
Abstract
Background:
Modified Lapidus procedure is well established for severe hallux valgus (HV). Nonetheless, postoperative recurrence remains a clinical concern. Peroneus longus (PL) functions as a dynamic stabilizer of the first ray, and its insertion at the base of the first metatarsal may be partially resected during osteotomy. Notably, PL dysfunction may contribute to recurrence by contributing to postoperative first ray instability. Nevertheless, extent of PL insertion resection during modified Lapidus procedure has not been quantified. This study aimed to evaluate the extent of resected PL insertion during modified Lapidus procedure.
Methods:
We retrospectively reviewed 80 feet from 74 patients with severe HV. We simulated 2 osteotomy methods: lateral wedge osteotomy at the base of the first metatarsal (M-method) and lateral wedge osteotomy at the distal medial cuneiform (C-method). On radiographs, resected lateral edge length of the first metatarsal (rM1-length) to correct intermetatarsal angle (IMA) to 0° was measured. Based on the rM1-length, 3-dimensional computed tomography models were used to measure whole PL insertion length, resected PL insertion length (rPL-length), and percentage of resected PL insertion (%-rPL). These parameters between the M-method and the C-method were compared. Cutoff value of the IMA for diagnosing feet with %-rPL greater than 50% using the M-method was evaluated.
Results:
rM1-length, rPL-length, and %-rPL were significantly greater with the M-method than with the C-method (all P < .001). Notably, the mean %-rPL with the M-method exceeded 50%. The IMA cutoff value was 21.4°; however, with the numbers available, no statistically significant difference was detected in the rPL-length and %-rPL with the C-method above and below this cutoff.
Conclusion:
Lateral wedge osteotomy at the first metatarsal may result in substantial PL insertion resection during the modified Lapidus procedure. Lateral wedge osteotomy of the medial cuneiform bone may better preserve PL insertion and potentially have implications for first ray stability.
Introduction
Hallux valgus (HV) is a common forefoot deformity affecting approximately 30% of adults and occurs more frequently in women and older individuals.1,2 It is associated with pain, gait disturbance, and reduced quality of life, particularly in severe cases.2-4 Although conservative treatments, including orthoses and physical therapy, may relieve symptoms, their ability to correct the HV angle (HVA) or underlying deformity is limited.5-7 As a surgical treatment for hallux valgus, the modified Lapidus procedure—arthrodesis of the first tarsometatarsal joint—is indicated for moderate to severe HV, particularly in the presence of first ray hypermobility, increased intermetatarsal angle (IMA), or recurrent deformity.8-10 Compared with distal metatarsal osteotomies, the modified Lapidus procedure provides greater correction of the IMA and HVA; however, recurrence still occurs in 3% to 9% of patients.11-13 Although factors such as metatarsal adductus and intercuneiform instability have been implicated, the risk factors for recurrence remain unclear.14-17 Several studies suggest that residual intercuneiform instability between the medial and intermediate cuneiforms may compromise correction, leading to postoperative widening of the IMA and recurrent HV.16,17 Therefore, maintaining postoperative IMA correction is considered important for preventing recurrence after the modified Lapidus procedure.
Recent studies have demonstrated that the peroneus longus (PL) acts as a dynamic stabilizer of the first ray by counteracting medial deviation of the first metatarsal.18-20 In HV, impaired PL function is associated with an increased IMA. 19 During the modified Lapidus procedure, osteotomy at the base of the first metatarsal—where the PL inserts—may partially resect the PL insertion. Anatomically, the PL inserts at the plantar-lateral aspect of the first metatarsal base, a region that directly overlaps with the resection zone in a lateral closing wedge osteotomy. Furthermore, although details of the osteotomy method varied among surgeons, 10 wedge osteotomy is often performed and may result in greater resection of the PL insertion.21,22 A cadaveric study demonstrated varus displacement of the first metatarsal following PL transection at its insertion, suggesting that PL insertion resection may contribute to intercuneiform instability and recurrent IMA after the modified Lapidus procedure. 20 Therefore, preservation of the PL insertion during wedge osteotomy may be important. However, the extent of PL insertion resection during the modified Lapidus procedure according to osteotomy level and correction angle remains unclear. We hypothesized that greater resection of the first metatarsal base for IMA correction would result in greater loss of the PL insertion. This study aimed to evaluate the extent of PL insertion resection during the modified Lapidus procedure using computed tomography (CT).
Methods
Patients
A retrospective review was conducted on 80 feet from 74 patients with HV who underwent surgical treatment between December 2013 and May 2025. This study included consecutive patients who met the inclusion criteria. Inclusion criteria comprised patients who underwent weightbearing plain radiography and routine foot CT scan before surgery and had an HVA greater than or equal to 40° on weightbearing plain radiography. Exclusion criteria involved patients with HVA less than 40° and those with systemic diseases such as rheumatoid arthritis, or a history of trauma or previous foot surgery (Figure 1). The cohort comprised 11 males and 69 females, with a mean age of 69.4 ± 12.9 (range, 20-90) years. This study was approved by the local ethics committee of our university and conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants included in this study.
