
Abstract
Background
To date, most reference data on foot and ankle morphology are derived from Western cohorts, potentially overlooking significant ethnic variation in Asian population. This study utilized 3D weight-bearing computed tomography (WBCT) to establish population-specific reference values of 3D foot and ankle parameters for a Korean cohort and compare these values with published European data.
Methods
This retrospective, cross-sectional study analyzed the asymptomatic contralateral feet of 39 Korean adults (≥18 years old) using WBCT under natural weight-bearing conditions. Automated 3D measurements—including Meary, talonavicular, and Saltzman view angles—were calculated across sagittal, axial, and coronal planes. Results were compared to a published European cohort (n = 100) using Welch t test. For the subgroup analysis, an independent sample t test was used to compare the parameters between male and female participants within the Korean cohort. Pearson correlation analysis was performed to assess the relationship between age and the measured foot parameters.
Results
Statistically significant differences were observed in 18 of the measured parameters between the Korean and European cohorts. The Korean cohort showed a significantly lower sagittal Meary angle, higher talonavicular angle, and lower Saltzman view angle than European data. Analysis of the Korean cohort revealed no significant sex-based differences across most 3D WBCT parameters, except for the sagittal third tarsometatarsal angle. Age was positively correlated with axial Meary angle, Saltzman view angle, and hallux valgus angle.
Conclusion
This study provides preliminary 3D WBCT reference values for the adult Korean foot and ankle. The distinct morphologic variations observed between Korean and European populations underscore the need for ethnic-specific reference values. These findings provide a foundational 3D metric for clinical diagnosis and surgical planning in East Asian populations.
This is a visual representation of the abstract.
Introduction
The precise evaluation of foot and ankle anatomy is fundamental for effective diagnosis, meticulous preoperative planning, and objective postoperative assessment of foot and ankle disease.1,2 To date, most reference data on foot and ankle morphology have been derived from Western cohorts, potentially overlooking significant ethnic variations in Asian populations. 3 However, foot and ankle anthropometrics exhibit significant variability across ethnic groups.
Morphologic characteristics, including bone dimensions, articular geometry, and alignment angles, can differ between Asian, Caucasian, African, and other populations. 4 Specifically, studies have suggested distinct features in foot and ankle morphometry within East Asian populations, including Korean individuals, compared to Western cohorts.5,6 Previous research has indicated that the Korean population tends to have a lower medial arch and a higher prevalence of flatfoot compared to Western populations. 7 Furthermore, morphometric analyses have shown that Koreans often exhibit a more varus orientation of the distal tibia, which may influence the development of specific degenerative patterns like medial ankle osteoarthritis. 5 Therefore, normative data established predominantly from Western populations, or studies focused on pathologic cohorts, may not be used as standard reference for preoperative planning or foot and ankle research in Korean or Asian population. The generation of population-specific normative databases using defined analytical methodologies is thus imperative for evidence-based clinical practice and for advancing orthopaedic research within specific ethnic groups.
For decades, weight-bearing 2-dimensional (2D) radiography has served as the conventional imaging standard of foot and ankle analysis, providing essential data on bone alignment.8,9 However, the 2D radiography presents significant limitations, including the superimposition of structures that complicates assessment of the hindfoot and midfoot, and an inability to accurately quantify rotational deformities or true 3-dimensional (3D) spatial relationships.10,11 These limitations compromise diagnostic accuracy and the precision of surgical treatment.
Weight-bearing computed tomography (WBCT) has emerged as a vital diagnostic tool, garnering significant interest in the field of foot and ankle surgery,12,13 overcoming the limitations of conventional CT by capturing 3D volumetric data sets under natural physiological loading.13,14 By enabling the visualization of complex multiplanar deformities and articular congruity with enhanced fidelity,15,16 WBCT improves our understanding of pathomechanics and the precision of treatments for conditions such as progressive collapsing foot deformity and hallux valgus. 17 To extract meaningful data from these rich data sets, specialized software has been developed for the semiautomated segmentation of bone and calculation of 3D axes. The reliability of these 3D measurements has proven superior to traditional 2D radiography. 18 For instance, Kvarda et al 10 reported higher reliability for key ankle parameters, whereas Sangoi et al 9 demonstrated that semiautomated 3D analysis more accurately characterizes complex rotational deformities. Despite these advancements, the clinical interpretation of 3D software analysis remains contingent on the availability of robust normative data.
However, to date, a comprehensive set of normative foot and ankle parameters for a Korean or Asian population has not yet been established. This knowledge gap limits the full clinical utility of WBCT analysis in this demographic. Therefore, the primary objective of this study was to establish population-specific reference values using 3D WBCT for an asymptomatic Korean cohort and compare them with established European data. Additionally, we aimed to evaluate the influence of sex and age on these 3D parameters to provide a more detailed understanding of population-specific anatomical characteristics.
