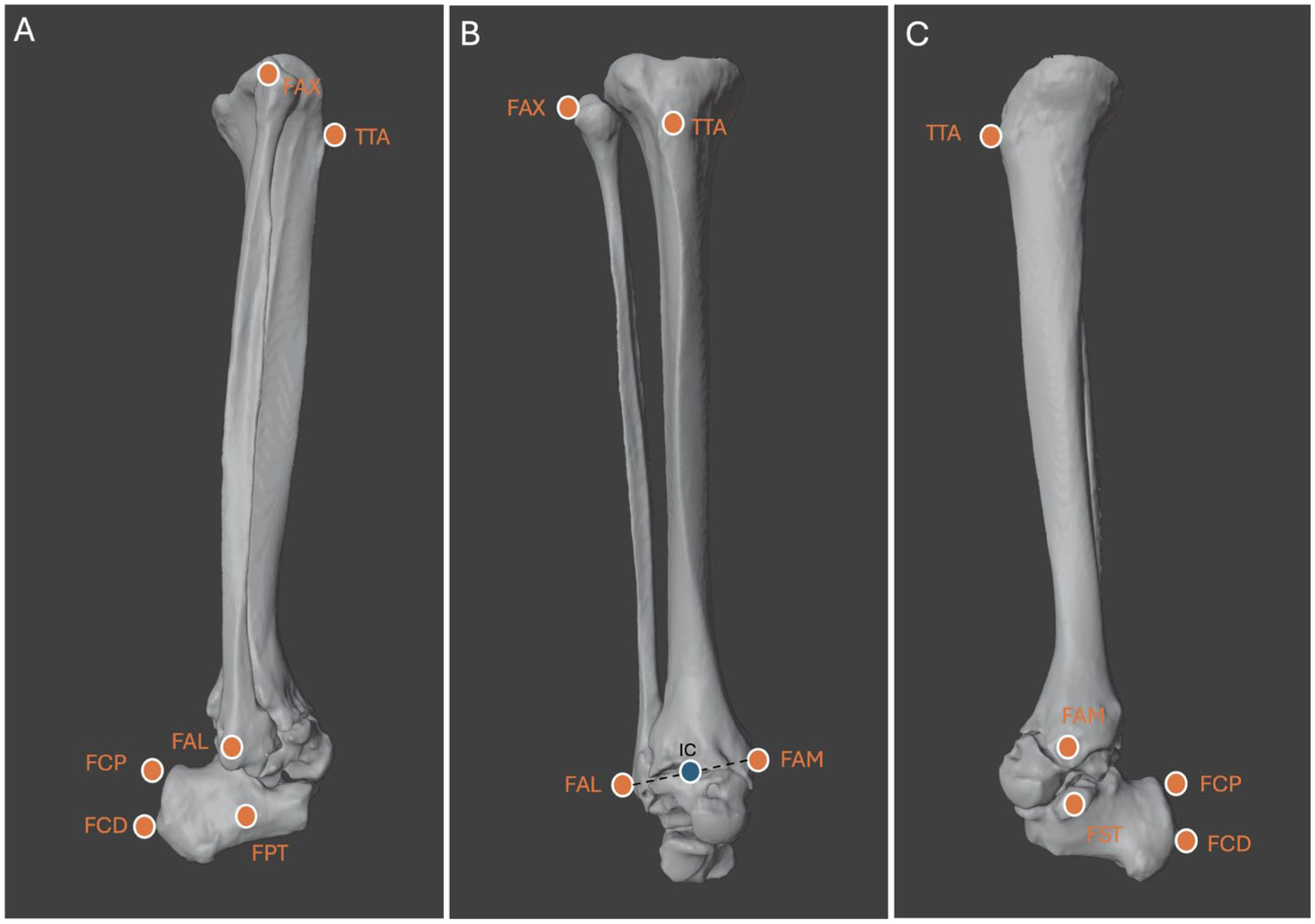
(A) Lateral view of the ankle joint complex. (B) Frontal view of the ankle joint complex. (C) Medial view of the ankle joint complex. The ankle joint complex (AJC) describes, collectively, the subtalar joint and the ankle (talo-crural) joint and is modelled as the interaction between the calcaneus and the shank segments (Shank-Calcaneus).11,13 The inter-segmental joint center was defined according to modified Rizzoli multi-segment foot model (IOR-4Segment-model 1) and is the midpoint between the malleoli markers. (IC) Four markers were placed on the shank segment: FAX, most proximal apex of the head of the fibular; TTA, most anterior prominence of the tibial tuberosity; FAM, distal apex of the medial malleolus; and FAL, distal apex of the lateral malleolus. Four markers were placed on the calcaneal segment: FCP, posterior proximal calcaneus; FCD, posterior distal calcaneus; FPT, lateral apex of the peroneal tubercle; FST, most medial apex of the sustentaculum tali.