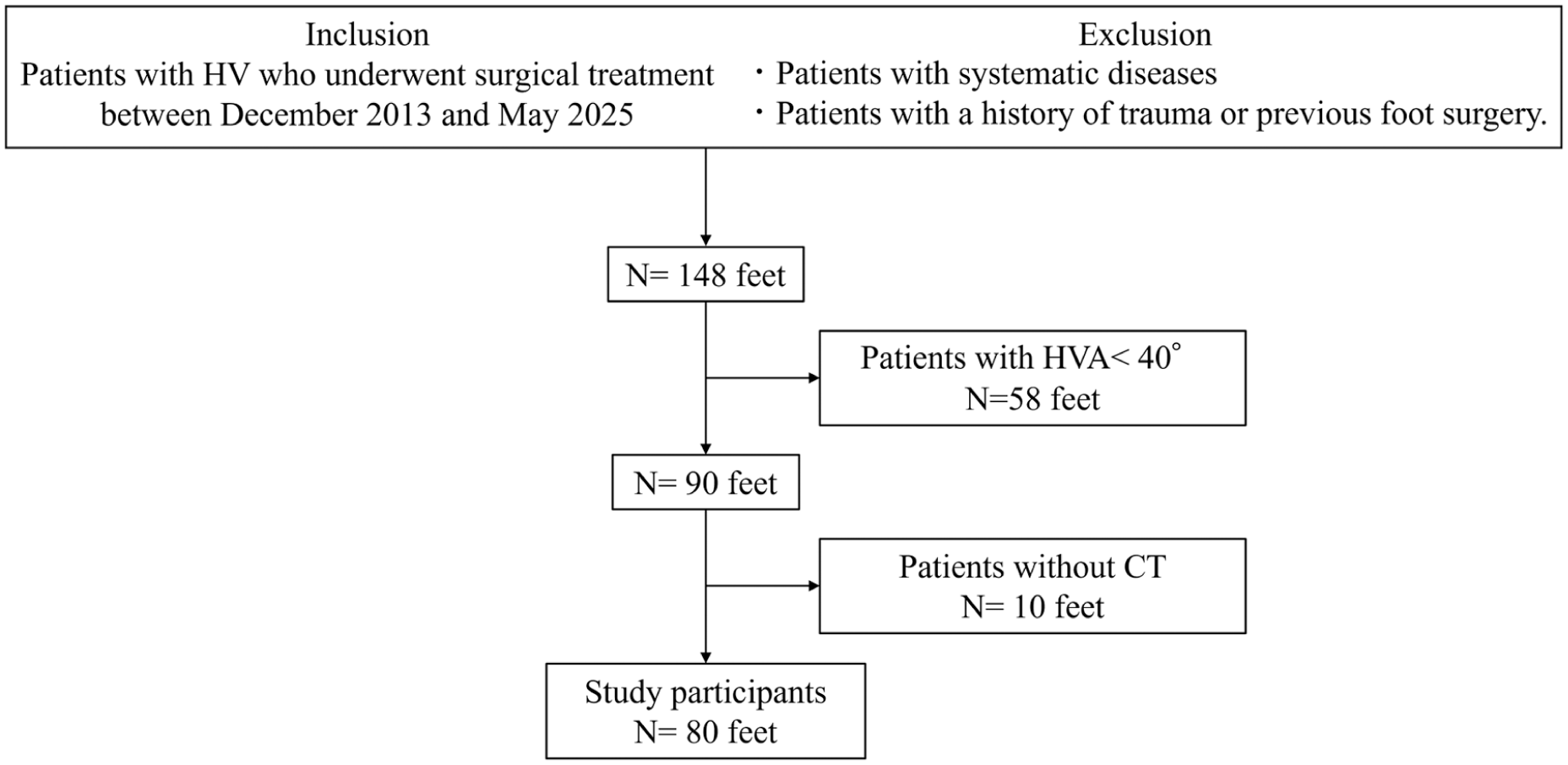
Participant flow chart. CT, computed tomography; HV, hallux valgus; HVA, hallux valgus angle.
Plain Radiograph Evaluation
Dorsoplantar radiographs of the foot in the standing position were performed and HVA and IMA between the first and second metatarsal bones were measured (Figure 2A). On radiographs, 2 osteotomy models were constructed: a lateral closing wedge osteotomy at the base of the first metatarsal (M-method) and at the distal medial cuneiform (C-method), with wedge resections defined according to the measured IMA. In this simulation, the IMA was corrected to 0° to create a standardized maximal correction condition, allowing direct comparison of osteotomy level on PL insertion resection rather than representing a clinical target. The osteotomy lines were geometrically defined according to the measured IMA and were not based on intraoperative techniques or surgeon-specific practices. The wedge size and orientation were determined by angular deformity rather than free-hand estimation or use of a cutting guide. In our clinical practice, bone resection is typically measured intraoperatively using a ruler to achieve the desired IMA correction; therefore, the geometrically defined osteotomy model represents a simplified measurement-based approach. Although the modified Lapidus procedure is clinically performed to address tarsometatarsal subluxation, the osteotomy in this study was modeled based on angular correction for standardized comparison. This simulation was based on 2-dimensional correction and did not account for 3-dimensional deformity, including rotational alignment of the first ray. In the M-method, a wedge osteotomy was performed at the base of the first metatarsal, and an osteotomy of the medial cuneiform bone was performed parallel to the distal articular surface (Figure 2B). In the C-methods, a wedge osteotomy was performed distal of the the medial cuneiform bone, and an osteotomy of the first metatarsal was conducted parallel to the proximal articular surface (Figure 2C). Subsequently, the length of the lateral edge of the first metatarsal resected along the expected osteotomy line (rM1-length) in both methods were measured.
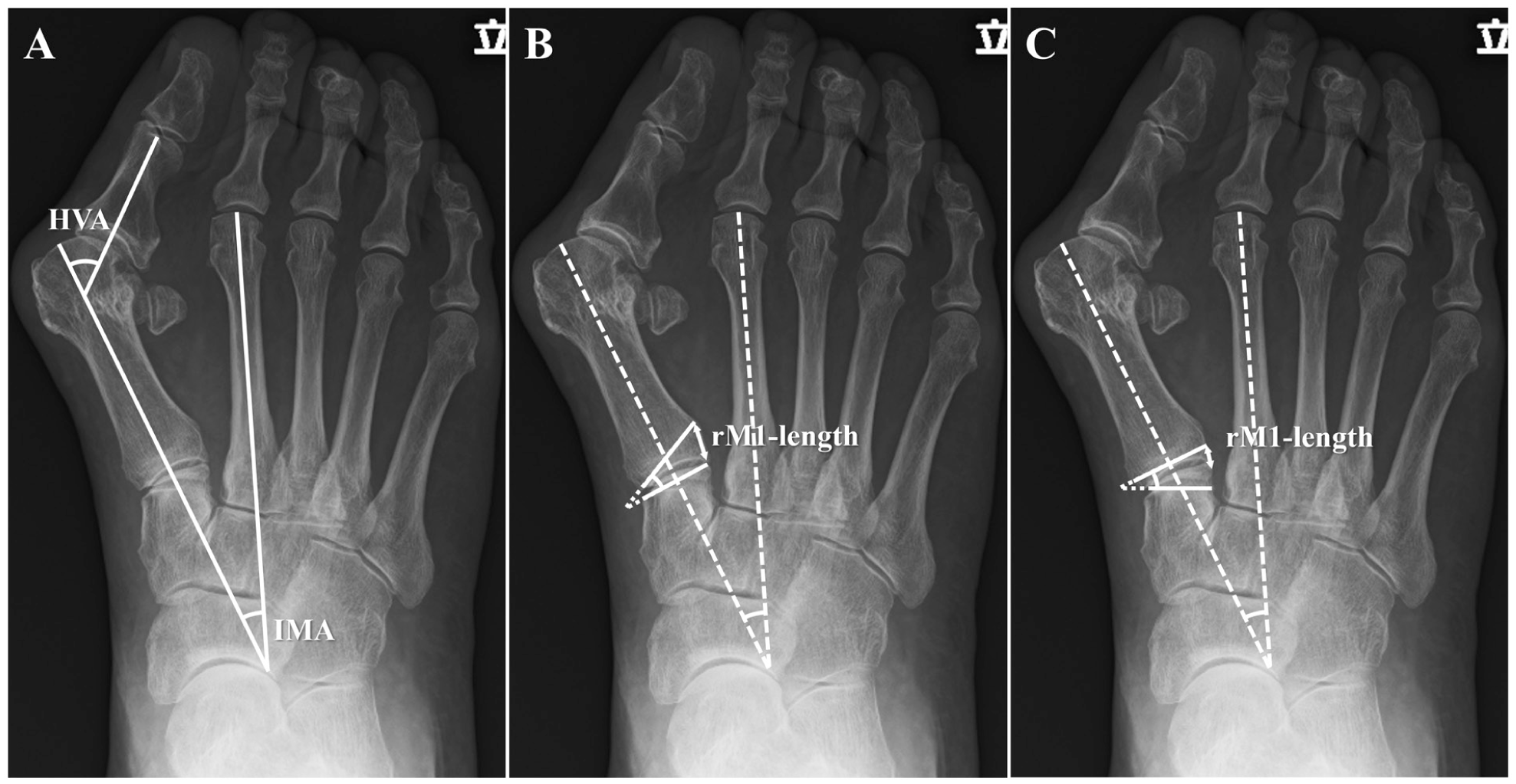
Two osteotomy methods and radiographic parameter measurements. (A) HVA and IMA. (B) Osteotomy using M-method. A wedge osteotomy is performed at the base of the first metatarsal to correct the IMA to 0° postoperatively. The length of the lateral edge of the first metatarsal resected along the osteotomy line is measured as rM1-length (double arrow). (C) The osteotomy line and rM1-length using the C-method. The wedge osteotomy is performed distal of the the medial cuneiform bone to correct IMA to 0° postoperatively. HVA, hallux valgus angle; IMA, intermetatarsal angle; rM1-length, resected length of lateral edge of first metatarsal.
