
Abstract
Background:
First metatarsophalangeal joint arthrodesis is a reliable treatment for painful end-stage degenerative, inflammatory, and post-traumatic conditions and severe deformities of the first ray. Although long-term functional outcomes are well documented, the incidence and relevance of degenerative changes in adjacent joints of the medial column after first metatarsophalangeal joint (MTP1) fusion remain uncertain.
Methods:
This exploratory single-center follow-up study included patients who underwent isolated MTP1 arthrodesis between 2012 and 2018. Preoperative and final follow-up weight-bearing radiographs were assessed for osteoarthritis progression in the interphalangeal (IP), tarsometatarsal (TMT1), naviculocuneiform (NC), and talonavicular (TN) joints using the Kellgren-Lawrence classification. Radiographic alignment parameters (hallux valgus angle, intermetatarsal angle, hallux-ground angle, and dorsal extension angle) were recorded. Clinical outcome was evaluated using American Orthopaedic Foot & Ankle Society hallux metatarsophalangeal-interphalangeal score (AOFAS HMI) score, Foot and Ankle Outcome Score (FAOS), Foot Function Index (FFI), and a study-specific questionnaire. Paired statistical tests and Pearson correlation analyses were performed.
Results:
Seventy-seven patients (45 female, 32 male) were available for follow-up at a mean of 106.9 ± 25.3 months. Radiographic osteoarthritis progression was significant in all assessed adjacent joints (P < .001) and was most pronounced in the IP joint (66 of 77 joints; 34 of 77 joints progressed by ≥2 grades). TMT1 progression occurred in 23 of 77 joints (≥2 grades in 5 of 77 joints), and NC or TN progression in 30 of 77 joints (≥2 grades: NC 6 of 77, TN 8 of 77). Radiographic alignment was not associated with adjacent-joint osteoarthritis progression, metatarsalgia, or patient-reported outcome. Overall, 90.9% reported good or excellent satisfaction. The mean AOFAS HMI score was 79.9 ± 9.1, FAOS 86.4 ± 15.2, and FFI 18.5% ± 9.3%. Wound healing complications were more frequent with dorsal plating than screw fixation. One nonunion required revision.
Conclusion:
MTP1 arthrodesis provides excellent long-term satisfaction and functional outcomes with low revision rates. Although radiographic adjacent-joint degeneration, particularly involving the interphalangeal joint, may occur over time, these changes do not appear to influence clinical outcomes.
This is a visual representation of the abstract.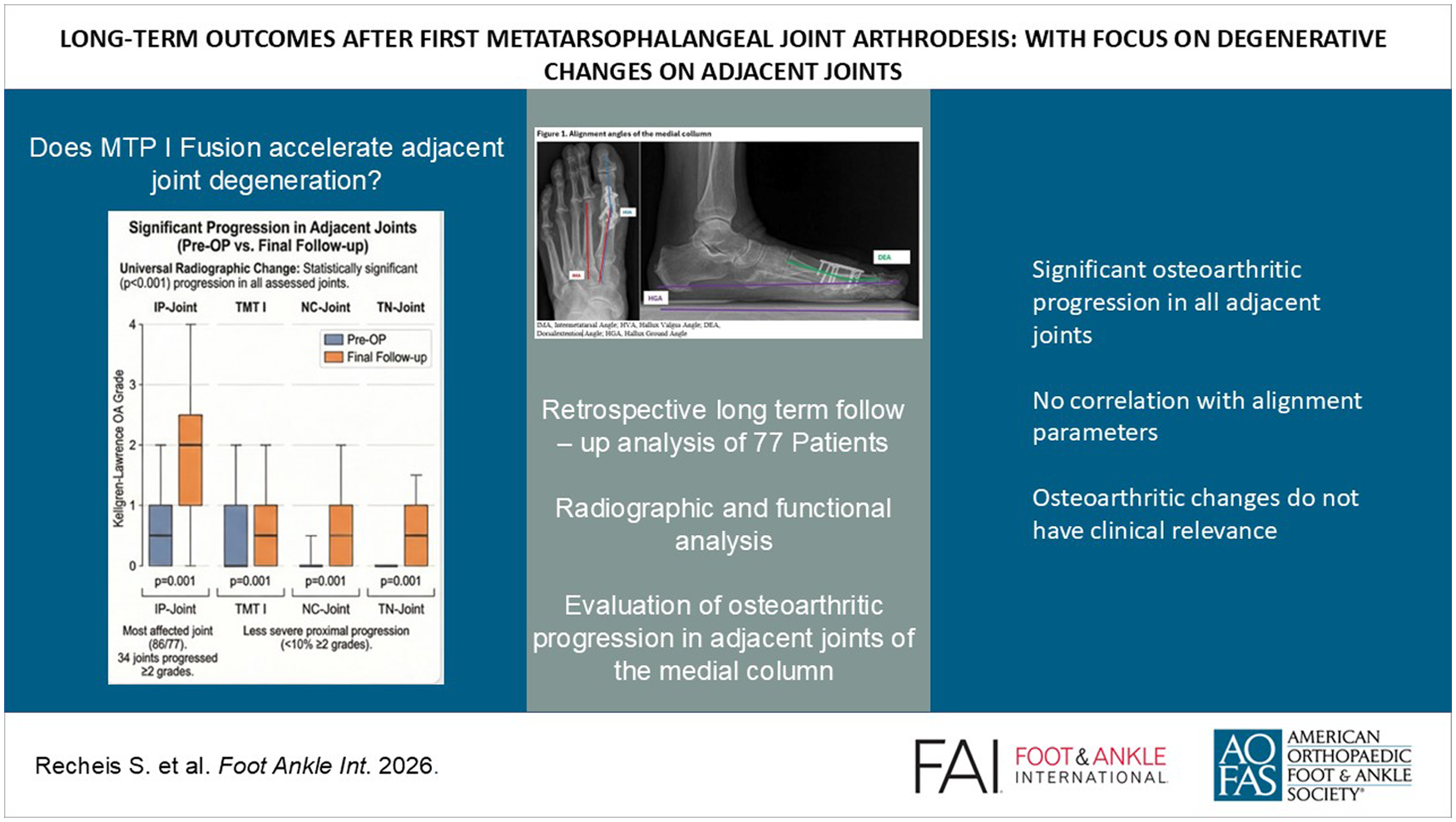
