
Abstract
Background:
Limited dorsiflexion (DF) after total ankle arthroplasty (TAA) is a challenge that has been associated with worse functional outcomes and lower patient-reported satisfaction. The purpose of this study was to identify predictive variables for limited DF following TAA.
Methods:
A retrospective cohort study was conducted on patients who underwent elective primary TAA between 2013 and 2023 by a single surgeon. Postoperative range of motion (ROM) was assessed using weight-bearing lateral radiographs obtained in maximal DF and plantarflexion (PF). Limited DF was defined as <20° and preoperative DF was based solely on clinical assessment (C-DF). Demographic variables, medical comorbidities, surgical history, and adjunctive procedures, including gastrocnemius recession and tendo-Achilles lengthening (TAL), were collected and compared between patients who achieved full vs limited postoperative DF. Additionally, Foot and Ankle Ability Measure activities of daily living subscale (FAAM-ADL) and visual analog scale (VAS) scores were collected. Multivariable logistic regression was performed to identify independent predictors of final DF.
Results:
A total of 175 patients were included in this study, with 111 (63.4%) demonstrating limited postoperative DF and 64 (36.6%) achieving full DF at a mean 3.3 years. Age was significantly greater in the full DF group (65.5 vs 61.5 years, P = .013). No significant associations were identified between body mass index / weight, tobacco use, diabetes, sex, medical comorbidities, polyethylene size, or adjuvant procedures and postoperative DF following TAA. Prior open reduction internal fixation was more prevalent in patients with limited DF (P < .05), whereas postoperative FAAM-ADL scores were more favorable in the full DF group (70.0 vs 86.9, P = .010). Multivariable regression analyses identified full C-DF as the only significant independent predictor of improved postoperative DF following TAA.
Conclusion:
Preoperative clinical dorsiflexion was the only significant independent predictor of postoperative dorsiflexion following TAA. A thorough preoperative discussion regarding anticipated postoperative motion can help establish appropriate expectations and potentially enhance patient satisfaction following TAA.
Introduction
End-stage ankle osteoarthritis is a debilitating condition that leads to significant impairments and marked reduction in quality of life for affected patients. 1 Total ankle arthroplasty (TAA) has become an increasingly popular treatment option, offering effective pain relief, improved functional outcomes, and the added benefit of preserving joint motion compared with ankle arthrodesis.2,3 Advances in surgical techniques and implant designs over the past 20 years have significantly improved outcomes and survivorship of TAA, with recent reports of 94% to 100% survivorship at mid-term follow-up.4-6
In TAA, increased ankle range of motion (ROM) and enhanced peak plantarflexion (PF) power contributes to more normal gait mechanics during walking and stair ascent when compared to ankle fusions. 7 Postoperative improvements in ankle ROM are also linked to reduced pain and better overall function. 8 In particular, limited dorsiflexion (DF) has been associated with altered gait kinematics which can have upstream effects on the hip, knee, and pelvis during walking.9,10 Furthermore, studies have proposed threshold values for adequate DF. 11 Attainment of these benchmarks, whether through adjunctive procedures such as tendo-Achilles lengthening (TAL) or gastrocnemius recession, or through structured rehabilitation, is an important marker of success following TAA.
Despite this, postoperative stiffness after TAA is a challenge, leading to worse functional outcomes and lower patient-reported satisfaction.8,12 The underlying etiology for stiffness after TAA remains poorly understood. Although previous studies have identified preoperative stiffness as a potential risk factor for decreased postoperative ROM,13,14 there is a lack of robust data on patient- or surgery-specific predictors of final ankle motion after TAA. Therefore, the purpose of this study was to identify predictors of postoperative DF following TAA. Secondary outcomes included evaluating correlations between DF and patient-reported outcome measures, PF, and global ankle ROM.
Methods
A retrospective cohort study of prospectively collected data was performed to identify predictive variables associated with postoperative stiffness following TAA. Following institutional review board (IRB) approval, a retrospective review was performed of all patients who underwent primary TAA between January 2013 and June 2023. All procedures were performed by a single surgeon, and a standardized postoperative rehabilitation protocol was used consistently throughout the study period. This routinely involved 2 weeks of nonweightbearing in a cast, followed by transition to a controlled ankle motion boot and then guided physical therapy.
A total of 281 cases were identified from our institutional database. Patients were included if they had a minimum 2-year follow-up. Exclusion criteria included revision TAA or reoperation on the index ankle prior to final follow-up (n = 26) and lack of radiographs greater than 1 year postsurgery (n = 80). The reoperations removed were categorized according to the COFAS-based guidelines prior to exclusion. These included operative treatment of superficial infection or incision problem (n = 1), operative treatment of deep infection requiring debridement (n = 2), deep infection requiring removal of all components (n = 4), revision of metal components because of implant failure (n = 13), debridement of gutter or heterotopic ossification with retention of components (n = 2), debridement ± grafting of osteolytic cyst(s) (n = 1), and subsequent operative treatment related to TAA but not involving TAA components (n = 3). After exclusions, 175 TAAs met inclusion criteria and comprised the final cohort (Figure 1). The mean follow-up duration was 4.9 years (range 2-12.2 years), with final radiographs and patient-reported outcome measures (PROMs) taken at a mean 3.3 years postoperatively.