CT Evaluation
CT images were obtained as part of routine preoperative evaluation to assess the detailed bone morphology. Coronal, sagittal, and axial images of the feet were acquired using a 64-multidetector-row CT scanner (Light-Speed QX/I; GE Healthcare). After scanning, 2-dimensional images were reconstructed with a 25-cm field of view, 1.25-mm retrospective slice thickness, and 0.63-mm overlap. Three-dimensional (3D) volume rendering of the first metatarsal was performed using image-rendering software (Synapse 3D, Fujifilm), and the resected amount of PL insertion was evaluated as follows (Figure 3). First, the PL insertion at tubercule on the first metatarsal was identified. 23 To address potential distortion in severe HV, the PL insertion was defined using consistent anatomical landmarks, including the plantar-lateral tubercle of the first metatarsal base, and confirmed on multiplanar CT reconstructions to ensure reproducibility. Although the PL insertion may extend beyond the tubercle, this landmark was used as a reproducible reference across cases. The resected length measured on plain radiographs (rM1-length) was then transferred to the 3-dimensional CT model using corresponding landmarks on the lateral aspect of the first metatarsal, including the lateral cortex of the first metatarsal base. The expected osteotomy lines for both methods were subsequently drawn on the CT model parallel to the adjacent joint surface (Figure 3A and B). Finally, the whole PL insertion length (wPL-length) and resected PL insertion length (rPL-length) perpendicular to the osteotomy line were measured and the percentage of rPL length relative to wPL length (%-rPL) was calculated using the following formula; %-rPL = rPL-length / wPL-length (Figure 3C).
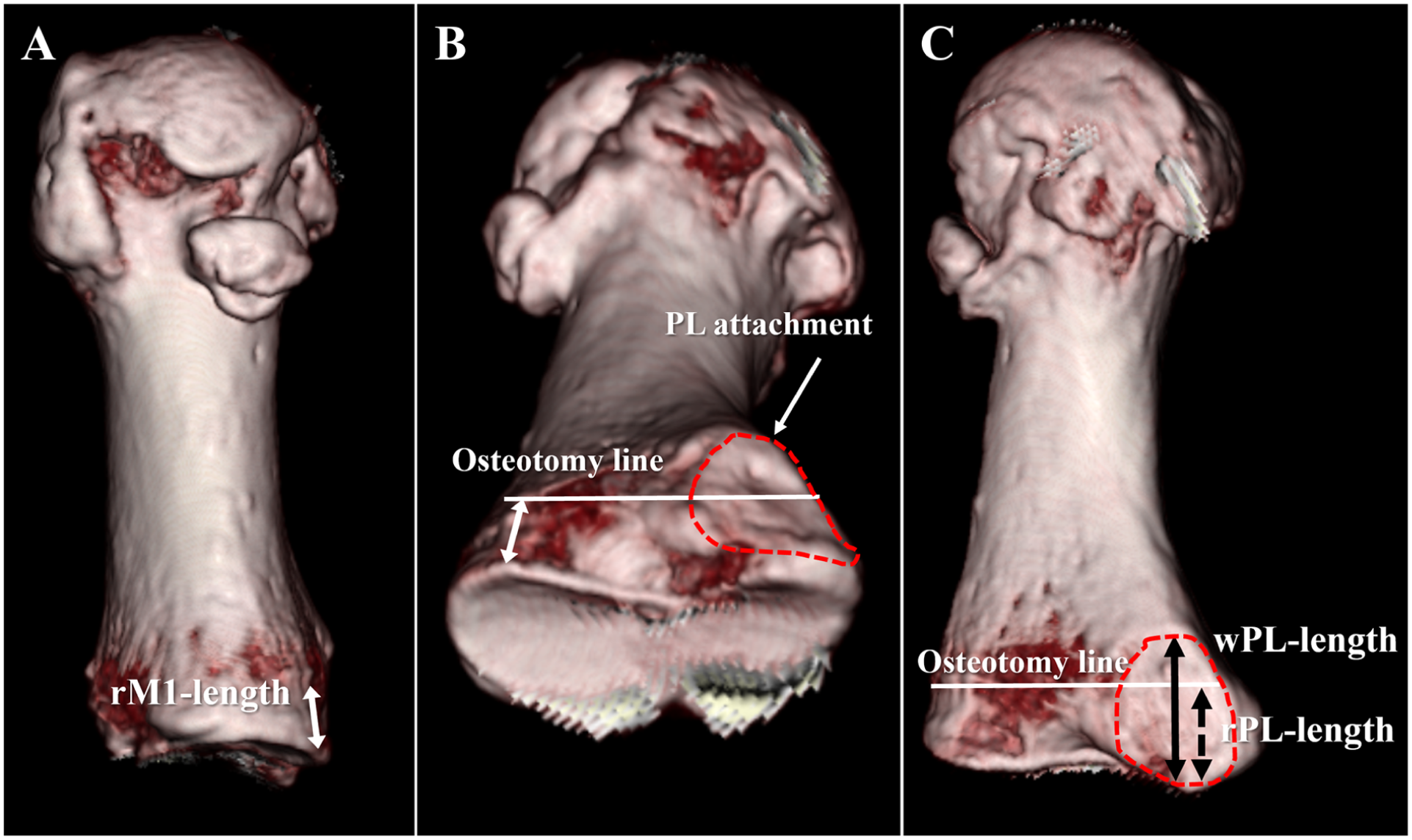
Measurements of the resected portion of the PL insertion. (A) The rM1-length measured on a plain radiograph was applied to the 3D-CT model of the first metatarsal. Double arrow: rM1-length. (B) On the 3D-CT model, an osteotomy line on the lateral aspect of the first metatarsal, parallel to the joint surface, was drawn. Double arrow: rM1-length; white line: osteotomy line; dashed-line area: PL attachment. (C) The whole length and resected length of the PL insertion, measured perpendicular to the osteotomy line, were defined as wPL-length and rPL-length, respectively. Double arrow: wPL-length; dashed double arrow: rPL-length; white line: osteotomy line; dashed-line area: PL attachment. 3D-CT, 3-dimensional computed tomography; PL, peroneus longus; rM1-length, the length of resected lateral aspect of the first metatarsal; rPL-length, the length of resected peroneal longus.
