
Abstract
Background:
Lateral lengthening calcaneal osteotomy (LLOT, Evans and Hintermann) is widely used to treat progressive collapsing foot deformity (PCFD). In the Evans osteotomy, the cut is performed proximal to the calcaneocuboid joint, carrying a risk of violating the anterior or middle subtalar facet. Hintermann proposed a modified technique placing the osteotomy between the middle and posterior facets to reduce risks. Although anatomical studies have shown potential facet involvement, clinical data on the actual incidence and its impact on long-term outcomes remain scarce. This study aimed to determine the incidence of subtalar facet penetration after LLOT and to evaluate its effect on clinical and radiographic results.
Methods:
All patients aged ≥18 years who underwent LLOT (Evans or Hintermann osteotomy) at our institution between January 1, 2010, and December 31, 2020, were included. Postoperative computed tomography (CT) was performed 6 weeks after surgery to assess possible subtalar facet violation. At a minimum follow-up of 5 years, magnetic resonance imaging (MRI) was obtained to evaluate cartilage and ligament integrity. Clinical outcomes at the time of MRI were assessed using the Foot Function Index (FFI) and the American Orthopaedic Foot & Ankle Society (AOFAS) score. Demographic variables, including type of osteotomy and outcome measures, were compared between patients with and without facet penetration.
Results:
Thirty-one patients met inclusion criteria. Subtalar facet penetration was detected in 11 patients (35%) on postoperative CT. No significant differences were observed between groups with respect to demographic variables. MRI analysis revealed no relevant differences in cartilage degeneration. FFI and AOFAS scores were comparable between groups.
Conclusion:
Subtalar facet penetration occurred in one-third of patients after LLOT (Evans and Hintermann). With the numbers available, no significant differences in clinical or radiographic outcomes were detected at a minimum 5-year follow-up, suggesting that minor facet violations may have limited clinical relevance.
Level of Evidence:
Level III, retrospective cohort study.
Keywords
Introduction
Progressive collapsing foot deformity (PCFD) is characterized by hindfoot valgus, forefoot abduction, and medial arch collapse.19,25 Lateral column lengthening (LCL) procedures, such as Evans and Hintermann osteotomies, are commonly used to correct PCFD by restoring the medial longitudinal arch and realigning the forefoot.19,25
In the traditional Evans osteotomy, a transverse osteotomy of the calcaneus is made 10 to 20 mm proximal to the calcaneocuboid joint to allow the insertion of a bone graft and thus lengthening of the lateral column.7,9,15,27,30,33 However, anatomical studies have shown that the anatomy of most calcanei shows a converging anterior and middle joint.3,17 As a result, this technique likely damages the anterior and middle facets of the subtalar joint in most cases, which can lead to postoperative complications. 3
To avoid the risk of a destabilization of the anterior calcaneal process, while preserving medial stabilizing structures and realizing a more physiological correction, Hintermann14,34 proposed a modified LCL osteotomy positioned between the middle and posterior facets of the calcaneus. Biomechanical analyses suggest that this modification reduces stress to the subtalar joint and may preserve joint integrity.13,37
Because of anatomical conditions, Hinterman osteotomy is hypothesized to lead to less subtalar joint violations compared with the Evans osteotomy. This could be verified in a cadaver study with 1/7 (14.3%) joint violations following the Hintermann osteotomy compared with 4/7 (57.1%) with the Evans osteotomy. 11
Despite these theoretical advantages, clinical data regarding the incidence of subtalar facet penetration and its potential impact on long-term outcomes remain limited.12,36
Therefore, the aim of this study was to determine the incidence of subtalar facet penetration following lateral lengthening calcaneal osteotomy and to evaluate its influence on clinical and radiographic outcomes at mid-term follow-up.8,37
Methods
This retrospective cohort study examined patients who underwent lateral lengthening calcaneal osteotomies for flexible flatfoot deformity using the Evans or Hintermann technique at a single university hospital between January 1, 2010, and December 31, 2020 (Figure 1). It was approved by the local research ethics committee (KEK No. 2022-01669).
