
Abstract
From 1987 to 1993, 20 athletes (22 feet) underwent cheilectomy 10 for Regnauld grade I, 7 grade II 16 hallux rigidus. Average age was 31 years (10 men and 12 women); mean follow-up was at 5.1 years. All patients performed high-level sports (judo, track & field, soccer, and skating). Indications for surgery included failure of nonsurgical treatment with persistent pain during sports activities, shoefitting problems, and recurrent bursitis.
The aim of our study was to evaluate the results clinically, radiographically, and objectively, using dynamic and static pedodynographic measurements. After a mean follow-up of 5 years, cheilectomy was demonstrated to be a reliable treatment method in athletes with Regnauld grades 1 and 2 hallux rigidus. Functionally, 14 excellent, seven good, and one fair result were noted. Radiological progression was noted in 7 of 13 patients, with a follow-up of >4 years.
Postoperative dynamic pedodynographic findings demonstrated moderate but significant changes in peak pressures under the first metatarsal head, the hallux, and in the center of pressure distribution under the forefoot.
INTRODUCTION
Injuries of the first metatarsophalangeal (MTP) joint in athletes have become a significant concern of athletes, coaches, and physicians.
17
Despite the increasing incidence of these lesions in athletes and the considerable disability associated with acute and chronic injuries (hallux rigidus), first MTP joint injury has received little attention in sports literature.
1,10,14
Hallux rigidus is the second most common deformity of the first
Repetitive hyperextension injury of the first MTP joint is one of the most common mechanisms leading to hallux rigidus. Joint kinematic studies reveal compression of the articular cartilage and the subchondral bone at the extremes of hyperextension of the first MTP joint. 17 Other factors described in the literature are metatarsus primus elevatus, hyperpronation, os-teochondritis dissecans, poor footwear, a long first metatarsal, abnormal gait, obesity, sex, and occupation. 10,11,13 .
The diagnosis of hallux rigidus in this study is based on the presence of pain in the first MTP joint and physical findings of restricted dorsiflexion (<30°), increased joint bulk (dorsally), and associated synovitis (swelling, tenderness, and pain with motion). Numerous procedures have been described in the literature to treat this condition, including cheilectomy 4,5,9,10 or exostosectomy, dorsiflexion osteotomy of the proximal phalanx, 8 resection arthroplasty, 12,13 different types of implant arthroplasty, 4,7,15,18,19 and arthrodesis 8,12,13 .
Although cheilectomy does not result in a normal hallux function in athletes, it offers the advantage of relieving the pain. It preserves a variable amount of motion and power that are lost after resection arthroplasty or arthrodesis. Furthermore, it avoids the potential complications of implant arthroplasty and arthrodesis. 4,5 Questions remain about the indications and the long-term effectiveness of cheilectomy. No studies have been found to describe the results of cheilectomy in a specific population of (high-level) athletes with hallux rigidus or to report objective data to quan-titate the efficacy of cheilectomy.
The purpose of this study was to assess functional and objective long-term results after cheilectomy, specifically in athletes with hallux rigidus. The hypothesis of this study was that athletes may receive greater benefit from cheilectomy then nonathletes.
MATERIALS AND METHODS
From February 1987 until October 1993, 71 cheilec-tomies were performed at the orthopaedic departments of the University Hospital Pellenberg (65 cases) and Heilig Hart Leuven (6 cases) by two of the authors (G.D. and T.M.). Inclusion criteria for this study were hallux rigidus, grade I (6 cases) and grade II (16 cases), and sports activities, either professional or high-level (>6 hr/wk, international or national level). Twenty-five procedures (35%) were performed on high-level athletes. Three patients were lost to follow-up. Twenty patients (22 procedures) were reviewed personally by the author (T.M.) after a mean follow-up of 5 years (range, 17–108 months). There were 13 men and 7 women (nine left and thirteen right [two bilateral]) cases of hallux rigidus. Preoperative x-ray grading 16 demonstrated six grade I, eight grade 11 A, and eight grade IIB cases.
The mean age at operation was 30.9 years (range, 19–45 years) and complaints averaged 4 years (6–312 months). Sports activities included soccer and judo (five cases each), volleyball (three cases), basketball, skating, dancing, and tennis (one case). Large shoes with a stiff sole, nonsteroidal anti-inflammatory drugs, and intra-articular injections were given preoperatively. If the pain (17 cases), shoefitting problems (seven cases), and recurrent bursitis (six cases) persisted during sports activities after an adequate trial with nonsurgical treatment, MTP cheilectomy was proposed.