Statistical Analysis
There were no missing data, and all cases were included in the final analysis. Differences in rM1-length, rPL-length, and %-rPL between the M-method and the C-method were compared using the Wilcoxon signed-rank test. Correlations between IMA and parameters including HVA, rM1-length, rPL-length, and %-rPL were assessed using Spearman correlation coefficient. Receiver operating characteristic curve analysis was performed to determine the IMA cutoff for diagnosing %-rPL >50% with the M-method. Patients were then divided according to the cutoff value, and group differences were analyzed using the Kruskal-Wallis test. Intra- and interobserver reliability were evaluated using the intraclass correlation coefficient (ICC), with values interpreted as poor (<0.40), fair to good (0.40-0.75), or excellent (>0.75) agreement. Statistical significance was set at P < .05. Analyses were performed using EZR (Saitama Medical Center, Jichi Medical University), a graphical user interface for R (R Foundation for Statistical Computing). Given the retrospective observational design, all analyses were considered exploratory, and no multiplicity adjustments were applied.
Results
The interobserver ICCs for rM1-length (0.99; 95% CI, 0.98-0.99), rPL-length (0.98; 95% CI, 0.96-0.99), and %PL (0.96; 95% CI, 0.94-0.98) were excellent. The intraobserver ICCs for rM1-length (0.95; 95% CI, 0.92-0.97), rPL-length (0.95; 95% CI, 0.92-0.97), and %-rPL (0.95; 95% CI, 0.92-0.97) were excellent.
The mean HVA and IMA were 48.2° ± 8.3° (range, 40.2°-83.8°) and 19.9° ± 3.9° (range, 12.5°-39.9°), respectively (Table 1). There was a significant correlation between HVA and IMA (r = 0.327, P < .01). The mean rM1-length was 6.1 ± 1.4 mm (range, 4.1-13.1 mm) with M-method and 2.2 ± 0.6 mm (range, 1.1-3.8 mm) with C-method (Table 2). The rM1-length with the M-method was significantly greater than that with the C-method (P < .001) (Figure 4). The rM1-lengths measured by both methods were significantly correlated with IMA (M-method: r = 0.467, P < .001; C-method: r = 0.246, P < .05) (Table 2). Regarding the PL insertion evaluation on the 3D model, the mean wPL-length was 10.3 ± 1.3 mm (range, 7.4-14.2). The mean rPL-length was 5.8 ± 1.5 mm (range, 2.6-10.8 mm) with the M-method and 1.6 ± 0.9 mm (range, 0-3.6 mm) with the C-method. The mean %-rPL was 56.4% ± 12.7% (range, 26.8%-87.4%) with the M-method and 15.3% ± 9.0% (range, 0%-34.7%) with the C-method (Table 2). The rPL-length and %-rPL with the M-method were significantly greater than those with the C-method (P < .001) (Figure 5). The rPL-length and %-rPL with the M-method were significantly correlated with IMA (rPL-length: r = 0.288, P < .01, %-rPL: r = 0.340, P < .01), whereas those with the C-method were not significantly correlated with IMA (Table 2).
Patients Demographics. a
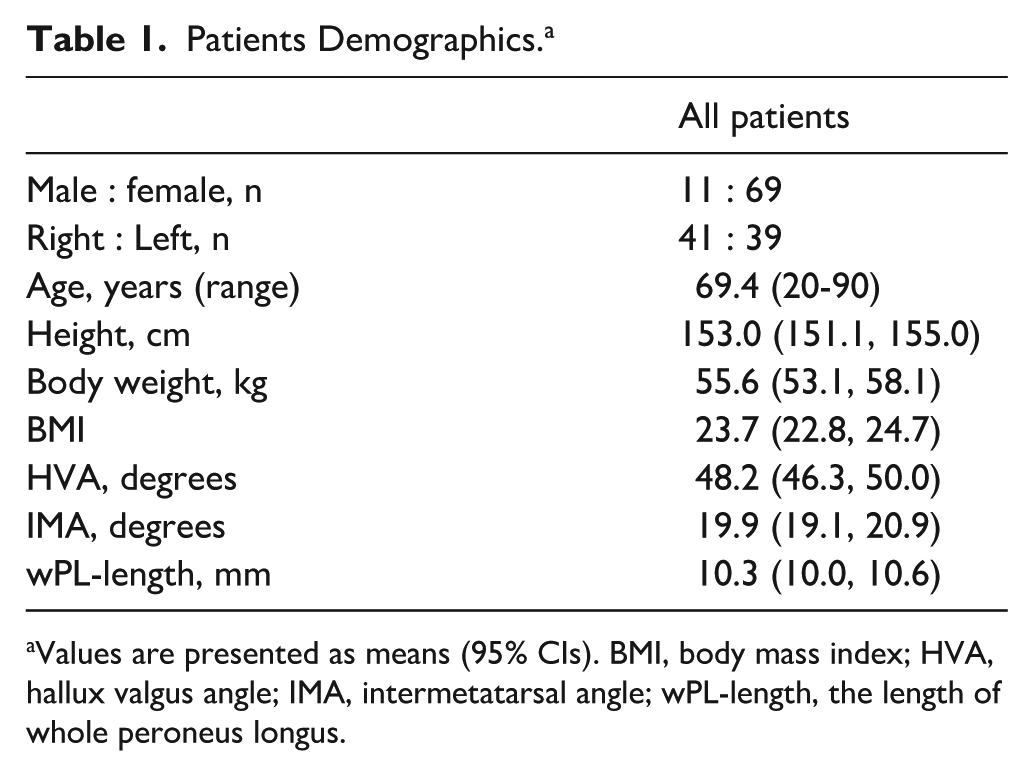
Values are presented as means (95% CIs). BMI, body mass index; HVA, hallux valgus angle; IMA, intermetatarsal angle; wPL-length, the length of whole peroneus longus.
