
Abstract
We report a case of bilateral Achilles tendon xanthoma as the first clinical manifestation of familial hypercholesterolemia. We review the literature and stress the need for orthopaedic surgeons to be familiar with this disease. An early diagnosis of this metabolic disorder is important to institute medical therapy and to alter the course of the disease before the onset of coronary artery disease.
INTRODUCTION
Achilles tendon xanthomas may appear as the first clinical manifestation of familial hypercholesterolemia (FH). 5,11,19,21 Patients may visit the orthopaedic surgeon without knowing they have a lipidic disorder. The orthopaedic surgeon needs to be able to diagnose the underlying disease, because Achilles tendon xanthomas are pathognomonic of FH. 2
It is important that orthopaedic surgeons be familiar with FH because patients with FH are at high risk for premature coronary atherosclerosis, 2 which might be prevented or delayed with adequate medical treatment. However, our exhaustive literature review yielded only a few reports on this disorder. 4,7–9,13,14,16–18,20 Consequently, we have decided to study one such case.
CASE REPORT
A 45-year old patient was treated at our hospital for the first time on September 15, 1993 for tumors in both Achilles regions that had been slowly growing for several years, causing pain and deformity. There were neither traumatic records nor a family history for this disorder. Physical examination revealed a moderate, uniform obesity of the patient (height, 158.2 cm; weight, 73.3 kg) and firm, diffuse tumors in both Achilles tendons (Fig. 1). The mobility of the ankles was not affected. No other nodules or skin lesions were observed in any other limb. The x-ray of the ankle and foot revealed a normal osseous structure. Axial and sagittal magnetic resonance imaging of both ankles revealed a uniform enlargement of both tendons of >8 cm, with areas of sacciform dilations (Fig. 2).
With a provisional diagnosis of hypercholesterolemic xanthoma, the patient was referred to the Lipids Unit of the Department of Internal Medicine. Laboratory studies revealed an increase in the level of cholesterol (585 mg/dL, N = 150–250 mg/dL), of the high density lipoprotein fraction (99 mg/dL, N = 35–50 mg/dL) and especially of low density lipoprotein (LDL) (463 mg/dL, N = 80–140 mg/dL), with normal triglycerides (76 mg/dL, N = 70–170 mg/dL). As several family members (mother, sister, son, and nephew) were also shown to be affected (although they did not present any tendinous xanthomas) the diagnosis was FH.
DISCUSSION
Achilles tendon xanthoma is a rare disorder of great interest for orthopaedic surgeons. It has important ramifications within Internal Medicine and Dermatology because it is associated with a specific disorder of lipidic metabolism, FH, and is characterized by increased LDL cholesterol, tendon xanthomas, coronary disease, and autosomal dominant transmission.
The primary defect in this disease is a mutation in the gene for the LDL receptor, as described by Goldstein and Brown. 11 The importance of the disease lies in the premature development of coronary disease, 25 times more common in affected patients than in unaffected patients. Their mean age of death by coronary disease is lower than that of the general population. 2
Xanthomas usually appear in the second decade of life, 11,19 and their detection is crucial for an early diagnosis, which is extremely important to begin medical therapy to alter the course of the disease before the onset of the coronary artery disease.
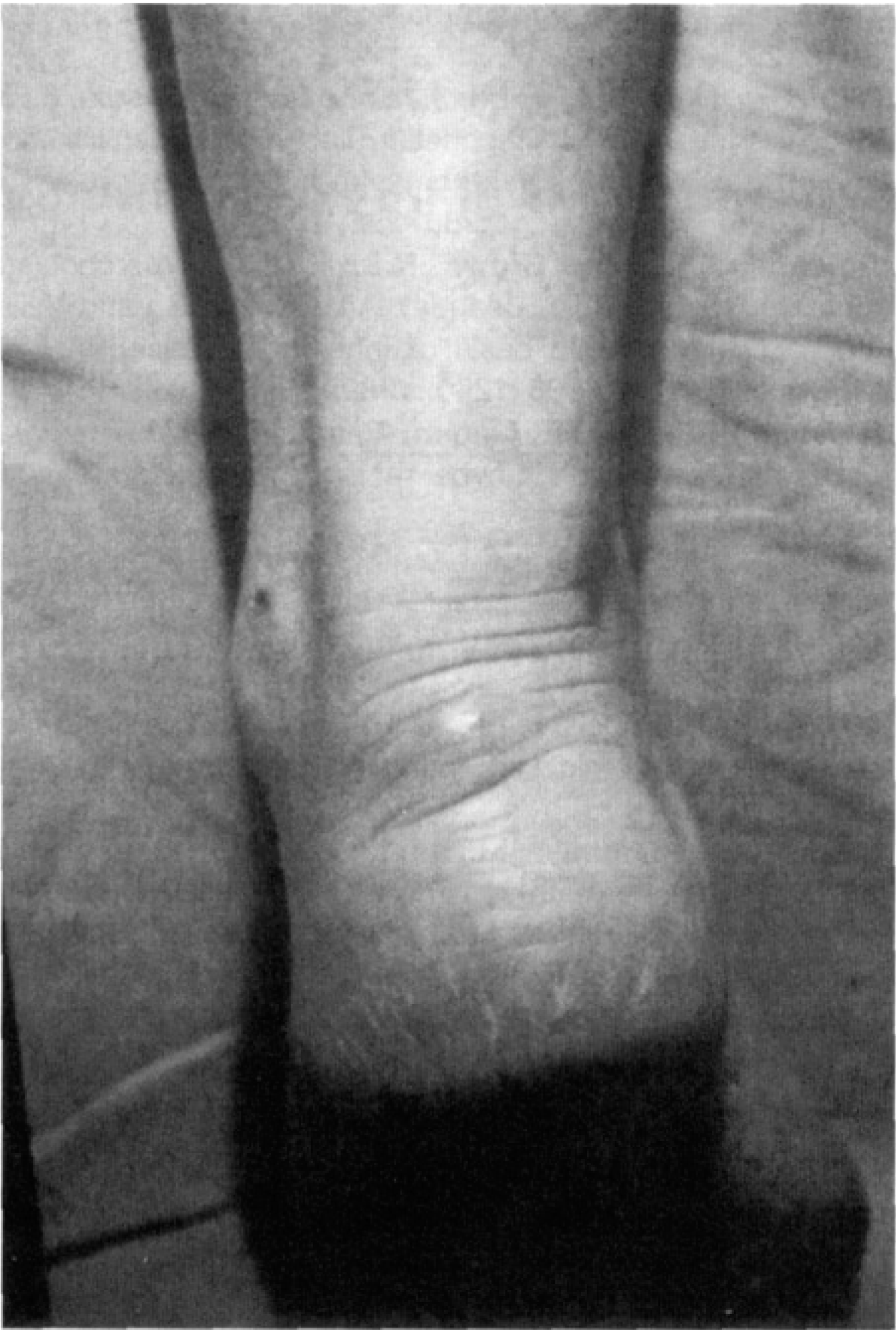
Clinical aspect of Achilles tendon affected by xanthomas.
