
Abstract
Background:
Early results of the fixed-bearing total ankle arthroplasty (TAA) have demonstrated improvement in patient-reported outcome measures (PROMs) for patients with end-stage ankle arthritis. The purpose of this study is to update the previously reported PROMs for the largest cohort of US patients undergoing modern fixed-bearing TAA with the Salto Talaris implant.
Methods:
A retrospective review was completed of 300 consecutive patients who underwent implantation with 321 modern fixed-bearing TAA by a single surgeon. PROMs were collected prior to surgery, at 3 and 6 months, and yearly thereafter. Collected outcome measures included Veterans RAND 12-Item Health Survey (VR-12), Ankle Osteoarthritis Scale (AOS), and visual analog pain scale (VAS). Presurgical and latest available follow-up (>2 years) PROMs were compared using a mixed effect linear regression with significance level alpha = 0.01 using a Bonferroni-adjusted significance threshold to account for testing across the 5 PROMs.
Results:
Of the 321 TAAs, an updated 300 procedures (282 patients) had a minimum 2-year follow-up. The average follow-up was 75.3 (range, 24-193.9) months. The mean physical VR-12 score increased significantly from prior to surgery to latest follow-up, while mental VR-12 scores did not (P < .001 and P = .608, respectively). AOS pain and disability scores and VAS pain scores improved significantly (P < .001). Clinical significance of PROMs was assessed using previously reported minimal clinically important differences (MCIDs), and the average changes in VR-12 physical composite score, AOS Pain and Disability scores, and VAS scores from preoperation to latest follow-up were all greater than the respective MCID values.
Conclusion:
At midterm follow-up, fixed-bearing TAA with the Salto Talaris implant was associated with improvement in quality of life, pain, and disability.
Level of Evidence:
Level IV, case series.
This is a visual representation of the abstract.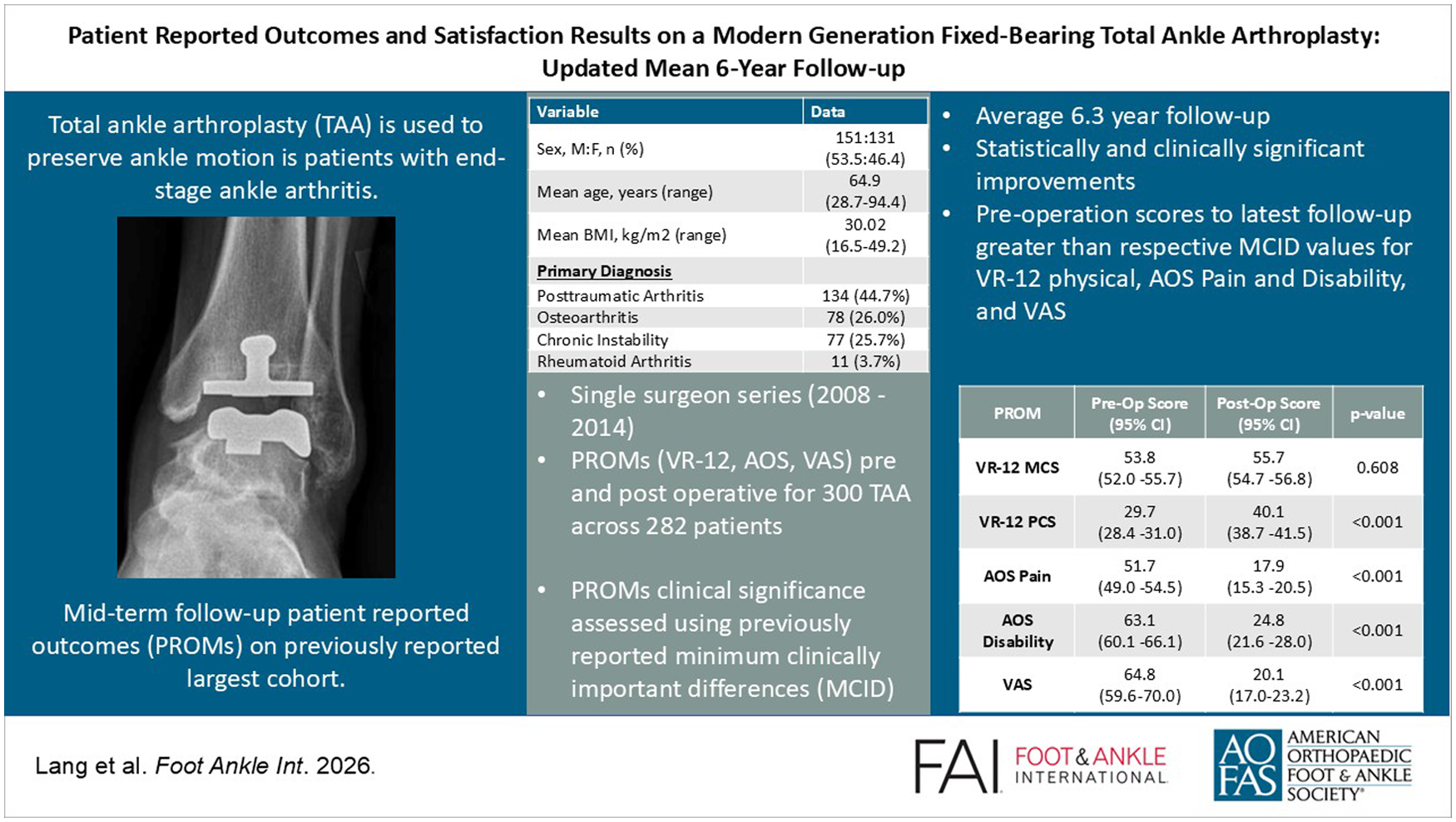
Introduction
The incident rate of total ankle arthroplasties (TAA) performed in the United States (US) has increased by 120.8% from 2009 to 2019, and this number is only expected to increase in the coming years.1,2 This rising popularity may be contributed to the equivalent, and in some cases even improved, outcomes of TAA compared with ankle arthrodesis, which has previously been the gold standard procedure in treating ankle arthritis.3-6
For patients considering TAA, the primary concern is often the expected recovery and clinical outcomes following the operation, rather than the technical aspects of the procedure itself. For this reason, there is a need to understand patient-reported outcome measures (PROMs) of TAA to help physicians guide patient expectations preoperatively. Early follow-up studies have shown that patients report improved pain, function, and quality of life at short-term follow-ups.7-13 Beyond these short-term results, a recent review of the quality of current TAA research revealed a need for more long-term outcome studies to help improve the understanding of TAA PROMs. 1
The Salto Talaris (Smith & Nephew) is a commonly used TAA implant that features a smooth surface tibial component, a rounded talar component, and a ultrahigh-molecular-weight polyethylene fixed bearing. 14 Previously, we reported the short-term PROMs from 300 consecutive patients who underwent TAA with the Salto Talaris implant. 7 The purpose of the present study is to report the updated midterm PROMs of this same cohort of patients. We hypothesize that PROMs collected at midterm follow-up after TAA with the Salto Talaris implant will be significantly improved from preoperative scores and will not differ by time to latest follow-up.