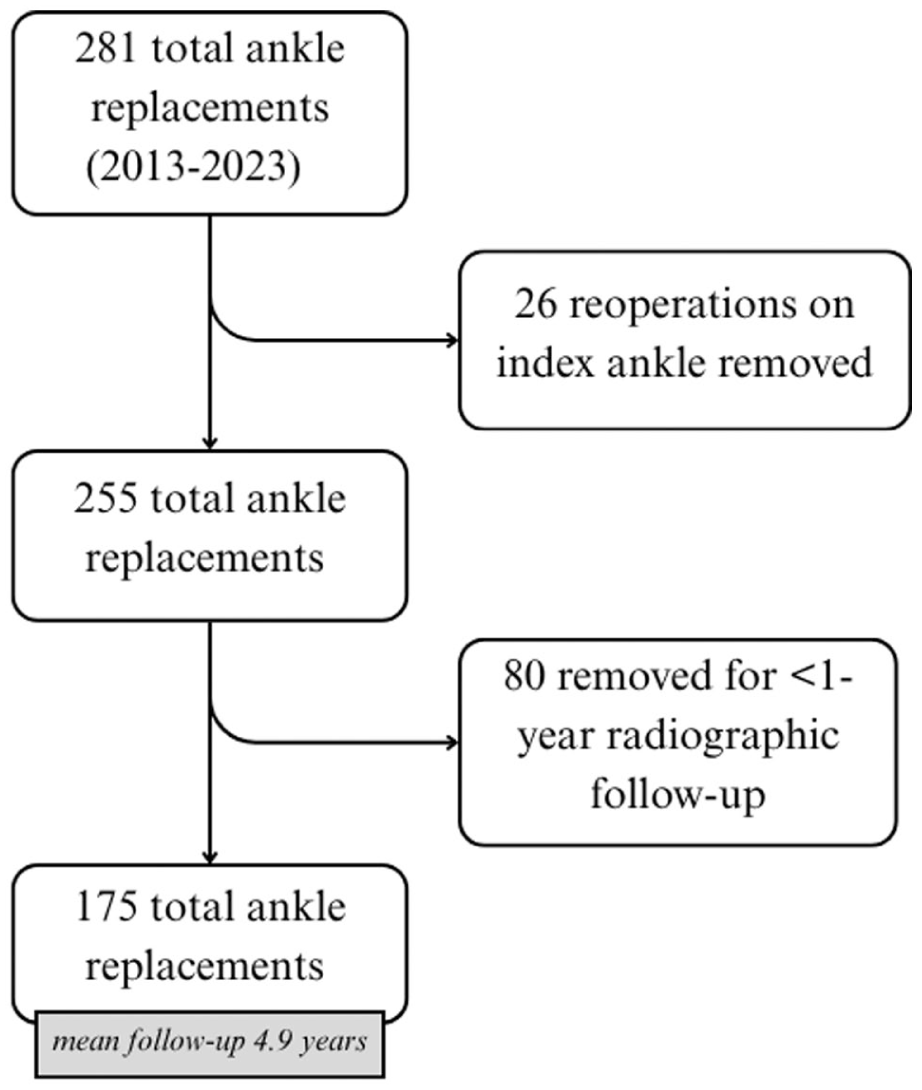
Cohort selection process of 175 total ankle replacements.
The primary outcome was to identify predictive variables associated with postoperative ankle DF at final radiographic follow-up. This was defined based on tibiopedal dorsiflexion measured from standardized radiographs using previously described methods. 15 The single surgeon included in this study obtains standard weightbearing dorsiflexion and plantarflexion radiographs at all postoperative TAA appointments. For radiographic assessment, DF was obtained by instructing the patient to step forward with the contralateral limb and flex the ipsilateral knee into maximal dorsiflexion. Both feet remained in full contact with the floor during imaging to simulate a stride length. The tibiopedal angles were determined by first defining the mechanical axis of the tibia through the centers of two circular fits along the tibial shaft. DF was then measured as the angle formed between the tibial axis and a line perpendicular to the floor on each respective radiograph. PF was measured in the same method, and total arc was calculated by summing DF + PF (Figure 2). In addition to the tibiopedal approach, radiographic ROM following TAA has also been quantified utilizing the tibiotalar measurement, which is taken between the long axis of the tibia and the talar axis.16,17 Although the tibiopedal angle may incorporate contributions from adjacent joints, this method likely better reflects functional weightbearing motion, which was the primary focus of this study.
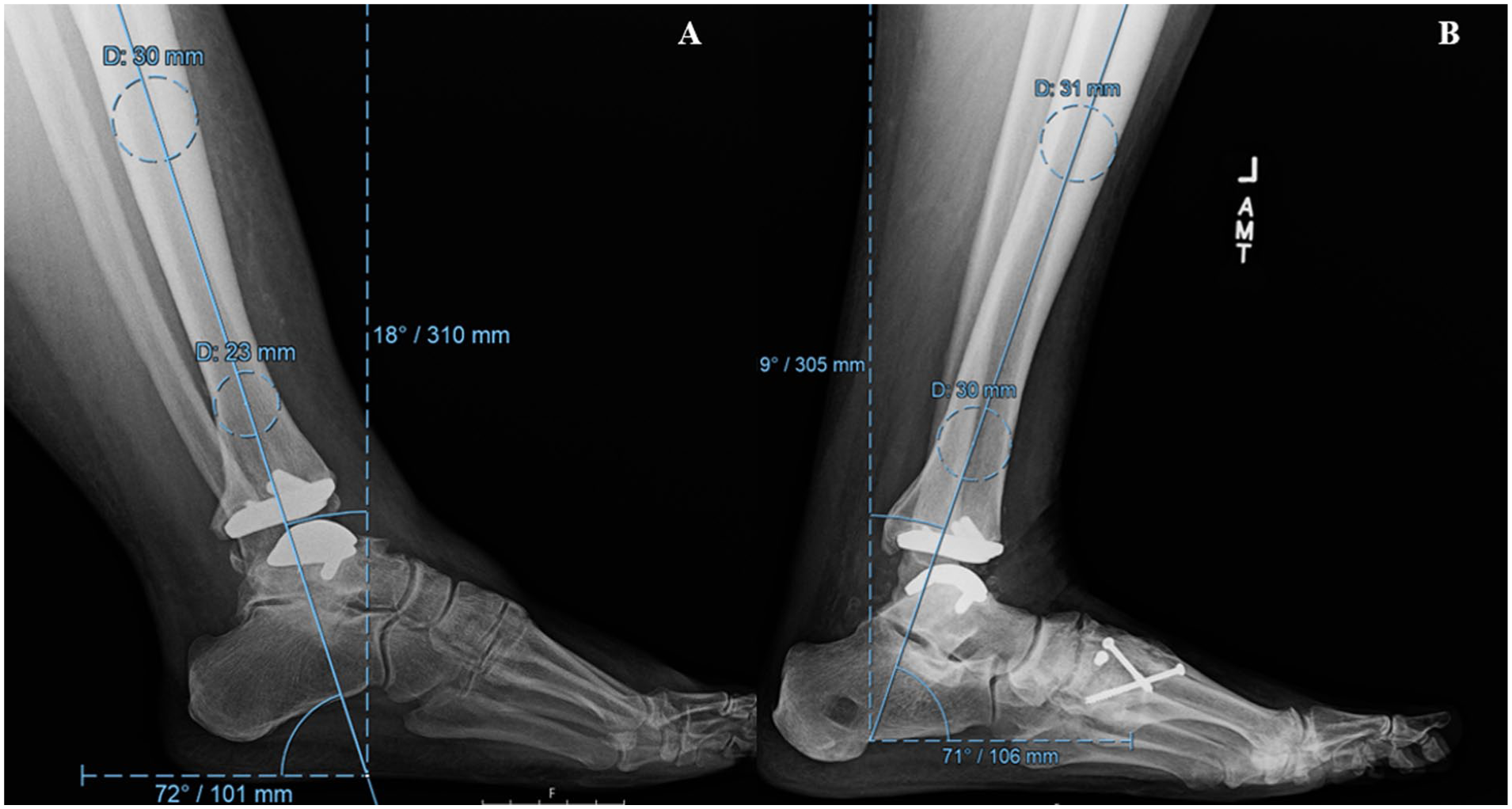
Maximal tibiopedal plantarflexion (A) and dorsiflexion (B) on lateral weightbearing radiographs.
Demographic data (age, sex, body mass index [BMI]) and comorbidities (eg, diabetes, tobacco and alcohol use, cardiovascular disease, rheumatoid arthritis, osteoporosis, gout) were extracted from the electronic medical record via SQL query. Preoperative and intraoperative variables were obtained through manual chart review. TAA implants included primarily the Cadence Total Ankle System (Smith+Nephew), the Scandinavian Total Ankle Replacement (STAR; Stryker), the Infinity Total Ankle System (Stryker), and the Salto Talaris Total Ankle Prosthesis (Smith+Nephew). We identified prior surgeries done outside of our institution through chart documentation or radiographic evidence. Because of inconsistencies in availability of preoperative flexed lateral radiographs, preoperative DF was determined from the operating surgeon’s clinical documentation (C-DF). C-DF was estimated at the time of clinical evaluation using the surgeon’s judgment and recorded in 5° increments. Reliable C-DF documentation was available for 139 of 175 patients. Full preoperative C-DF was defined as ≥20°, and limited as <20°. This threshold was defined based on several factors. First was the surgeon’s aforementioned routine clinical documentation