Patient recruitment. LCL, lateral calcaneal lengthening.
Exclusion criteria were individuals aged <18 years, persons incapable of judgment or considered vulnerable, pregnant women, and those who refused the secondary use of their health data. All patients had received a postoperative computed tomography (CT) control 6 weeks after surgery.
A pelvic crest allograft was used as a spacer for both the Evans and Hintermann osteotomies, with a 3.5-mm titanium screw inserted from the anterior calcaneal process to the posterior aspect to stabilise the osteotomy.
To investigate the influence of joint penetration on clinical outcome and subtalar joint degeneration, all patients were invited to a clinical assessment 1 year postoperatively and a clinical and radiographic assessment with a minimum follow-up of 5 years. We created 2 groups: one consisting of patients who experienced subtalar facet penetration as a result of the operation and another without joint facet injury.
Clinical Follow-up
An assistant or senior physician performed a clinical follow-up 1 year postoperatively and at a minimum follow-up of 5 years. Clinical outcomes at both time points were compared with preoperative values. Patients completed the Foot Function Index (FFI), the Tegner Score, and the American Orthopaedic Foot & Ankle Society (AOFAS) score.1,2,21,29 Additionally, data on surgical data (additional Cotton osteotomy, flexor digitorum longus transfer, and spring ligament repair) were collected during the final follow-up.
Radiographic Analysis
A senior radiologist conducted radiographic follow-up. Six weeks after surgery, a CT scan was obtained to evaluate the anterior, medial, and posterior facets of the subtalar joint for penetration, step formation, and other joint surface damage. Standard radiographs (ankle AP, foot lateral, and foot dorsoplantar views) were taken to evaluate longitudinal arch collapse of the foot based on the Meary angle, talonavicular coverage, and the talocalcaneal angle. MRI scans were performed at the final follow-up to assess subtalar joint degeneration, which is defined as cartilage defects involving more than 50% of the joint’s depth. 24 The scans also evaluated tendon integrity with regard to partial- or full-thickness tears.
Demographic and clinical data, including age, sex, body mass index (BMI), the American Society of Anesthesiologists (ASA) physical status classification, and treatment course, were extracted from medical records. Radiographic parameters were evaluated, and the results were compared with the clinical outcomes. During postoperative follow-up, data collection included whether patients underwent surgical revision. All 31 patients included in the study contributed complete data for all key outcomes (FFI, AOFAS, and MRI assessments), and no missing values were present.
Statistics
Statistical analysis was performed using IBM Statistics (IBM Corp) 18 and Stata (StataCorp). Differences between groups were compared with Fisher exact test, Kruskal-Wallis test, Wilcoxon rank-sum test (for nonnormally continuous distributed variables), or t tests (for normally distributed continuous variables). Univariate logistic regression analyses were carried out to identify clinical and radiographic parameters associated with facet joint penetration (facet joint penetration present vs absent on postoperative CT scans). A P value of <.05 was considered statistically significant.
A multivariable linear regression analysis was performed to evaluate the association between facet penetration and clinical outcome (FFI) while adjusting for potential confounders including age and body mass index. To avoid model overfitting, the number of covariates included in the model was limited.
Results
Thirty-one patients met the inclusion criteria and were included in the final analysis. Postoperative CT demonstrated subtalar facet penetration in 11 patients (35%; Figure 2). Of the 31 LCL procedures performed, 26 were Hintermann osteotomies (9 with facet injury, 35%) and 5 were Evans osteotomies (2 with facet injury, or 40%). Of the Evans osteotomies, 1 involved an anterior facet injury and 1 involved a medial facet injury. In the Hintermann osteotomy, the medial facet was injured 7 times and the posterior facet twice.