All toes were treated by cheilectomy according to Mann, 8 Mann and Clanton, 9 and Mann et al. 10 A curved dorsomedial incision was used, medial from the extensor hallucis longus tendon. The joint space was inspected, and any loose bodies and synovitis were excised. The dorsal, medial, and lateral osteo-phytes of the metatarsal head and proximal phalanx were largely removed, along with the dorsal one-third to one-fourth of the metatarsal head, and the sesam-oids were inspected. The dorsal bone block was removed, allowing a preoperative mobility of 60° to 80°. The raw bone surfaces were rasped smooth. Occasionally, drilling of subchondral bone was added for articular defects. Routine surgical closure, preserving the obtained amount of dorsiflexion, was followed by a compression bandage. Postoperatively, 24-hour elevation was followed by wooden-sole partial weight-bearing ambulation for 2 weeks and immediate active and passive mobilization. Sports activities were permitted after 6 weeks.
METHODS
The patients were questioned and examined preop-eratively and at the time of the last clinic. A cheilectomy assessment sheet was used. This assessment sheet included (Table 1): (1) a detailed questionnaire, (2) a subjective functional evaluation similar to that of Hattrup and Johnson, 5 (3) a clinical evaluation similar to Mann and Clanton, 9 and (4) a radiological grading. 15 Regnauld's classification was used: grade I, normal x-rays with subtle changes, flattening of the metatarsal head and proximal phalanx, and enlargement of the two articular joint surfaces but no structural disease of the sesamoid except enlargement or minor osteophytes; grade II, narrowing of the first MTP joint, flattening of the metatarsal head and base of the proximal phalanx (2A), and hypertrophy of the sesamoids (2B); and grade III, severe loss of the first MTP joint space and extensive dorsal, medial, and bridging osteophytes from the proximal phalanx to the sesamoids.
Cheilectomy Assessment Sheet
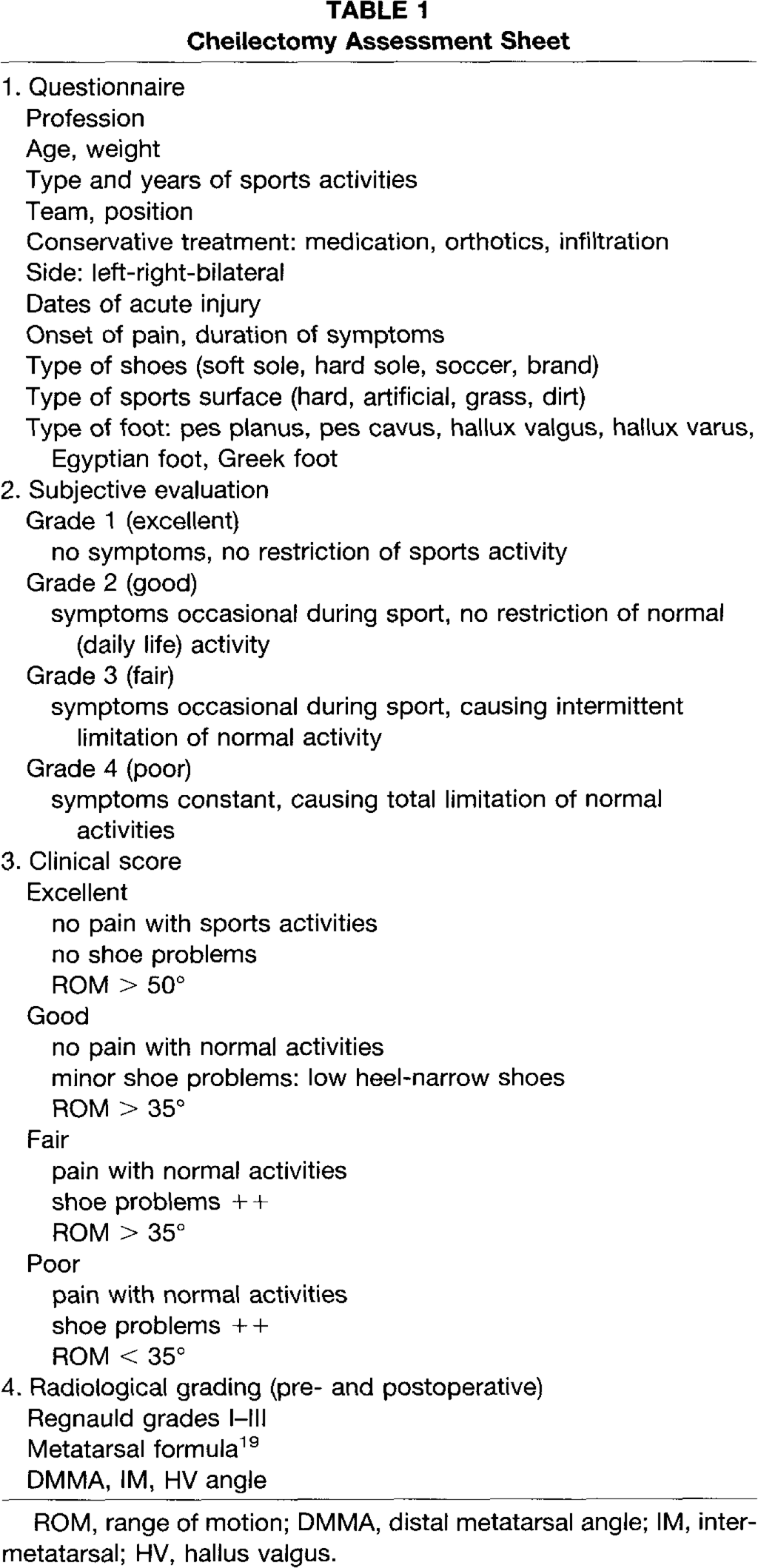
ROM, range of motion; DMMA, distal metatarsal angle; IM, inter-metatarsal; HV, hallus valgus
Pre- and postoperative standing AP and lateral views were performed. At final review, an axial view of the sesamoids and a nonweightbearing lateral view in maximal dorsiflexion of the first MTP joint was performed. This film demonstrates the impingement of the dorsal osteophytes on the proximal phalanx and provides a document of maximal dorsiflexion.
The intermetatarsal angle, MTP, and distal metatarsal angle were measured on standing x-rays. The relative length of the metatarsals was measured and classified according to Viladot 19 as index minus (second metatarsal shorter then the first metatarsal), index plus minus (equal length), or index plus (second metatarsal longer then the first metatarsal). The relationship between clinical result and radiological grade of disease was assessed.