Methods
Study Design and Patient Selection
This retrospective, cross-sectional study was approved by the institutional review board of our institution. From August 2024 and April 2025, patients who visited our outpatient clinic for the treatment of foot and ankle diseases or trauma and underwent WBCT examination were included in the study. WBCT was performed on both feet and ankles, and only normal contralateral feet without trauma, deformity, or other pathologic conditions were included for the semiautomated 3D analysis. Exclusion criteria included age <18 years, any history of trauma or surgery, congenital or acquired deformities of the contralateral foot and ankle, and insufficient radiographic data. A fellowship-trained foot and ankle surgeon with 10 years of experience reviewed all WBCT images to confirm the absence of any apparent clinical deformity. Initially, 61 patients were included in the study. However, 10 pediatric patients, 5 patients with hallux valgus, 2 patients who had undergone hallux valgus surgery, 2 patients with flatfoot, and 3 patients with insufficient imaging data were excluded. Consequently, a total of 39 patients’ feet were ultimately included in the final analysis (Figure 1). The demographics including sex, age, and diagnosis of the participants were evaluated by reviewing the patients’ electronic medical records. The primary clinical diagnoses of the symptomatic index-side pathologies included ankle or foot fracture (n = 17), hallux valgus (n = 5), ankle sprain (n = 5), implant removal (n = 3), os navicular (n = 3), metatarsalgia (n = 3), plantar fasciitis (n = 1), bunionette (n = 1), and ankle arthritis (n = 1).
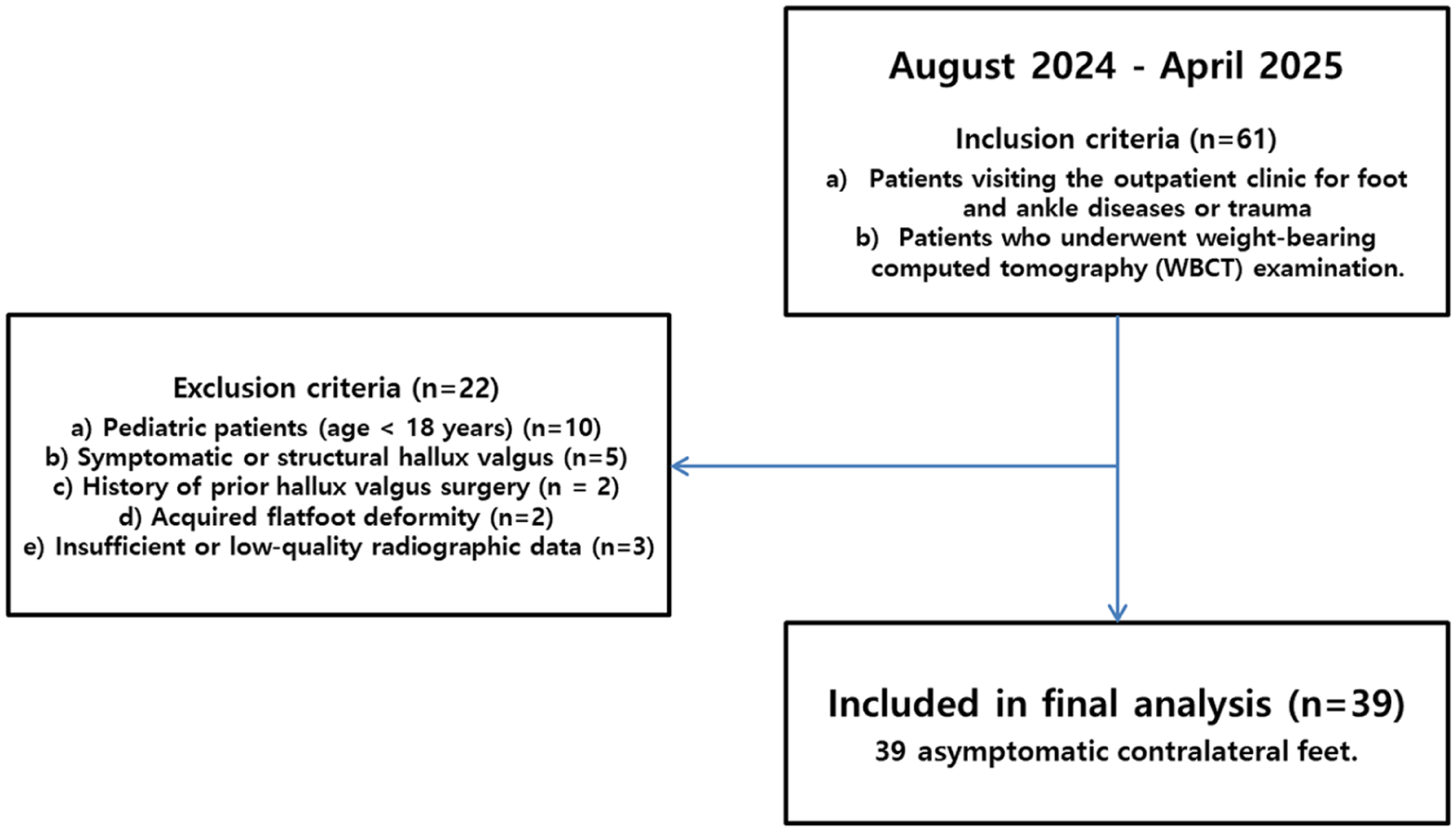
Flow diagram of participant enrollment and selection.