Methods
This institutional review board–approved study included patients that received a TAA implant from a single surgeon (J.C.C.). Three hundred consecutive patients received a total of 321 primary TAAs (21 bilateral) from May 2008 to January 2014. Of these procedures, data sets with a minimum of a 2-year follow-up were updated and collected for 300 TAA procedures (282 patients). At the time of this report, data for 21 ankles were not included because of not having minimum 2-year data (17), or they were lost to follow-up (4). Forty-six patients included in this cohort are now deceased after their latest follow-up.
All patients received the Salto Talaris ankle implant (Smith & Nephew), and the operation was performed according to the manufacturer’s standard technique guide. Following surgery, patients were hospitalized for 1 to 2 days. Patients were discharged in a plaster splint once pain was appropriately managed, and they were adequately mobile. After 2 weeks in the splint, patients were placed in an Aircast XP walker (Donjoy Orthopedics, LLC) for an additional 4 weeks. Patients began physical therapy following this 4-week period. One day after surgery, patients could be 50% weightbearing with assisted devices and by 6 weeks postoperatively the patient progressed to 100% weightbearing, given that there was radiographic evidence of implant incorporation. A standardized 5-view weightbearing set of radiographs was taken at each patient’s visit. These views included anteroposterior (AP), lateral and oblique ankle, maximum dorsiflexion, and maximum plantarflexion.
Data collected included patient demographics, ancillary procedures at the time of the index TAA, any complication (intra-, peri-, and postoperative) related to the index TAA through the latest clinical follow-up, and PROMs. PROMs were collected for each patient pre- and postoperatively at 3 months, 6 months, 1 year, and yearly thereafter. As this is an updated longitudinal study, this report will only focus on preoperative measures, and postoperative measures collected at the patient’s latest available follow-up (≥2 years). Clinical significance of PROMs was assessed using previously reported minimal clinically important differences (MCIDs) in similar orthopaedic populations.15-17 The PROMs collected included the Veterans RAND Health Survey (VR-12),18-20 Ankle Osteoarthritis Scale (AOS), 21 and the visual analog scale for pain (VAS).22,23 The VR-12 is a 12-question survey designed to evaluate mental (MCS) and physical (PCS) quality of life across 8 domains. The results of the survey are normalized to a score of 50 with an SD of 10.18-20
Statistical Analysis
To account for within-patient variability, a mixed effect linear regression was performed to analyze the change in PROMs pre- to postoperatively and the difference in postoperative PROMs scores as a function of points per day following surgery. Pre- and postoperative scores and days to latest follow-up where set as the fixed effects, and patient identify was set as the random effect. Both analyses were performed in R (R version 2025.05.1+513). To account for testing across 5 patient-reported outcomes, a Bonferroni-adjusted significance threshold of alpha = 0.01 was used for both analyses.
