
Abstract
Background:
Patients treated with an Ilizarov external fixator often feature risk factors that impair wound healing such as diabetes, peripheral arterial disease, obesity, and renal insufficiency. A 2-staged approach, with initial bony correction (Kirschner wire or hybrid) followed by delayed Ilizarov application by 5 days, is intended to support wound healing by allowing for reduction of soft tissue swelling and enhancing postoperative wound care. We hypothesized that this method is associated with fewer wound complications but increased use of resources.
Methods:
A retrospective review of 98 cases treated with an Ilizarov fixator (2004-2024) was conducted. Surgical management included 2-stage (n = 53, 54%) and single-stage (n = 45, 46%) procedures. Baseline characteristics and risk factors for compromised wound healing were recorded. Patients were stratified into 3 subgroups to enable comparative analysis: infection-related reconstructions (IRR), Charcot arthropathy (CA) and other applications. Preoperative presence of infection and ulceration was recorded. Primary endpoints were rates of impaired wound healing and wound revisions within 3 months post removal. Secondary endpoints were hospital length of stay after bony fixation, and total hospitalization costs.
Results:
Wound revision rates were significantly lower in the 2-stage group (9% vs 36%; OR 5.3, 95% CI 1.8-17.9; P = .0025) particularly in the CA subgroup (0% vs 38%; P = .010) or when an infection was present (14% vs 44%; OR 4.6, 95% CI 1.2-22.3, P = .0138). Impaired wound healing was significantly lower in patients with a 2-stage procedure (30% vs 55%; OR 2.9, 95% CI 1.3-6.6, P = .021). As an exploratory secondary outcome, no statistically significant difference in length of hospital stay or total hospitalization costs was observed.
Conclusion:
Two-stage Ilizarov ring fixator application in high-risk foot and ankle surgery was associated with lower rates of impaired wound healing and wound revisions, particularly in CA and infection cases, without increasing hospital stay or costs.
Introduction
The Ilizarov ring fixator enables precise multiplanar application of compression forces and a higher stability compared with external tube fixation. In foot and ankle surgery, it is therefore an established treatment option when external fixation is required for healing and internal fixation is not appropriate. It is typically used for patients who require stabilization in cases of Charcot arthropathy (CA) foot reconstruction in the presence of infection (eg, osteomyelitis or reconstructive foot and ankle surgeries in high-risk patients due to the patient’s soft tissue conditions or medical comorbidities).7,16,25,26 These conditions are well-established risk factors for impaired wound healing, posing substantial challenges in the postoperative wound management in this patient population.12,22,28 Although long-term outcomes are well documented in the literature, such as the reported limb preservation rate exceeding 90% in CA, wound complications and short-term complications in general remain less thoroughly explored.5,16,30 However, this is particularly of interest as the ring fixator makes postoperative wound care more difficult because of the poorer accessibility to the wound as seen in Figure 5.10,27,30,31
At our institution, we have observed that wound care is more effective with a 2-stage application of the ring fixateur. This would include an initial surgical procedure for reconstruction and a second surgery to apply the Ilizarov ring fixation approximately 5 days later. This 2-stage application of the Ilizarov external fixator has been routinely implemented since 2020, as seen in Figure 1.
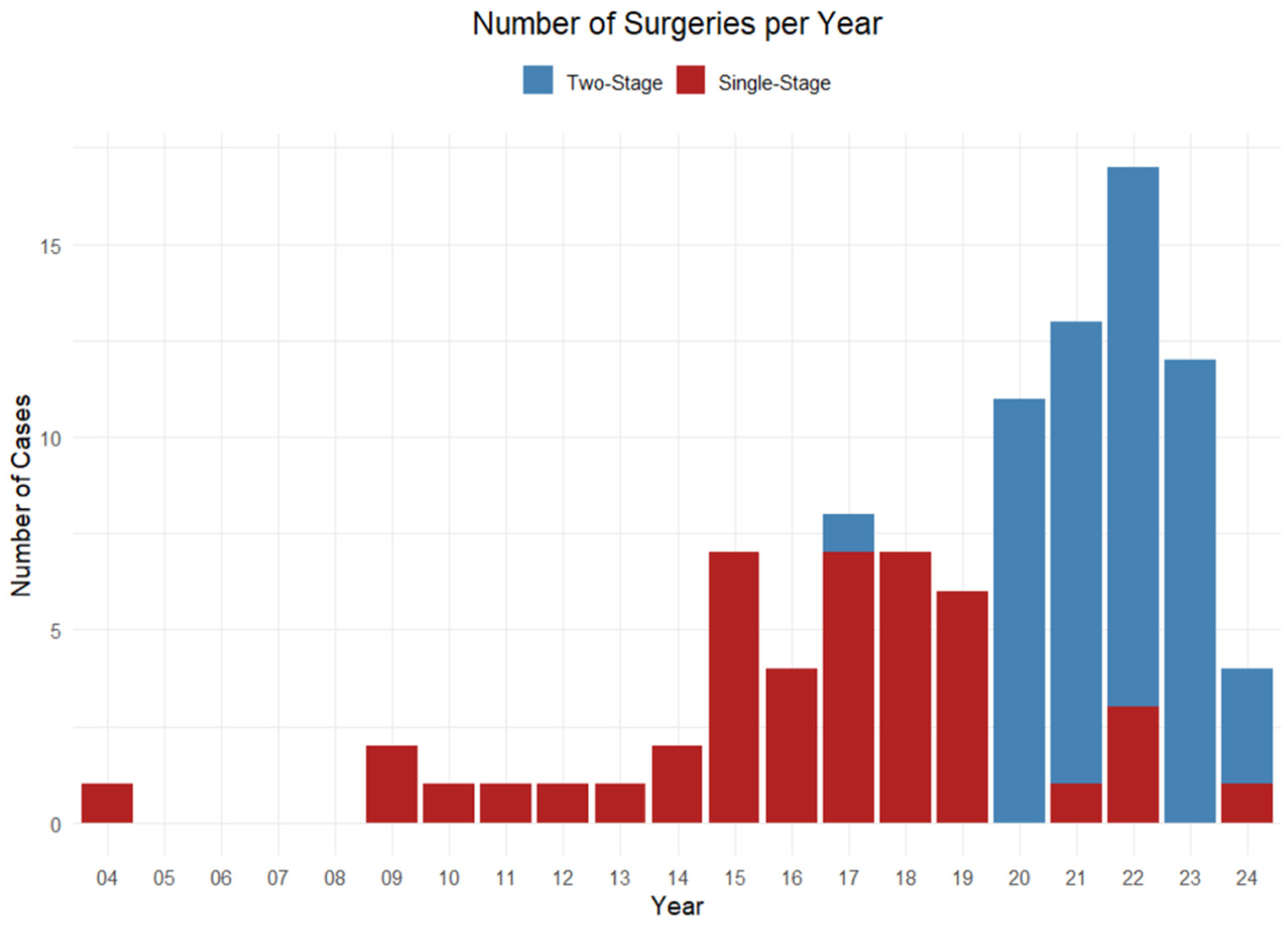
Yearly distribution of Ilizarov applications at our department in foot and ankle surgery between 2004 and 2024. The 2-stage procedure was more broadly used as of 2020. Seven surgeries were performed before 2014.
We hypothesized that this approach offers advantages in wound healing, potentially leading to fewer wound complications and subsequently fewer wound revision surgeries compared to a 1-stage procedure.