Radiographic Evaluation
For image acquisition, each patient underwent 3D WBCT scans (Genoss®, Suwon, South Korea) and conventional weight-bearing radiographs of both feet and ankles. Standardized patient positioning was maintained for all WBCT scans to ensure consistent and reproducible results. As illustrated in Figure 2A, patients were instructed to stand within the gantry in a natural, upright, double-leg weight-bearing position with their weight distributed equally between both feet. The WBCT scans were performed ensuring that images were captured under natural physiological weight-bearing conditions. Standard 2D radiographic views, including anteroposterior, lateral foot and ankle radiographs, were obtained following established protocols. To obtain normative values from semiautomated 3D measurements of WBCT scans, the raw DICOM data from each WBCT scan (axial image slice < 0.7 mm) were analyzed using the FDA-approved automated software (Bonelogic version 2.1, DISIOR).2,11 The software has previously been validated and shown to have high reliability in foot and ankle research.9,10 After manual identification and registration of each bone, the program generated interaxis angular measurements automatically for the 3D evaluation of sagittal, axial, and coronal alignment. A total of 18 foot and ankle parameters were analyzed and categorized, in accordance with previously published literature, into the following groups: hindfoot-forefoot relationship, hindfoot alignment angles, coronal plane relations, intra-forefoot relationships, and tarsometatarsal relationships. 2 Hindfoot sagittal alignment was assessed using the sagittal Meary angle and the calcaneal inclination angle. To evaluate hindfoot alignment in the axial and coronal planes, the talonavicular angle (TNA), axial Meary angle, talar tilt, and Saltzman view angle were analyzed. An experienced orthopaedic surgeon who was not involved in clinical treatment performed the semiautomated 3D measurements of WBCT scans (Figure 2). After acquiring the normative values from the Korean participants in the present study, these data were compared with previously published normative values from European populations. 2 In addition, subgroup analyses were performed among the participants to assess sex-based differences in the measured parameters, as well as to evaluate the correlations between age and foot parameters.
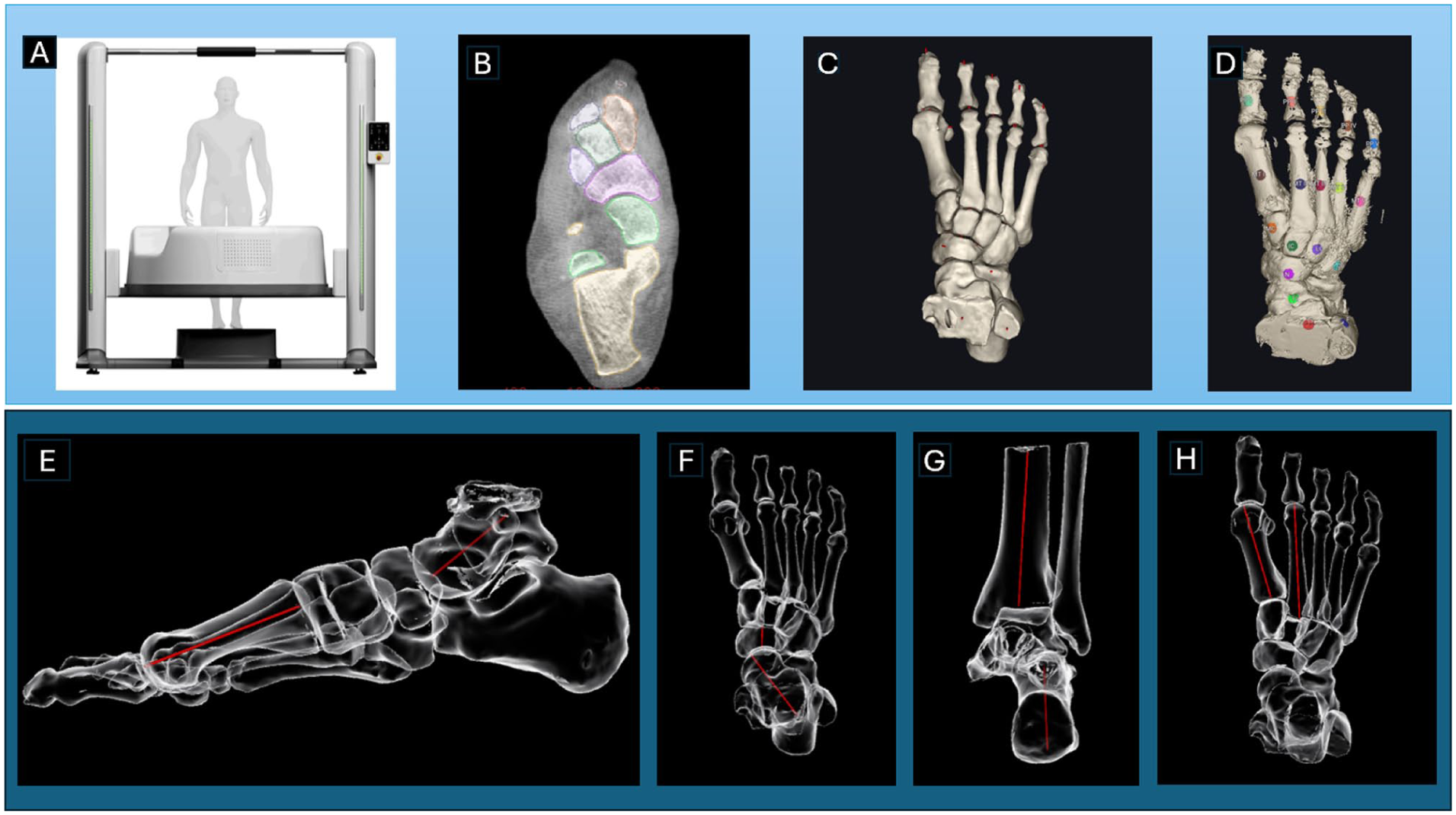
Overview of the study workflow and 3D analysis methodology. (A) Weight-bearing CT image scan of contralateral normal foot of the patient. (B) DICOM file download of axial images raw data (<0.7-mm slice). (C) Reconstructed 3D CT image. (D) Manual identification and registration of each bone using 3D software. Generation of interaxis angular measurements automatically for the 3D evaluation of (E) sagittal Meary angle, (F) talonavicular angle, (G) Saltzman view angle, and (H) first-second intermetatarsal angle. CT, computed tomography.