Although xanthomas have also been described in the absence of FH, 8,12 this disorder is considered to be pathognomonic of FH, 2 and it may be the first clinical manifestation of the disease. 5,11,19,21 Thus, it is important that the orthopaedic surgeon should be able to detect it. This explains why so many imaging techniques have been used for diagnosing xanthomas before they could be clinically detectable. These techniques included radiographs, 1 xeroradiographs, 19 gammagraphies, 10 ultrasonography, 3,12 computed tomography, 5 and magnetic resonance. 3,6
Xanthomas are composed of connective tissue and foam cells that contain cholesterol, cholesterol esters, triglycerides, and phospholipids. These foam cells infiltrate the tendon and adjacent tissues. 7 There is a correlation between the number and size of lesions and the patient's cholesterol level, age, and sex. 15
Surgical treatment is only indicated when the xanthoma becomes large, painful, and irritable from rubbing against the shoe. 7,13,17 Of the 173 cases reported by Fahey et al. 7 in 1973 in the British literature, only 15 cases were surgically treated, and only 9 cases were reported on later. 13,14,16,18,20,21 Among the surgical methods proposed, the excision of tumoral nodules and subtotal resection result in a relatively high recurrence rate. 7,16 The best technique, when there is severe, diffuse infiltration into the tendon or when the tendon is torn, may be the total resection of the area between the musculotendinous and the calcaneus junctions and the reconstruction of the defect with fascia graft. This procedure yields satisfactory results and a lower recurrence rate 13,18,20
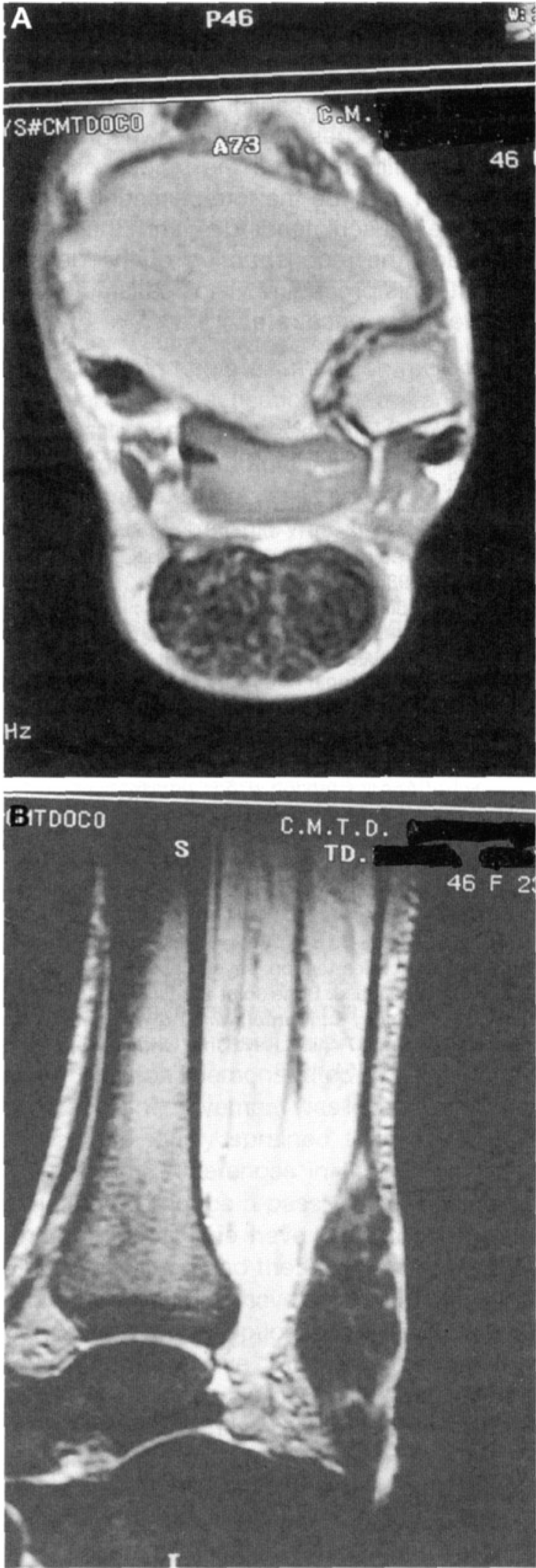
Axial (A) and sagittal (B) magnetic resonance images showing the enlargement of Achilles tendons with areas of sacciform dilations.