From a pathophysiological perspective, surgical trauma triggers an inflammatory cascade with peak vasodilatation and maximal edema formation occurring approximately 72 to 96 hours postoperatively.3,13,24 In patients with already compromised soft tissue, due to diabetes, peripheral artery disease, or preexisting ulceration, this inflammatory response is amplified and wound healing capacity is diminished.12,22,28 Although early stabilization of fractures generally improves the soft tissue envelope by reducing ongoing motion at the injury site, the clinical scenario in elective reconstructive foot and ankle surgery differs fundamentally: the primary bony correction already provides provisional stability through temporary fixation with Kirschner (K) wires or hybrid constructs. Primary stabilization is mostly achieved with provisional K-wire fixation, whereas hybrid constructions using screws or plates are applied selectively when additional stability is required prior to definitive fixation.4,8,11,15,17,20
Application of the Ilizarov frames system during the phase of maximal postoperative edema may mechanically compromise wound closure and impede direct wound access, which is critical during the early inflammatory and proliferative phases of healing.8,30 Conversely, a short delay of approximately 5 days before frame application allows for postoperative edema management through elevation and compression bandaging, unimpeded wound inspection and care, and subsidence of the acute inflammatory phase, analogous to the well-established principle of staged surgery in trauma and damage control orthopaedics.6,14,18,21,29
However, as a delayed application requires 2 surgeries, we hypothesized that the 2-stage approach significantly increases hospitalization costs and length of stay.
The aim of this study was to evaluate whether a delayed, 2-staged application of the Ilizarov external fixator is associated with lower rates of wound healing complications and revision surgeries, and to assess its impact on resource utilization, especially on postoperative length of stay and total hospitalization costs, particularly in patients with comorbidities such as CA or infection.
Materials and Methods
A retrospective chart review was conducted to assess early postoperative complications in the first 3 months, following Ilizarov ring fixator removal in foot and ankle surgeries at our institution between 2004 and 2024. The study was approved by the local ethics committee, and informed consent was obtained from all patients included.
Baseline data were complete for all included patients with the exception of the American Society of Anesthesiologists (ASA) score, which was unavailable in 5 cases in the single-stage group. No imputation was performed for missing values, and affected cases were excluded from the respective variable analysis. Patients with insufficient follow-up (<3 months after frame removal, n = 10) or missing general consent (n = 18) were excluded from the study (Figure 2). Cost data were available only from 2016 onward, resulting in a reduced sample for cost analysis (n = 80).
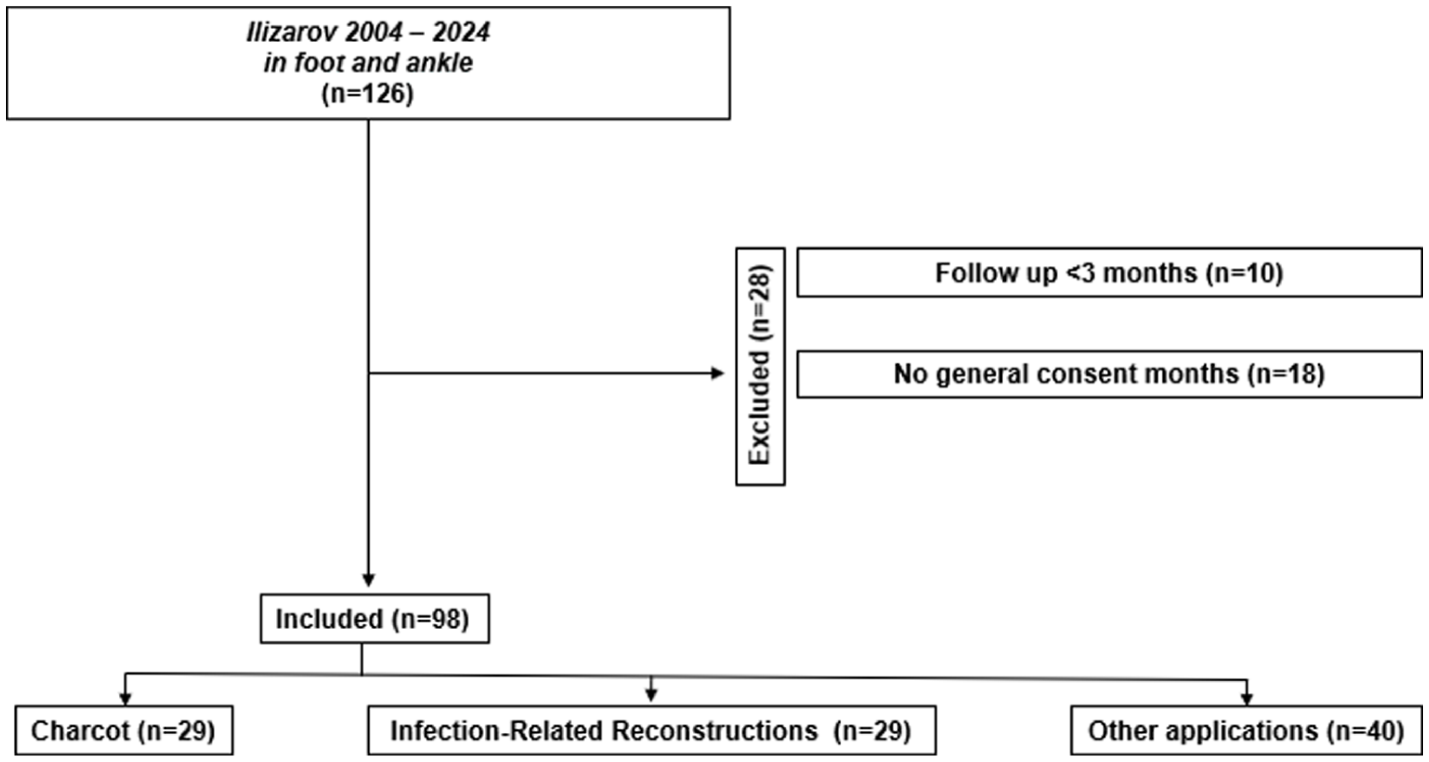
Inclusion and exclusion criterion flowchart.
Of the 126 patients identified, 28 patients had to be excluded because of a lack of follow-up data for at least 3 months (10 patients), missing general consent (18 patients). Inclusion and exclusion criteria are shown in Figure 2. If a patient was treated more than 1 time with Ilizarov ring-fixation system, the surgery was included as a new case if wound healing was completed and the patient has been discharged in the meantime. All procedures involved either a single-stage Ilizarov application (n = 45; 46%) or a 2-stage approach (n = 53; 54%), defined as preliminary bony correction, followed by delayed Ilizarov application by approximately 5 days in a second procedure. Patient demographics and risk factors for impaired wound healing (ASA score, obesity, smoking status, diabetes mellitus, peripheral arterial disease, and renal insufficiency) were recorded, along with the Charlson Comorbidity Index.1,2,12,22,28 Additionally the Ilizarov wearing time was recorded, and if the frame had to be removed prematurely. Patients were broken into the following subgroups defined as patients with osteomyelitis (OM) diagnosed in MRI or clinical soft tissue abscess, further referred to as infection-related reconstructions (IRRs). Patients with a diagnosis of CA that did not meet the inclusion criterion for the IRR subgroup. A collective subgroup that did not meet the inclusion criteria for either the IRR or the CA subgroups, further referred to as other applications. If the CA patients met the inclusion criterion for the IRR subgroup, they were counted in the IRR subgroup (single-stage 6 and 2-stage 8 patients). Primary stabilization was achieved with K-wire fixation in the majority of cases. Hybrid constructions, incorporating screws or plates for additional stability, were used in 9 cases in the 2-stage group (17%) and 1 case in the single-stage group (2%, P = .02). No cases involved internal fixation as the sole method of definitive stabilization.