Introduction
Arthrodesis of the first metatarsophalangeal joint (MTP1) is an established procedure for the treatment of advanced hallux rigidus and other severe first-ray deformities.1,2 Long-term studies with follow-up periods extending up to 3 decades have demonstrated high rates of patient satisfaction, durable pain relief, and restoration of forefoot function.3,4 Optimal alignment of the fused joint is essential to achieve favorable functional outcomes.3,4
However, fusion of any joint inevitably alters local biomechanics and load distribution, potentially increasing stress on adjacent articulations. 5 This may contribute to degenerative changes—commonly referred to as adjacent joint arthritis—over time. The development of such degenerative changes is well documented after hindfoot and ankle fusions, 5 but their incidence and clinical relevance following MTP1 arthrodesis remain unclear.
Although the effects of MTP1 fusion on the IP joint have been described, 6 its influence on proximal articulations remains largely unknown. Prior studies indicate that arthrodesis of the MTP1 joint for hallux valgus correction may alter alignment and improve congruence of the first tarsometatarsal (TMT1) joint. 7 However, it remains unclear whether biomechanic alterations due to MTP1 fusion lead to increased mechanical loading and subsequent degenerative changes in proximal medial-column joints over the long term. Given that midfoot arthritis itself represents a clinically relevant condition, clarifying whether MTP1 arthrodesis predisposes to degenerative changes in proximal joints is of particular importance.
Therefore, the present study aims to evaluate long-term clinical and radiologic outcomes after MTP1 arthrodesis, with specific focus on degenerative changes in adjacent joints.
Methods
Institutional review board approval was obtained, and all participants provided informed consent before enrollment. Patients who underwent MTP1 arthrodesis between 2012 and 2018 were eligible for inclusion. Patients with revision surgeries or concomitant arthrodesis of any other joint in the foot were excluded.
Surgical Procedure
All procedures were performed under regional or general anesthesia with tourniquet control using a standardized dorsal approach. Joint preparation was carried out using a cup-and-cone reamer system to achieve maximal bone-to-bone contact. The bone surfaces were perforated with a 2.0-mm drill bit to enhance bleeding and promote fusion.