Statistical Analysis
Statistical analyses were performed with SPSS, version 22, for Windows (IBM Corp). The normality of the data was assessed using the Shapiro-Wilk test. To demonstrate the statistical precision and reliability of the established 3D parameters, 95% CIs were calculated for all normative values and mean differences. Although the primary comparison between ethnic cohorts was sufficiently powered, the subgroup analysis comparing male (n = 12) and female (n = 27) participants within the Korean cohort was exploratory. Given the smaller sample size of the male subgroup, this specific analysis may have limited statistical power to detect sex-based differences. Statistical analysis was performed with the presentation of descriptive statistics, including the mean values, SDs, and 95% CIs, for each measured parameter. For the comparative analysis, Welch t test was used to compare the mean values of the parameters obtained from the Korean cohort and European cohorts. To quantify the magnitude of the differences between these cohorts, effect sizes were calculated using Cohen d. An independent samples t test was used to compare the parameters between male and female participants within the Korean cohort. Pearson correlation analysis was performed to assess the relationship between age (years) and the measured foot parameters. P <.05 was considered statistically significant.
Results
General Characteristics of Korean Cohort
A total of 39 feet were analyzed from 39 adult patients. The mean age of the participants was 45.56 ± 16.67 years. In the cohort, 27 patients (69.23%) were female and 12 patients (30.77%) were male. After acquisition of the WBCT scans, the images were semiautomatically analyzed in the sagittal, axial, and coronal planes, yielding measurements for 18 foot and ankle parameters.
Comparison of 3D WBCT Parameters Between Korean vs European Cohorts
The comparison of 3D WBCT parameters between the Korean cohort (n = 39) and the published European cohort (n = 100) revealed statistically significant differences in multiple parameters (Table 1). The mean sagittal Meary angle in the Korean group (−12.20° ± 7.67°) was significantly lower than the European mean (−4.26° ± 6.06°) (P < .001). Axial TNA in the Korean cohort (40.67° ± 7.07°) was significantly higher compared to the European cohort (30.75° ± 8.23°) (P < .001). The 20° Saltzman view angle of Korean mean (−0.13° ± 9.11°) was significantly lower than that of the European mean (9.08 ± 6.43, P < .001)
Comparison of Foot and Ankle Measurements Between Korean and European Cohorts.
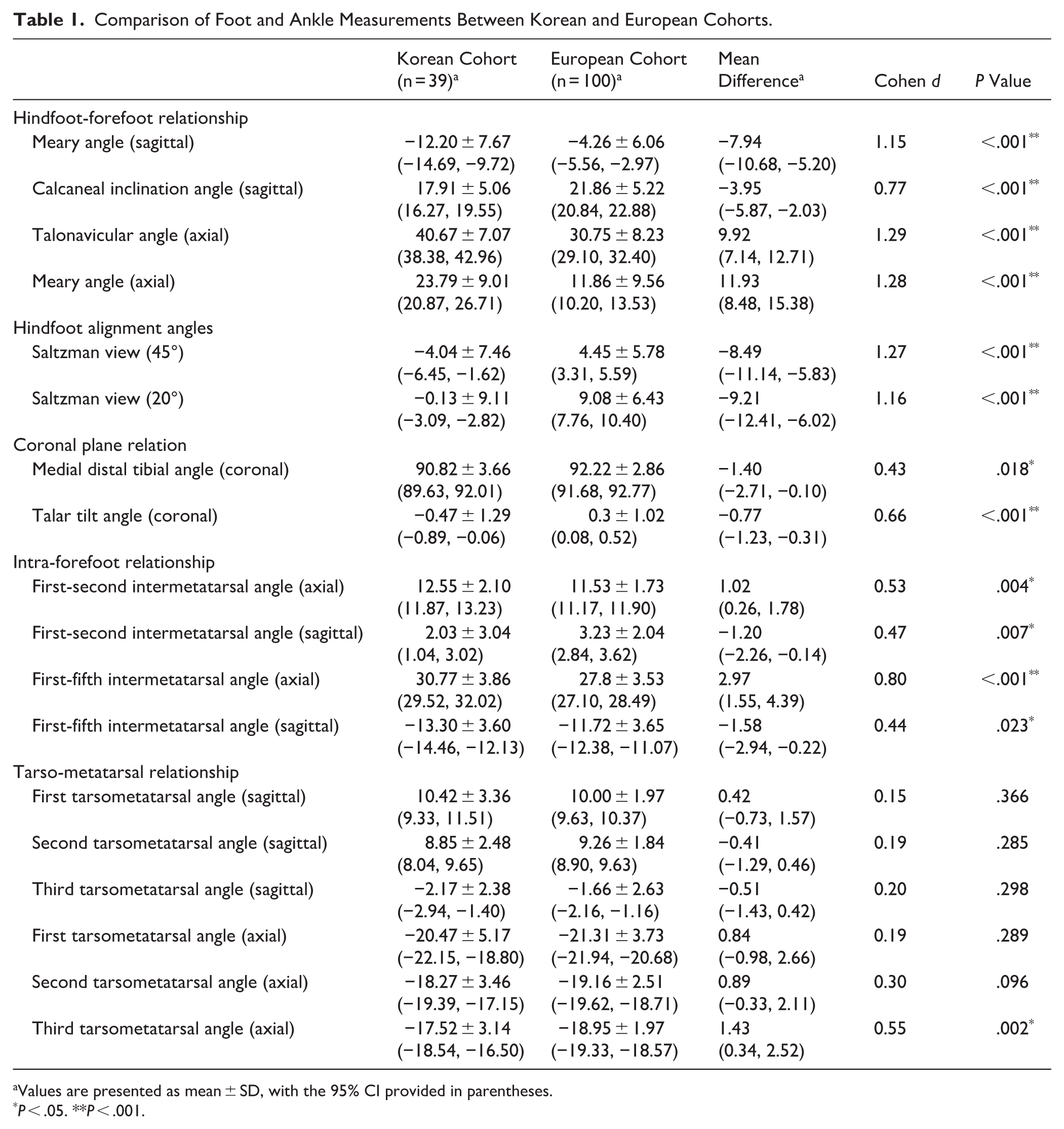
Values are presented as mean ± SD, with the 95% CI provided in parentheses.