To account for the potential negative impact of infection on wound healing, the presence of infection at the time of bony correction was documented as an additional stratification criterion. Infection was considered present if patients belonged to the IRR subgroup or had more than 2 positive microbiological tissue cultures. This approach aimed to capture cases of low-grade or occult infection. A further stratification based on severity was intentionally avoided as such differentiation is clinically challenging and would have further reduced subgroup size.
Perioperative wound care was standardized, including daily dressing changes starting on the second day. Pin sites were cleansed daily with iodine. After discharge patients were regularly monitored by wound care specialists according to institutional protocols.
Primary endpoints were wound revision rates and the rate of impaired wound healing, which was defined as any wound dehiscence, including partial or complete separation of wound edges, occurring after planned suture removal and requiring prolonged wound care beyond routine postoperative management. Wound revision was defined as any unplanned return to the operating room for surgical wound debridement, secondary closure, or other operative wound intervention within 3 months after frame removal. Below-knee amputations performed within this period due to persistent deep wound infection were also classified as wound revisions.
Secondary endpoints were hospital length of stay after bony correction, and total hospitalization costs, which included direct operational costs and facility usage costs.
To avoid nonrelated preoperative influences, we defined hospital length of stay from the date of reconstructive surgery, further referred to as bony correction (basically first-stage surgery in the 2-stage group and definitive surgery in the 1-stage group) to discharge. In cases involving multiple surgeries, the last surgical intervention was used to standardize comparisons.
Total hospitalization costs were obtained from the hospital’s finance department and included all inpatient-related expenses from 2016 onward for each hospitalization. These included direct operational costs and facility usage costs, encompassing expenditures for surgery, anesthesia, wound care, medical supplies, inpatient care, nonmedical inpatient costs, as well as costs related to the facilities. Because the hospitalization costs could only be obtained starting 2016, we could include a total of 53 in the 2-stage and 27 in the single-stage group. In the subgroup analysis, the numbers were as follows: CA, 16 two-stage and 6 single-stage; IRR, 13 two-stage and 11 single-stage; other applications, 24 two-stage and 10 single-stage.
Statistical Analysis
Group differences in baseline characteristics were assessed using t tests for normally distributed variables, Mann-Whitney U tests for non-normal variables, and χ2 (expected count >5) or Fisher exact tests for categorical variables. Binary postoperative outcomes were analyzed using multivariable logistic regression including treatment type and infection status. Length of hospital stay and costs were compared using Mann-Whitney U tests. Because of right-skewed cost data, generalized linear models with a Gamma distribution and log link were applied. Interaction terms between treatment type and predefined subgroups (CA, IRR, and other applications) were included to evaluate subgroup-specific effects. Two-sided P values <.05 were considered statistically significant.
Results
Subgroups, Baseline Characteristics, Risk Factors for Impaired Wound Healing and Frame Wearing Time and Operation Time
Patient subgroups, characteristics and the recorded risk factors for impaired wound healing are summarized in Table 1. There were no statistically significant differences between 2-stage and single-stage groups. The mean time of interval from reconstruction to Ilizarov application in the 2-stage group was 5.6 ± 2.01 days. Notably, there was a trend to more infections present in the single-stage group compared to the 2-stage group (53% vs 76%) in all patients and in the CA subgroup (31% vs 74%). The frame had to be removed prematurely in 6 cases in the single-stage and in 5 cases in the 2-stage group. These cases were excluded in the calculation of the Ilizarov wearing time. In the single-stage group, the mean wearing time was significantly longer than in the 2-stage group (17.82 ± 5.16 weeks vs 14.11 ± 3.4 weeks; P = .001). In the 2-stage group, the other application group included 15 cases of hindfoot corrections, fusions or fusion revisions, 6 midfoot corrective procedures, 2 combined hindfoot and midfoot corrections, and 1 revision of a distal tibial pseudarthrosis. In the single-stage group, the distribution consisted of 10 hindfoot correction, fusions or fusion revision procedures, 3 combined hindfoot and midfoot corrections, and 3 revisions of distal tibial pseudarthrosis. In the 2-stage group the mean operative time for Ilizarov application was 69 ± 29.2 minutes.
Demographic Parameters for All Patients. a
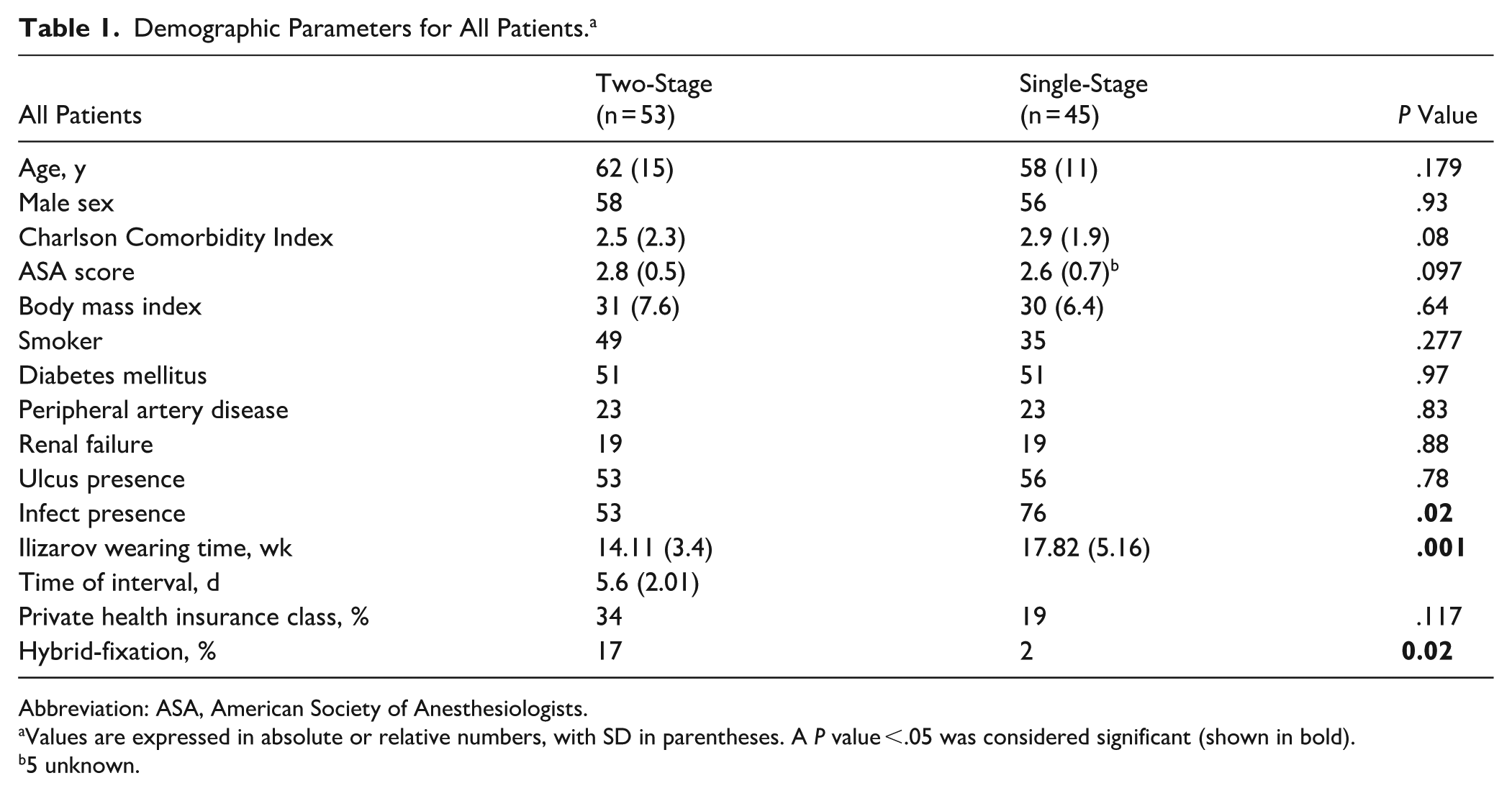
Abbreviation: ASA, American Society of Anesthesiologists.