The Resected Amount Parameters of 2 Osteotomy Methods. a
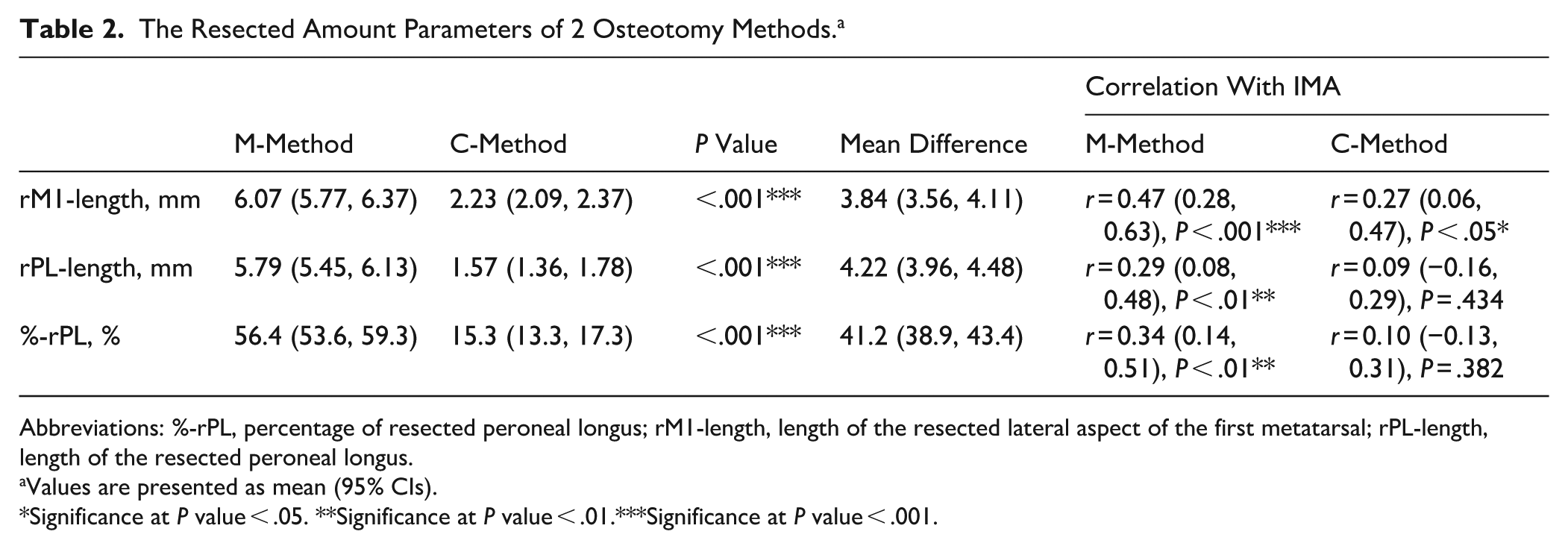
Abbreviations: %-rPL, percentage of resected peroneal longus; rM1-length, length of the resected lateral aspect of the first metatarsal; rPL-length, length of the resected peroneal longus.
Values are presented as mean (95% CIs).
Significance at P value < .05. **Significance at P value < .01.***Significance at P value < .001.
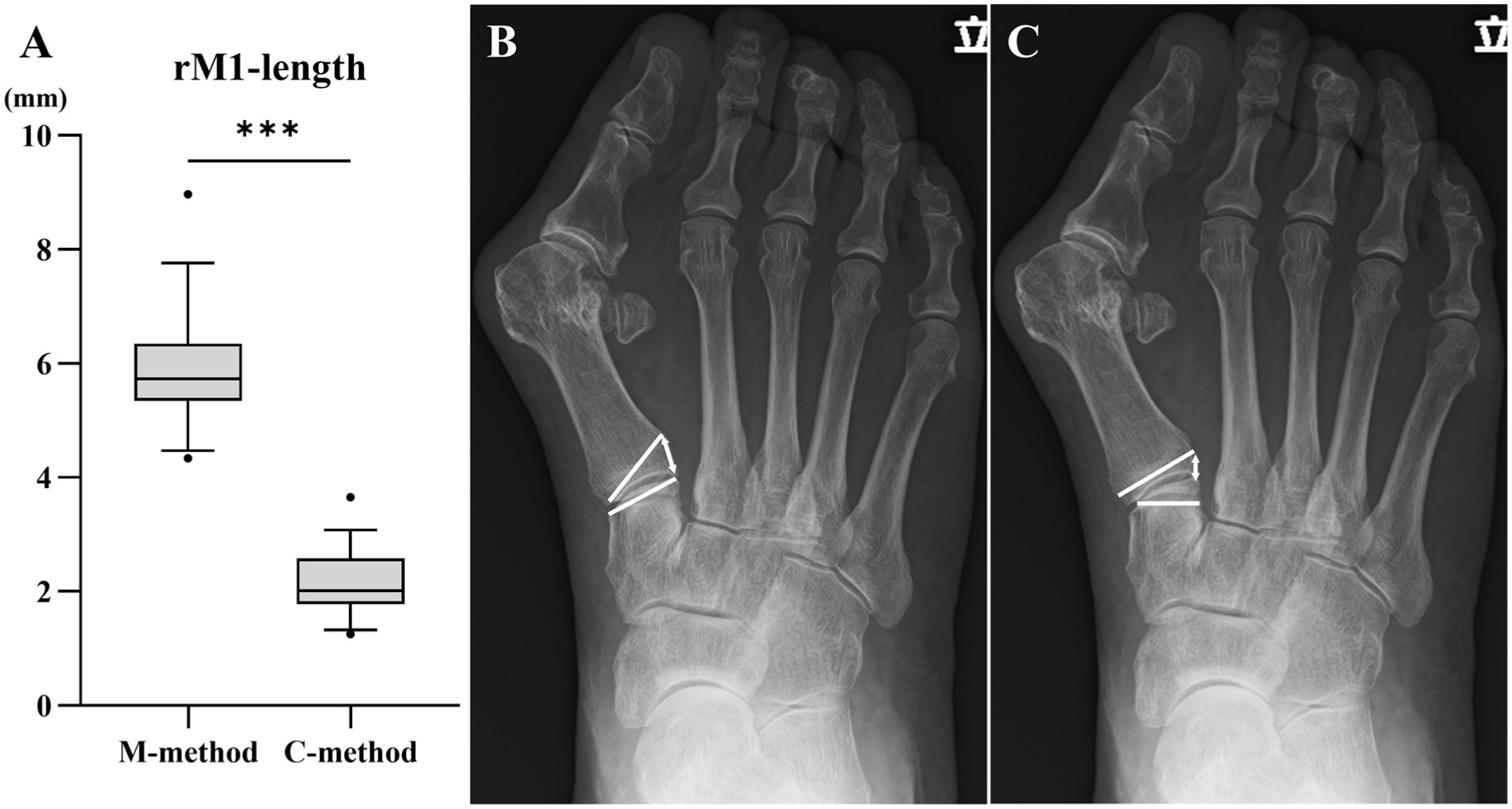
rM1-length measured using the M-method and C-method. (A) Box-and-whisker plots. (B) Representative radiographic image of the M-method. Yellow line: osteotomy line; double arrow: rM1-length. (C) Representative radiographic image of the C-method. Yellow line: osteotomy line; double arrow: rM1-length. rM1-length, resected length of the lateral edge of the first metatarsal. ***Significance at P value < .001.