of dorsiflexion in increments of 20°, which maintained consistency pre- and postoperatively. Additionally, this threshold created a binary descriptive comparison with adequate balance between groups (63.4% vs 36.6%). The authors acknowledge literature that suggests ~10° of DF is sufficient for normal ambulation, whereas values closer to 20 represent a more physiologic maximum but are not necessarily required for function. To mitigate any potential bias created by this threshold, a supplemental analysis of final DF as a continuous variable was performed.
PROMs, including the Foot and Ankle Ability Measure activities of daily living subscale (FAAM-ADL) and visual analog scale (VAS) pain scores, were collected when available. VAS scores were available for 141 patients preoperatively and 52 at the time of corresponding radiographic follow-up. FAAM-ADL scores were available for 45 patients preoperatively and 45 patients at the time of corresponding radiographic follow-up. PROM analysis was performed using a complete-case basis. No external funding or commercial support was received for this study.
Continuous variables were reported as means and SDs, whereas categorical variables were expressed as counts and percentages. Comparisons between patients with limited vs full postoperative DF were performed using independent t tests or Mann-Whitney U tests for continuous variables and χ2 or Fisher exact tests for categorical variables. To evaluate the validity of preoperative C-DF, we assessed its association with available radiographic weight-bearing DF using Spearman’s rank correlation. Multivariable logistic regression was performed to identify factors associated with achieving ≥20° of DF at final follow-up whereas multivariable linear regression was used to evaluate predictors of final DF angle as a continuous measure. Covariates included age, sex, BMI, preoperative C-DF, and prior open reduction internal fixation (ORIF). Statistical significance was set at P <.05. No imputation was performed for missing data. This study is explorative and therefore adjustments for multiple comparisons were not performed. All analyses were conducted using R software (version 3.6.3; R Foundation for Statistical Computing).
Results
Demographic and Baseline Characteristics
A total of 175 patients were included in this study, with 111 (63.4%) demonstrating limited postoperative DF and 64 (36.6%) achieving full DF at a mean 3.3 years. The mean age of patients with full DF was significantly higher than those with limited DF (65.5 vs 61.5, P = .013). With the numbers available, no significant difference could be detected in sex, BMI, weight, tobacco or alcohol use, and comorbidities including diabetes, anemia, gout, osteoporosis, heart disease, and rheumatoid arthritis. Overall, aside from age, demographic and comorbidity profiles were comparable between patients with limited and full postoperative DF (Table 1).