Values are expressed in absolute or relative numbers, with SD in parentheses. A P value <.05 was considered significant (shown in bold).
5 unknown.
Only one 2-stage case was performed before 2020, whereas the majority of 2-stage procedures occurred from 2020 onward (Figure 1).
No major postoperative medical complications such as pulmonary embolism, myocardial infarction, or pneumonia were documented in either group.
Wound Revision Rate
The need for wound revision was significantly less in the 2-stage group compared with the single-stage group (9% vs 36%; OR 5.3, 95% CI 1.8-17.9, P = .0025). Breaking down this result to the subgroups revealed that revision rate was significantly reduced for the 2-stage procedure within the CA subgroup (0% vs 38%; P = .010), whereas the other subgroups showed favorable trends for less wound revisions for the 2-stage approach without reaching significance. When stratifying for infection presence at the time of surgery, the 2-stage group showed a significant benefit (14% vs 44%; OR 4.6, 95% CI 1.2-22.3, P = .0138). The results are summarized in Table 2. Bivariate logistic regression analysis confirmed that surgical procedure type was significantly associated with wound revision risk. Two-stage application had a 4.26-fold decreased risk of revision, independent of infection status (OR 4.26, 95% CI 1.43-14.49, P = .013). Furthermore, infection presence was associated with a 5.9-fold increased risk of revision, regardless of the surgical procedure performed (OR 5.9, 95% CI 1.49-39.5, P = .025).
Demographic Parameters in Subgroups. a
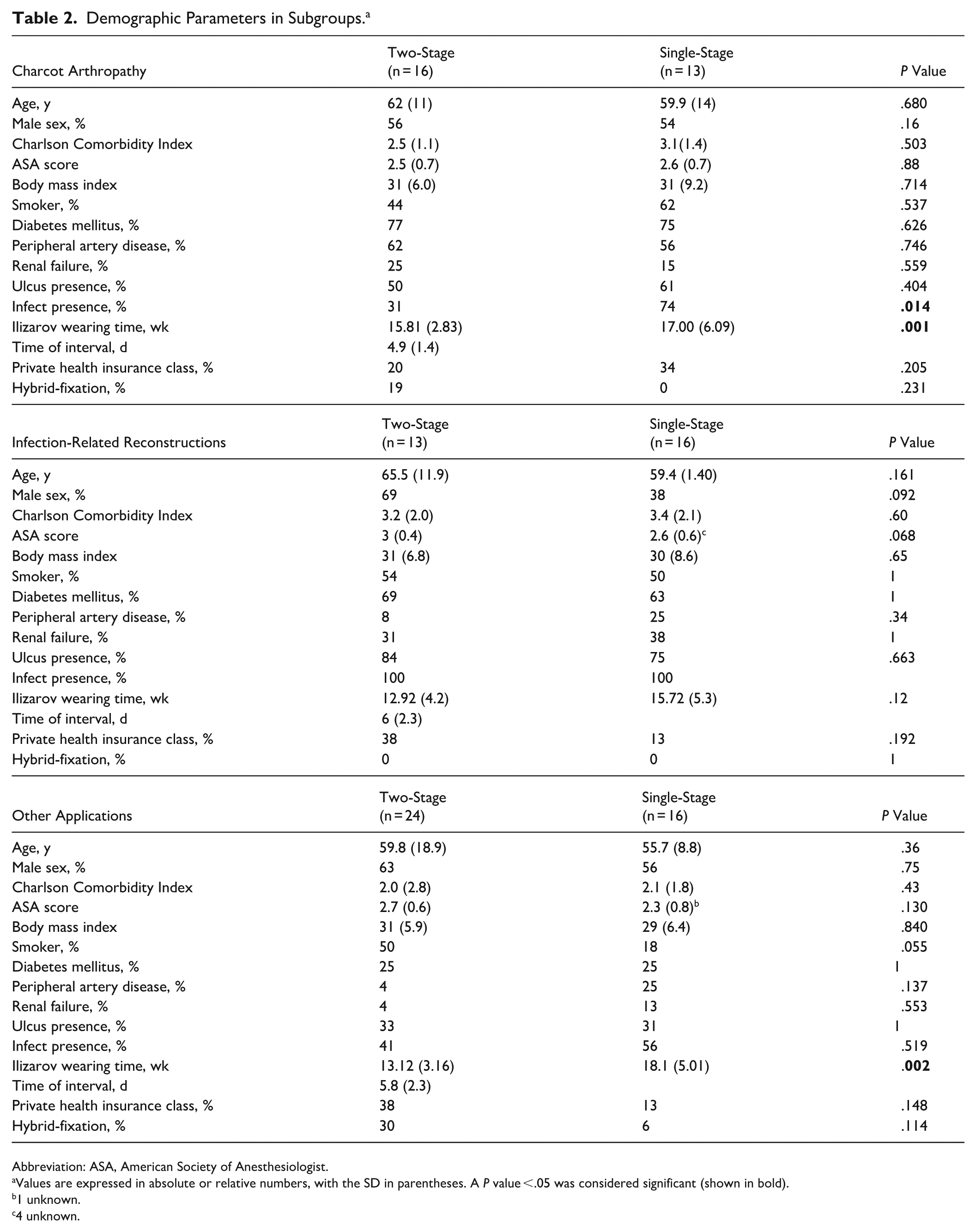
Abbreviation: ASA, American Society of Anesthesiologist.
Values are expressed in absolute or relative numbers, with the SD in parentheses. A P value <.05 was considered significant (shown in bold).
1 unknown.
4 unknown.
Two patients in the single-stage group underwent below-knee amputation within 3 months after planned frame removal due to persistent infection, 1 in the IRR subgroup and 1 in the other applications subgroup following hindfoot correction. These cases were classified as wound revisions in the primary analysis.