P < .05. **P < .001.
Significant differences were found in the coronal plane relation for the medial distal tibial angle (90.82 ± 3.66° vs 92.22 ± 2.86°, P = .018) and talar tilt angle (−0.47 ± 1.29° vs 0.3 ± 1.02°, P < .001). In the intra-forefoot relationship, all axial and sagittal intermetatarsal angles (first-second and first-fifth) were significantly different (P < .005) between the 2 groups. In the tarso-metatarsal relationship, only the axial third tarsometatarsal angle showed a significant difference (P = .002).
Comparison of 3D WBCT Parameters by Sex (Korean Cohort)
The comparison of 3D WBCT data between male and female participants within the Korean cohort revealed comparable results in most parameters (Table 2). The sagittal third tarsometatarsal angle was only parameter which showed significant difference (P = .036). The mean sagittal third tarsometatarsal angle for males was −3.35° ± 2.70°, which was significantly lower (more plantarflexed) than the mean for females (−1.64° ± 2.06°). All other measured parameters did not show statistically significant differences based on sex (P > .05).
Comparison of Foot and Ankle Measurements by Sex (n = 39).
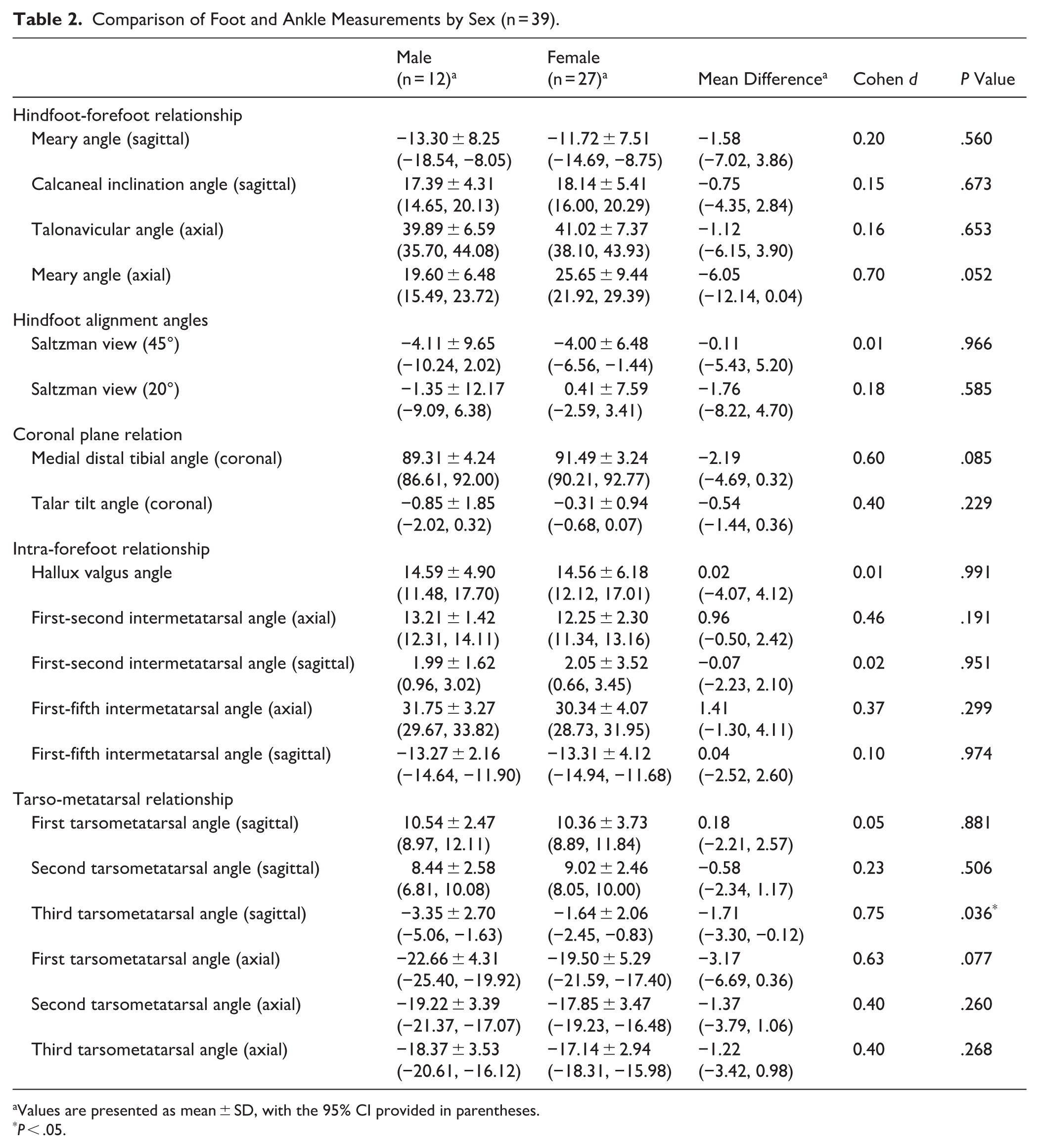
Values are presented as mean ± SD, with the 95% CI provided in parentheses.