Results
The mean age for this cohort of 282 patients at the time of their index TAA was 64.9 (range, 28.7-94.4) years, and 53.5% (151) were male. The primary preoperative diagnosis for TAA in this cohort of patients was posttraumatic arthritis (44.7%) (Table 1). Two hundred thirty-one index TAA procedures included were concomitant, and the most common were Achilles or gastroc tendon lengthening (123; 41%), lateral ligament repair (90; 30.0%), hardware removal (41; 13.78%), heterotopic osteophyte excision (17; 5.7%), deltoid repair or release (14; 4.7%), subtalar fusion (10; 3.3%), or talonavicular fusion (5; 1.7%). The mean time from surgery to the latest follow-up was 75.3 (range, 24-193.9) months.
Preoperative Demographic, Diagnosis and COFAS type.
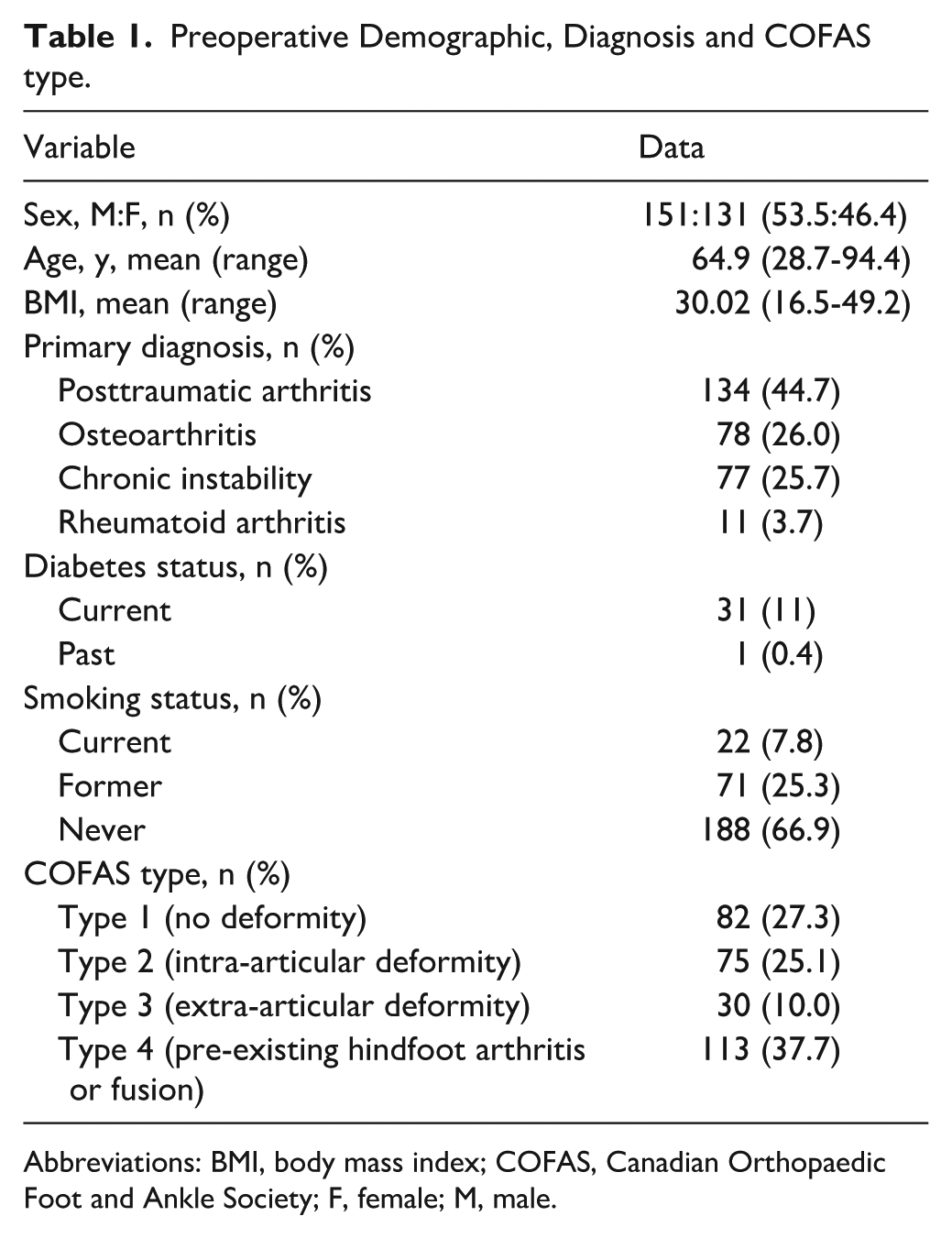
Abbreviations: BMI, body mass index; COFAS, Canadian Orthopaedic Foot and Ankle Society; F, female; M, male.