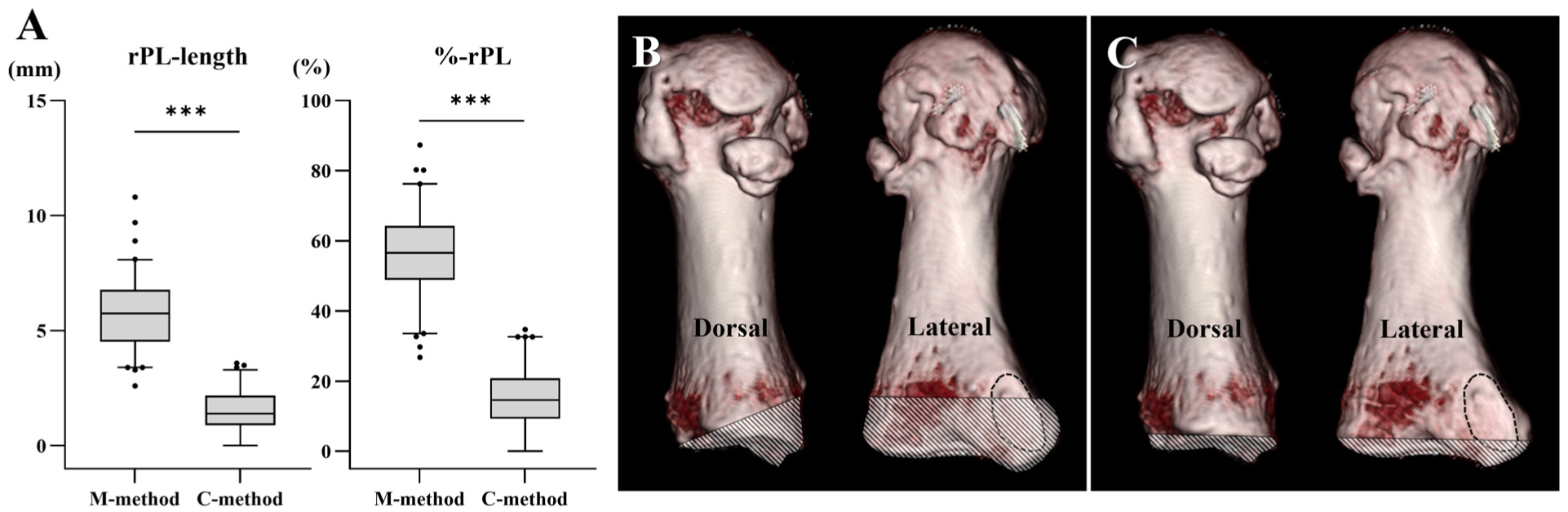
rPL-length and %-rPL of the M-method and C-method. (A) Box-and-whisker plots. (B) Representative 3D-CT image of the lateral aspect of the first metatarsal using the M-method. Dashed-line area: PL attachment; striped area: resected lesion with osteotomy. (C) Representative 3D-CT image of the lateral aspect of the first metatarsal using the C-method. Dashed-line area: PL attachment; striped area: resected lesion with osteotomy. 3D-CT, 3-dimensional computed tomography; PL, peroneus longus; %-rPL, percentage of resected peroneal longus; rM1-length, length of the resected lateral aspect of the first metatarsal; rPL-length, length of the resected peroneal longus.
Among all patients, 58 feet (72.5%) had %-rPL greater than 50% with the M-method. The cutoff point of the IMA for %-PL greater than 50% with the M-method was 21.4°, with 39.7% sensitivity and 90.9% specificity (Figure 6). With the numbers available, no statistically significant difference was detected in the rPL-length and %-rPL with the C-method between <21.4° and >21.4° in IMA (Table 3).
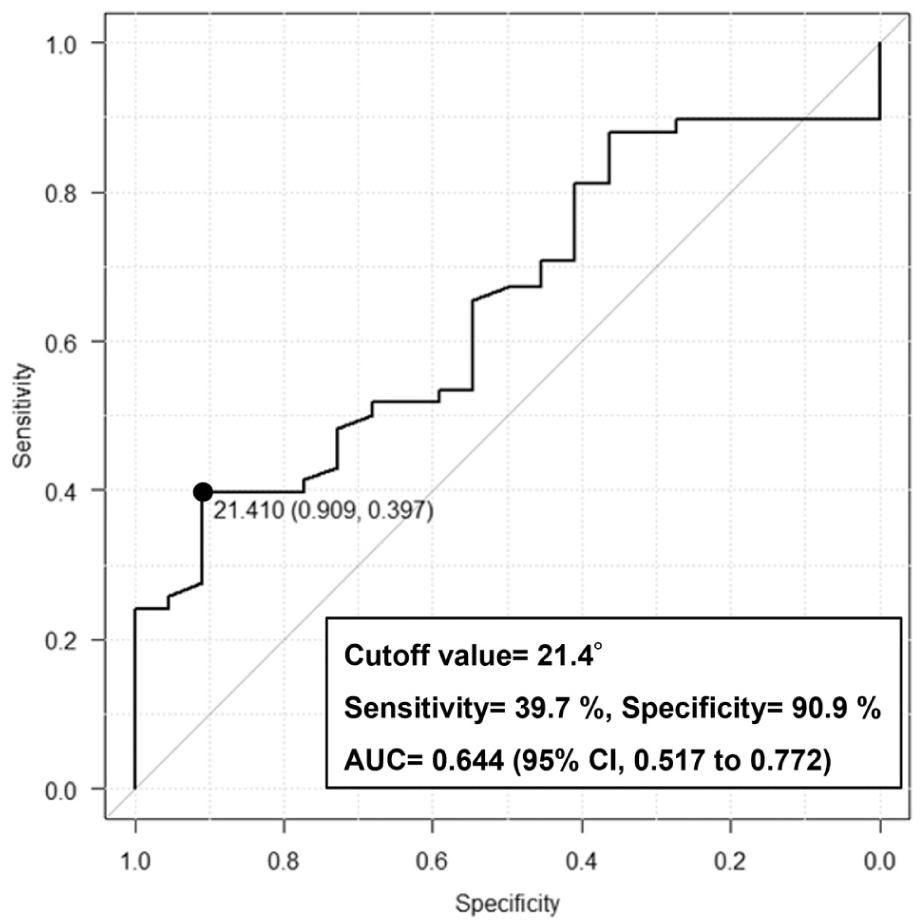
Receiver operating characteristic analyses of IMA to determine the optimal cutoff value for those who have %-rPL greater than 50% with the M-method in participants. AUC, area under the curve; IMA, intermetatarsal angle; %-rPL, percentage of resected peroneal longus.