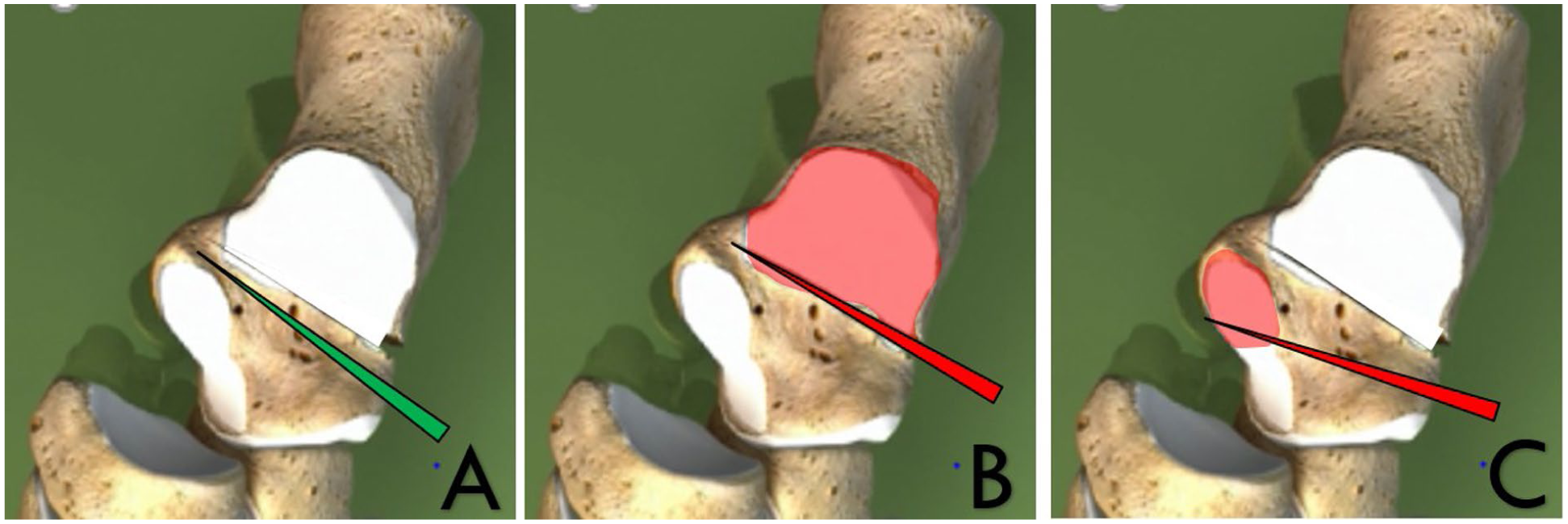
Facet joint penetration: (A) Correct Hintermann osteotomy, (B) penetration of the posterior facet, (C) penetration of the medial facet.
There were no statistically significant differences between patients with and without facet penetration (Table 1). In detail, there were no significant differences in age (median 55 vs 61 years, P = .742), gender distribution (64% vs 55% male, P = .642), or BMI (median 26.9 vs 26.0, P = .522). Other factors such as diabetes (0% vs 10%, P = .198), smoking status (27% vs 15%, P = .079), ASA classification (P = .740), and side of surgery (P = .186) were also comparable. 20 The mean follow-up duration was comparable between both groups 77 vs 78 months (P = .940). No statistically significant association was found between facet joint penetration and revision surgery during follow-up (27% vs 35%, P = .490; Table 2). Revisions included 7 times implant removal, 1 osteophyte resection in the Lisfranc joint, and 2 medializing calcaneal osteotomies for persistent deformity. All patients with facet penetration underwent implant removal only. Also, in this study population, no early revisions were performed. There were no significant differences in additional procedures (Cotton osteotomy, flexor digitorum longus transfer, spring ligament repair) between groups (Table 2). There was no significant difference in facet penetration between Evans and Hintermann osteotomies (Evans 40%, Hintermann 35%, P = .595).