All patient-reported outcomes, except VR-12 MCS scores, improved significantly from preoperative to the latest follow-up (P < .001) (Table 2). With the numbers available, no significant difference in postoperative PROMs by follow-up duration could be detected (all P > .01; Table 2).
Patient-Reported Outcome Measures (PROMs) From Preoperatively to Latest Follow-up.
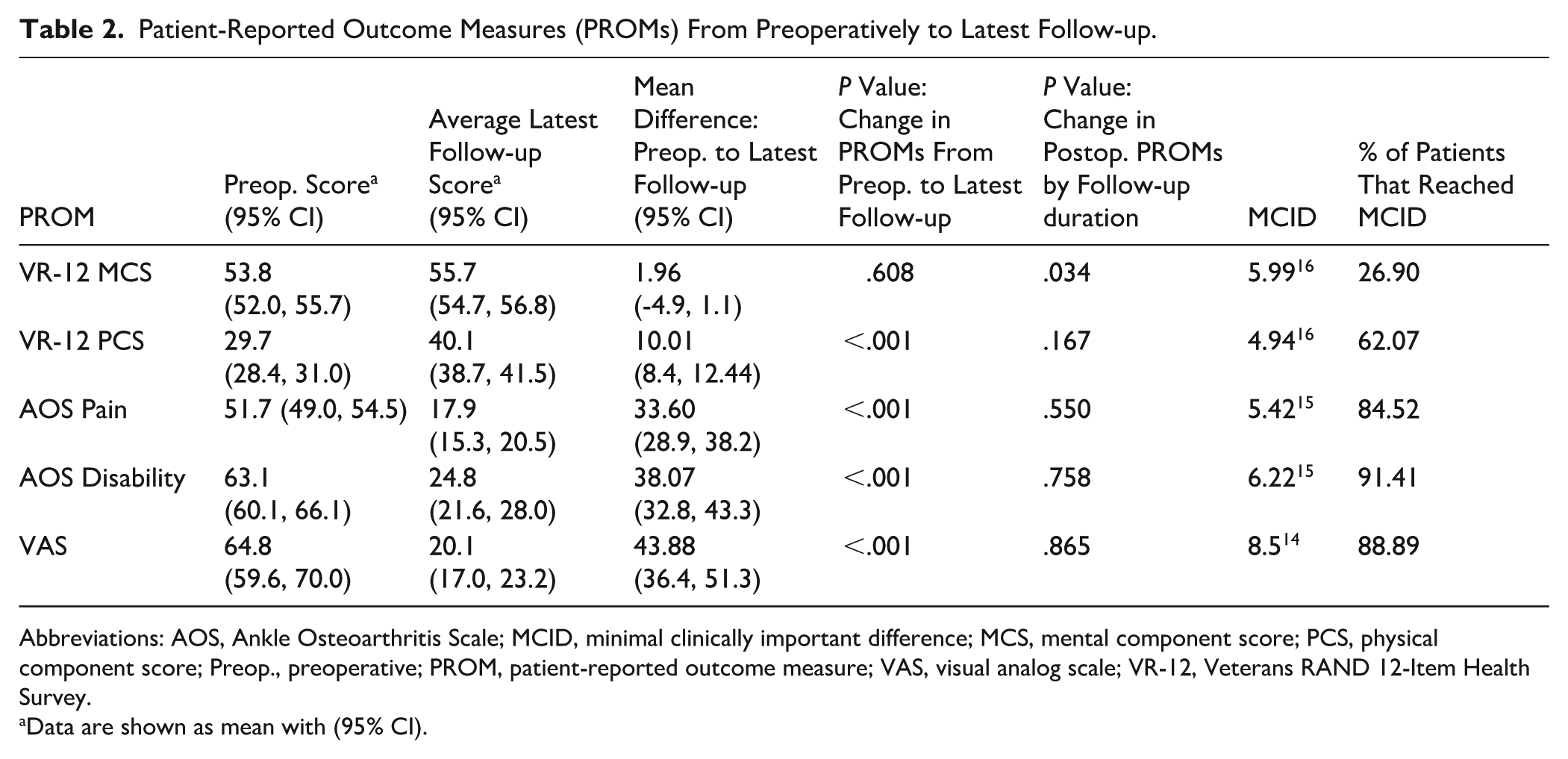
Abbreviations: AOS, Ankle Osteoarthritis Scale; MCID, minimal clinically important difference; MCS, mental component score; PCS, physical component score; Preop., preoperative; PROM, patient-reported outcome measure; VAS, visual analog scale; VR-12, Veterans RAND 12-Item Health Survey.
Data are shown as mean with (95% CI).