The hallux was positioned in a physiologic valgus alignment of approximately 10° to 15° relative to the first metatarsal axis with neutral rotation. Dorsiflexion of the hallux was assessed clinically using a flat plate to simulate weightbearing. Optimal dorsiflexion was adjusted to allow a smooth rollover during gait with reliable toe-floor contact in a plantigrade position. Fixation was achieved using either 4.0-mm compression screws or a combination of a compression screw and a low-profile dorsal plate, depending on bone quality and surgeon preference.
Postoperatively, weight-bearing in a forefoot offloading shoe was permitted according to surgeon preference. After radiographic confirmation of union at 6 weeks, patients were transitioned to regular footwear, and physiotherapy was initiated.
Radiologic Assessment
Radiologic evaluation was based on dorsoplantar and lateral radiographs taken preoperatively and at follow-up. Osteoarthritis in the first-ray joints (interphalangeal [IP], tarsometatarsal [TMT], naviculocuneiform [NC], and talonavicular [TN]) was graded according to the Kellgren-Lawrence criteria. 8
Radiographic alignment of the first ray was evaluated on standardized weight-bearing radiographs using following parameters (Figure 1):
Hallux valgus angle (HVA) angle between the longitudinal axes of the first metatarsal and proximal phalanx on dorsoplantar view.
Intermetatarsal angle (IMA) angle between the longitudinal axes of the first and second metatarsals on dorsoplantar view.
Dorsal extension angle (DEA): angle between longitudinal axis of the first metatarsal and the proximal phalanx on lateral view.
Hallux-ground angle (HGA): angle between the longitudinal axis of the proximal phalanx of the hallux and the ground surface on lateral view.

Alignment angles of the medial column. DEA, dorsal extension angle; HGA, hallux ground angle; HVA, hallux valgus angle; IMA, intermetatarsal angle.
Functional Evaluation
Functional outcome was assessed using a modified American Orthopaedic Foot & Ankle Society hallux metatarsophalangeal-interphalangeal score (AOFAS HMI), Foot Function Index (FFI) and the Foot and Ankle Outcome Score (FAOS). In the modified AOFAS score, the 10 points allocated for joint motion were excluded, resulting in a maximum possible score of 90 points. We further evaluated subjective satisfaction with outcomes, use of orthotic devices, ability to achieve active hallux ground contact, and pain while weight-bearing and active motion.
Statistical Analysis
Preoperative and postoperative radiographic levels were compared using the paired t test or Wilcoxon test depending on distribution. Distribution was assessed visually and via Shapiro-Wilk test. Categorical data were compared using chi-square tests. Correlation analysis was conducted using Pearson product-moment correlation. Missing data were excluded in statistical analysis. Because of the study design, we conducted no multiplicity correction. Therefore, all findings should be considered exploratory, and all values should rather be considered descriptive than confirmatory. Statistical significance was set at alpha = .05.
Results
Of 230 eligible patients, 77 (45 women, 32 men) were included. Fixation consisted of dorsal plating in 12 patients and screw fixation in 65. Mean age at surgery was 66.6 ± 9.7 years, with a mean follow-up of 106.9 ± 25.3 months. Primary diagnosis for surgical intervention was primary degenerative arthritis in 71 cases, inflammatory arthritis (gout arthritis) in 1 case, severe posttraumatic arthritis in 1 case, and severe hallux rigidovalgus in 4 cases. Of the 230 patients operated, 89 accepted our invitation. Five patients were excluded because of previous Keller-Brandes procedure, and 7 patients were excluded because of previous nonunion and revision arthrodesis. In addition, 141 patients were lost to follow-up. Demographic characteristics are summarized in Table 1.
Summary of Patient Characteristics.