Baseline Characteristics of the Groups.
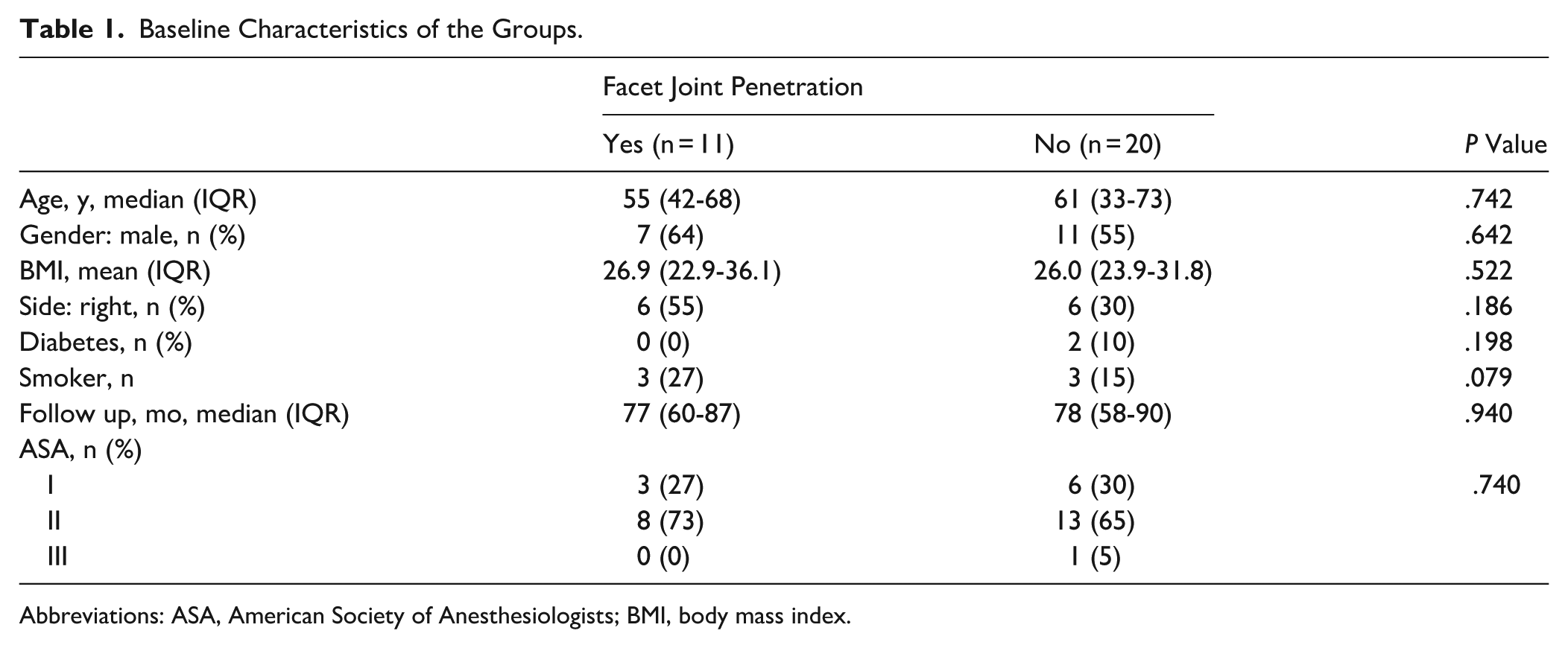
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index.
Association of Surgical Parameters With Facet Joint Penetration.