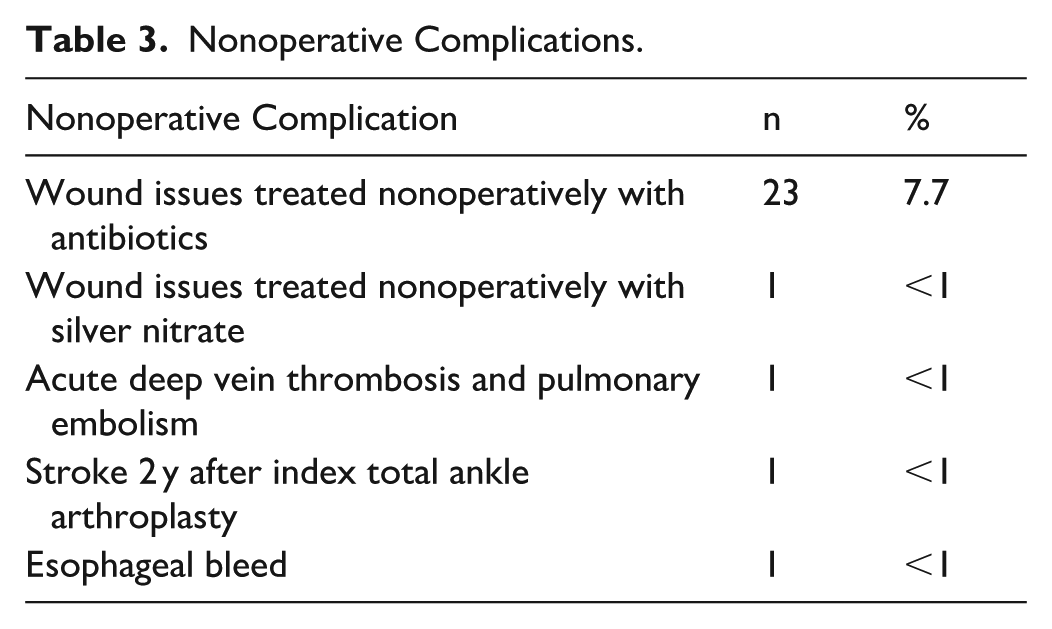
Seventy-five ankles (74 patients) experienced at least 1 complication following the index TAA, including nonoperative complications (Table 3). Fifty-two ankles developed 1 or more intraoperative or postoperative complications that, if left unaddressed, had the potential to compromise the integrity of the TAA prosthesis (Table 4). The early weightbearing of 50% did not impact or increase any complications. One patient experienced a medial malleolar fracture intraoperatively that required a screw fixation. Four ankles required irrigation and debridement after the index TAA, and 2 ultimately underwent free flap surgery.
Nonoperative Complications.
Series of Reoperation and Revision Coding by COFAS.
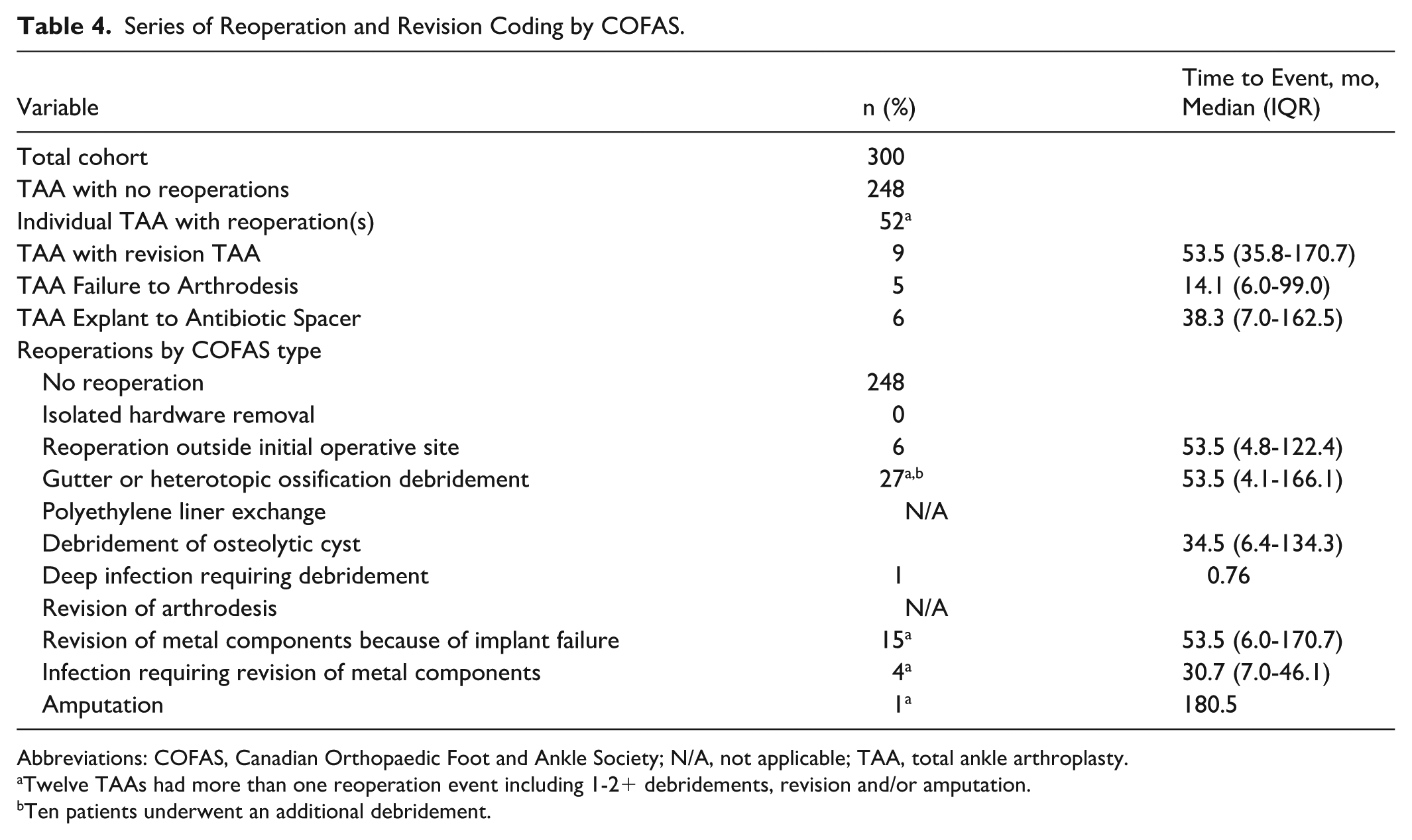
Abbreviations: COFAS, Canadian Orthopaedic Foot and Ankle Society; N/A, not applicable; TAA, total ankle arthroplasty.
Twelve TAAs had more than one reoperation event including 1-2+ debridements, revision and/or amputation.
Ten patients underwent an additional debridement.
Overall, implant survivorship for this group of patients was 93.3%, with the endpoint defined as any reoperation of ankle components. Twenty ankles required reoperation of a TAA component because of at least 1 complication affecting the integrity of the prosthesis. There were 9 revision total ankle surgeries, 5 conversions to arthrodesis using a femoral head allograft (FHA), and 6 failures with removal of the index TAA prosthesis to antibiotic spacer (Table 5). The mean age in this TAA failure group was 58.6 years, with 50% male patients. The 9 revised total ankle procedures included a polyethylene exchange and a revision of the tibial component (1), talar component (4), and both (4). One patient ultimately underwent a below-the-knee amputation (BKA) 15 years after his primary TAA. He was a 28.7-year-old male at the time of the index TAA after post-traumatic arthritis due to a motorcross accident. At 13.5 years