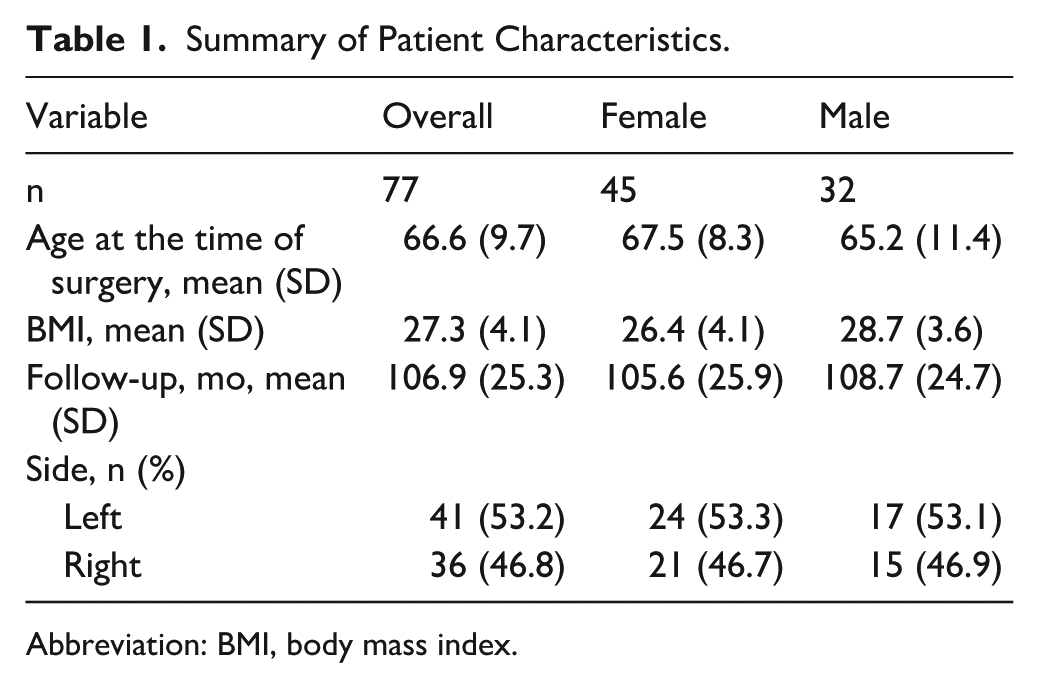
Abbreviation: BMI, body mass index.
Radiographic Progression of Osteoarthritis
Radiographic progression of osteoarthritis from preoperative to final follow-up imaging was seen in all evaluated joints (P < .001) (Figure 2). Progression was most pronounced in the IP joint, affecting 66 of 77 patients, with 34 showing progression of at least 2 grades on the Kellgren-Lawrence scale (P = .001, 95% CI −1.98, −1.49).
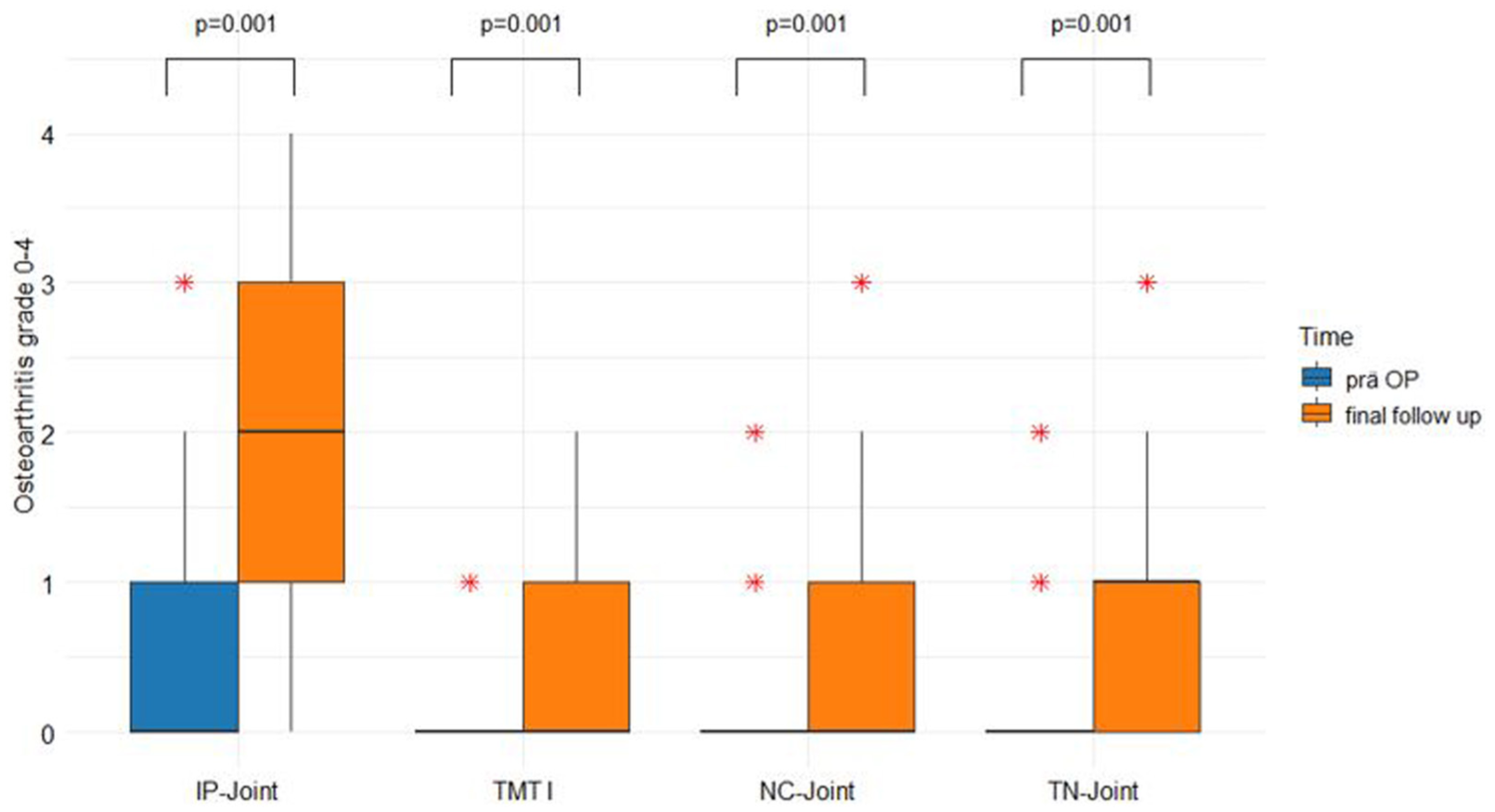
Progression of osteoarthritis of the medial column.
Osteoarthritis progression occurred in 23 patients in the tarsometatarsal (TMT) joint and in 30 patients in the naviculocuneiform (NC) and talonavicular (TN) joints; ≥2 grade progression was seen in 5 (TMT), 6 (NC), and 8 (TN) patients (P = .001, 95% CI −1.49, −1.00).