Pre- and postoperative static and dynamic pedody-nographic (PDG) measurements were performed and examined by one of the authors (L.P.). Calluses were not trimmed by the examiners before collecting pressure data. No attempt was made to ensure that patient gait velocity was constant between pre- and postoperative measurements. An in-shoe transducer was used; small disk-like transducers that can record dynamic and static foot pressure were applied to the sole of the foot. A total of 128 sensors (force sensing resistor) were evenly distributed over the area. Measurements were made point-to-point so that they were totally independent, one from another. Patients were asked to walk in a straight line at a comfortable gait velocity, with the sensor insole (having a cross section of 7.5 mm) in a standard shoe (PDG system, Delaware Industrial Systems, Grote Steenweg Noord, Gent, Belgium). Each sensor was connected by two leads, which ruled out any cross-talk between sensors. Sensor reaction time was almost immediate (0.5 msec), whereas registration intervals were taken to be 16.7 msec. The same pair of standard shoes (ranging from size 35–44) are used for all pre- and postoperative measurements. These shoes have a flat footbed and a small heel height (12 mm). Because of their construction, they are adaptable to practically all feet so that a snug fit can still be obtained, even after possible resizing of the foot postoperatively. Possible relocation or resizing of the foot in relation to the insole sensors across different measurements over time, has to be compensated for by the computing program. 2 Several trials were stored and consistent trials with each foot were used in the final analysis. Each pair of insoles is calibrated under increasing and decreasing hydrostatic pressure. With this conductive type of transducer, deformation of a portion of a transducer results in the resistance to current flow through the transducer. 2,3 This change in current is registered as a change in voltage output and can be related to the force applied (force-sensing resistor). The in-shoe transducers are linked with cable connections with the portable measurement module and to a computerized instrumentation system (master unit) to measure the distribution of vertical load under the foot. 2 The machine prints an outline of the load-cell matrix with the peak force in newtons recorded by each cell during walking. The variation of the center of pressure during foot contact can be superimposed, as can the peak forces for a particular area of interest. 3 With these PDG examinations, static and dynamic measurements can be obtained as well as peak forces, peak pressures (highest peak force ÷ area of one load cell), curve of total force against time, % of total force (and pressure)/area of interest, mean total forces associated with heel contact-foot flat, foot flat-heel off, and heel-off toe-off.