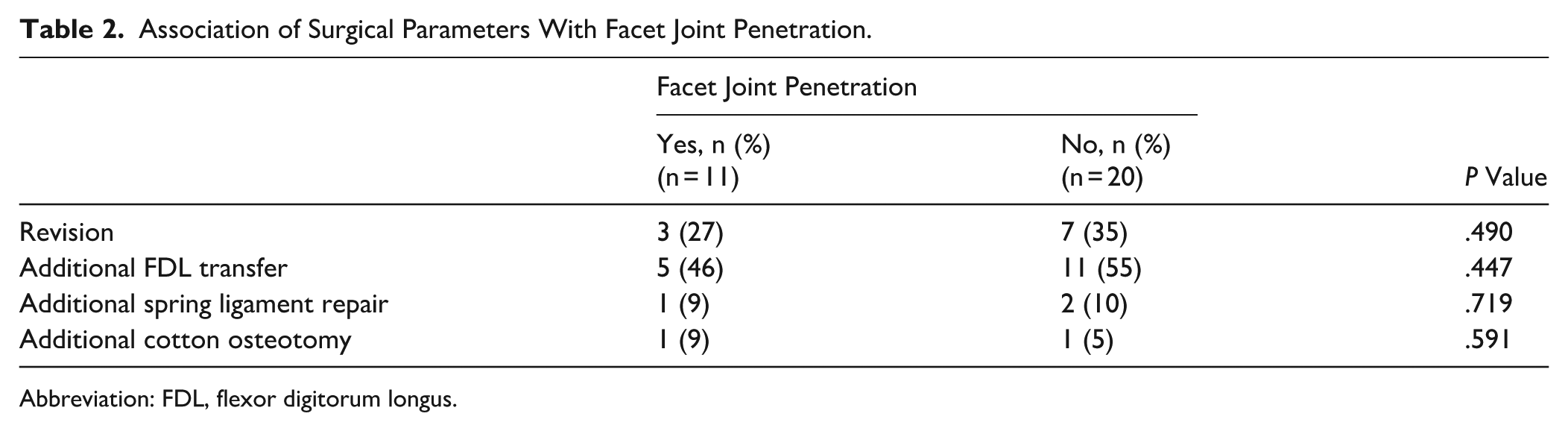
Abbreviation: FDL, flexor digitorum longus.
Clinical outcomes were also comparable. The Foot Function Index and AOFAS scores did not differ significantly between patients with and without facet penetration between groups (FFI last follow-up mean [SD]: 47 [46] vs 77 [53], P = .119; AOFAS mean [SD]: 80 [19] vs 66 [23], P = .092; Table 3).
Association of Clinical Parameters With Facet Joint Penetration.
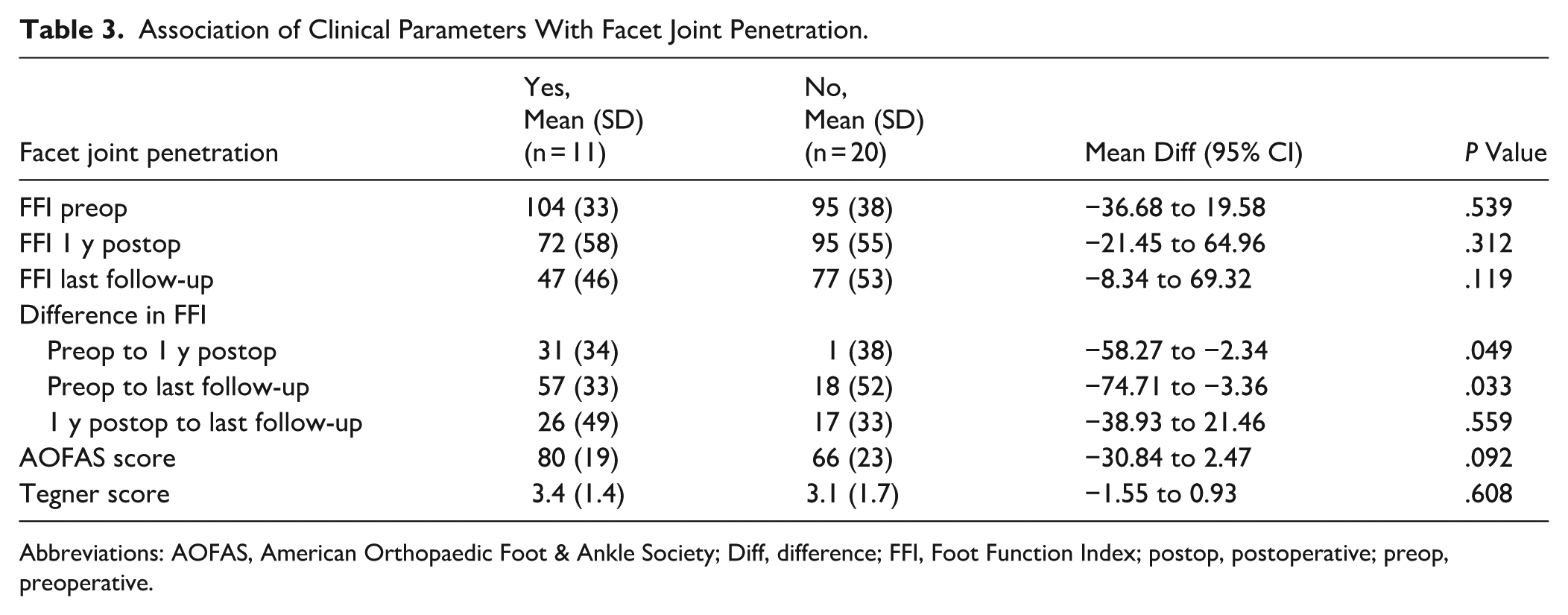
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; Diff, difference; FFI, Foot Function Index; postop, postoperative; preop, preoperative.
Paradoxically, the difference between the FFI preoperatively and 1 year postoperatively (mean [SD]: 31 [34] vs 1 [38], P = .049) and the difference between the FFI preoperatively and the FFI at the last follow up (mean [SD]: 57 [33] vs 18 [52], P = .033) was significantly different and overall better in the facet penetration group.
MRI evaluation at follow-up demonstrated no statistically significant differences in cartilage pathology of the anterior, medial, or posterior subtalar facets between the 2 groups (Supplemental Table S1). Also, the presence of osteoarthritis in the ankle, calcaneocuboidal, and Lisfranc joints was not significantly associated with facet penetration (Supplemental Table S1). Similarly, there was no association between facet penetration and tendinopathy in any of the examined structures, including the flexor/extensor groups and peroneal tendons (P > .1 in all cases, Supplemental Table S1). Even when measuring the joint in patients with facet joint injury, only 2 patients showed a step of 1-2 mm (18%), whereas 9 of 11 patients (82%) showed no step in the joint facet. Overall, calcaneocuboid joint osteoarthritis was present in 11 of 31 patients (35.5%), with comparable rates in patients with and without facet penetration (4/11 [36.4%] vs 7/20 [35.0%]; P = .364).
In the multivariable linear regression analysis with FFI at final follow-up as the dependent variable, facet penetration was not significantly associated with the FFI score after adjustment for age and BMI (β = −30.05, 95% CI −68.7 to 8.6, P = .139; Table 4).
Multivariable Regression Analysis for Clinical Outcome (FFI at Last Follow-up).