P < .05.
Correlation Analysis Between Age and Foot, Ankle Parameters
Pearson correlation analysis revealed that age was significantly correlated with 4 of the measured foot and ankle parameters (Table 3). The significant positive correlations were observed for axial Meary angle (r = .331, P < .05), 45° Saltzman view (r = 0.345, P < .05), 20° Saltzman view angle (r = 0.422, P < .01), and hallux valgus angle (r = 0.368, P < .05). No other parameters showed a statistically significant correlation with age (P > .05).
Correlation Analysis Between Age and Foot and Ankle Parameters (n = 39).
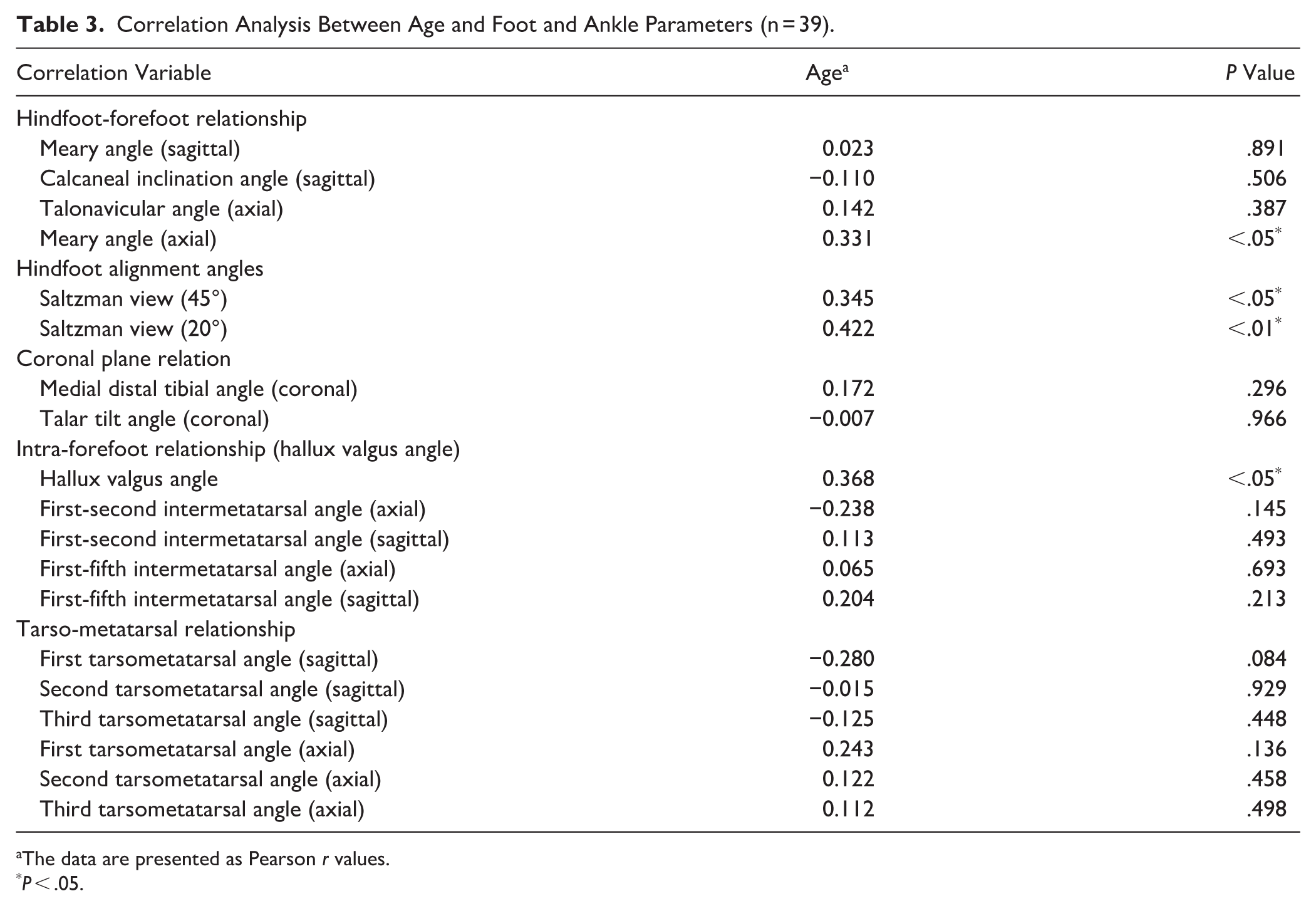
The data are presented as Pearson r values.
P < .05.
Discussions
The most important finding of this study is the presence of distinct morphologic differences between Korean and European populations in the sagittal, axial, and coronal planes of the foot and ankle. These results support our hypothesis regarding the necessity of establishing population-specific anatomical standards for the application of 3D morphometry in East Asian orthopaedic research and clinical practice.