When using these PDG measurements and the PDG system as an objective evaluation tool, some disadvantages can be noted. The output of conductive-type transducers tends to drift with use, and a relatively high coefficient of variation is observed with most of the measurement devices. In laboratory conditions, this variation with the PDG system was only 2%. 2 Other limitations include interobserver variations, poor spatial resolution, relatively low correlation of clinical findings and PDG measurements (70–80%), inability to measure vertical and horizontal shear forces with the pedodynograph, and lack of reference studies and normative values. 2,3
RESULTS
Subjective Evaluation
Preoperatively, five cases were ranged as grade II, sixteen cases as grade III, and one case as grade IV. Postoperatively, fourteen procedures were grade I, seven were grade II, and one was grade
Clinical Score
Preoperatively, five patients had a poor rating, five good, and twelve fair. Postoperatively, the score changed to one fair, nine good, and twelve excellent patients. Return to sports activities was at 11.5 weeks (range, 4–21 weeks). Preoperative dorsiflexion was 27° (range, 0–50°), and plantarflexion was 19° (range, 10–40°). Postoperative dorsiflexion was 40° (range, 10–60°) and plantarflexion was 23° (range, 15–45°). The unaffected contralateral hallux demonstrated 56° dorsiflexion and 17°° plantarflexion.
Radiographic Results
There were no x-ray changes (deterioration in the Regnauld grading) at final review in four of six grade I patients. In two patients, slight deterioration (grades l-IIA) occurred. In six of sixteen grade II patients, there was a degeneration at the metatarsosesamoid joint without detectable changes in the MTP joint. Of eight grade IIA patients, four worsened to grade MB, and two patients with grade IIB involvement deteriorated to grade III. The intermetatarsal angle, distal metatarsal angle, and hallux valgus angle did not change; preoperative and postoperative angles were, respectively, 8° and 7°, 18° and 19°, 22° and 22°. The metatarsal formula (as measured according to Viladot) 19 was 31% index +, 13% index ±, and 56% index-. No correlation was found in our study between clinical results and radiological grading.
Complications
Complications seen in two patients included one reflex-sympathetic dystrophy and one neuroma.
Recurrences
Mild radiographie recurrences were noted in two cases, after 2 and 5 years, respectively. No further surgery has been performed at present in these patients.
PEDODYNOGRAPHIC FOOT PRESSURE MEASUREMENTS
Peak Loads Under the First MTP Joint
Preoperatively, the mean peak load under the head of metatarsal 1 was 1.4 (range, 0.9-2.2 kg/cm2) (Table 2). Postoperatively, the mean peak load was 1.6 kg/ cm2 (range, 1.1-2.2 kg/cm2). Postoperatively, none of the patients demonstrated abnormal high pressure (>3 kg/cm2), 2,3 14% had low or no pressure (<0.5 kg/cm2), and 84% had normal pressure (0.5-2.5 kg/ cm2) under the first MT head (preoperatively, 7% high, 80% normal, and 13% low or no pressure.
Distribution of Areas of Maximum Pressure
Preoperatively, the area of maximum pressure under the forefoot was located under the first metatarsal head in 31% of our patients (Fig. 1). The area of maximum pressure was localized under the second metatarsal in 15% of cases, under the third in 17%, under the fourth in 32%, and under the fifth metatarsal head in 5%. Postoperatively, the maximum pressure was situated under the first metatarsal head in 55% of cases, under the second in 6%, under the third in 11%, under the fourth in 17%, and under the fifth metatarsal in 11%.
DISCUSSION
Hallux rigidus is a common forefoot problem. The ideal surgical procedure for the management of symptomatic hallux rigidus remains a controversial subject. 13 Many authors suggest that although relief of pain can be achieved with any procedure (arthrodesis, arthroplasty, or total implant), the cheilectomy technique simultaneously increases joint motion, 15 maintains stability, 4 avoids shortening with loss of purchase power, 5 and avoids the prolonged healing time with increased morbidity of an osteotomy or arthrodesis. 7,8,13 Disadvantages include that it does not treat the cause and can be joint destructive 4 and that it is not as successful in late Regnauld grade II or III changes. 5 The typically involved patient is a middle-aged female with unilateral hallux rigidus. 10 Different authors have described the results after cheilectomy in this population group. 4,5,9,15,19 .
Averaae Maximum Pressures for the Detailed Foot Zones a

In kg/cm.
