
Abstract
We report three patients with lateral ankle and foot pain, with the diagnosis of stenosing tenosynovitis of the peroneus longus tendon associated with a markedly enlarged peroneal tubercle. Stenosing tenosynovitis of the peroneus longus tendon associated with an atraumatically enlarged peroneal tubercle has rarely been reported, and these reported cases were associated with an os peroneum. 4,6 One of our patients had no demonstrable associated os peroneum but did have a bony tunnel enveloping the peroneus longus tendon. Our other two patients had an os peroneum, but were asymptomatic at the lateral outer border of the cuboid tunnel; one patient had involvement of the peroneus longus and brevis tendons.
CASE REPORTS
Case 1
A 44-year-old Caucasian man complained of pain on the lateral aspect of the left ankle that had been progressive during the past 3 months. He complained of swelling below his fibula and clicking in the same region. No history of previous trauma was reported.
At physical examination, the patient's gait was antalgic on the left. Swelling, as well as tenderness, was noted in the region of the peroneal tubercle. Pain was associated with resisted eversion of the foot. Subtalar motion was equal to the unaffected extremity. Ankle AP, mortise, and lateral radiographs were normal.
The patient was diagnosed with tenosynovitis of the peroneus longus tendon and was given a trial of immobilization and nonsteroidal anti-inflammatory medication. With no significant improvement noted after 2 weeks of treatment, the peroneal tendon sheath was injected with Celestone and Xylocaine. The patient noted improvement after the injection, but his symptoms recurred 1 month later.
His examination was unchanged. A Harris heel radiographic view was obtained which demonstrated a tunnel-like bony structure on the lateral aspect of the calcaneus at the level of the peroneal tubercle (Fig. 1). AP, lateral, and oblique foot films were normal, and no associated os peroneum was seen. The diagnosis was stenosing tenosynovitis secondary to impingement at the peroneal tubercle.
Surgery was discussed and accepted. Partial tearing and fraying of the peroneus longus tendon was present, and the enlarged peroneal tubercle formed a complete osseous tunnel through which the tendon passed. The tunnel was opened with an osteotome, and the peroneus longus tendon was delivered and retracted from the tubercle. The peroneal tubercle and osseous tunnel were removed with an osteotome. The tendon was inflamed with longitudinal tearing and fraying but was still intact. The damaged part of the tendon was debrided, and tendon borders were oversewn with absorbable suture. The patient was maintained in a nonweightbearing short leg cast for 4 weeks, and then he progressed to full weightbearing in a short leg walking cast. At 6 weeks, immobilization was discontinued. Seven months after excision of his peroneal tubercle, the patient was asymptomatic and had full foot and ankle strength and motion.
Case 2
A 54-year-old Caucasian male silk screen designer for an automotive glass plant sustained a twisting injury to his left ankle while working. Six months after injury, he complained of lateral ankle pain and swelling just anterior and inferior to his lateral malleolus. Neither associated bony trauma nor history of calcaneal fracture was reported.
At physical examination, swelling and tenderness were localized over the peroneal tubercle. Resisted eversion was painful. Passively, subtalar motion was normal and equal to the uninvolved ankle.