Previous study by Zaidi et al 2 established a comprehensive normative database for the foot and ankle in a cohort of 100 asymptomatic European individuals using semiautomated 3D measurements of WBCT scans. This study provided critical baseline values for various sagittal, axial, and coronal parameters, offering a standard reference for characterizing normal 3D foot morphology in western populations. Building on this foundation, a recent study by Song et al 11 used the similar semiautomated 3D analysis to evaluate pre- and postoperative WBCT images of patients with CMT disease. By comparing these results with the normative European data established, they demonstrated that joint-sparing surgery could effectively restore foot alignment to levels that showed comparable results from the European mean.2,11 These studies highlight a significant shift in the current research trend: the clinical utility of WBCT-based 3D analysis is maximized when pathologic data are compared against population-specific normative values, enabling more profound and advanced orthopaedic insights.
The comparative analysis across the sagittal, axial, and coronal planes revealed a fundamental and consistent distinction in the native osseous alignment of the Korean foot and ankle. It is noteworthy that the Korean cohort demonstrated a significantly lower sagittal Meary angle, higher TNA, and lower Saltzman view angle compared to European cohort. These parameters indicate lower longitudinal arch, forefoot abduction, and hindfoot valgus, respectively in the Korean cohort compared to European cohort. Taken together, the present data suggests that the asymptomatic Korean foot exhibits a greater tendency toward flat foot (but not progressive collapsing foot deformity) compared with its European counterpart under physiological loading (Figure 3). These findings are consistent with previous anthropometric studies suggesting that East Asian populations generally possess lower arch profiles and broader foot shapes than Caucasian populations. 18 The divergence in 3D alignment between these ethnic groups might be associated with a combination of genetic factors and environmental influences, particularly lifestyle habits. 19 For instance, unlike Western cultures where footwear is commonly worn indoors, the traditional Korean or Asian lifestyle involves barefoot indoor activities and floor-seated postures. 20 Such prolonged weight-bearing without the structural support of shoes, combined with repetitive kneeling or cross-legged sitting, may influence the ligamentous laxity and the progressive remodeling of the foot’s bony architecture over time. 21 Furthermore, differences in historical physical activity levels and footwear design preferences between the 2 regions may have contributed to these distinct morphotypes. 18
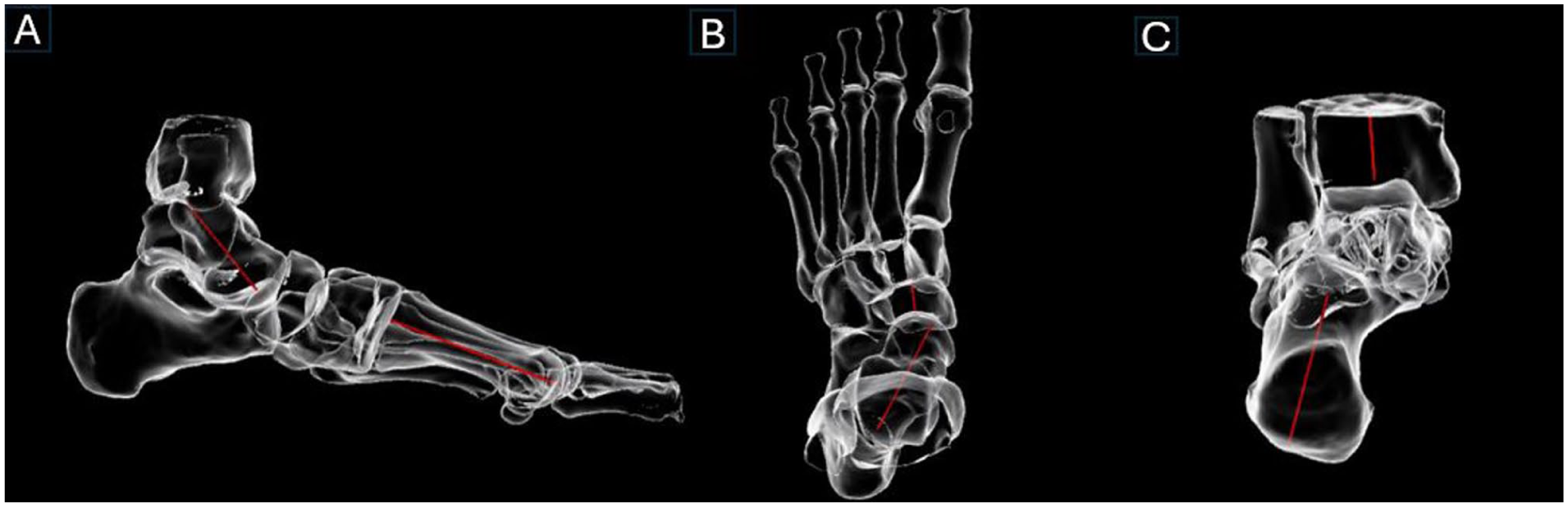
Three-dimensional weight-bearing CT images of 21-year-old male patients from the Korean cohort were analyzed using 3D software. The images demonstrated a (A) low sagittal Meary angle, (B) an increased talonavicular angle, and (C) a decreased Saltzman view angle, indicating a reduced longitudinal arch, forefoot abduction, and hindfoot valgus alignment.
Key parameters in the coronal plane, such as the medial distal tibial angle and talar tilt angle, also showed statistically significant differences. The Korean cohort exhibited greater distal tibial varus than that of the European cohort. This finding is consistent with previous epidemiologic studies reporting a higher prevalence of varus-type ankle osteoarthritis in East Asian populations compared with Western cohorts. 22 This suggests that the native alignment of the Korean ankle is inherently more predisposed to medial compartment loading, which may influence the progression of degenerative changes. 23 The Korean cohort exhibited greater valgus talar tilt than that of the European cohort. We presume that, because Korean tend to exhibit a greater predisposition toward pes planus compared with Europeans, this anatomical characteristic may be associated with a stronger tendency toward greater valgus talar tilt. Overall, our data demonstrates that the distal tibia and talus assume a unique multiplanar orientation within the tibiotalar joint in the Korean cohort, which is essential for preoperative planning in cases of ankle deformity or instability.