MT, metarsal; T, toe; Preop, preoperative; Postop, postoperative
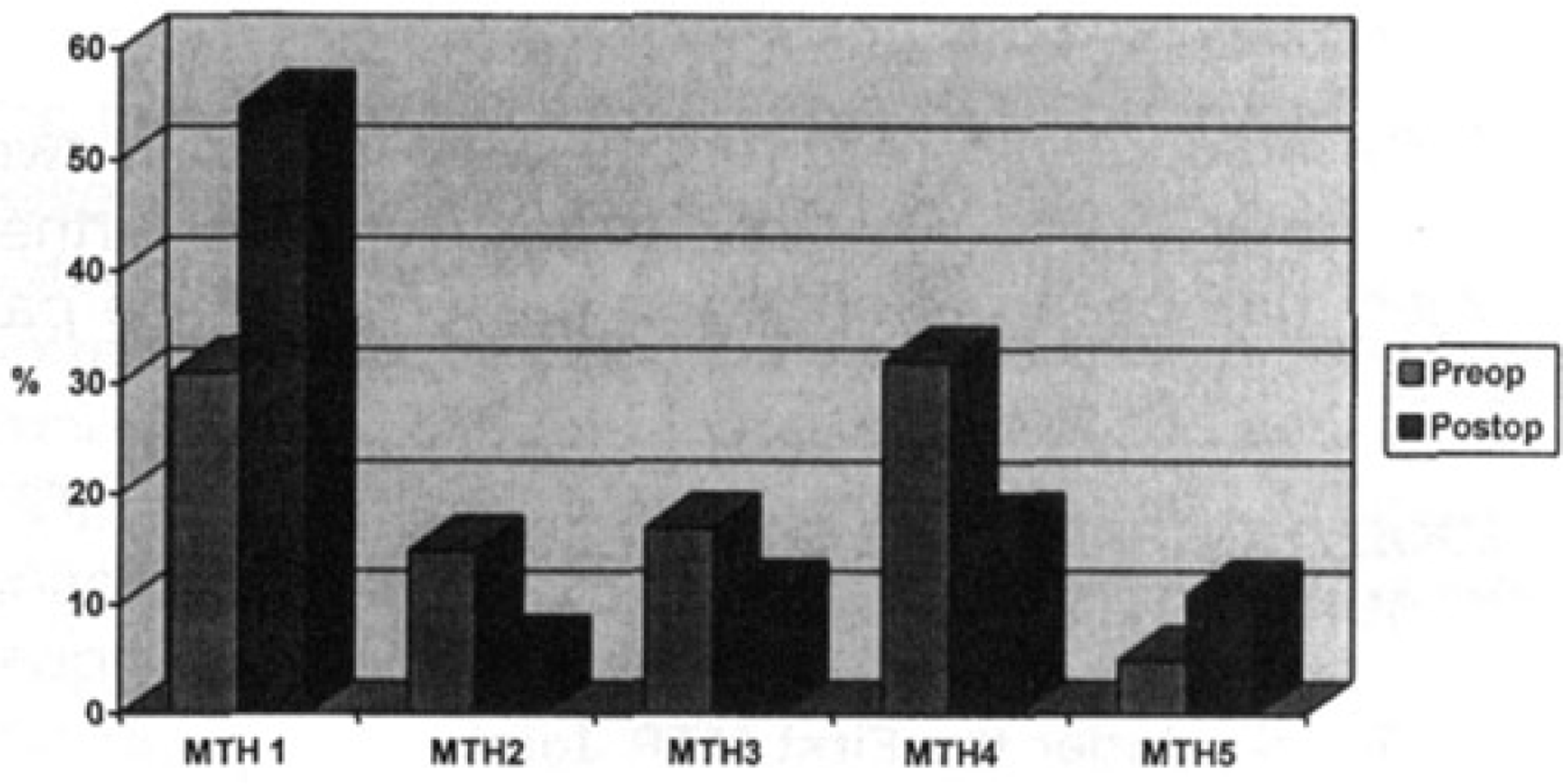
Distribution of areas of maximum pressure.
In our series, 78% good and excellent results were noted in these patients. According to these studies, relief of pain, improvement of joint motion, and long-term degenerative changes are important in the evaluation of results after cheilectomy. A second group of patients with hallux rigidus are high-level athletes. 1,14 Objective data are needed to evaluate the results in this frequently involved, high demand population.