Patient Demographics and Comorbidities by Postoperative Dorsiflexion Status. a
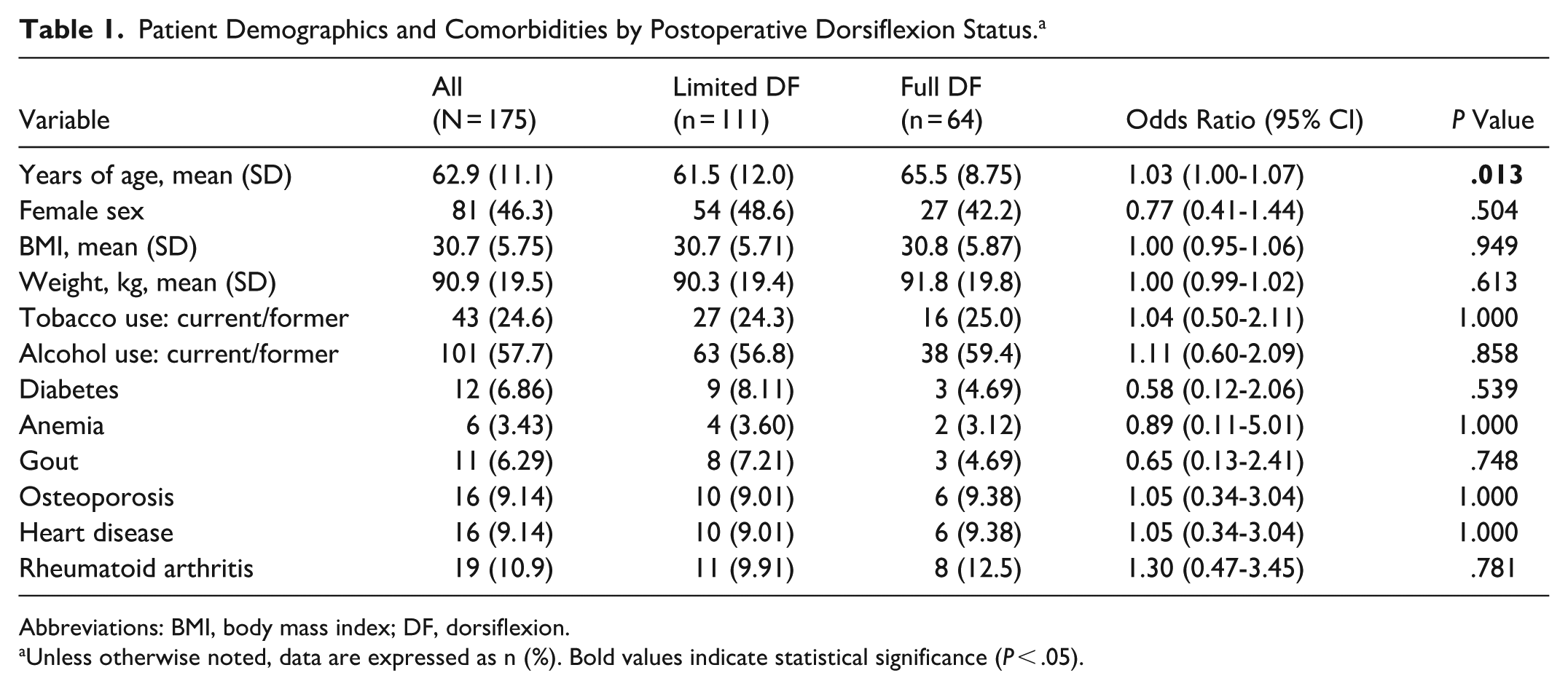
Abbreviations: BMI, body mass index; DF, dorsiflexion.
Unless otherwise noted, data are expressed as n (%). Bold values indicate statistical significance (P < .05).
Operative Characteristics
Patients who achieved full postoperative DF were more likely to have had full preoperative C-DF compared to those with limited postoperative DF (53.8% vs 32.2%, P = .019). Patients with and without available preoperative C-DF data (n = 36) did not differ significantly in age (P = .903), BMI (P = .237), sex (P = .287), and diabetes (P = .464) or tobacco history prevalence (P = .472) from those who did (n = 139). Further, C-DF demonstrated a moderate-to-strong correlation with radiographic weight-bearing DF (Spearman ρ = 0.63, 95% CI 0.48-0.74, P < .001). A history of prior ankle ORIF was significantly more common among patients with limited postoperative DF (38.7% vs 20.3%, P = .019). Rates of post-traumatic arthritis, preoperative steroid injection, and concomitant procedures such as TAL or gastrocnemius recession did not differ significantly between groups (all P > .05). There was no difference between groups regarding implant type (P = .053). Patients in the limited DF group had comparable preoperative patient-reported outcomes (P > .05) and there was no significant difference in polyethylene insert size between groups (P = .216) (Table 2).