When stratifying for preoperative ulcers it showed favorable tendencies toward the 2-stage application but did not reach statistical significance as seen in Tables 3 and 4. When pooling cases with a present infection, 82% of revision surgeries were associated with infection, regardless of severity. Only 1 revision occurred in patients without documented infection in each group. No revision case in the 2-stage group was ulcer free, whereas 69% of the single-stage cases requiring a wound revision had a preoperative ulcer. One wound revision was in a case with hybrid fixation in the 2-stage group, subgroup other applications, there was no infection present preoperatively
Wound Revisions Rates for the 2 Main Groups, Subgroups and Additional Stratification (Presence of Infection and Preoperative Ulcer Status). a
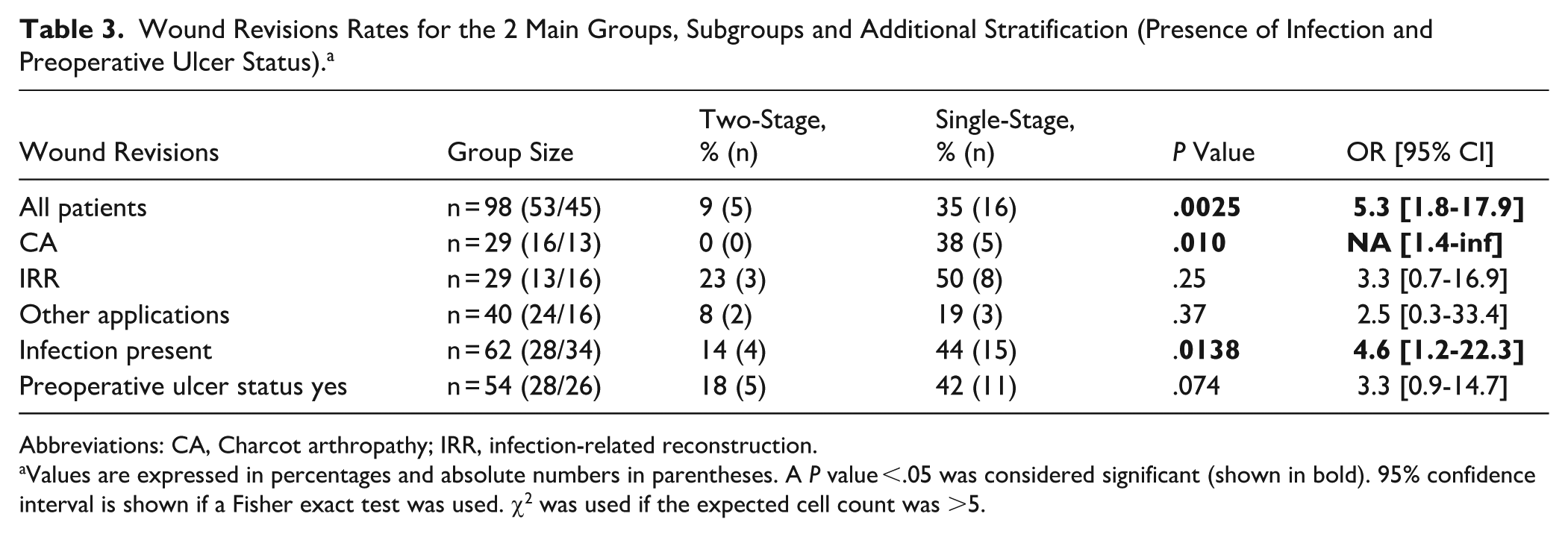
Abbreviations: CA, Charcot arthropathy; IRR, infection-related reconstruction.
Values are expressed in percentages and absolute numbers in parentheses. A P value <.05 was considered significant (shown in bold). 95% confidence interval is shown if a Fisher exact test was used. χ2 was used if the expected cell count was >5.
Impaired Wound Healing Rates for the 2 Main Groups, Subgroups and Additional Stratification (Presence of Infection and Preoperative Ulcer Status). a
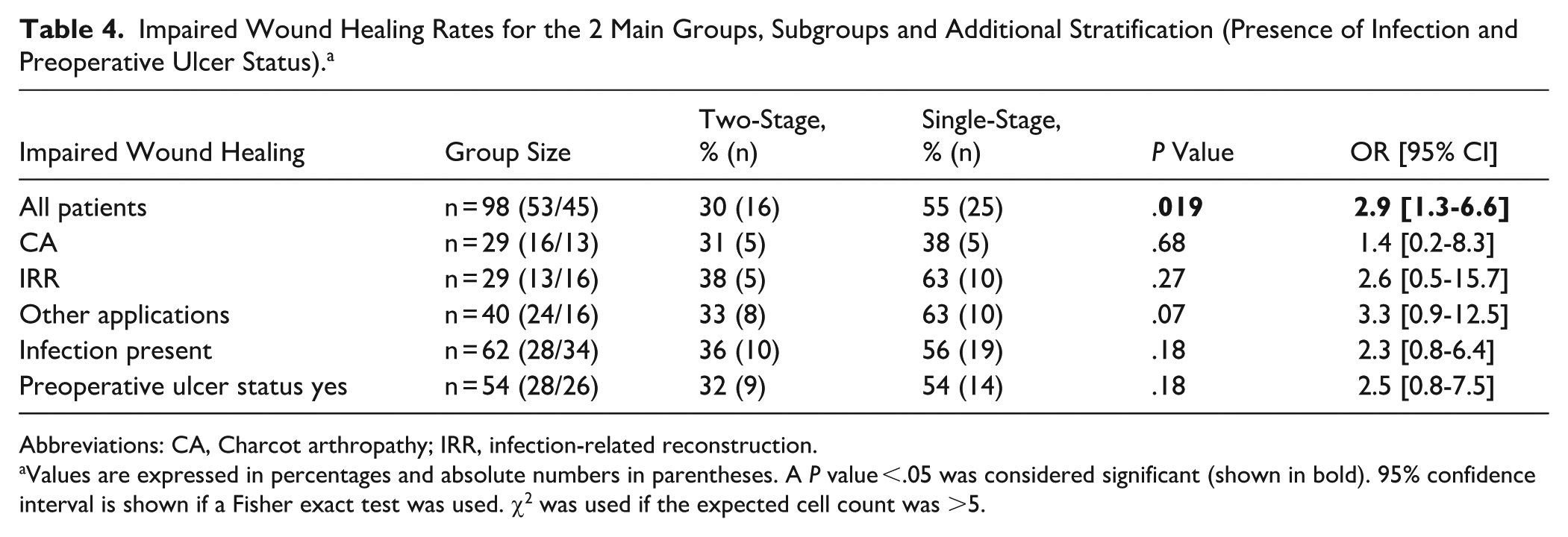
Abbreviations: CA, Charcot arthropathy; IRR, infection-related reconstruction.
Values are expressed in percentages and absolute numbers in parentheses. A P value <.05 was considered significant (shown in bold). 95% confidence interval is shown if a Fisher exact test was used. χ2 was used if the expected cell count was >5.
Impaired Wound Healing
Impaired wound healing was significantly less frequent in the 2-stage group (30% vs 55%; OR 2.9, 95% CI 1.3-6.6, P = .019). The subgroup analysis revealed a consistent tendency toward the 2-stage procedure but did not reach statistical significance. When stratifying for infection presence at the time of surgery (36% vs 56%; OR 2.3, 95% CI 0.8-6.4) and preoperative ulcer (32% vs 54%; OR 2.5, 95% CI 0.8-7.5), the same tendency was found. The results are summarized in Table 3.