after the index TAA, he underwent a medial gutter debridement and developed a superficial wound infection and within a month had a second debridement, an infected TAA that led to an explant of the TAA components with placement of an antibiotic spacer. At 13.8 years, the spacer was then removed, and a revision TAA was completed; he later developed chronic pain and a BKA was performed 15 years after the index TAA.
Reoperations With Compromised TAA Component in 20 Ankles.
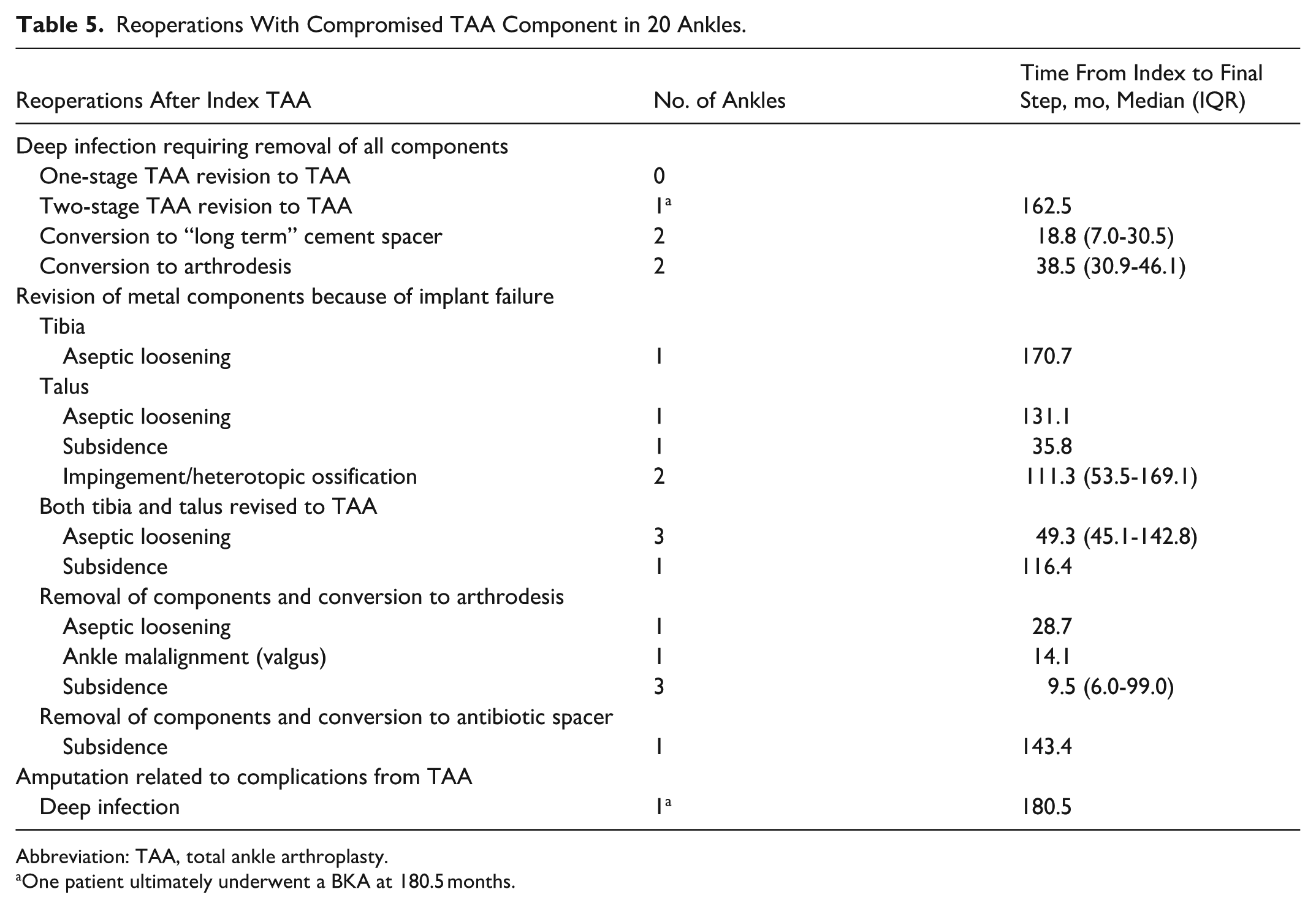
Abbreviation: TAA, total ankle arthroplasty.
One patient ultimately underwent a BKA at 180.5 months.
Discussion
The primary goal of this study was to report the updated midterm PROMs from our previously published short-term results. This study did not include analysis of radiographic data, range of motion, or other commonly reported biomechanical factors, as our primary aim was to understand a patient’s perception of their recovery. The results of this study provide valuable insight into patients’ perspectives of their long-term recovery after TAA, which can be used by physicians to help guide and manage expectations for future TAA patients.
The primary finding of this study revealed that all PROMs, besides VR-12 MCS, were significantly higher at the latest follow-up visit than preoperative measures. At an average of 75.3 months after TAA operation, patients reported statistically significant improvements in physical quality of life, pain, disability, and overall function compared with their preoperative assessments. Additionally, the reported average change in VR-12 PCS, AOS Pain and Disability, and VAS scores from preoperation to latest follow-up were greater than the respective MCID values. This indicates that these improvements in quality of life, pain, and disability were clinically significant to patients.