Operative Characteristics and Preoperative Status by Postoperative Dorsiflexion Status. a
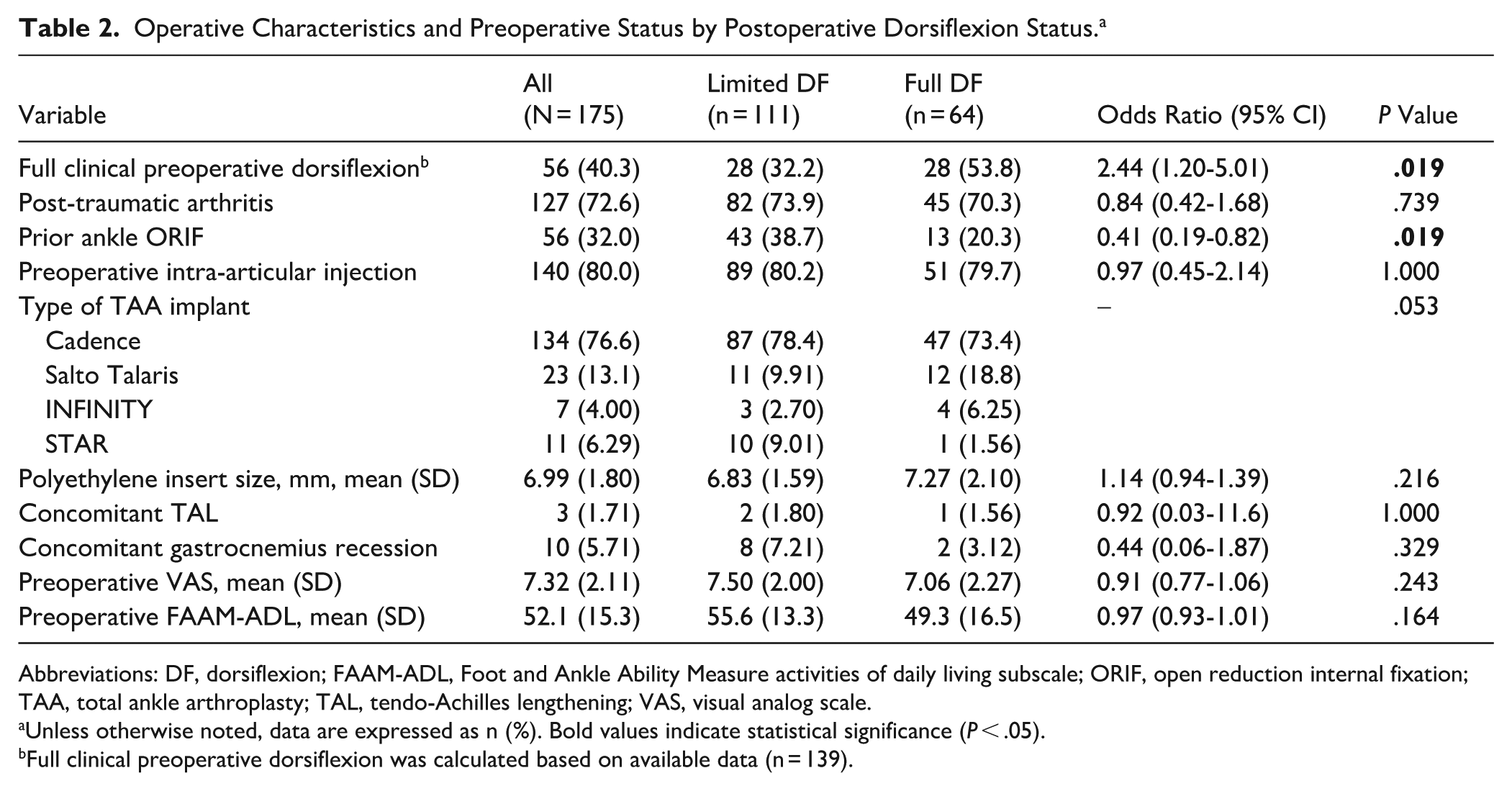
Abbreviations: DF, dorsiflexion; FAAM-ADL, Foot and Ankle Ability Measure activities of daily living subscale; ORIF, open reduction internal fixation; TAA, total ankle arthroplasty; TAL, tendo-Achilles lengthening; VAS, visual analog scale.
Unless otherwise noted, data are expressed as n (%). Bold values indicate statistical significance (P < .05).
Full clinical preoperative dorsiflexion was calculated based on available data (n = 139).
Postoperative Outcomes
Average final DF in the full DF group was 23.6° vs 13.9° in the limited DF group (P < .001). Additionally, full DF patients reported significantly higher postoperative FAAM-ADL (70.0 vs 86.9, P = .010) but not VAS (3.60 vs 3.23, P = .674). In adjusted linear regression, each additional degree of DF was associated with a 0.82‑point increase in FAAM‑ADL (95% CI 0.23-1.88). Radiographic follow-up duration was similar between groups (P = .151). Final average plantarflexion was 16.4° and total arc was 32.7°. Neither total arc or plantarflexion were associated with postoperative DF (P > .05) (Table 3).
Postoperative Outcomes. a
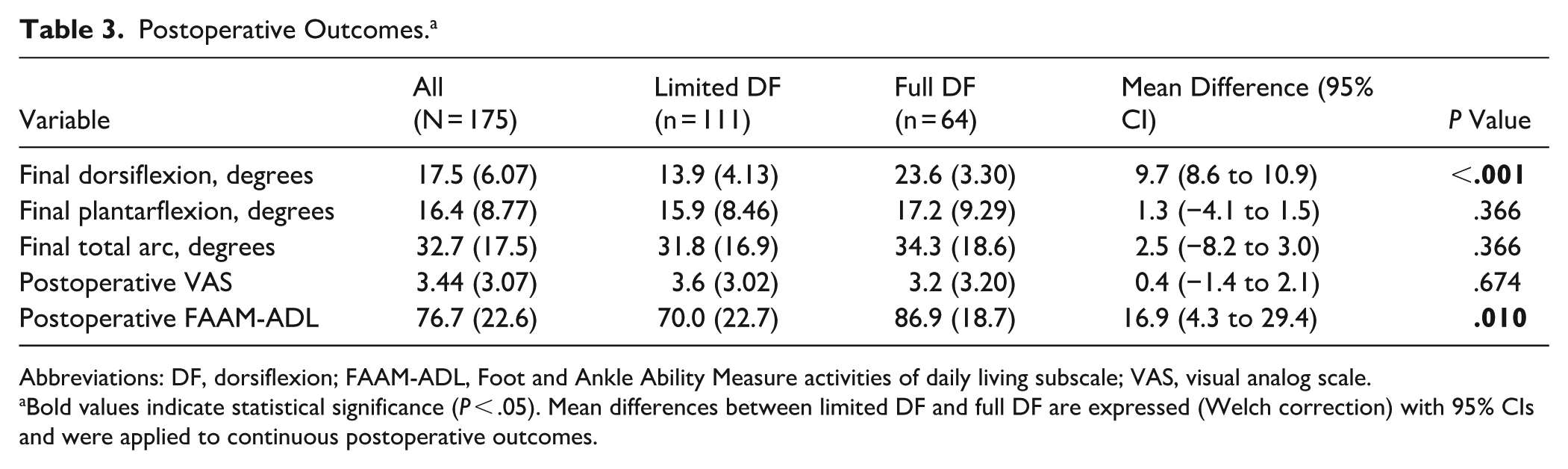
Abbreviations: DF, dorsiflexion; FAAM-ADL, Foot and Ankle Ability Measure activities of daily living subscale; VAS, visual analog scale.
