
Abstract
Background
Next-generation DNA sequencing (NGS) has improved detection of bacterial species and expanded understanding of the microbiome’s influence on postoperative outcomes in orthopaedic patients. Although NGS has identified organisms linked to reoperations in shoulder surgery, its application in the foot and ankle remains unexplored. This study uses NGS to determine whether patients undergoing hardware removal exhibit a unique microbiome profile.
Methods:
A prospective study recruited 34 patients undergoing hardware removal surgery from the foot or ankle during 2020-2023. Patients were excluded based on any concern for infection prior to surgery. During the operation, the surgeon collected the removed hardware for analysis at a CLIA (Clinical Laboratory Improvement Amendments of 1988)–licensed molecular diagnostic laboratory. Majority of patients underwent surgery for painful orthopaedic hardware (70.6%). The cohort was predominantly female (62.2%) and mean age was 53.3 years (range 17-78). The mean time from primary implantation to hardware removal was 40.1 months (range 2.8-276.6 months).
Results
NGS identified bacterial DNA in 5 cases (14.7%), detecting 9 total organisms. Staphylococcus species were most common (44.4%), followed by Corynebacterium (22.2%). No significant associations were found between bacterial detection and patient demographics or with hardware removal performed for painful implants.
Conclusion:
This study found no consistent microbiome among patients undergoing hardware removal surgery, with Staphylococcus species being the most frequently detected organisms. These preliminary findings suggest that foot and ankle hardware does not consistently harbor bacteria detectable by NGS, although the small sample size limits generalizability and further investigation is warranted.
This is a visual representation of the abstract.
Introduction
Orthopaedic hardware removal is a common procedure performed for pain, mechanical irritation, or concern for occult infection, yet the microbial environment of explanted foot and ankle implants remains largely unknown. Next-generation sequencing (NGS) is an innovative technology that advances infection diagnosis and management. Unlike traditional culture-based methods, NGS processes all DNA present in a sample, allowing for detection of a wide range of bacterial and fungal organisms.
NGS has been used in previous studies to analyze the microbiomes associated with various types of infected and aseptic orthopaedic implants, including joint arthroplasty in the hip, shoulder, and knee.1 -3 Additionally, a recent study by Hoch et al 4 examining the microbiome of ankles undergoing arthroplasty or arthrodesis has identified Cutibacterium acnes and staphylococci as the most commonly native bacteria in the ankle joint. Bacterial colonization of implants has been shown to cause complications necessitating removal of orthopaedic hardware, including postoperative infections, pain and stiffness at the implant site, loosening of the implant, and device failure. 5
Despite growing interest in orthopaedic microbiome research, no studies to date have investigated the microbiome associated with explanted foot and ankle hardware. These procedures are common and often performed for pain, mechanical irritation, or suspicion of occult infection, yet the microbial environment of these implants remains largely unknown. The aim of this study is to describe the microbial profile of orthopaedic hardware removed from the foot and ankle using NGS, as a preliminary step toward understanding the microbiome of this anatomical region.
Methods
After institutional review board (IRB) approval, a prospective study enrolled 34 patients undergoing foot or ankle hardware removal between January 2021 and February 2023 with one of 2 fellowship-trained orthopaedic foot and ankle surgeons at a single academic medical center. Patients were included based on undergoing removal of hardware from the foot or ankle, identified via Current Procedural Terminology (CPT) code 20680. Patients were excluded if they had preoperative concern for infection, were under 18 years of age at the time of surgery, or were non–English speaking. Any concern for preoperative infection was evaluated with erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) laboratory testing, with normal values taken to exclude infection without other obvious evidence to the contrary (such as a drainage wound or open sinus tract).
Surgical site preparation followed a standardized aseptic protocol. Initial decontamination consisted of a thorough wash using 4% chlorhexidine gluconate, followed by 70% isopropyl alcohol. Subsequently, the site was treated with 2 antiseptic applicators containing a solution of 2% chlorhexidine gluconate in 70% isopropyl alcohol before sterile draping was performed. Following sterile preparation, hardware location was identified via fluoroscopy and removed. In all surgeries, adjacent bone cultures were obtained to serve as an internal control and confirm the absence of underlying osteomyelitis. The removed hardware (n = 34) was then sent to MicroGen Diagnostics for NGS.