These results are consistent with previously published midterm outcomes for the Salto Talaris fixed-bearing TAA. A study by Nunley et al 24 investigated the PROMs for 43 patients who received Salto Talaris fixed-bearing implants at an average of 4.5 years following surgery. This study used VAS, 36-Item Short Form Health Survey (SF-36), Foot and Ankle Disability Index (FADI), Short Musculoskeletal Functional Assessment (SMFA), and American Orthopedic Foot & Ankle Society (AOFAS) ankle-hindfoot scores and found that all outcomes improved significantly from preoperation to latest follow-up. Additionally, a study by Stadler et al 25 on a cohort of 171 patients with the Salto Talaris implant found that all components of the AOFAS score improved from before surgery to a mean 7.2-year follow-up. Similarly, a study with 72 patients by Stewart et al 26 found a significant increase in VAS, AOFAS, SF-36, and SMFA scores from the preoperative period to 5 years postoperatively for patients receiving the Salto Talaris fixed-bearing TAA. Lastly, a multicenter study with 314 patients and a minimum 4-year follow-up by Mathews et al 27 found improvements in pain and the physical component of the SF-36 1 year following surgery and remained steady through their 9-year follow-up.
Although limited long-term follow-up exists for Salto Talaris implant, the results of the present study are comparable to other widely used TAA implants. A recent study by Bianchi et al 28 on the long-term follow-up (minimum 10-year follow-up) of Bologna-Oxford TAA (Istituto Ortopedico Rizzoli, Bologna, Italy and Oxford Orthopedics Engineering Center, Oxford, UK) reported that patients saw a decrease in VAS scores from 8.5 to 2.9 from pre- to postoperative time points (P < .01) and an increase in AOFAS score from 28.6 to 11.8 (P < .01). Additionally, a study by Yoon et al 29 reported that TAA patients with the HINTEGRA prothesis (Integra Life Sciences, Newdeal SA) experienced significant improvement in VAS, AOFAS, and AOS pain and disability scores from the preoperative visit to 2 years, 4-6 years, and 10 years postoperatively.