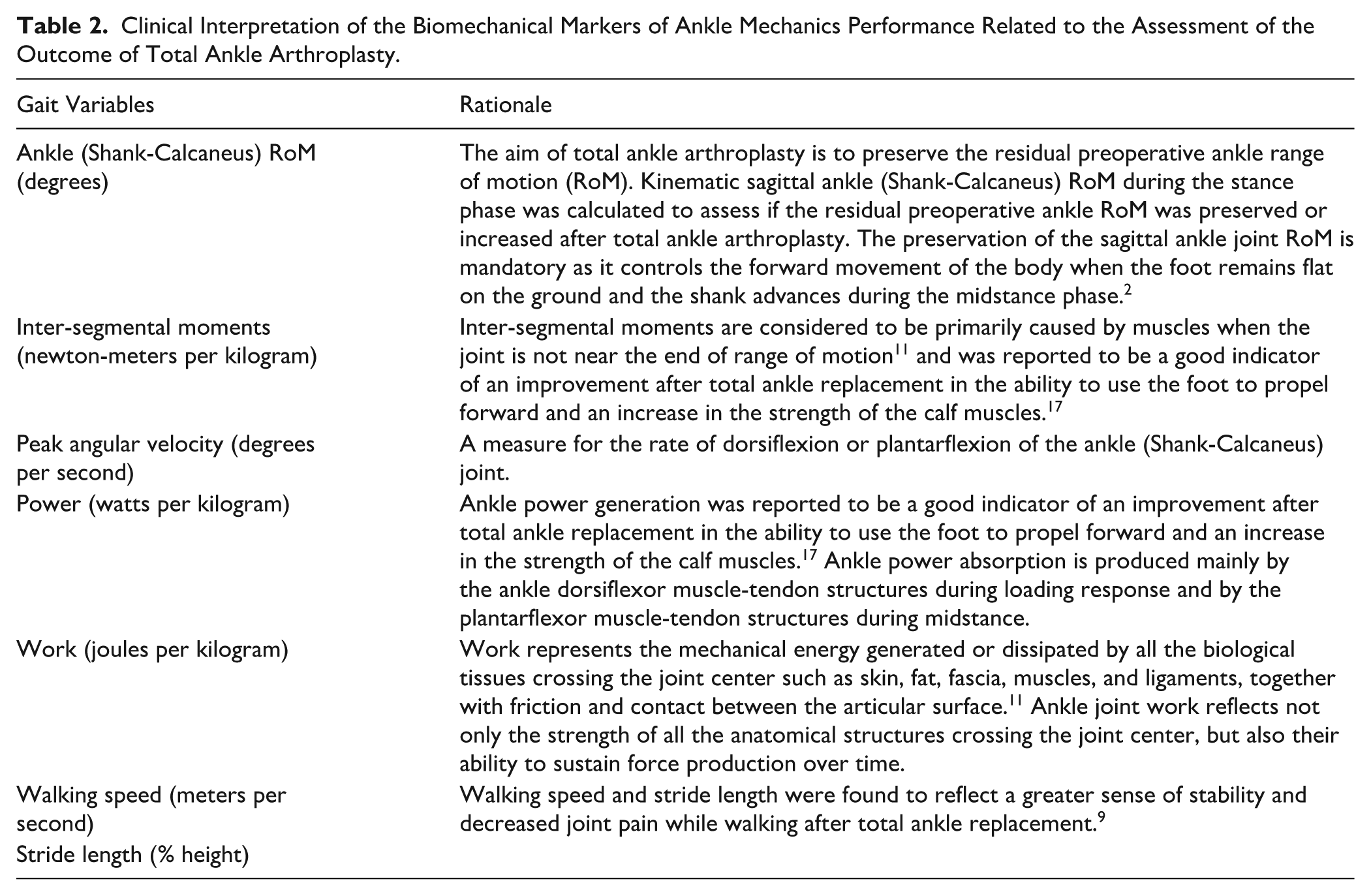
Inter-segmental joint kinematics and kinetics was calculated according to the modified Rizzoli multi-segment foot model (IOR-4Segment-model 1).11,13 This model incorporates 5 segments: shank, calcaneus, midfoot, metatarsus, and hallux. The term joint is defined in this study as the modelled biomechanical interaction between 2 neighbouring foot segments or between 1 foot segment and the ground. 40 The ankle joint complex describes, collectively, the subtalar joint and the ankle joint and is modelled as the interaction between the calcaneus and the shank segments (Shank-Calcaneus).11,13 The inter-segmental joint center was defined according to modified Rizzoli multi-segment foot model (IOR-4Segment-model 1) and is the midpoint between the malleoli markers.11,13 A bottom-up inverse dynamic method was used to quantify the inter-segmental forces and moments in the Joint Coordinate System.12,23 Marker trajectories and force signals were filtered using a low-pass zero-lag, fourth-order, Butterworth filter, with a cut-off frequency of 10 Hz. A proportionality scheme, which was validated in a similar population study, was used to distribute the ground reaction forces and moments over each segment of the IOR-4Segment-model 1. 14 For example, if 35% of the vertical force acted on the hindfoot, it was assumed that 35% of the total horizontal force and vertical moment also acted on the hindfoot. 14 For every sample, the estimation of the ground contact subarea of each segment was obtained by projecting the markers’ position vertically onto the pressure sensor grid. The resulting center of pressure (CoP) of each estimated ground contact subarea was then used as the CoP for the corresponding foot segment in the inverse dynamics calculations. Inter-segmental kinematics and kinetics was computed using an in-house-developed Matlab program (Matlab2016b; The MathWorks, Natick, MA). Internal inter-segmental moments, power, and work variables were normalized by subject-mass and time-normalized to 100% of the stance phase. The following outcome variables for the ankle (Shank-Calcaneus) joint were investigated: RoM during the stance phase, peak internal plantarflexion moment, peak angular plantarflexion and dorsiflexion velocity, peak joint power generation and absorption, and the positive and negative mechanical joint work. The clinical interpretation of the biomechanical markers of ankle mechanics performance, related to the assessment of the outcome of TAA, are described in Table 2.
Clinical Interpretation of the Biomechanical Markers of Ankle Mechanics Performance Related to the Assessment of the Outcome of Total Ankle Arthroplasty.
Study Endpoints and Statistical Analysis
Normality and heteroskedasticity of continuous data were assessed using Shapiro-Wilk and Levene tests, respectively. When the data were normally distributed, an independent sample t test was performed. When the data were not normally distributed, a Mann-Whitney test was used. An adjusted P value (.05/2 = .025) was used to control the type I error rate. Cohen d was computed as a measure of effect size in this analysis. Cohen d measures the number of SDs between sample means, that is, the difference between sample means divided by the pooled SD. The pooled SD is a measure of variability common to both groups. Demographic data and pre-operative gait data of both groups was first compared to ensure that the groups were not significantly different at baseline (Table 1). The primary purpose of the analysis was to report if the 2 subtypes of posttraumatic ankle OA would benefit differently from TAA in terms of ankle mechanics during gait. Therefore, the mean preoperative to postoperative differences between the 2 groups were compared (PFOA vs PSOA). The Cohen d effect size was computed in the PFOA and compared with the PSOA direction; hence, positive d values correspond to lesser average increases in outcomes in the PFOA group than the PSOA group. Effect size (d) was interpreted as follows: d = 0.20 (small effect), d = 0.50 (medium effect), d = 0.80 (large effect), and d = 1.30 (very large effect). Statistical analysis was performed using EasyMedStat (version 3.21; www.easymedstat.com).