No associations were found between IP joint progression and distal phalangeal ground contact (P = .78, 95% CI 0.384, 0.50). Also, no association was found between dorsal extension angle (DEA) and osteoarthritis progression in either joint or metatarsalgia (all P > .05, 95% CI −0.50 to 0.12 and −0.21 to 0.35, respectively).
Radiologic Alignment in Relation to Arthritis Progression
Alignment measurements are summarized in Table 2.
Analysis of Alignment.
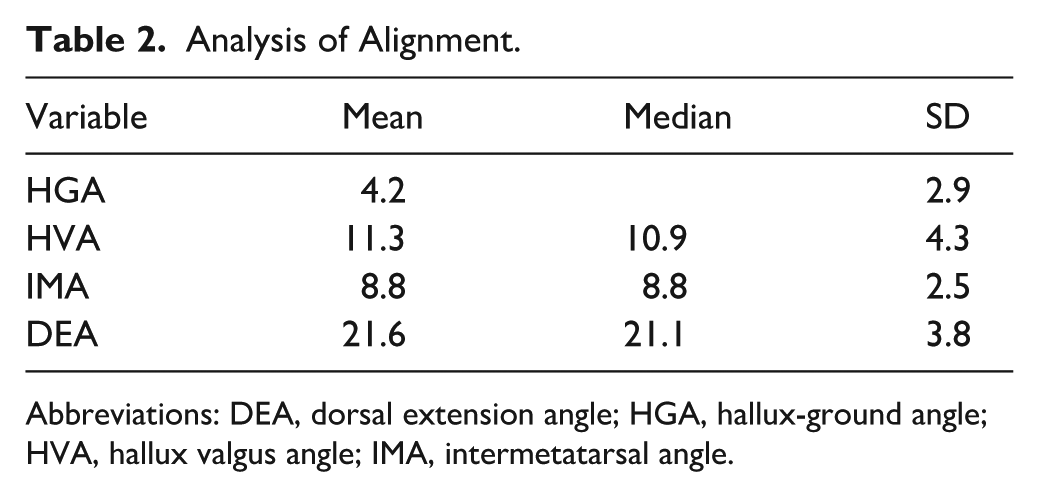
Abbreviations: DEA, dorsal extension angle; HGA, hallux-ground angle; HVA, hallux valgus angle; IMA, intermetatarsal angle.