In contrast to all other PROMs investigated, VR-12 MCS scores did not change significantly from the preoperative visit to the latest follow-up (P = .608), nor did the mean difference in pre- to postoperative scores surpass the MCID. This finding is consistent with our previous work, which found no significant change in VR-12 MCS from the preoperative visit to 2-year follow-up. Additionally, a multicenter study by Mathew et al 27 found that the SF-36 mental quality of life score increased over time following TAA with the Salto Talaris, with an average 3.1-point increase in patients with >5-year follow-up, but this increase failed to meet clinical significance. Of the PROMs collected, the VR-12 MCS score is the only one designed to evaluate mental quality of life, whereas all the others are designed to evaluate physical components of life. Mental quality of life is a complex construct, and additional work is needed to further explore why this PROM does not change following TAA.
The results of this study also found that PROMs did not differ significantly with follow-up duration. Although the current study was not designed to demonstrate stability of PROMs over time, the data indicate that there was no significant difference detected in PROMs collected between the 24- and 193.9-month visits following surgery. With the numbers available, no significant difference in postoperative PROMs across the range of follow-up durations (24-193.9 months) could be detected. This finding is consistent with another follow-up study on patients with Salto Talaris fixed-Bearing TAA with an average follow-up of 10.7 years. 30 This study used the VAS, SF-36, Foot and Ankle Disability Index, and Short Musculoskeletal Function Assessment, and found no significant changes between 5- and 10-year outcome measures.
The results of this study also found a 93.3% metal component retention rate for patients receiving the Salto Talaris fixed-bearing TAA at an average 6.3-year follow-up. This finding is consistent with previous studies on the midterm results of the Salto Talaris fixed-bearing TAA, which found a 95.8% survivorship rate at 6.8 year follow-up and 84.2% at 10.7 years.26,30 This result is also comparable to long-term survivorship rates previously identified for other common TAA implants, such as the Bologna-Oxford TAA that had 66% survivorship at 10 years, the Scandinavian Total Ankle Replacement (Stryker) that had 76.6% survivorship at 15.8 years, and the HINTEGRA that had a 93.5% survivorship at 11.3 years follow-up.28,29,31 This high metal component retention rate indicates that fixed-bearing TAA with the Salto Talaris implant may offer long-term viability and functional restoration to patients hoping to maintain ankle mobility.
The study design presents many strengths, such as the large cohort size, long follow-up duration, and procedural consistency, given that all surgeries were performed by a single experienced surgeon who performs a high volume of TAA cases each year. Despite these strengths, the study is not without limitations. First, this study is a cohort retrospective study with no controls and is subject to all the common limitations of this study design. These include under-detection of minor or subclinical complications and inability to account for patients who were treated for complications or any additional ankle surgeries or TAA failures at an outside facility. Second, although a single-surgeon model improves internal validity, it may limit the generalizability of the presented results to locations with a low volume of TAA procedures or surgeons with limited numbers of cases. Also, this was intended to be a long-term follow-up study with a minimum follow-up of approximately 11 years; however, we were unable to achieve this as many patients stopped filling out the annual PROMs surveys before this time point. Thus, we could not evaluate the stability of PROMs over time. Future research is needed to better understand the stability of PROMs following TAA.
Conclusion
Evaluation of PROMs following TAA suggested improvement in quality of life, pain, disability, and function of the ankle at midterm follow-up after TAA with the Salto Talaris implant. Knowledge of these patient-reported outcomes can help physicians guide and educate patients considering TAA on the expected path to recovery.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007261454946 – Supplemental material for Patient-Reported Outcomes and Satisfaction Results on a Modern Fixed-Bearing Total Ankle Arthroplasty: Updated Mean 6-Year Follow-up
Supplemental material, sj-pdf-1-fai-10.1177_10711007261454946 for Patient-Reported Outcomes and Satisfaction Results on a Modern Fixed-Bearing Total Ankle Arthroplasty: Updated Mean 6-Year Follow-up by Daisy L. Lang, Blake R. McReavy, Ryan K. Moen, Rebecca Stone McGaver, Jacquelyn E. Fritz, Kayla J. Seiffert and J. Chris Coetzee in Foot & Ankle International
Footnotes
Ethical Considerations
Institutional review board (IRB) approval was obtained from University of Minnesota IRB (IRB 1206M15670).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J. Chris Coetzee, MD, reports general disclosures outside of this work: Responsive Arthroscopy LLC: stock; Arthrex, Inc: other professional activities; DePuy Synthes Products LLC: other professional activities; and Smith & Nephew, Inc: other professional activities. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.