Results
Preoperative Baseline Comparison Between PFOA and PSOA Groups
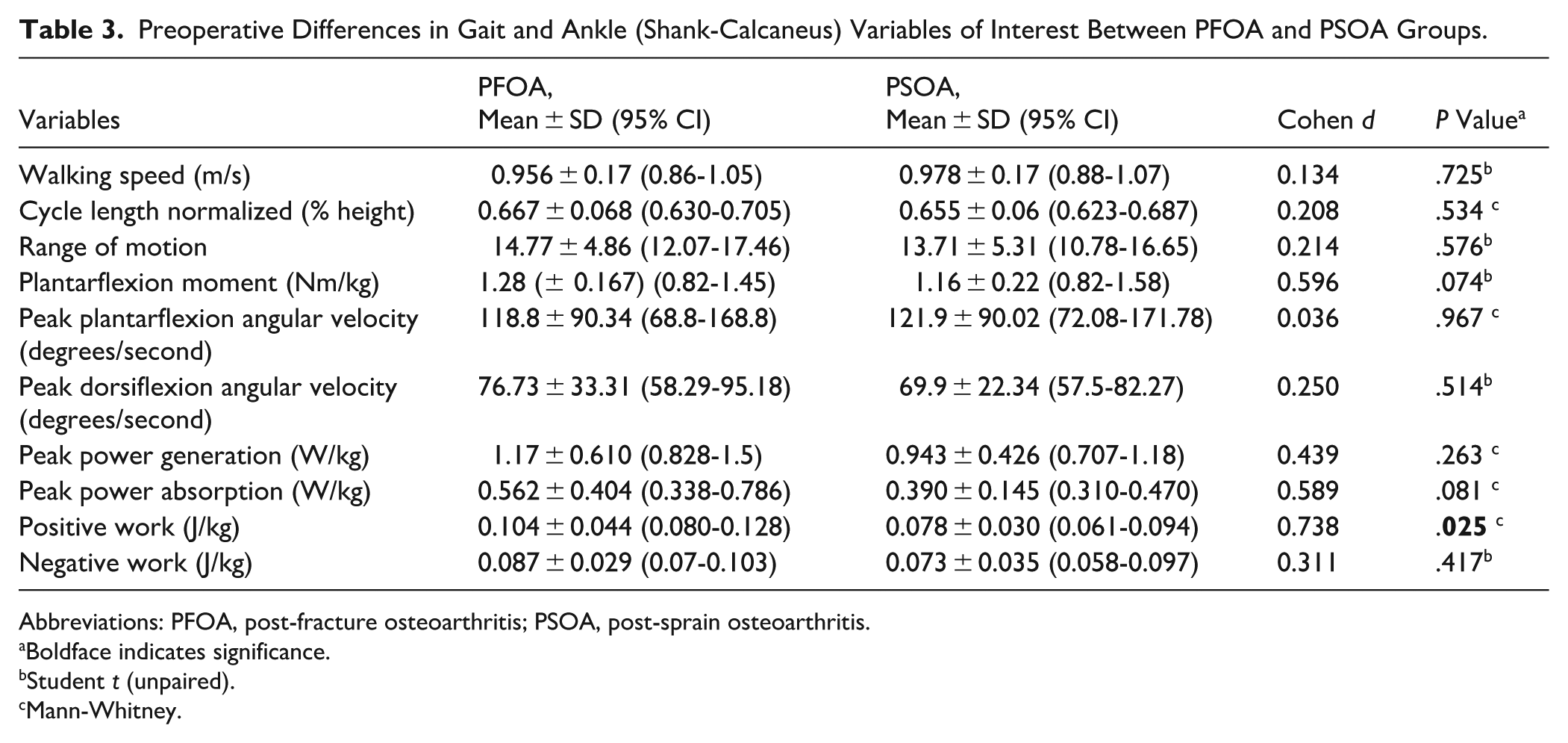
No significant differences between the 2 groups were found for age, weight, height, or BMI (Table 1). The radiographic results found that the PSOA group exhibited preoperatively a more inverted hindfoot and ankle position compared with the PFOA group (Table 1). The preoperative spatiotemporal parameters showed no statistically significant differences in walking speed or normalized stride length (Table 3). Apart from the PFOA group demonstrating greater preoperative positive ankle (Shank-Calcaneus) joint work compared with the PSOA group, no statistical differences were observed between the 2 groups for the outcome variables of the ankle (Shank-Calcaneus) joint in preoperative condition (Table 3). No difference in ankle (Shank-Calcaneus) joint RoM, peak ankle (Shank-Calcaneus) plantarflexion moment, and power generation were found between both groups in preoperative condition (Table 3).