Secondary Outcome: Length of Hospital Stay
Median hospital stay from bony correction to discharge was 13 days (SD 5.15; 95% CI 11.5-15.10) in the single-stage group and 14 days (SD 9.86; 95% CI 12.5-19.5) in the 2-stage group. Statistical analysis revealed that, with the numbers available, there was no significant difference between the 2 main groups (P = .397) and the subgroups (CA, P = .269; IRR, P = .419, other applications P = .266). The results are summarized in Figure 3. Median hospital stay for CA was 14 days for 2-stage (SD 5.97; 95% CI 11.00-15.00) and 15 days for single-stage (SD 10.15; 95% CI 11.49-24.49). For IRR 18 days in both groups, 2-stage (SD 4.74; 95% CI 13.5-19.5) and single-stage (SD 10.3; 95% CI 14.53-27), for other applications 11 days for 2-stage (SD 4.28; 95% CI 10.0-14.50) and 9 days for single-stage (SD 6.570; 95% CI 8.0-14.5). One outlier with extended hospitalization of more than 30 days was seen in the 2-stage and 4 in the single-stage group.
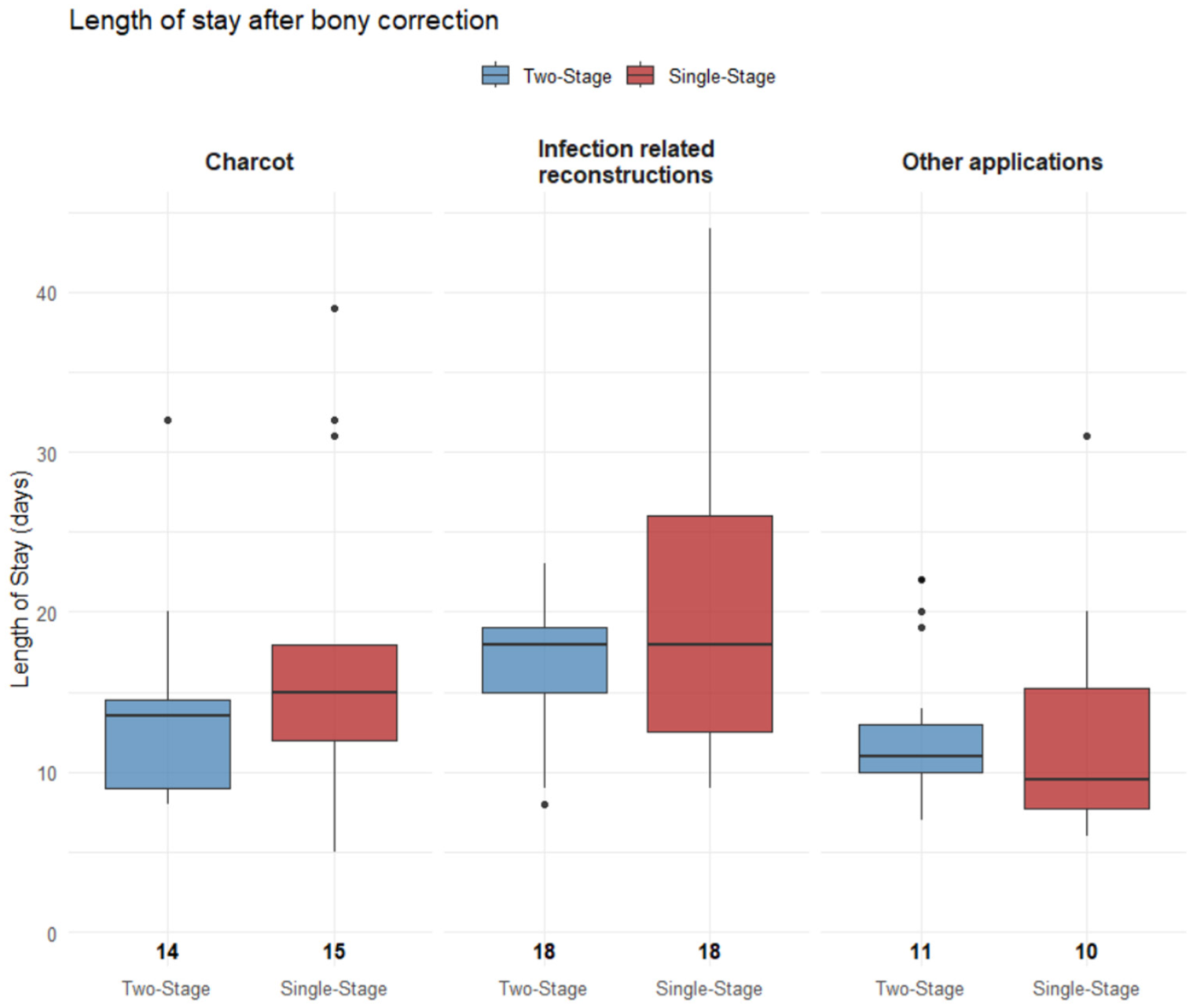
Box plots illustrate the hospital length of stay in days following bony correction, stratified by surgical strategy: 2-stage and single-stage. Subgroups include Charcot arthropathy, Infection-Related reconstructions, and other applications. Median values are displayed below each box. Outliers are shown as black dots.
Secondary Outcome: Total Hospitalization Costs
With the numbers available, no significant difference could be detected in total hospitalization costs between the 2 groups (P = .772). Median total cost was 46.842 CHF (SD 21.458; 95% CI 37.425, 48.979) in the 2-stage and 43.201 CHF (SD 35.147; 95% CI 37.055, 63.570) in the single-stage group. Only in the subgroup other applications (P = .981), costs were lower in the single-stage group (24.777 CHF, SD 13.262; 95% CI 21.427-37.866 vs 34.582 CHF, SD 19.806; 95% CI 29.617-45.465), whereas trends favored the 2-stage application in the CA subgroup (P = .653; 37.333 CHF [SD 12.920; 95% CI 32.174-44.836] vs 34.591 CHF [SD 17.976; 95% CI 34.310-63.077]) and in the IRR subgroup (P = 0.445; 60.728 CHF [SD 25.609; 95% CI 45.512-73.355] vs 52.449 CHF [SD 45.141; 95% CI 43.306-96.660]) subgroups. Results are summarized in Figure 4.