No correlation was found between HGA and progression of osteoarthritis in the first ray (Table 3).
Correlation Analysis of HGA and Osteoarthritic Progression.

Abbreviations: HGA, hallux-ground angle; IP, interphalangeal; NC, naviculocuneiform; TMT, tarsometatarsal; TN, talonavicular.
Based on the recommended DEA alignment of 20° to 25°, 9 the DEA was categorized into 3 groups: <20° (group 1), 20° to 25° (group 2 = optimal), and >25° (group 3). Across all evaluated joints (IP, TMT, TN, NC), no significant correlation was found between osteoarthritis progression and suboptimal DEA alignment (groups 1 and 3) (Table 4).
Influence of Suboptimal Alignment on Osteoarthritic Progression.
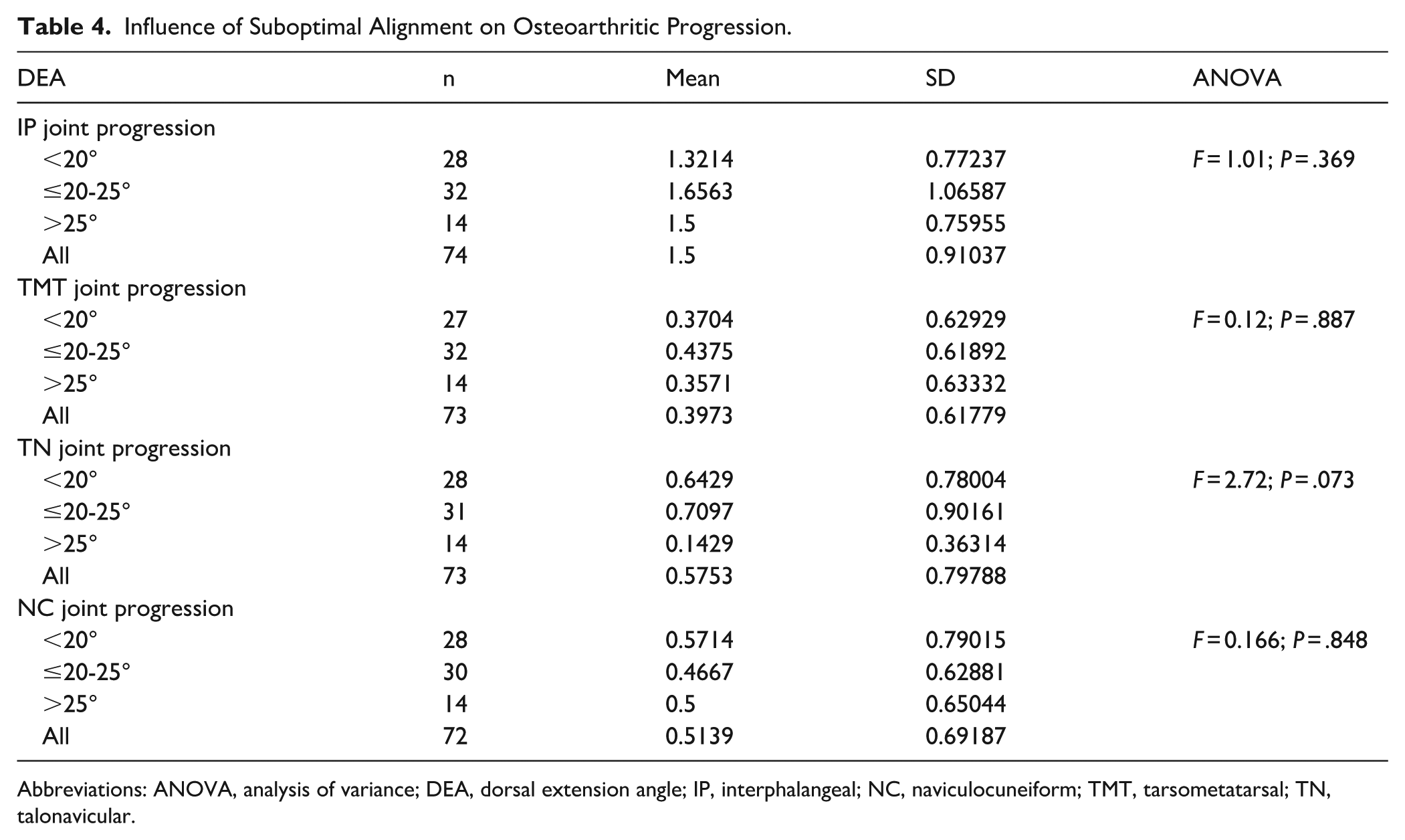
Abbreviations: ANOVA, analysis of variance; DEA, dorsal extension angle; IP, interphalangeal; NC, naviculocuneiform; TMT, tarsometatarsal; TN, talonavicular.