Preoperative Differences in Gait and Ankle (Shank-Calcaneus) Variables of Interest Between PFOA and PSOA Groups.
Abbreviations: PFOA, post-fracture osteoarthritis; PSOA, post-sprain osteoarthritis.
Boldface indicates significance.
Student t (unpaired).
Mann-Whitney.
Comparisons in outcome increase or decrease from preoperative to postoperative condition between PFOA and PSOA
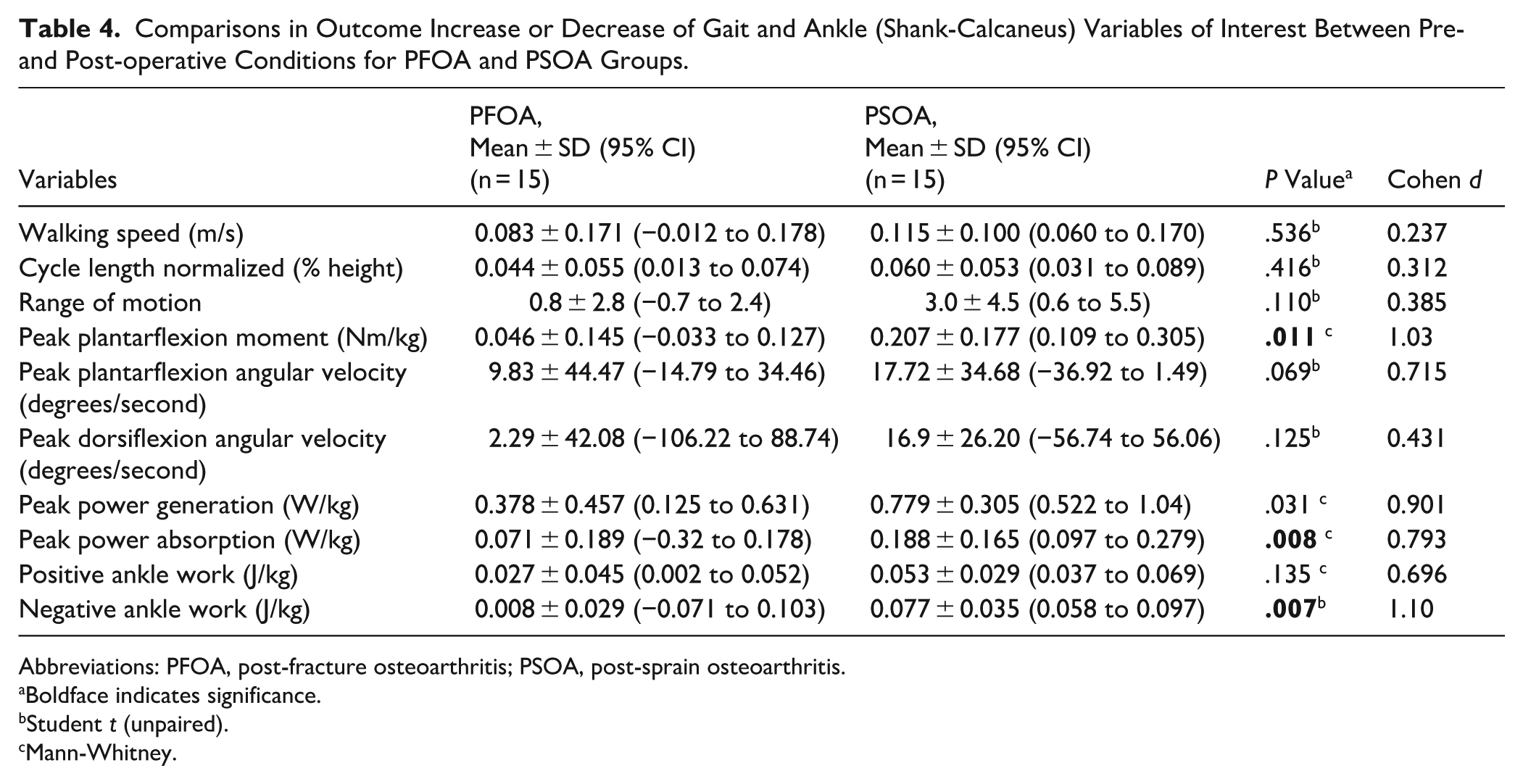
The PSOA group exhibited significant pre- vs. postoperative increases in ankle (Shank-Calcaneus) joint peak plantarflexion moment (P = .011 / d = 1.030 (large)) and power absorption (P = .008 / d = 0.793 (medium)), and in ankle (Shank-Calcaneus) joint negative work after TAA (P = .007; d = 1.100 (large)) compared to the PFOA group (Table 4). A trend was also shown toward greater increases in peak ankle (Shank-Calcaneus) joint power generation (P = .031; d = 0.901(moderate)) and in positive ankle (Shank-Calcaneus) joint work (P = .135; d = 0.696 (moderate)) for the PSOA group compared to the PFOA group (Table 4).