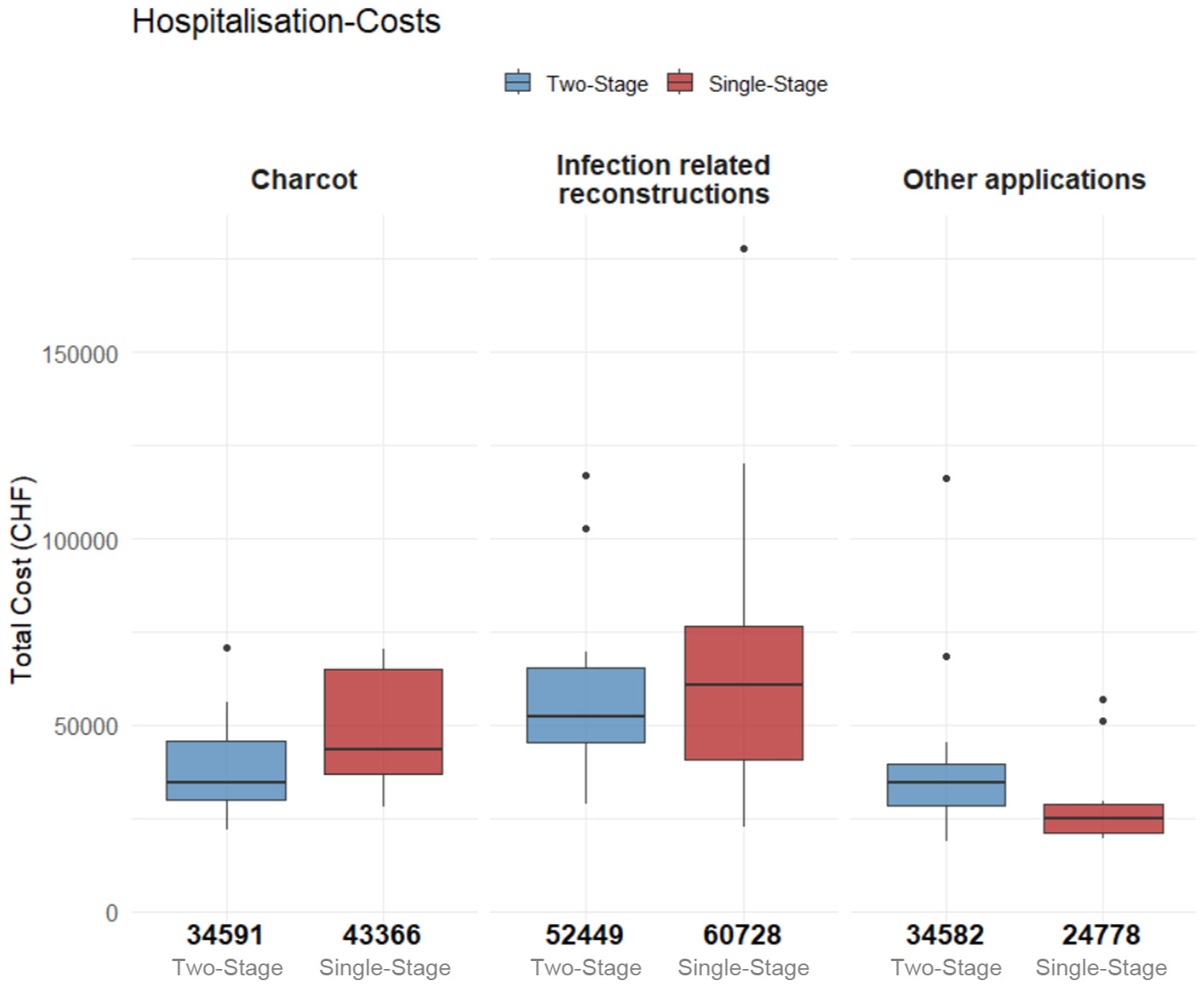
Box plots illustrating total hospitalization costs (in CHF) by surgical strategy of all cases between 2016 and 2024. A total of 53 cases were included in the 2-stage group and 27 in the single-stage group. In the subgroup analysis, the numbers were as follows: CA, 16 two-stage and 6 single-stage; IRR, 13 two-stage and 11 single-stage; other applications, 24 two-stage and 10 single-stage. Median values are displayed in bold at the base of each box. Outliers are shown as black dots.
Patients With >1 Ilizarov Application
One patient had a 2-stage procedure done on both feet. A total of 7 patients underwent multiple procedures involving either single-stage or 2-stage Ilizarov procedure on the same foot. These repeat procedures included 5 single-stage (2 IRR and 3 other applications) and 2 two-stage (1 CA and 1 IRR). In the single-stage group, 1 of these repeat applications in the subgroup other applications required a wound revision and 3 had impaired wound healing, whereas in the 2-stage group no wound revision was required and 1 impaired wound healing occurred. Exclusion of these cases would not have altered our results in terms of statistical significance of wound revision rates and impaired wound healing.
Discussion
The principal finding of this study is that the 2-stage group experienced significantly fewer wound revisions (9% vs 35%; P = .0025) and impaired wound healing (30% vs 55%; P = .019) compared with the single-stage protocol. Delaying the application of the Ilizarov ring fixator by approximately 5 days postoperatively may facilitate immediate postoperative wound care and effective edema control and may be associated with improved early wound healing as seen in Figure 5.18,19
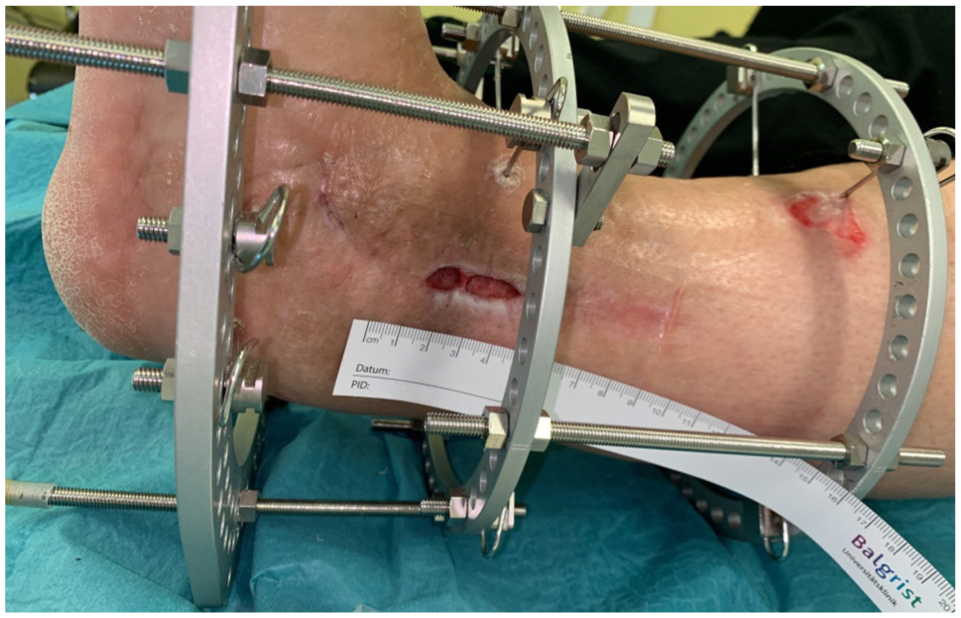
Image of a patient with impaired wound healing wearing an Ilizarov ring fixator. The large circular rings visibly limit access to the wound site, making wound care challenging.
We have also analyzed for which indications a 2-stage approach should be preferred in this context. Our cohort could be stratified in 3 subgroups (IRR, CA, and other applications). In general, all subgroups favored the 2-stage approach to avoid wound complications. This was observed as a trend in the IRR and other application group but significantly lower wound revisions rates in the 2-stage procedure could only be observed in the CA subgroup. Although our findings were not significant in the IRR group, we found a significant difference for fewer wound complications when stratified for presence of infection (patients with 2 positive tissue cultures and IRR subgroup) as well as in all groups (9% vs 35%). These findings suggest that the 2-stage procedure may be especially beneficial for patients with infection and/or CA.