At final follow-up, 63.6% of patients were able to achieve active ground contact of the distal hallux in plantigrade foot position. The degree of dorsal extension, as categorized by the 3 DEA angle groups (<20°, 20°-25°, >25°), showed no influence on the ability to obtain ground contact.
As the HGA has not been previously described in the literature, an estimated target range for optimal alignment was derived based on established recommendations for MTP1 dorsal extension. Prior studies suggest an optimal dorsal extension angle of 20° to 25° following MTP1 arthrodesis. 9 Based on this reference range, the corresponding mean HGA—defined as the angle between the longitudinal axis of the proximal phalanx and the ground surface on weight-bearing lateral radiographs—was calculated to be 4.5° ± 2.9°.
Clinical Outcomes
At final follow-up, 90.9% (70 of 77) of patients rated their subjective satisfaction as good or excellent, whereas 9.1% (7 of 77) reported their outcome as fair; no patient was dissatisfied. Metatarsalgia was present in 10.4% of patients and 37.7% reported using insoles.
At final follow-up, the mean postoperative AOFAS HMI score was 79.9 ± 9.1, FAOS 86.4 ± 15.2, and FFI 18.5% ± 9.3%.
Neither the dorsal extension angle nor the HGA showed any correlation with the functional outcome scores.
Wound healing complications were significantly higher with dorsal plating (3 of 12 patients) than with screw fixation (P = .045, 95% CI 0.046, 0.250). Only 1 nonunion occurred in our study cohort, where a screw fixation was used and had to be revised with revision surgery.
Discussion
The present study examines the long-term effects of first metatarsophalangeal (MTP1) joint arthrodesis on adjacent joints of the medial column, with a particular focus on osteoarthritic progression.
It is well established that arthrodesis of one joint affects the biomechanics and the strain on adjacent joints, particularly in the foot where closely interconnected joints are subjected to substantial weight-bearing forces.5,10 Brodsky reported increased mechanical stress on the IP joint following MTP1 joint arthrodesis. Although osseous union of the MTP joint was achieved in 100% of cases undergoing simultaneous MTP and IP joint arthrodesis, a nonunion of the IP joint was observed in 40% of patients. 11 Alkaramany et al 12 evaluated the risk of secondary IP joint arthrodesis following isolated MTP1 arthrodesis and, based on a database analysis of 15 771 patients, reported that only 1% required a subsequent arthrodesis.
To our knowledge, the effects of MTP1 arthrodesis on the proximal joint row of the medial column have not been previously described.
Our findings support the observation of Brodsky et al, 11 as we found that the progression of IP joint arthrodesis was the most severe and frequent, where 66 of 77 patients had developed a progression of osteoarthritic changes and 33 of at least 2 grades on the Kellgren-Lawrence scale. In contrast, the more proximal joints showed relatively mild changes. The TMT1 joint was least affected, with 23 patients, and 5 of them had an osteoarthritic progression of at least 2 grades. In the NC and TN joint groups, 30 patients had a progression at the time of follow-up compared with preoperative; 6 patients in the NC and 8 in the TN joint group had progression of at least 2 grades. It is somewhat surprising that the TMT joint exhibited the least degenerative change, because one might expect it to experience increased strain after first MTP arthrodesis.10,13
We hypothesized that a lower fixed DEA and missing ground contact with the hallux should have negative effects on the adjacent joints, as it increases the lever arm of the first row and brings stress to adjacent joints. Therefore, we compared the progression of osteoarthritis in each joint with possible influential alignment factors like a suboptimal DEA (<20° and >25°)9,14 and whether ground contact with the distal phalanx of the hallux possible or not possible. No correlation was found between these parameters. This finding supports earlier observations by Traynor and Jastifer that proximal congruence may even improve post-fusion. 7 Age-related remodeling rather than mechanical failure likely accounts for the minimal proximal changes. 10 Notably, no patient in our cohort required a secondary surgical intervention because of adjacent-joint arthritis progression.