Retrospective Data Collection
Retrospective chart review captured demographics, comorbidities, surgical indications, postoperative complications, 90-day readmissions, and reoperations. Demographics included age, BMI, sex, race, smoking status, and pack-year history. Most patients underwent hardware removal for pain (70.6%). The cohort was predominantly female (62.2%) and White (62.2%). Mean age was 53.3 years (range 17-78), mean BMI was 31.1 (range 19.0-49.7), and mean follow-up was 16.4 months (range 0.59-51.4). The mean time from primary implantation to hardware removal was 40.1 months (range 2.8-276.6 months).
Data Analysis
Statistical analyses were performed using IBM SPSS Statistics, version 27.0. Pearson correlation assessed associations between continuous variables. Group comparisons were conducted using 2-tailed Student t tests or χ2 tests, with Fisher exact test applied when χ2 assumptions were violated (>20% of expected counts <5). Statistical significance was set at P = .05.
Results
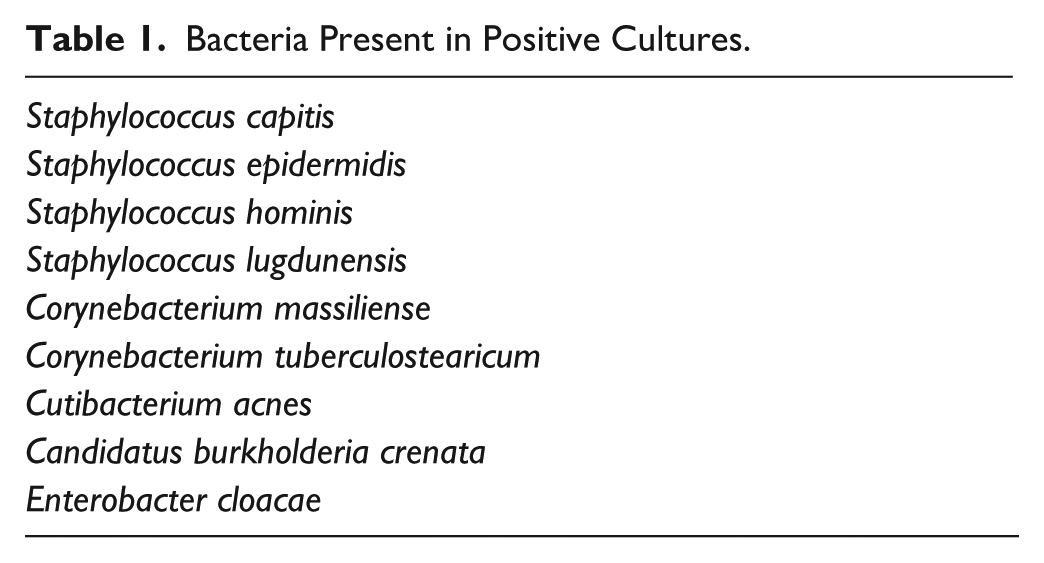
Of the 34 samples submitted for NGS, 5 (14.7%) tested positive, yielding a total of 9 bacterial identifications. Conversely, 29 samples (85.3%) showed no bacterial presence. Of the 9 microbes detected, Staphylococcus and Corynebacterium were the most frequent, accounting for 44.4% and 22.2% of the findings, respectively. C acnes was observed in only 1 case. A comprehensive list of the isolated organisms is provided in Table 1. Notably, all concurrent bone cultures remained negative.
Bacteria Present in Positive Cultures.