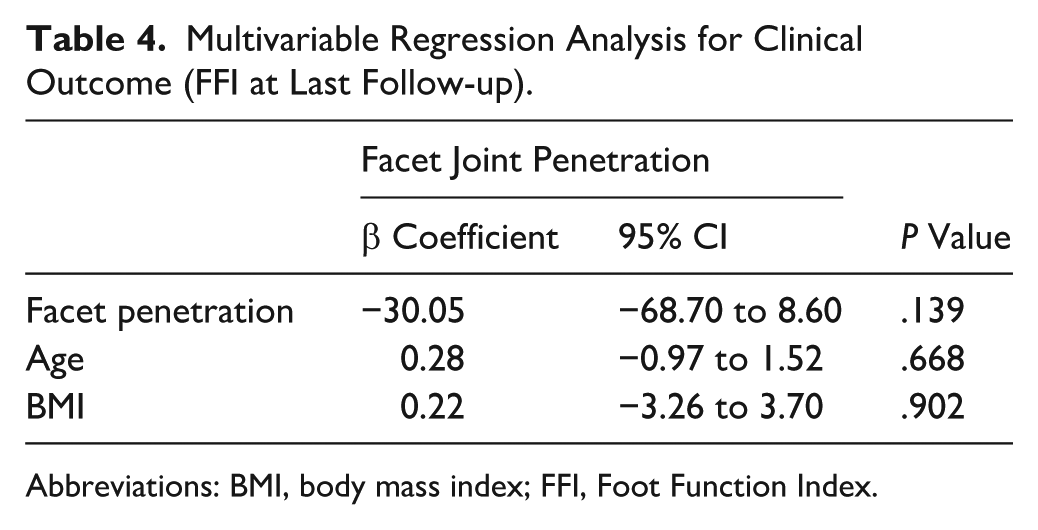
Abbreviations: BMI, body mass index; FFI, Foot Function Index.
Discussion
The present study investigated the incidence of subtalar facet penetration in lateral column lengthening osteotomies and its impact on midterm clinical and radiographic outcomes.
Our findings demonstrate that facet penetration occurred in approximately one-third of cases, which is comparable to in vitro studies, 0% to 57%.3,4,11,28 The relatively high incidence of facet penetration observed in this study may partly reflect the use of routine postoperative CT imaging, which allows detection of small articular violations that might otherwise remain undetected. Regarding our study results, the Hintermann osteotomy did not prove to be more effective than the Evans procedure in terms of subtalar facet penetration.
Interestingly, it was not associated with worse clinical or radiographic outcomes. One possible explanation for the lack of influence of joint injury on the clinical or radiographic outcome may be explained by the fact that in most cases facet penetration did not lead to step or gap formation in our study group. This suggests that the absence of a significant intra-articular step, rather than the penetration itself, likely explains why clinical outcomes were not adversely affected. Another explanation is that the clinical relevance of the facet injury is minor, likely because the facet joint contributes only partially to load transmission and stability in the affected region; this would be consistent with the findings of Magnan et al, 22 who also found no correlation between facet joint injury and clinical outcome following calcaneal fractures.
Other authors, such as Ettinger et al, 11 describe, for example, an injury to the peroneus brevis and longus tendon in about 14%, a finding we could not replicate. In line with our study, Shih et al 32 also reported that radiographic assessment of a modified extraarticular lateral column lengthening procedure showed no increased prevalence of osteoarthritis or tendinopathy following lateral column lengthening osteotomies. And in the clinical assessment, we also have the same results as Shih et al, 10 that clinical outcome scores did not differ significantly after lateral column lengthening osteotomies, whether a facet penetration had occurred or not.
The only statistically significant finding regarding facet penetration was the difference in the FFI between the preoperative assessment and the 1-year postoperative follow-up and between the preoperative assessment and the last follow-up examination when comparing the 2 groups. Surprisingly, the group with facet penetration showed significantly better results. Although differences in FFI and AOFAS scores were not statistically significant, they exceeded reported minimal clinically important difference (MCID) thresholds of approximately 7 to 12 points.5,26 This suggests potential clinical relevance; however, given the small sample size and high variability, these findings should be interpreted with caution. High variability and the limited sample size indicate that this study may have been underpowered, and results should be interpreted cautiously. In our view, this is a bias in the retrospective study design. However, it underscores our statement that patients with facet joint penetration do not experience worse outcomes in the midterm. This supports the potential effectiveness of LCL procedures in symptom reduction, regardless of facet penetration.