Bold values indicate statistical significance (P < .05). Mean differences between limited DF and full DF are expressed (Welch correction) with 95% CIs and were applied to continuous postoperative outcomes.
Multivariable Regression Analysis
Multivariable regression analyses identified full preoperative C-DF as a significant independent predictor of improved postoperative DF following TAA. In the logistic model assessing the likelihood of achieving ≥20° of DF, patients with full preoperative C-DF had over twice the odds of attaining this threshold compared to those without (OR 2.20, 95% CI 1.05-4.66, P = .038). In the linear regression model, patients who had full preoperative C-DF achieved 2.93° greater final postoperative DF than those who did not (95% CI 0.85-5.01, P = .0062). Other variables, including sex, BMI, age, and history of prior ankle ORIF, were not significant predictors in either model (all P > .05) (Table 4).
Multivariable Logistic and Linear Regression Analyses Evaluating Predictors of Postoperative Dorsiflexion Following Total Ankle Arthroplasty (TAA). a
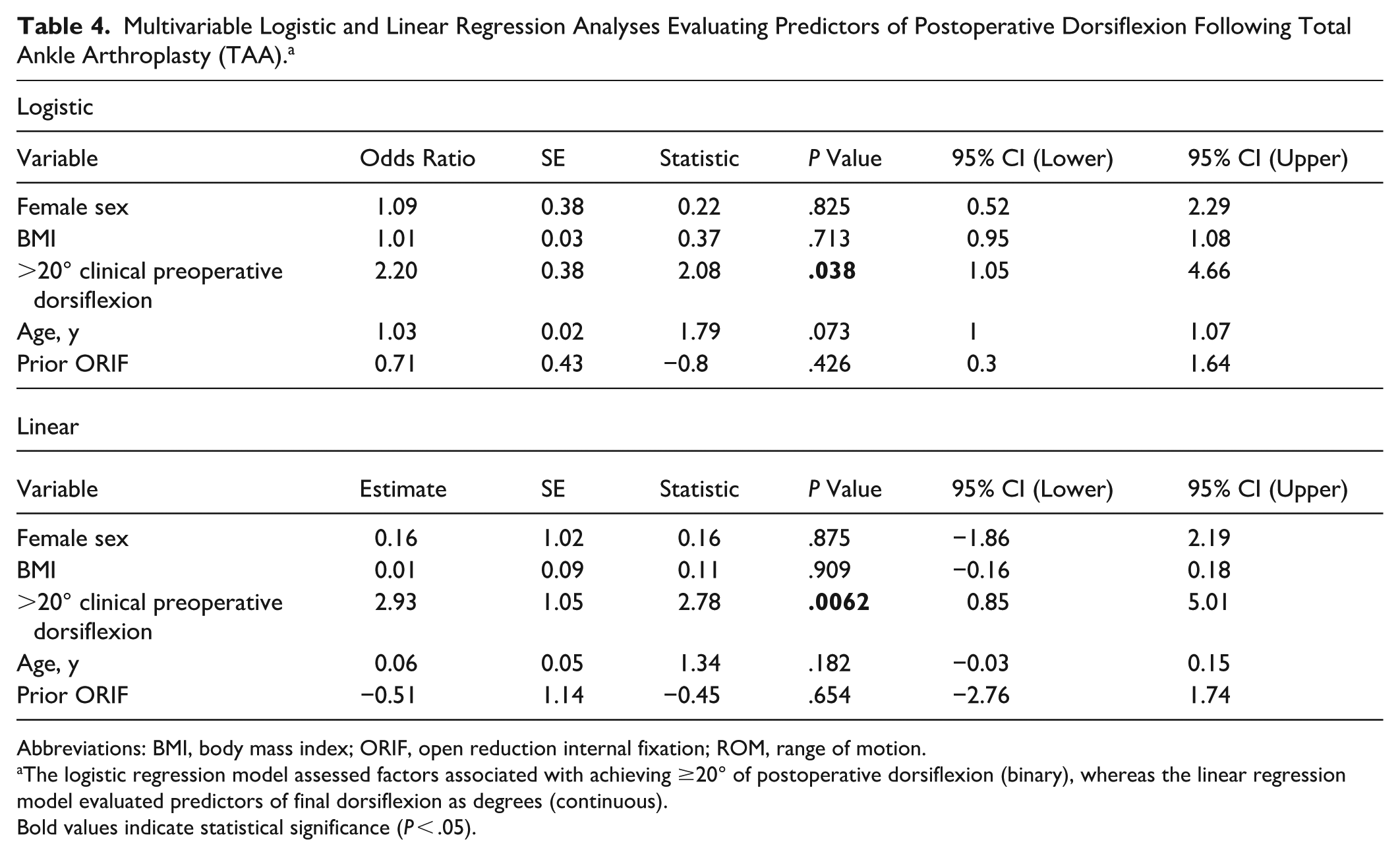
Abbreviations: BMI, body mass index; ORIF, open reduction internal fixation; ROM, range of motion.
The logistic regression model assessed factors associated with achieving ≥20° of postoperative dorsiflexion (binary), whereas the linear regression model evaluated predictors of final dorsiflexion as degrees (continuous).
Bold values indicate statistical significance (P < .05).