While no statistically significant differences in the overall prevalence of comorbidities were observed between the primary cohorts, patients in the other applications subgroup exhibited a generally more favorable preoperative risk profile, as reflected by lower mean values for the ASA score, Charlson Comorbidity Index, and body mass index. Nevertheless, our cohort as a whole and in subgroup analysis demonstrated a high burden of risk factors. These findings suggest a comparable distribution of comorbidities across the treatment groups as well as within their respective subgroups. Concerning risk factors for wound healing, a difference was noted in patients with a present infection, which were more frequently seen in the single-stage group (76% vs 53%). Because infection was associated with wound complications in our study, a higher prevalence of infection in the single stage might have a bias on our finding. We therefore stratified for the presence of infection at the time of surgery and found similar results for revision rate (14% vs 44%) and impaired wound healing (36% vs 55%). Bivariate logistic regression analysis demonstrated that the presence of infection was independently associated with an increased risk for revision surgery by 5.9-fold, whereas the use of the 2-stage protocol was associated with a significantly reduced risk by 4.26-fold. These findings suggest the interpretation that the differences in clinical outcomes may not be merely driven by the unequal distribution of infections, but rather may reflect an independent association with the surgical approach. Hybrid fixation was more frequently applied in the 2-stage cohort; however, only 1 wound revision occurred in a hybrid case. Given the limited number of revision events (n = 21), the study was underpowered to evaluate hybrid fixation as an independent predictor.
Notably, the additional anesthetic exposure required by the 2-stage protocol did not result in any documented major medical complications, which may help alleviate concerns regarding the perioperative safety of a staged approach in this already comorbid patient population.
Although the core principles of perioperative wound care remained consistent throughout the study period, including daily dressing changes and standardized pin site care with iodine, the specific wound care products, dressing materials, and postoperative management protocols have inevitably evolved over 2 decades. The availability of advanced wound dressings, improved antiseptic agents, and more structured outpatient wound monitoring may have contributed to improved outcomes in the more recent 2-stage cohort, independently of the staged approach itself. This temporal confounding cannot be fully separated from the treatment effect in our retrospective design.
Our cohort consisted of 7 cases of more than 1 Ilizarov applications on the same foot, which leads to a potential bias. Because wound healing was completed in each case and the patient was discharged before the next application it was viewed as a separate case, possibly introducing a potential nonindependence bias. Notably exclusion of the repeat procedures would have not altered our results.
After adjusting for cases with premature frame removal, the Ilizarov fixator was worn longer in the single-stage group, with a mean duration of 18 weeks compared to 14 weeks in the 2-stage group (P = .001). This difference was particularly evident in the other applications subgroup. The prolonged fixator duration in the single-stage group (mean 18 vs 14 weeks, P = .001) may reflect evolving criteria for frame removal. Earlier cases were potentially managed with a more conservative approach, relying primarily on radiographic evidence of complete consolidation before frame removal. More recent practice has incorporated clinical assessment of stability alongside radiographic findings, potentially allowing for earlier frame removal. Additionally, the higher proportion of infection-related cases in the single-stage group may have necessitated prolonged fixator wear to achieve adequate bony consolidation in a compromised biological environment. 30
Earlier frame removal in these subgroups may reflect a potential follow-up bias, as the cumulative time from bony correction to the end of follow-up was possibly longer. However, given the already extended follow-up period, comprising 18 or 14 weeks of fixator wear plus an additional 12 weeks, we believe that any such effect is likely negligible. The interval between bony correction and Ilizarov application was comparable between subgroups. The range of the interval was 4-7 days, only 3 cases belonging to the IRR group had less than 4 days and 3 cases had more (2 times 9 days and 1 time 13 days).
Nevertheless, we think a strength of this study is the standardization of follow-up to 3 months after Ilizarov removal, regardless of total fixator wearing time. Still, the retrospective nature and evolving clinical practices over a 20-year period introduce potential bias. Only one 2-stage procedure was performed before 2020, whereas the 2-stage protocol became routine thereafter, reflecting an institutional paradigm shift.
During this 20-year study period, a learning curve has inevitably been navigated by the surgical and nursing teams. Advances in wound care products, perioperative management protocols, and a growing institutional experience with ring fixation may have contributed to improved outcomes in the more recent 2-stage cohort independently of the staged approach itself. For example, the adoption of modern wound dressings, standardized pin site care protocols, and more structured postoperative rehabilitation pathways are all developments that may confound the observed treatment effect. Furthermore, treatment allocation was not randomized but rather reflects an evolving institutional practice pattern (Figure 1), and selection bias cannot be excluded. However, the indication spectrum remained broadly comparable throughout the study period, and all procedures were performed by experienced foot and ankle surgeons, with 2 attending surgeons participating in each case, which limits but does not eliminate the potential influence of temporal confounding.
Although pin tract infections represent a relevant complication of circular fixation, they were not included as a formal endpoint because documentation was not standardized across the study period, precluding reliable comparative analysis.
Recent evidence indicates that circular external fixators remain underused, partly because of concerns related to operative duration. In our cohort, application of the Ilizarov frame, which was not prebuilt required 69 ± 29.2 minutes in the 2-stage group. A staged approach may help address this issue by reducing the perceived operative burden, thereby facilitating wider adoption.9,23
Outcomes may be influenced by surgeon experience; however, all procedures were performed with the involvement of 2 senior foot and ankle surgeons, making a relevant volume-related effect unlikely, though not entirely excludable.
Contrary to the initial hypothesis, staging the procedure was not associated with a significant increase in hospitalization duration or costs. The median stay after bony fixation was even lower in the 2-stage group (13 vs 14 days). Notably the subgroup other applications had the shortest length of hospital stay and was the only subgroup that had a longer stay in the 2-stage group (11 vs 10 days). It was also the group that had the most preferable risk profile and fewest complications. The influence of nonmedical factors on discharge timing, such as availability of rehabilitation or nursing facility, cannot be excluded and may have affected length of stay.
The same was true for total hospitalization costs. No statistically significant differences were observed across subgroups. However, within the other applications, median hospitalization costs were notably higher in the 2-stage group compared with the single-stage group.
It is important to note that hospitalization costs in our institution reflect a combination of direct operational costs and infrastructure use fees. As such, the reported figures are suitable for relative comparisons within this study but are not directly comparable to absolute cost values across different institutions. It is important to note that hospitalization duration and costs are heavily influenced by local health care structures, discharge practices, and reimbursement systems, which limits generalizability of these secondary findings to other settings. Nonetheless, these data suggest that the 2-stage procedure was not associated with a significant increase in short-term costs. This finding complements the potential long-term financial advantages of the 2-stage approach, in addition to lower rates of wound revisions and impaired wound healing, which may be associated with reduced rehospital admissions and the need for prolonged outpatient wound care.
Conclusion
In conclusion, the 2-stage application of the Ilizarov ring fixator appears to be a valuable strategy in the management of high-risk patients in foot and ankle surgery. Delaying the application by approximately 5 days after bony correction was associated with significantly reduced early wound complications, such as wound revisions and impaired wound healing, especially in patients with CA or if an infection is present. Delaying the application was not associated with a significant increase in hospitalization costs or length of stay significantly. These results support consideration of a 2-stage Ilizarov frame application in patients with CA or infection.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007261440490 – Supplemental material for Two-Stage vs Single-Stage Ilizarov Application in High-Risk Patients: Impact on Early Complications and Resource Utilization
Supplemental material, sj-pdf-1-fai-10.1177_10711007261440490 for Two-Stage vs Single-Stage Ilizarov Application in High-Risk Patients: Impact on Early Complications and Resource Utilization by Lukas Fischer, Arnd Viehöfer, Carmen Castroviejo, Alexandros Tsolakidis, Flamur Zendeli, Andreas Flury and Stephan Wirth in Foot & Ankle International
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from the Cantonal Ethics Committee Zurich (BASEC-Nr: 2021-00642)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.