Resected Amount Parameters Divided by the IMA Cutoff Value. a
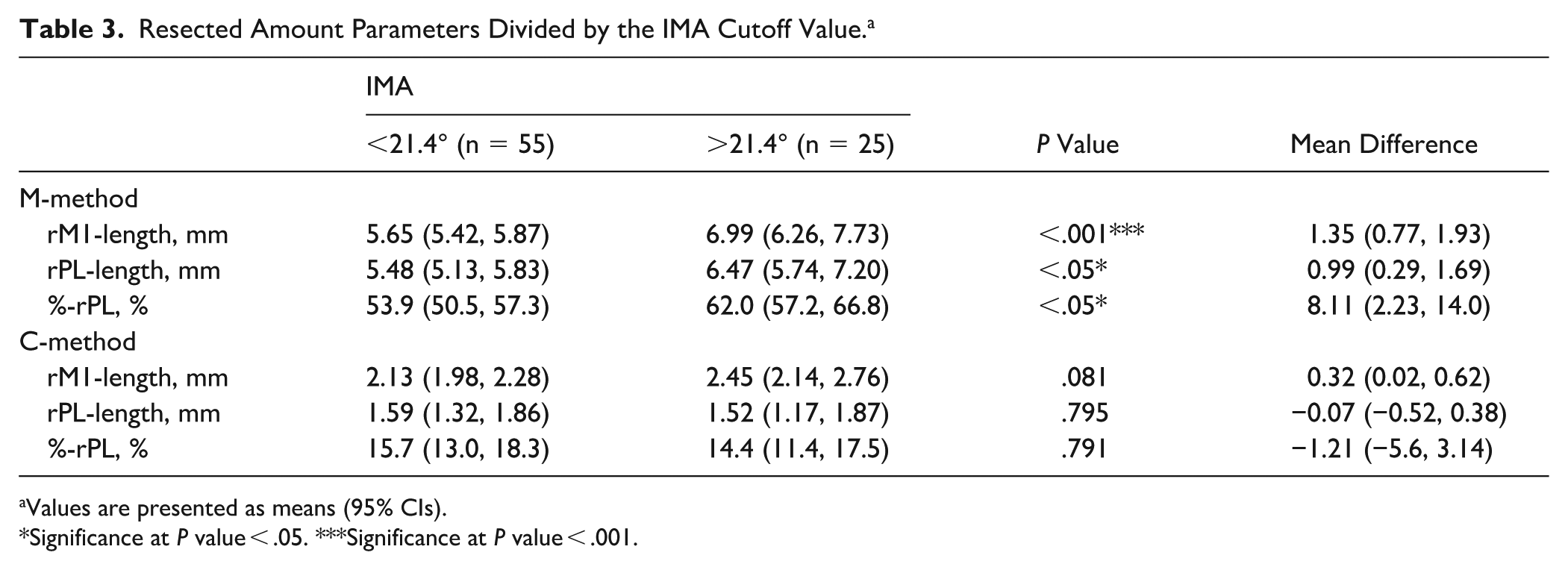
Values are presented as means (95% CIs).
Significance at P value < .05. ***Significance at P value < .001.
Discussion
This study demonstrated that when a wedge osteotomy was performed at the base of the first metatarsal, the mean resection of the PL insertion exceeded 50%. Conversely, a wedge osteotomy distal of the medial cuneiform resulted in significantly less resection of the PL insertion compared with an osteotomy at the metatarsal base. Therefore, during closed wedge osteotomy in the modified Lapidus procedure, performing a wedge osteotomy at the medial cuneiform may be preferable for preserving PL insertion, may have implications for first-ray stability, and may help reduce the need for excessive resection at the metatarsal level.
Although the widely performed modified Lapidus procedure involves arthrodesis of the first tarsometatarsal joint, the detailed surgical technique for the modified Lapidus procedure varies among surgeons. 10 Although several comparative studies have investigated fixation methods,24-26 little attention has been paid to osteotomy techniques, and there is no consensus on the optimal osteotomy method. Specifically. some reports have described only removal of the articular cartilage without wedge osteotomy21,22; nonetheless, insufficient bone resection is reported to result in inadequate postoperative correction of the intermetatarsal angle. 27 Although some surgeons perform lateral wedge osteotomy to correct the IMA, others do not routinely perform wedge resection, particularly in minimally invasive techniques. Therefore, there is no consensus regarding the necessity of wedge resection or the optimal osteotomy method.21,22,28 Here, we evaluated the amount of PL insertion resected during lateral wedge osteotomy aimed at achieving postoperative correction of the IMA to 0° using these 2 osteotomy techniques. As a result, resection of the lateral aspect of the first metatarsal was greater in the metatarsal-level osteotomy than in the distal cuneiform osteotomy and showed a significant positive correlation with IMA. This difference is attributable to the anatomical location of the osteotomy. In the C-method, the wedge is created at the medial cuneiform, allowing correction of the IMA without directly resecting the lateral cortex of the first metatarsal. Therefore, even with similar angular correction, resection affecting the PL insertion is reduced compared with the M-method. However, this finding may also reflect the assumptions of the radiograph-based simulation, as the amount of bone resection in clinical practice does not necessarily increase with deformity severity and may be similar between osteotomy level. Accordingly, for the correction of a large IMA in severe HV, wedge osteotomy at medial cuneiform may be preferable for preserving PL insertion, as the base of the first metatarsal is minimally resected parallel to the articular surface (Figure 5C). Although anatomical variation of PL insertion has been reported, all cadaveric studies have demonstrated insertion at the base of the first metatarsal. In the present study, the PL insertion tubercle was consistently identified on 3D-CT, with a mean length of 10.3 mm, suggesting that substantial metatarsal resection may markedly reduce the tubercle. PL resection correlated significantly with IMA only in metatarsal-level osteotomy, indicating progressive loss of PL insertion with increasing deformity severity. Additionally, an IMA cutoff of 21.4° predicted resection of more than 50% of the PL insertion with this method. As cadaveric studies have shown that resection exceeding 50% of the peroneal tendons substantially reduces stiffness,29,30 these findings suggest that metatarsal-level lateral wedge osteotomy may compromise PL function in patients with large IMAs. Moreover, the cutoff value showed low sensitivity (39.7%) but high specificity (90.9%). This suggests that an IMA >21.4° is useful for identifying patients at high risk of more than 50% PL insertion resection; however, such risk cannot be excluded when the IMA is <21.4°. The low sensitivity also indicates that IMA alone may be insufficient to reliably predict substantial PL insertion resection. Therefore, when preservation of the PL insertion is prioritized, cuneiform-level osteotomy may be considered as an alternative to metatarsal-level osteotomy, particularly in severe deformities. However, previous studies have shown that first tarsometatarsal procedures may still affect the PL tendon, indicating that complete preservation is not always achieved even with cuneiform-level osteotomy. 21
Our findings regarding PL insertion preservation may have clinical implications for recurrent HV after the modified Lapidus procedure. Kim et al 16 reported greater postoperative widening between the medial and intermediate cuneiforms in recurrent cases, despite comparable preoperative findings. They suggested that loss of motion at the first tarsometatarsal joint may increase compensatory motion at the intercuneiform joint, leading to joint widening. Additionally, fixation between the medial and intermediate cuneiforms has been reported to reduce postoperative first metatarsal displacement.31,32 Based on this, although direct evidence is limited, our findings suggest that lateral wedge osteotomy of the first metatarsal substantially affects the PL insertion and may be associated with recurrence after modified Lapidus procedure. Because PL is considered one of the dynamic stabilizers of the first metatarsal, substantial resection of PL insertion may contribute to displacement of the fused first metatarsal and medial cuneiform with intercuneiform widening after modified Lapidus procedure (Figure 7). However, the threshold at which PL insertion resection causes functional impairment remains unclear. Although cadaveric studies suggest that complete resection may affect first ray mechanics, 18 the impact of partial resection has not been established, making it difficult to define a safe amount of PL insertion to preserve. In addition, postoperative recurrence is likely multifactorial, with factors such as bony union, adequacy of correction, intercuneiform stability, distal soft tissue balance, and sesamoid reduction also influencing outcomes; therefore, the contribution of PL insertion resection to recurrence remains unclear.