These results are consistent with recent anatomical and clinical studies suggesting that subtalar facet violation may not necessarily translate into worse midterm outcomes.10,16,31,35
Although the number of patients was small, our subgroup analysis showed no relevant difference between Evans and Hintermann osteotomies. This is also similar to other results. Wu et al 35 and Ragab et al 31 compared Evans and Hintermann osteotomies and similarly reported no clear superiority regarding radiographic correction or clinical results, although the Hintermann technique was designed to minimize facet penetration risk. 16 Furthermore, Xu et al 37 demonstrated in finite element and cadaveric analyses that graft positioning and osteotomy type can alter subtalar loading patterns, but such changes may not inevitably progress to clinically relevant degeneration. Our data confirm these biomechanical insights in a mid- to midterm clinical setting.
Interestingly, the lack of radiographic differences in cartilage degeneration between our 2 groups aligns with prior observations that radiographic osteoarthritis following hindfoot procedures does not always correlate with clinical symptoms.6,23 This underscores the multifactorial nature of postoperative outcomes in PCFD, in which soft tissue balance, correction of hindfoot alignment, and patient-related factors may outweigh subtle joint surface changes.6,23
Limitations
Several limitations must be acknowledged. First, this study was retrospective and included a relatively small sample size, which may limit the statistical power to detect small differences between groups. Second, no a priori power analysis was performed because of the exploratory nature of the study. Third, the AOFAS score was used as part of the clinical assessment, although it has recognized limitations as a patient-reported outcome measure. Finally, this was a single-center study, which may limit the generalizability of the findings.
Conclusion
Subtalar facet penetration occurred in approximately one-third of patients undergoing lateral lengthening calcaneal osteotomy. With the numbers available, no significant differences in clinical or radiographic outcomes were detected at midterm follow-up, suggesting that limited facet violation may have minimal clinical relevance.
Supplemental Material
sj-docx-2-fai-10.1177_10711007261450617 – Supplemental material for The Incidence of Subtalar Facet Penetration and Its Impact on Clinical and Radiographic Outcome in Lateral Lengthening Calcaneal Osteotomies
Supplemental material, sj-docx-2-fai-10.1177_10711007261450617 for The Incidence of Subtalar Facet Penetration and Its Impact on Clinical and Radiographic Outcome in Lateral Lengthening Calcaneal Osteotomies by Fabrice A. Scheurer, Daniel Suter, Benjamin Fritz, Maria A. Smolle, Silvan Beeler, Arnd Viehöfer and Stephan Wirth in Foot & Ankle International
Supplemental Material
sj-pdf-1-fai-10.1177_10711007261450617 – Supplemental material for The Incidence of Subtalar Facet Penetration and Its Impact on Clinical and Radiographic Outcome in Lateral Lengthening Calcaneal Osteotomies
Supplemental material, sj-pdf-1-fai-10.1177_10711007261450617 for The Incidence of Subtalar Facet Penetration and Its Impact on Clinical and Radiographic Outcome in Lateral Lengthening Calcaneal Osteotomies by Fabrice A. Scheurer, Daniel Suter, Benjamin Fritz, Maria A. Smolle, Silvan Beeler, Arnd Viehöfer and Stephan Wirth in Foot & Ankle International
Footnotes
Acknowledgements
The authors thank the clinical and administrative staff of the Department of Orthopaedics, Balgrist University hospital, for their support in patient data retrieval.
Ethical Considerations
This study was approved by the Ethics Committee of Zurich (KEK Nr: 2022-01669). All patients in this study between January 2010 and December 2020 provided written informed consent allowing the use of their medical data for research purposes. The study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
Not applicable. No identifying images or personal details of individual participants are included in this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by internal funding from Balgrist University Hospital (Zurich, Switzerland) for X-Ray and MRI examinations (CHF 12,600).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available because of Swiss medical data protection regulations. Deidentified data may be made available from the corresponding author upon reasonable request and with approval from the Ethics Committee of Zurich.
Supplemental material
Supplementary material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.