Several studies have discussed the optimal alignment in dorsal extension for the MTP1 arthrodesis, generally recommending approximately 20° to 25° of DEA.1,3,9 Surgeons often use a flat plate intraoperatively to simulate weight-bearing and determine its alignment before fixation. In our point of view, precisely measuring this angle during surgery is impractical because of limited intraoperative measurement options. Instead, we found it more practical to orientate on the longitudinal axis of the flat plate, simulating the contact surface and the proximal phalanx. We defined this orientation as the hallux-ground – angle. The mean HGA calculated of all patients in the optimal range of 20° to 25° of DEA was calculated as 4.5° ± 2.87°. Proper alignment is considered important to achieve the best functional results.14,15
Effective hallux ground contact has been thought to ensure a good push-off during gait and thereby prevent metatarsalgia.15,16 At final follow-up, only 63.6% of patients had sufficient ground contact, yet only 10.4% had developed metatarsalgia. We found no significant correlations between a suboptimal HGA and any of the clinical scores (AOFAS, FAOS, FFI), nor between HGA and the occurrence of metatarsalgia. This finding contrasts with biomechanical expectations that insufficient hallux alignment would lead to transfer lesions. 13 Similarly, Hoveidaei et al reported no significant correlation between postoperative radiographic alignment parameters of the first metatarsophalangeal joint and clinical outcome scores following MTP1 arthrodesis. These findings further support the notion that minor deviations in radiographic alignment may not necessarily translate into inferior functional outcomes or increased forefoot symptoms. 17
The MTP1 arthrodesis provides good functional outcomes and high satisfaction rates, consistent with other reports. Our mean AOFAS and FAOS scores were similar to those reported in other long-term studies,3,19 whereas the mean FFI in our cohort was slightly worse than values reported by others.3,15,16
Plate fixation has been increasingly adopted as the standard fixation technique for MTP1 arthrodesis over the past years, as it has fewer nonunion rates and a more stable alignment in long term follow-up.18,19 Cone et al 20 stated in their study that the use of an additional lag screw increases stability and therefore decreases the change of dorsiflexion angle significantly in long term follow-up. In our study in 12 patients, a dorsal plating—and in 65 patients a crossed-screw fixation—was used. Only 1 patient developed a painful nonunion and had to undergo revision arthrodesis of the MTP1 joint. In this patient, initially a crossed-screw fixation was used. Wound healing disorders, however, were significantly higher in the plate fixation cohort as we had 3 cases among the 12 (P = .045). This may be due to greater dorsal hardware prominence causing soft tissue irritation. Although a few studies have compared these fixation techniques, none have found a significant difference in wound complications between plating and screws.21,22
Our study has several limitations. The exploratory, single-center design and moderate sample size limit the generalizability of the findings and preclude definitive causal conclusions. Additionally, radiographic progression does not always correlate with clinical symptoms, and interobserver variability in grading is possible. To ensure a homogeneous study cohort, all revision procedures and patients with arthrodesis in adjacent joints were excluded. However, this methodologic decision may introduce a potential selection bias and potentially limit the generalizability of the study findings.
In summary, first MTP1 arthrodesis yields excellent long-term functional and radiologic outcomes with low complication rates. Although mild radiographic degeneration occurs—mainly at the IP joint—these findings have little clinical consequence.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007261441611 – Supplemental material for Long-term Outcomes After First Metatarsophalangeal Joint Arthrodesis: With Focus on Degenerative Changes on Adjacent Joints
Supplemental material, sj-pdf-1-fai-10.1177_10711007261441611 for Long-term Outcomes After First Metatarsophalangeal Joint Arthrodesis: With Focus on Degenerative Changes on Adjacent Joints by Simon Recheis, Dietmar Mattausch, Nils Kuehn, Harald Kindermann, Reinhold Ortmaier, Martin Bischofreiter and Thomas Stumpner in Foot & Ankle International
Footnotes
Ethical Considerations
The local Ethical Review Board Committee had no objection against the implementation of this survey registered at the Ethical Committee of the Johannes-Kepler University Linz as EK 1340/2023.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.