Comparisons in Outcome Increase or Decrease of Gait and Ankle (Shank-Calcaneus) Variables of Interest Between Pre- and Post-operative Conditions for PFOA and PSOA Groups.
Abbreviations: PFOA, post-fracture osteoarthritis; PSOA, post-sprain osteoarthritis.
Boldface indicates significance.
Student t (unpaired).
Mann-Whitney.
Discussion
TAA is a widely used treatment approach in patients sustaining end-stage posttraumatic ankle OA.10,31,32,36 A plethora of studies have demonstrated the efficacy of total ankle arthroplasty, with results suggesting significantly improved gait outcomes such as spatio-temporal parameters and ankle kinematics compared with the pre-operative condition, and irrespective of the type of ankle prosthesis used. 10 Despite this, it is not known how the sub-aetiology of posttraumatic ankle OA may affect the outcomes of TAA in terms of ankle mechanics during gait.
The findings of this study revealed that patients sustaining PFOA would have lesser improvements in ankle (Shank-Calcaneus) joint moment and work during gait after TAA compared to patients sustaining PSOA. The results would appear to corroborate previous findings that PFOA patients may exhibit greater functional impairments, because of soft tissue contracture as a result of previous osteosynthesis surgeries or contracture of muscle-tendon units after scarring of tendons in their sheaths or fibrosis of their muscles. 18 Hoekstra et al 19 found reduced ankle RoM in patients with a history of trimalleolar ankle fracture. Although restoring ankle mobility is a primary objective in all rehabilitation protocols, our findings together with those of Hoekstra et al suggest that postoperative rehabilitation in patients who have undergone an osteosynthesis procedure for their ankle fracture should focus on restoring the complete RoM of the affected ankle joint and limiting the development of arthrofibrosis and muscle adhesions at the posterior aspect of the ankle joint. Additionally, it is likely that surgical variables, such as the quality of fracture reduction and the extent of soft tissue injury, may play a substantial role in determining long-term joint health. The preservation of full ankle plantarflexion mobility, as well as strength of the calf muscles during pre-swing, is key for propelling the body forward during walking.5,19 Combining these 2 aspects may help reduce the risk of developing posttraumatic ankle OA and limit functional impairments of the affected ankle joint.5,19
The combination of dynamics parameters and kinematics parameters provides significant added value in interpreting ankle (Shank-Calcaneus) joint function during the stance phase of gait. Although there was no significant pre- to postoperative ankle (Shank-Calcaneus) RoM difference between the 2 groups, the PFOA group showed at least twice lesser improvement in ankle dynamic parameters (such as peak plantarflexion moment, peak generation/absorption joint power, and positive/negative joint work) compared with the PSOA group. From a clinical perspective, this may suggest that the PSOA group had a greater active force-generating capacity of the plantarflexor muscles after TAA compared to that of the PFOA group. Furthermore, the differences observed in the dynamic parameters were not related to a difference in walking speed, as no significant differences were observed in the baseline walking speed, or in the pre- to postoperative increase in walking speed, between the 2 groups. This pre- to postoperative difference in dynamic parameters seems to point towards the presence of either weakness of the calf muscles, or muscle adhesions at the posterior aspect of ankle joint, which may impede the active force-generating capacity of the plantarflexor muscles. Another possible explanation for this is that lesser improvement in peak ankle plantarflexion moment observed in the PFOA compared to the PSOA group may be partially related to the number of ancillary procedures performed in each group (PFOA: 4 procedures vs PSOA: 11 procedures). Previous studies have suggested that concomitant triceps surae lengthening may substantially decrease the active force-generating capacity of the plantarflexor muscles.9,28 However, the number of Achilles lengthening was similar in both groups.