Discussion
Limited dorsiflexion after total ankle replacement is a challenging problem, with previous reports associating decreased ankle ROM with worse functional outcomes and lower patient-reported satisfaction following TAA.8,12 The purpose of this study was to identify predictive variables for postoperative DF following TAA. In an analysis of 175 ankles, limited preoperative C-DF was found to be the greatest predictor of postoperative DF following TAA. Prior ORIF on the index ankle was also more prevalent in patients with limited postoperative DF. Furthermore, limited postoperative DF was associated with less favorable FAAM-ADL scores.
Total ankle replacement has emerged as an increasingly effective treatment option for end-stage ankle arthritis, associated with improvements in pain and function as well as improved gait and increased ROM.2,18 A number of clinical and radiographic factors have been associated with increased risk of complications following TAA, including BMI, age, diabetes, tobacco use, hindfoot fusion, and preoperative deformity.19-25 Additionally, limited tibiotalar motion in the sagittal plane following TAA has been associated with lower FAAM functional scores and higher VAS pain.8,12 As indications and patient demand for TAA continues to expand, a thorough understanding of modifiable and nonmodifiable risk factors is vital to reduce complications and improve patient outcomes.
Previous reports have suggested that preoperative ankle ROM predicts postoperative ROM following TAA.13,14,17 There remains, however, limited evidence investigating the role of demographic variables and medical comorbidities in stiffness after ankle replacement. In a review of 175 TAA performed by a single surgeon, the current study did not find an association with patient factors such as BMI/weight, tobacco use, DM, sex, medical comorbidities, or inflammatory arthropathy and postoperative dorsiflexion following TAA. Younger age and history of previous ankle ORIF was associated with increased likelihood of stiffness following TAA; however, these findings did not hold true when analyzed in multivariable logistic and linear regression analyses. Notably, this study also demonstrated that limited postoperative ankle motion is common, with only 36.6% of patients achieving dorsiflexion greater than 20° at final follow-up. Additionally, there was a subtle but nonsignificant difference in implant type distribution between groups. Ten of 11 patients with a STAR implant demonstrated less than 20° of dorsiflexion at final follow-up. Although prior studies have not established consistent differences in dorsiflexion between individual implant designs, an important distinction exists between the mobile-bearing design of the STAR and the fixed-bearing designs of the Cadence, INFINITY, and Salto Talaris systems. Mobile-bearing implants have been proposed to allow for greater overall range of motion; however, the evidence remains inconsistent. 26 For example, a recent randomized trial by Queen et al 27 demonstrated no significant difference in peak plantarflexion or sagittal plane range of motion between fixed- and mobile-bearing designs.
Patients with preoperative dorsiflexion >20° were twice as likely to achieve full DF following TAA in this current cohort. These findings are consistent with previous reports, which identified preoperative ROM as predictive of overall ROM and gait function after TAA.13,14 Despite having a higher likelihood of postoperative stiffness, patients with limited preoperative motion may still benefit from a motion-sparing procedure such as TAA. In a report of 67 patients who underwent isolated TAA for end-stage ankle arthritis, Brodsky et al 13 found that patients with limited preoperative motion still experienced clinically significant improvements across numerous parameters of gait, although the absolute values were lower than in the patients with higher preoperative ROM. Ruiz et al 17 reported similar findings, indicating that although patients with preoperative stiffness exhibited improvements in sagittal motion, TAA offers limited capacity to meaningfully increase the preoperative range of ankle motion.
Despite these findings, patients undergoing TAA have shown consistent improvements in pain, function, and gait parameters regardless of ankle ROM, suggesting TAA can still offer clinically meaningful improvements for these patients.13,14 Identifying risk factors for complications and suboptimal outcomes following may facilitate more effective physician-patient communication throughout the perioperative period. Enhanced preoperative patient education and the establishment of appropriate expectations have been shown to be key determinants of postoperative satisfaction following TAA. 28 Patients whose expectations are met report greater improvement in pain and function, whereas those with unmet expectations—even if their pain and function improve—may be less satisfied. Providing a detailed explanation of anticipated ankle joint motion, especially in individuals with preoperative stiffness, may support more accurate postoperative expectations and has the potential to enhance overall patient satisfaction.
Understanding that limited preoperative range of motion is the strongest predictor for postoperative stiffness following TAA naturally raises the question of which adjunctive treatments or procedures might help mitigate this risk. The impact of concomitant TAL and gastrocnemius recession on motion after TAA remains controversial. Although limited compared with the overall cohort, the current study did not find an association between patients who underwent concomitant TAL or gastrocnemius recession and postoperative ROM. Previous studies have demonstrated an improvement in ankle dorsiflexion after such procedures; however, their impact on total arc of motion remains limited, most likely from a reciprocal loss of plantarflexion.15,29 In a prospective, nonrandomized study of 229 patients undergoing TAA, Queen et al 30 found that the use of a concomitant TAL or gastrocnemius recession procedure resulted in equivalent functional outcomes and gait mechanics compared with TAA alone. In addition to adjuvant procedures, intraoperative techniques may also play a role in tibiotalar motion, specifically joint line height. Elevated joint line has been associated with both decreased postoperative ROM and worse clinical outcomes after TAA.12,31 We did not find a correlation between postoperative dorsiflexion and plantarflexion or global ankle ROM. A substantial proportion of ankle range of motion is typically contributed by plantarflexion, which may partially obscure any association between dorsiflexion and global ankle ROM. 32 This effect could also signify a reciprocal loss of plantarflexion. Although plantarflexion strength is critical for push-off and forward propulsion during gait, deficits in dorsiflexion may have a more pronounced impact on proximal joint mechanics compared with isolated plantarflexion limitations. 33
Despite the use of various surgical techniques to improve range of motion after TAA, total postoperative ROM often remains comparable to preoperative values. 34 Moreover, a substantial discrepancy has been observed between the motion achieved intraoperatively and that ultimately realized postoperatively. Kim et al 35 reported that nearly 14° of motion was lost between the intraoperative and postoperative period. These findings prompt consideration of the role that postoperative immobilization may play in the loss of motion; however, interventions such as early mobilization appear to have minimal influence on postoperative ROM or functional outcomes. In a randomized controlled trial, Ramaskandhan et al 36 found no significant differences in ankle dorsiflexion, spatiotemporal gait characteristics, and functional outcomes scores between early mobilization and 6 weeks of plaster cast immobilization after TAA.