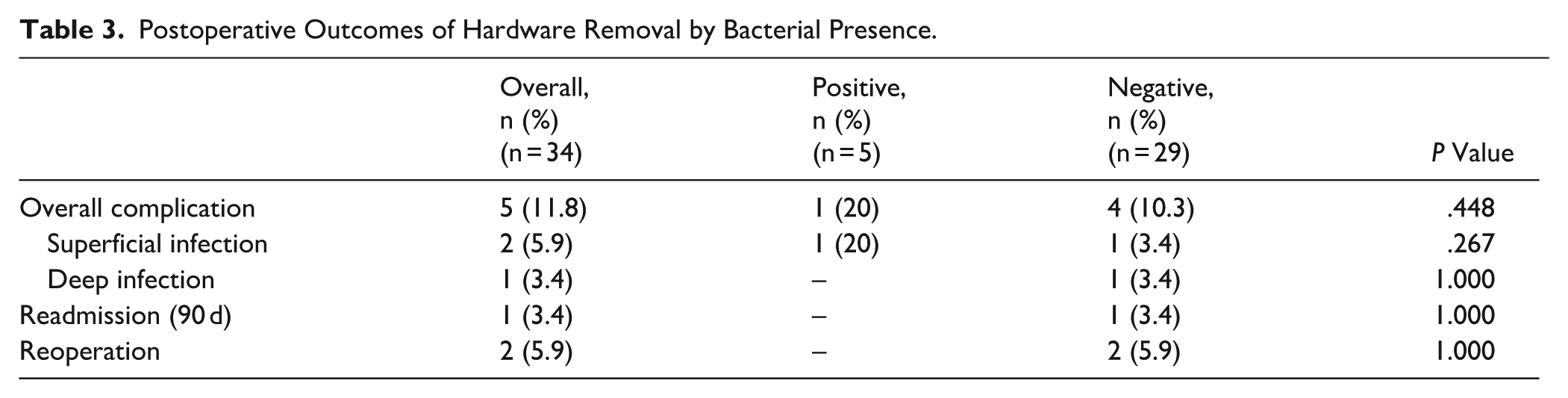
The presence of bacteria did not differ in any demographic or medical comorbidity, including removal due to painful orthopaedic hardware (Table 2). No statistically significant difference in complication rates was detected between NGS-positive and NGS-negative patients (Table 3). For the entire cohort, the overall complication rate was 11.8% (4/34), consisting of superficial infection in 2 cases (5.9%), deep infection in 1 case (2.9%), and one 90-day readmission and reoperation (2.9% each); all complications occurred in NGS-negative patients.
Demographics and Medical Comorbidities Between Subjects Identified as Positive and Negative for Bacteria Presence. a
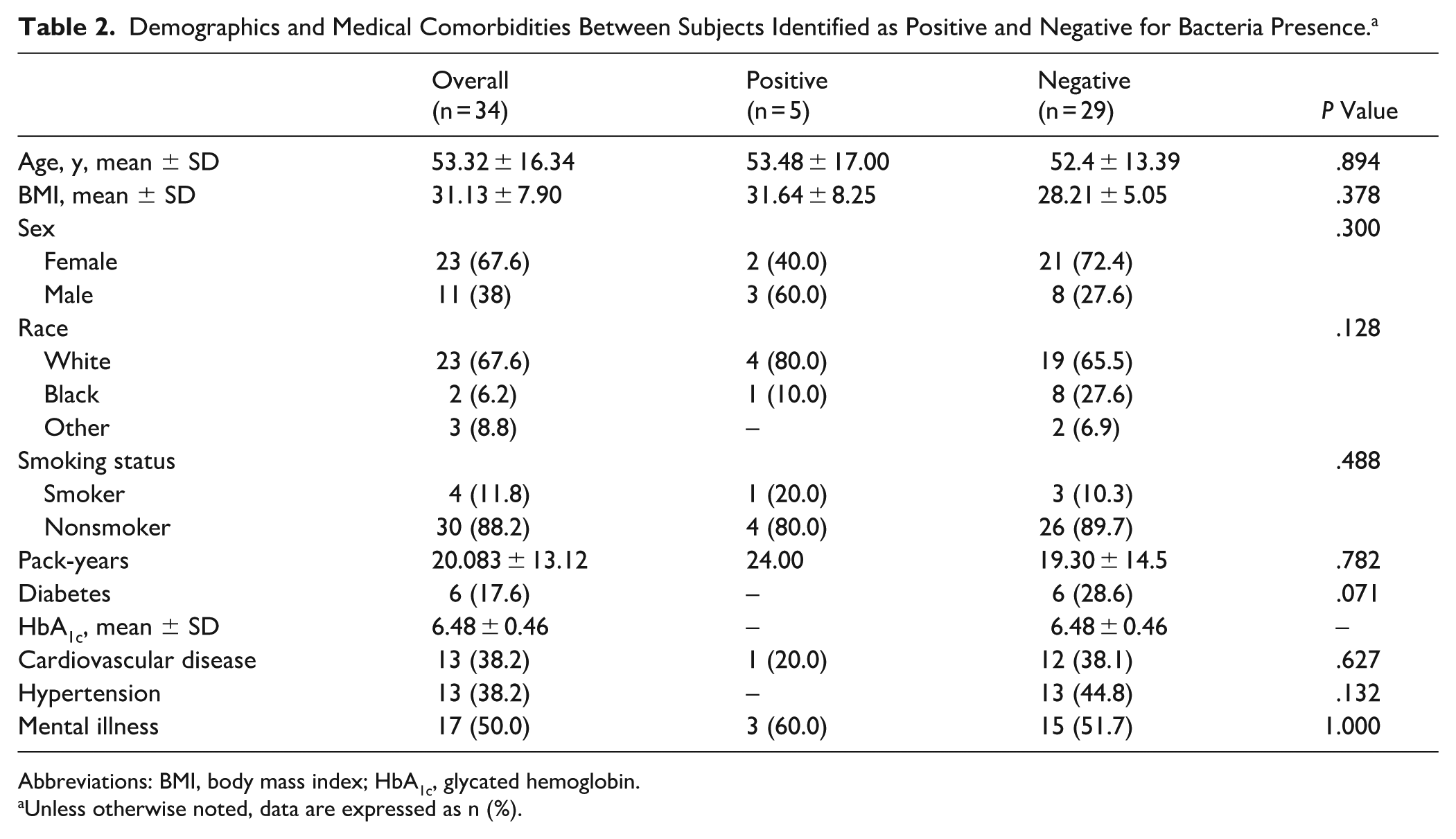
Abbreviations: BMI, body mass index; HbA1c, glycated hemoglobin.