Representative images of recurrence after modified Lapidus procedure with M-method: (A) preoperative; (B) immediately after operation; (C) 1 year postoperatively. The first metatarsal shifts medially with intercuneiform joint widening.
To our knowledge, this is the first study to quantitatively evaluate PL insertion resection associated with different lateral wedge osteotomy techniques in the modified Lapidus procedure. Although the anatomical location of the PL insertion is well established, its relationship with deformity severity and osteotomy level has not been clarified. By demonstrating a deformity-dependent increase in PL insertion resection and identifying a clinically relevant IMA cutoff value of 21.4°, this study provides a potential biomechanical explanation for postoperative instability and recurrence. Our findings provide an anatomical rationale for surgical strategy; however, their direct clinical implications remain speculative and require prospective validation. Future prospective clinical studies correlating PL insertion preservation with recurrence rates, intercuneiform widening, and patient-reported outcomes will be necessary.
This study has several limitations. First, PL insertion resection was evaluated only in lateral wedge osteotomy, although alternative techniques involving cartilage resection and first metatarsal shortening have been reported.4,21,33 Second, osteotomy was designed to correct the IMA to 0° in a 2-dimensional manner, despite hallux valgus requiring 3-dimensional correction, including rotation.34,35 Because rotational alignment was not assessed because of the lack of weightbearing CT, the amount and distribution of bony resection may have been overestimated. In addition, estimation based on preoperative radiographs may introduce bias, as hallux valgus deformity involves both angular malalignment and tarsometatarsal subluxation, and bone resection does not necessarily increase proportionally with deformity severity in clinical practice. Third, wedge osteotomy may clinically involve both the first metatarsal and medial cuneiform, and blade thickness of the bone saw was not considered. 22 Furthermore, the tubercle may not represent the full extent of the PL insertion, potentially underestimating the resected area. However, the primary aim of this study was comparative evaluation between osteotomy methods rather than determination of the exact amount resected. Fourth, the clinical impact of PL insertion resection on recurrence after the modified Lapidus procedure remains unclear. Although complete PL resection has been shown to cause medial displacement of the first metatarsal in cadaveric studies, 18 the effect of partial resection (>50%) on postoperative alignment is unknown, and the role of the PL in first ray stability remains uncertain. It should also be noted that clinical experience with peroneus longus tendon transfer for peroneus brevis insufficiency suggests that loss of PL function does not consistently produce instability at the first tarsometatarsal or intercuneiform joints, raising the possibility that the PL may not be an essential stabilizer of the first ray. Accordingly, the clinical significance of PL insertion resection during the modified Lapidus procedure remains speculative, and preservation of the insertion should be viewed as an anatomical consideration rather than an established determinant of postoperative stability. Fifth, the study was not powered to detect a specific difference between cases above and below the cutoff value. Finally, anatomical variation of the PL insertion should be considered. Edama et al 36 reported medial cuneiform attachment in 20.2% of specimens, indicating that cuneiform-level osteotomy may not always completely preserve the PL insertion. However, substantial PL fibers consistently insert into the first metatarsal, and their effect on joint stability appears limited.36,37 Therefore, minimizing resection at the first metatarsal insertion remains clinically relevant, although further studies are needed to clarify its effect on clinical outcomes.
Conclusion
In patients with severe HV and a large IMA, a metatarsal-level lateral wedge osteotomy may require substantial PL insertion resection. Cuneiform-level osteotomy may better preserve PL insertion, which may have implications for first ray stability.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007261457068 – Supplemental material for The Amount of Peroneus Longus Insertion Resection With Modified Lapidus Procedure for Severe Hallux Valgus: Comparative Radiographic Study of 2 Different Osteotomy Methods
Supplemental material, sj-pdf-1-fai-10.1177_10711007261457068 for The Amount of Peroneus Longus Insertion Resection With Modified Lapidus Procedure for Severe Hallux Valgus: Comparative Radiographic Study of 2 Different Osteotomy Methods by Satoru Sakurai, Tomoyuki Nakasa, Yasunari Ikuta, Saori Ishibashi, Dan Moriwaki, Taro Chujo and Nobuo Adachi in Foot & Ankle International
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from the ethics committee of Hiroshima University (Approval number: E-14).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.