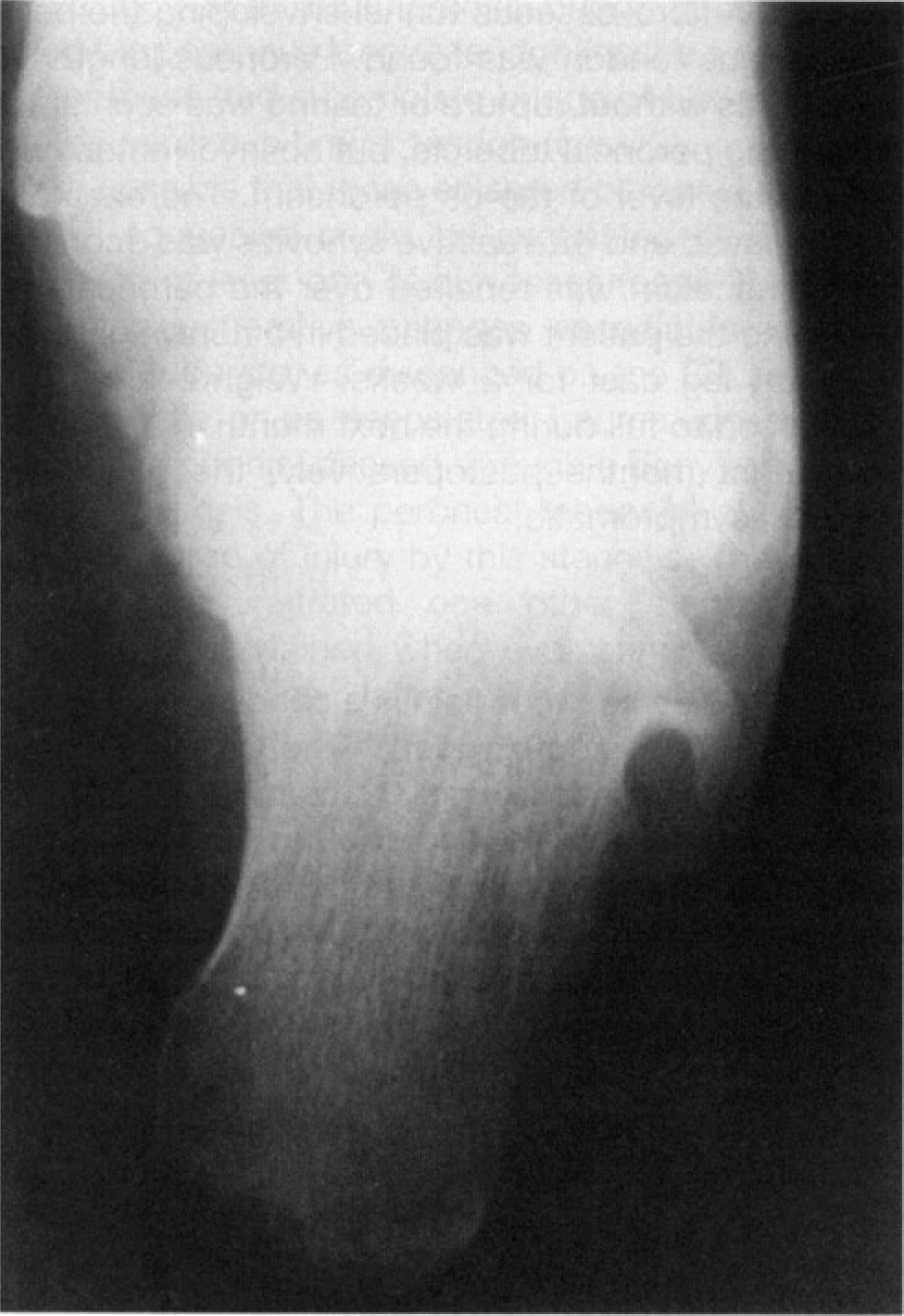
Harris heel radiograph of case 1 showing an enlarged, tunnel-like peroneal tubercle.
AP, mortise, and lateral radiographs demonstrated a spike-like prominence on the lateral calcaneus of his involved ankle and only a small protuberance on his uninvolved ankle. An os peroneum was demonstrated on both feet. The computed tomography (CT) scan of the hindfoot revealed enlargement of his peroneal tubercle with the formation of a near-complete tunnel enveloping both his peroneus longus and brevis tendons (Fig. 2).
The patient was diagnosed with stenosing tenosynovitis of his peroneal tendons. He was treated with a short leg walking cast and nonsteroidal anti-inflammatory medication for 4 weeks. This treatment failed to relieve his symptoms. At surgery, the roof of bone surrounding the peroneus longus and brevis tendons was removed and the tendons retracted. The tendons demonstated chronic inflammatory changes, but no tearing or rupture was seen. The exostosis was removed.

CT scan of the hindfoot in case 2 revealing enlargement of the peroneal tubercle with the formation of a near complete tunnel enveloping the peroneus longus and brevis tendons.
Postoperative management was a nonweightbearing short leg cast for 2 weeks and progressive weightbearing in a short leg ankle immobilizer during the next month. The patient returned to full duty work 5 months after surgery with minimal symptoms and no limp. At 2 1 /2 years postoperatively, the patient remained asymptomatic.
Case 3
A 45-year-old Caucasian woman complained of a 1-month history of right lateral ankle and foot pain with no associated trauma history. The pain and swelling were progressive and confined to the lateral ankle and hindfoot.
At physical examination, she demonstrated tenderness and swelling over the peroneal tendons in the region of the peroneal tubercle. Resisted eversion reproduced her symptoms. Passively, her subtalar motion was normal.