Unless otherwise noted, data are expressed as n (%).
Postoperative Outcomes of Hardware Removal by Bacterial Presence.
Discussion
Our study found no statistically significant association between the microbiome detected on explanted foot and ankle implants and the preoperative indication for hardware removal, including painful hardware. These findings are preliminary and should be interpreted with caution given the small sample size and low number of positive detections, which preclude clinically meaningful conclusions.
A negative NGS result does not necessarily indicate a sterile implant, nor does a positive result confirm infection. As described by Pottinger et al, 6 bacterial sampling from orthopaedic implants occurs in a nonhomogeneous environment, meaning samples from uninvolved areas may yield negative results despite bacterial presence elsewhere on the implant. Furthermore, bacterial detection alone does not equate to infection, particularly in the absence of standardized diagnostic criteria for chronic, low-grade orthopaedic implant infections.
Consistent with prior orthopaedic microbiology studies, coagulase-negative Staphylococcus species were the most frequently identified organisms in our cohort. 7 Additionally, 2 species of Corynebacterium were identified in positive samples in our study. Corynebacterium species have been isolated in other types of orthopaedic infections, although in general they are a far less common cause of orthopaedic infections than staphylococci species.8 -10 C acnes appeared only once, which is expected given its preference for sebaceous skin regions such as the face, chest, and back and its lower prevalence in the lower extremities. 5
Foot and ankle hardware removal remains an understudied area, and this study serves as an initial step toward characterizing the microbiome of orthopaedic implants in this region. Limitations include the small sample size, absence of parallel standard cultures as a control, lack of investigator blinding, and the inherent risk of specimen contamination during hardware collection despite adherence to strict sterile technique. Future studies should enroll larger cohorts, incorporate simultaneous standard cultures alongside NGS, and record the time elapsed between primary implantation and hardware removal to better contextualize microbial findings.
Conclusion
In this preliminary series of 34 patients undergoing foot and ankle hardware removal, NGS identified bacterial DNA in 14.7% of cases. No association was found between bacterial detection and patient demographics or postoperative complications. These findings are exploratory and hypothesis-generating; larger studies with parallel culture controls are needed before any clinical conclusions can be drawn.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007261438460 – Supplemental material for Does Implanted Ankle Hardware Harbor Bacteria? Identification of the Microbial Profile Using Next-Generation DNA Sequencing? A Short Report
Supplemental material, sj-pdf-1-fai-10.1177_10711007261438460 for Does Implanted Ankle Hardware Harbor Bacteria? Identification of the Microbial Profile Using Next-Generation DNA Sequencing? A Short Report by Luke LaRochelle, Joshua L. Morningstar, Caroline Hoch, Solangel Rodriguez Materon, Hana Hashioka, Daniel J. Scott and Christopher E. Gross in Foot & Ankle International
Footnotes
ORCID iDs
Ethical Considerations
This study was reviewed and approved by the Medical University of South Carolina Institutional Review Board via the South Carolina Research eIRB system (IRB approval #Pro00093145) on January 16, 2020.
Consent to Participate
All participants provided written informed consent, including review and signature, prior to study participation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Daniel J. Scott, MD, MBA, is a paid consultant for Metric, Orthofix, Paragon28, Smith & Nephew, and Vilex and receives research support from Arthrex, Orthofix, Paragon28, Stryker, and Vilex. Christopher E. Gross, MD, is a paid consultant for Enovis and Paragon 28 and receives research support from Paragon28 and Stryker. Disclosure forms for all authors are available online.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.