Subjective assessment of our athletes demonstrated that 75% had complete relief of pain, and 20% had occasional symptoms (95% good and excellent results). These results are comparable with those of Mann et al. 10 and Mann and Clanton. 9 These authors noted 85% and 88% relief of pain, respectively. Surprisingly in our series, we noted that six patients with radiographie grade I involvement and five patients with clinical grade II involvement were subjected to the risks of surgery. These patients had definite problems during sports activities that did not respond to non-surgical treatment. In our series, 7 of 22 patients reduced their sports activities postoperatively. In five patients this was caused by problems not related to the hallux rigidus deformity. This can be explained by the fact that evaluation of our athletes was performed using the same subjective assessment methods as were described in other series on a general population. 5,9,10 A good outcome in our series may theoretically still result in a lower level of sports activity, with serious financial implications for the professional athlete.
Although it may be difficult to compare measurements between different series, functional analysis showed that the range of motion (62%) was better in athletes than in the general population (Mann et al., 10 36°; Mann and Clanton, 9 48°; and Pontell and Gu-das, 14 58°). This can be explained by the younger age group (30 years) of our study, the specific population of athletes, a lesser radiological involvement, and immediate postoperative mobilization. A definite amelioration of the range of motion (46–63°) was seen in the first MTP joint, which was not always the case in other series.
In our series of athletes, with a mean follow-up of 5 years, good long-term results were obtained in grades I and II hallux rigidus. Two mild recurrences were noted after 2 and 5 years, respectively. No clear deterioration was observed with longer follow-up. Reviewing the literature, Gould 4 reported on a group of 12 patients with a follow-up of 2.4 years, all leading to good results. Hattrup and Johnson 5 were the first to report on a group of patients with a follow-up of >3 years. The functional results were analyzed according to the preoperative radiological appearance. The failure rate was 15% for grade I, increasing to 37.5% for grade III. These authors concluded that cheilectomy was not indicated in grade III hallux rigidus.
In contrast, Mann et al. in 1979 and Mann and Clanton in 1988 reviewed 56 patients, 9,10 all having degenerative arthritis with a follow-up of 4.5 years. Cheilectomy may be a better treatment method in their cases for hallux rigidus than arthrodesis, resection arthroplasty, or flexible-implant arthroplasty.
Radiological progression after surgery is still open for debate. 6 Mann and Clanton 9 reported that little deterioration occurred with time. Pontell and Gudas 14 documented limited osteophyte reformation and continued joint space narrowing in four of eight patients after 66 months. We reviewed our patients with a follow-up of >4 years (13 cases). In half of the grade II patients, a degeneration was seen at the metatarso-sesamoid joint on lateral radiographs without detectable changes in the MTP joint. There were minimal changes in the radiographie appearance of the grade I patients at final follow-up. No correlation was observed between clinical results and radiological grading.
There are little objective data available in the literature to evaluate the efficacy of cheilectomy in promoting a more normal distribution on the plantar aspect of the foot within the shoe during walking. 18 Our study reports some new objective data about the effects of the cheilectomy procedure on the foot pressure distribution under detailed areas of the foot and, also, the temporal characteristics during stance phase.
Rather than using the average pressures throughout the total time, the maximum pressures were tested during only the load phase of the zone. This gives a better idea of the real loading of the different areas of the foot. 2 .
Comparing preoperative and postoperative peak pressure measurements, we made the following observations: 1) the distribution of the areas of maximum pressure was preoperatively localized more frequently under the lesser metatarsals then postoperatively, and peak pressures under the first metatarsal head were found more distally under the hallux; 2) the changes of pre- and postoperative foot pressure measurements under the toes, the forefoot, and the heel were nonsignificant in our athletes; and 3) the mean peak pressure under the first metatarsal head did change slightly (1.4 kg/cm2, preoperatively, and 1.6 kg/cm2, postoperatively). The peak pressure under the hallux (phalanx) was higher preoperatively (1.2 kg/cm2) than postoperatively (0.8 kg/cm2).
Finally, it is important to note that although dynamic gait analysis revealed a number of important observations, some limitations became apparent using this tool as an objective evaluation method. 2,3 Additionally, with each different PDG system, the enormous amount of data are processed using different software programs. This makes comparison between studies difficult. Pressure values obtained in our study were slightly lower than the ones reported in other series in the literature. 2 .
CONCLUSION
After a mean follow-up of 5 years, cheilectomy was demonstrated to be a reliable treatment method in athletes with Regnauld grades I and II hallux rigidus. Subjective assessment demonstrated 90% good and excellent results in athletes. Objective assessment with dynamic PDG findings demonstrated changes in peak pressures under the first metatarsal head and hallux