Ankle AP, mortise, and lateral as well as Harris heel radiographs were obtained. The ankle radiographs were normal and demonstrated an os peroneum. The Harris heel view revealed a beak-like projection of the peroneal tubercle (Fig. 3). A CT scan demonstrated a beak-like projection of an enlarged peroneal tubercle (Fig. 4). Stenosing tenosynovitis of the peroneal tendons was the diagnosis, and treatment consisted of immobilization and nonsteroidal anti-inflammatory medication for 3 weeks.

Harris heel radiograph of case 3 demonstrating an enlarged, beak-like projection of the peroneal tubercle.
Failing nonoperative management, the patient elected surgical excision of this enlarged peroneal tubercle. A fibro-osseous tunnel enveloping the peroneus longus tendon was found. Peroneus longus tenosynovitis without rupture or tearing was seen at the level of the peroneal tubercle, but no involvement was seen at the level of the os peroneum. The exostosis was removed and the reactive synovitis was debrided. The retinaculum was repaired over the peroneal tendons, and the patient was placed in a nonweightbearing short leg cast for 2 weeks. Weightbearing was progressed to full during the next month in a short leg cast. Eight months postoperatively, the patient remained asymptomatic.

CT scan of the hindfoot revealing the beak-like projection of the enlarged peroneal tubercle of case 3.
DISCUSSION
Lateral ankle and foot pain is a condition commonly seen by orthopaedic surgeons. The differential diagnosis includes the following: (1) lateral ankle ligament injury, (2) lateral ankle and foot avulsion or stress fractures, (3) subluxation of the peroneal tendons, (4) peroneal tenosynovitis, (5) sural nerve entrapment, (6) painful os peroneum syndrome 6 (encompassing many related os peroneum problems), and (7) intra-articular conditions such as synovitis because of a Bassett's lesion of the talar dome. The obscure diagnosis of stenosing tenosynovitis of the peroneus longus tendon has rarely been reported in the literature, and most of the time it is associated with trauma or calcaneal fracture. 1,5,8 Burman 1 first reported enlargement of the peroneal tubercle as a cause for lateral ankle pain, and he believed that a congenital explanation for this process existed. Trevino et al. 8 reported on stenosing tenosynovitis of the peroneal tendons in four patients, but these cases were either related to trauma or “nonspecific” causes.
Lateral ankle and foot pain caused by osteochondromata involving the peroneal tubercle has been reported. 2,3,7 Rosenberg et al. 5 studied the CT scan evaluation of peroneal tendons in 25 normal ankles and 30 abnormal ankles after trauma; they found variations of the peroneal tubercle that predispose the peroneal tendons to abnormal mechanical stresses. 5 Peirson and Inglis 4 reported one case of stenosing tenosynovitis of the peroneus longus tendon associated with hypertrophy of the peroneal tubercle and an os peroneum. Sobel et al. 6 coined the term “painful os peroneum syndrome” and reported one case of lateral plantar foot pain associated with an enlarged peroneal tubercle and an os peroneum. Sobel et al. also stated that the Harris heel view could be used to demonstrate the presence of an enlarged peroneal tubercle.
The three cases presented in this series had significant stenosing tenosynovitis of the peroneus longus in association with an enlarged peroneal tubercle; two cases showed a circumferential bridge of bone enveloping the peroneus longus tendon (cases 1 and 2), and one of these had a complete bridge of bone enveloping the peroneus brevis tendon (case 2).
It is possible that these enlarged peroneal tubercles have a congenital origin, as suggested by Burman. 1 However, at least one of our cases (case 2) had significant degenerative changes associated with the peroneal tubercle, as evidenced on the CT scan (Fig. 2). With little or no associated trauma, possibly the peroneal tendon(s) passed through a bony tunnel producing stenosis. The peroneal tendon(s) showed an varying degree of injury by this stenosis. These three patients demonstrated one other diagnosis that should be entertained when evaluating lateral ankle and foot pain. The Harris axial heel view is helpful when looking for enlargement of the peroneal tubercle.
READER EXCHANGE
Are you retiring, cleaning your basement, or going on-line? Do you have old copies of Foot & Ankle/Foot & Ankle International or bound volumes? We are willing to try to find appropriate homes for your Journals.
Are you trying to locate old copies of Foot & Ankle/Foot & Ankle International? Here are three addresses that may be of help to you.
Footnotes
ACKNOWLEDGMENT
No grants were received supporting this manuscript.