
Abstract

Several methods of midtarsal fusion have been described. The dowel technique is useful for in situ fusions and allows limited dissection but requires specialized trephination equipment. 5 Inlay bone grafting can be used for in situ or corrective (realignment) fusions. 2,4,7 Both of these techniques necessitate the harvesting of autogenous bone graft from the iliac crest or other sources, including the proximal tibia, 6 distal tibia, 3 and calcaneus. 1 Joint resurfacing methods allow for corrective or in situ fusions and, when carefully performed, can at times maintain relative joint configuration and minimize bone shortening. 8 In situations where the joint resection is too wide to approximate the surfaces without affecting the adjacent joints or without shortening the ray, or where grafting from a separate site is not desired, the sliding wedge local bone graft method may be used successfully.
TECHNIQUE TIP
Harvesting a bone graft and performing an arthrodesis in this manner accomplishes several goals. A local structural graft obviates donor site morbidity. The piece is contoured without difficulty to fill any created void between the prepared surfaces. An in situ arthrodesis maintains bone length and preserves alignment of adjacent joints. Alteration of alignment can be achieved, if desired, through the prepared joint surfaces.
We will discuss the procedure as performed at the second metatarsocuneiform joint. After satisfactory ankle block anesthesia, a longitudinal incision is made over the involved joint just lateral to the dorsalis pedis artery. The branch of the dorsal medial cutaneous nerve is identified and reflected. The surgeon then palpates for the dorsalis pedis artery and vein and the deep peroneal nerve. A deeper incision is then made down to the bone, at least 2 to 4 mm lateral to the neurovascular bundle, and the small branches that cannot be reflected are cauterized. The incision should permit medial and lateral elevation of the periarticular capsular-periosteal flap. This elevation is facilitated by placing a Freer elevator intracapsularly over the dorsal joint line and using it as a lever to reflect the tissues. Cartilage, scar tissue, and bone are resected until subchondral bleeding is visible. Using a microsagittal saw, two vertical cuts are made in the cuneiform (in length, approximately three-fourths of the bone depth), leaving adequate lateral borders (Fig. 1). A vertical oblique cut is then made with a chisel, starting 45° to the proximal cuneiform base and exiting at a depth similar to that of the lateral cuts. The wedge is then translated distally with a bone tamp to fill the fusion site. This technique requires minimal or no alteration of the adjacent bones or joints. The alignment is then temporarily secured with a Kirschner wire directed from the metatarsal base across the wedge and into the proximal cuneiform base. After confirming position by fluoroscopy, a 3.5- or 4.0-mm screw of appropriate length is used to stabilize the fusion site.
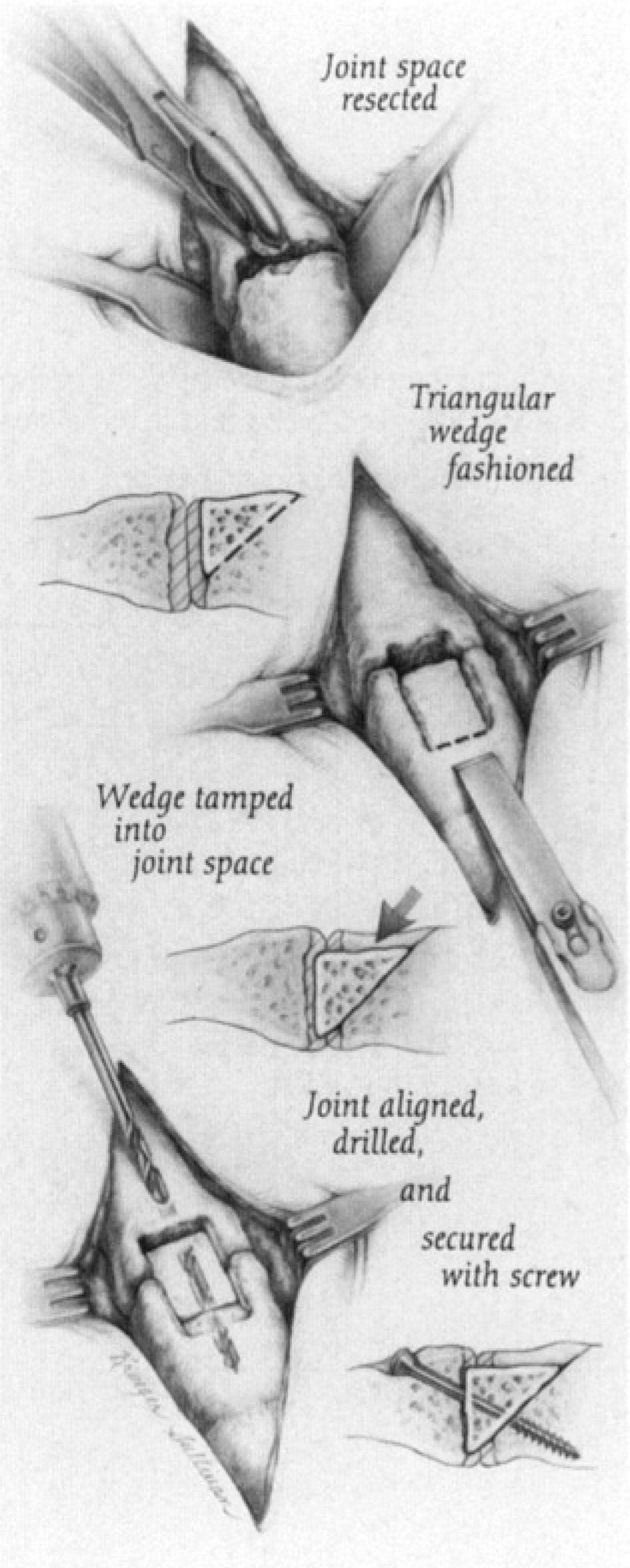
Artist's sketch of technique used for second metatarsocuneiform arthrodesis.
For an isolated fusion, immobilization typically is accomplished with a postoperative shoe, and weightbearing may be permitted on the heel and/or lateral side of the foot. For a more extensive fusion, immobilization with a “U” and posterior splint and/or a boot brace, is indicated, and weightbearing is avoided for 6 weeks. Between 6 and 12 weeks, gradual, progressive weightbearing is allowed, adding 20 lbs every week.
Footnotes
ACKNOWLEDGMENT
The authors wish to thank Lianne Krueger Sullivan for the illustration of this technique.