Knowledge gained from total knee arthroplasty (TKA) may offer valuable insights into addressing deficits in ankle joint power generation and calf muscle atrophy. Studies on TKA have demonstrated that implementing preoperative muscle strengthening and protein supplementation can enhance postoperative outcomes.15,24,37 Preoperative rehabilitation programs have been shown to improve quadriceps strength at 3 months, reduce postoperative pain at 6 months, and enhance knee RoM at 1 and 3 months, as well as improve postoperative walking endurance.17,37 Furthermore, studies have shown that protein supplementation may decrease muscle atrophy after TKA. 30 However, the long-term benefits of these interventions remain to be fully investigated. Although direct evidence is lacking for TAA, the benefits observed in TKA suggest that it is therefore reasonable to hypothesize that prehabilitation and targeted nutritional support could benefit TAA patients by mitigating calf muscle atrophy and strength deficits. However, more research is needed to validate this practical approach.
The findings of this study should be considered in the context of several limitations. A first limitation was the inability to isolate the true ankle (talo-crural) mechanics from the subtalar joint due to the current limitations of multi-segment foot models. To address this challenge, previous studies have employed techniques involving bone-anchored markers and biplanar videoradiography in an attempt to provide more accurate measures of isolated ankle joint motion.21,25,29,39 However, it should be noted that the invasive or ionising nature of these alternative methods precludes their applicability for routine clinical gait analysis. A second limitation was the limited sample size and lack of asymptomatic control subjects. However, a matching procedure between the groups was performed in order to control for confounding variables such as walking speed, age, gender, and BMI, which may have affected the kinematic and kinetic outcome variables. 4 A third limitation was the lack of control over the interventions completed during the rehabilitation process between the 2 groups. Future studies should investigate whether specialized rehabilitation programs, which prioritize the restoration of ankle joint mobility through passive and active exercise, as well as the enhancement of muscle force production with fast high-intensity resistance training, could facilitate improvements in ankle mechanics for the PFOA group, bringing them to the level of the PSOA group. 27 A primary limitation is the small, matched sample without asymptomatic controls; deformity type (varus/valgus) was intentionally not matched and may confound postoperative mechanics by etiology. This methodological choice may introduce a potential confounding effect, as differences in baseline alignment could influence postoperative ankle mechanics independently of the osteoarthritis etiology. Although the decision was deliberate to preserve key biomechanical distinctions between the groups, it may reduce comparability in terms of deformity-related outcomes.
In conclusion, the outcomes of this prospective study seem to support the hypothesis that patients sustaining PFOA have lesser improvements in ankle (Shank-Calcaneus) joint moment, power, and work during gait after TAA compared with patients sustaining PSOA. Considering the limited postoperative gains observed in PFOA patients, prehabilitation and targeted nutritional support warrant prospective evaluation and may help mitigate calf muscle atrophy and strength deficits in selected patients.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007251387708 – Supplemental material for Are There Differences in Ankle Mechanics After Total Ankle Arthroplasty in Patients Suffering From Post-fracture vs Post-sprain End-Stage Ankle Osteoarthritis?
Supplemental material, sj-pdf-1-fai-10.1177_10711007251387708 for Are There Differences in Ankle Mechanics After Total Ankle Arthroplasty in Patients Suffering From Post-fracture vs Post-sprain End-Stage Ankle Osteoarthritis? by Arnaud Delafontaine, Alexandre Naaim, Thibaut Leemrijse, Laurence Chèze, Raphaël Dumas, Bernhard Devos Bevernage, Jean-Luc Besse, Ivan Birch, Corentin Malherbe and Paul-André Deleu in Foot & Ankle International
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the Academic Ethical Committee Brussels Alliance for Research and Higher Education (Approval Number: B200-2017-061).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the Belgische Vereniging voor Orthopedie en Traumatologie (BVOT) research Grant (BDB 2017/12), Fund Moïse & Paul Blaimont (managed by the King Baudouin Foundation), and the FONDATION CARE (Chirec). The sponsors had no involvement in the writing of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
The data sets generated during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.