Furthermore, the mean axial first-fifth intermetatarsal angle of the Korean cohort was significantly larger than the European cohort, indicating a greater physiological forefoot spread or splay. This finding has critical implications for reconstructive procedures, particularly for hallux valgus correction surgery. For instance, a Korean patient with a naturally wide forefoot may require a different surgical goal compared with a European patient to avoid overcorrection or undercorrection of the deformity. 24
The analysis of sex differences within the Korean cohort revealed remarkable uniformity between males and females. Only the sagittal third tarsometatarsal angle demonstrated a significant difference—being more plantarflexed in males than in females—a finding that appears clinically insignificant. However, the analysis of aging effects showed compelling evidence for dynamic changes in osseous alignment over time. Age was positively correlated with the axial Meary angle, Saltzman view angles, and hallux valgus angle. This indicates a generalized tendency toward greater forefoot abduction, hindfoot varus, and hallux valgus progression with increasing chronological age, even in individuals without overt symptoms. 25 Further investigation is warranted to clarify the precise etiologic factors underlying these age-related changes in foot morphology, including whether they are attributable to prolonged use of specific types of footwear or to habitual barefoot walking. In addition, it is necessary to analyze the clinical implications of these age-related morphologic changes in the foot and to determine their relevance to aging from a clinical perspective. This age-related morphologic drift must be incorporated into the clinical interpretation of WBCT measurements, reinforcing the principle that assessment of deformity might be normalized against both ethnic- and age-matched values. 26
This study has several strengths. To our knowledge, this is the first study to establish a population-specific reference value for the asymptomatic Korean foot and ankle using a semiautomated 3D analysis of WBCT scans. By providing multiplanar reference values derived from sophisticated 3D methodology, our findings offer a vital standard for future WBCT-based research, not only for the Korean population but also for the broader East Asian demographic. Furthermore, this is the first investigation to directly compare 3D WBCT morphologic data between Korean and European cohorts, revealing significant ethnic variations. These results highlight the limitations of applying western-centric normative data to Asian patients and provide a scientific foundation for more precise, population-specific diagnostic and treatment planning.
This study has several limitations. First, internal reliability was not assessed for this specific data set, acknowledging that software validation does not eliminate operator-dependent error in landmark selection. Second, we could not statistically compare age, sex, or BMI distributions with the European cohort, which could act as a confounder for the observed ethnic differences. Third, the inclusion of contralateral feet from patients with unilateral pathologies (eg, hallux valgus) warrants caution, although radiographic screening confirmed no signs of deformity.
The external validity is also restricted because the sample consisted of a relatively small number of patients from a single tertiary hospital, which introduces the possibility of selection bias. Accordingly, it must be emphasized that these results should not be directly extended or generalized to the “real normative value” of the wider Korean or Asian populations. Instead, they should be interpreted as population-specific reference values derived from asymptomatic contralateral feet within a clinical cohort. Although statistically significant differences were found between Korean and European, a larger, multicenter cohort is needed for enhanced statistical power and more robust determination of narrow CIs. Our subgroup analysis regarding sex-based differences was limited by insufficient statistical power. Because of the relatively small number of subgroup participants, we cannot definitively conclude that no morphologic differences exist between Korean males and females. Furthermore, as the software is highly automated and minimizes observer-related variability, 5 we relied on previously validated reliability benchmarks rather than performing an intraclass correlation coefficient analysis in the current study. Also, given the multiple comparisons performed across various 3D parameters, the findings should be interpreted cautiously because of the potential risk of type I error. Finally, a significant limitation of this study is the absence of clinical and symptomatic correlation, because our analysis was limited to radiologic parameters obtained from WBCT scans. Although we identified clear ethnic differences in foot and ankle morphology, we did not evaluate them and how they parameters may relate to symptom severity, functional outcomes, or their implications for preoperative planning.
Conclusion
This study provides preliminary 3D WBCT reference values for the adult Korean foot and ankle. The results suggest distinct morphologic patterns compared to European cohorts, highlighting a tendency toward a lower medial longitudinal arch and greater forefoot abduction. The most significant contribution of this study is the provision of these initial reference values, which may serve as a baseline for future WBCT-based foot and ankle research, not only for the Korean population but also potentially for the broader East Asian population.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007261435466 – Supplemental material for Semiautomated Weight-Bearing CT-Based 3D Analysis of Normal Foot and Ankle in a Korean Population: A Comparison With European Data
Supplemental material, sj-pdf-1-fai-10.1177_10711007261435466 for Semiautomated Weight-Bearing CT-Based 3D Analysis of Normal Foot and Ankle in a Korean Population: A Comparison With European Data by Sung-Jun Moon, Eun Soo Park, Chan Kang, Min-Gi Jeong and Jae Hwang Song in Foot & Ankle International
Footnotes
Acknowledgements
We would like to thank Sangkil Kim, the CEO of the Genoss Co, for supporting the study.
Author Note
The investigation was performed at the Department of Orthopaedic Surgery, Konyang University Hospital, Daejeon, South Korea
Ethical Considerations
Ethical approval for this study was obtained from the Konyang University Hospital Institutional Review Board (KYUH 2025-05-013).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.