Importantly, patient-reported outcomes revealed a clinically meaningful pattern. Although preoperative VAS scores were higher in those with limited postoperative DF, this did not reach statistical significance. Similarly, preoperative FAAM-ADL scores were not significantly different between groups. In contrast, final FAAM-ADL scores were significantly higher in the full DF cohort. This suggests that FAAM-ADL may function as a strong proxy for postoperative radiographic range of motion whereas reported pain is not associated. However, this finding should be interpreted with caution, as substantial missing PROM data limited statistical power and the observed association was modest. Furthermore, the patients who did not fill out their PROM surveys could have differed systemically from those who did, which introduces an area of bias.
Postoperative motion following TAA remains a complex and multifactorial issue. To the authors’ knowledge, this is the first study to examine the influence of demographic factors and medical comorbidities on postoperative ankle motion. Although few associations were identified, the findings of this study reinforce the existing literature demonstrating the substantial impact of preoperative stiffness on postoperative motion and their negative effects on clinical outcomes.
This study has several limitations. First, as a retrospective analysis, inherent limitations exist and should be considered. Second, as previously mentioned, motion after TAA is a complex and multifactorial issue. When analyzing factors that impact postoperative motion, concomitant factors exist and should be considered in the context of the analysis. An effort was made to limit these variables by performing multivariable logistic and linear regression models; however, there remains the potential for additional concomitant variables that were not controlled for or included in this study. Additionally, ankle motion was measured relative to the tibial axis and the floor, which reflects the composite sagittal plane motion rather than isolated tibiotalar kinematics. This approach may introduce variability from adjacent joint motion and midfoot deformity. Furthermore, based on the observed proportions of patients achieving full dorsiflexion in the limited DF (32.2%) and full DF (53.8%) groups, the study had only approximately 70% power to detect this difference using a 2-sided α of 0.05. Therefore, these results should be considered hypothesis generating and interpreted with caution. Finally, preoperative plantarflexion and dorsiflexion radiographs were not available for the majority of patients, so preoperative dorsiflexion was rather defined as limited (<20° of dorsiflexion) or full (>20° of dorsiflexion) based on preoperative clinical documentation (C-DF). Because of this, preoperative motion analysis was performed in a binary fashion. Although it demonstrated a moderate to strong correlation with radiographic ROM, this measure was not intended as a substitute. Furthermore, the relatively high percentage of patients (31.4%) with adequate follow-up but inadequate postoperative radiographs should be considered a source of potential bias. Despite the aforementioned, the results of this study further enforce the impact preoperative motion has on postoperative stiffness following TAA, with limited evidence supporting the influence of patient demographics and medical comorbidities.
Conclusion
Preoperative clinical dorsiflexion was identified as the only significant predictor of postoperative dorsiflexion following TAA. Accordingly, a thorough preoperative discussion regarding anticipated postoperative motion can help establish appropriate expectations and potentially enhance patient satisfaction.
Supplemental Material
sj-pdf-1-fai-10.1177_10711007261457413 – Supplemental material for Predictors of Limited Weight-Bearing Dorsiflexion Following Total Ankle Arthroplasty
Supplemental material, sj-pdf-1-fai-10.1177_10711007261457413 for Predictors of Limited Weight-Bearing Dorsiflexion Following Total Ankle Arthroplasty by Grant M. Thomas, Joseph A. S. McCahon, Yoni Dulitzki, Zhongxuan Chen, Selene G. Parekh, Joseph N. Daniel and David I. Pedowitz in Foot & Ankle International
Footnotes
Acknowledgements
The authors thank Matthew Sherman, BS, for his assistance with data analysis.
Author Note
This investigation was performed at the Rothman Orthopaedic Institute at Thomas Jefferson University, Philadelphia, Pennsylvania.
Ethical Considerations
Approved by Thomas Jefferson University Institutional Review Board under iRISID-2024-0816.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Selene G. Parekh, MD, MBA, reports financial relationships within the past 3 years, including intellectual property royalties from Paragon, Extremity Medical, OrthoHelix, Arthrex, Novastep, Additive Orthopaedics, and Smith & Nephew. He also holds stock in Restor3d, TensorFlow, Immersive Tech, Acuitive Technologies, Addivation Medical, Oxford Performance Materials, Curvebeam AI, WishBone Medical, OSSIO, GLW, Carbon 22, Alafair Biosciences, Resolute, Extremis Robotics, Operative Armour/Sharp Fluidics, Scalpel Ventures, Tyber Medical, Plantiga, Active Medical, Protect3D, and ![]() . He has participated in other professional activities with Arthrex, ACUMED, CONMED Corporation, Smith & Nephew Orthopaedics, and Auxano Medical. These relationships are unrelated to the content of this manuscript and are not perceived to introduce bias. Joseph N. Daniel, DO, reports Stryker: paid consultant; paid presenter or speaker; Wright Medical Technology, Inc: paid consultant. Disclosure forms for all authors are available online.
. He has participated in other professional activities with Arthrex, ACUMED, CONMED Corporation, Smith & Nephew Orthopaedics, and Auxano Medical. These relationships are unrelated to the content of this manuscript and are not perceived to introduce bias. Joseph N. Daniel, DO, reports Stryker: paid consultant; paid presenter or speaker; Wright Medical Technology, Inc: paid consultant. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.