
Abstract
Klebsiella pneumoniae remains a major cause of invasive infections and is highly capable of acquiring antimicrobial resistance. This exploratory study investigated the antimicrobial resistance profiles and virulence determinants of Klebsiella pneumoniae isolates collected between January and December 2022 at a tertiary-care hospital in Panama City, Panama. A subset of 27 K. pneumoniae isolates was phenotypically and genetically characterized using antimicrobial susceptibility testing. (VITEK® system), 16S rRNA gene sequencing, multilocus sequence typing (MLST), and virulence gene screening. Our results indicated multidrug resistance (MDR) in 52% (14/27) of these isolates. Virulence gene analysis revealed a high prevalence of genes associated with fimbriae 96% (26/27), capsule formation 96% (26/27), lipopolysaccharide synthesis 59% (15/27), and siderophore production 48% (13/27). The MLST of 14 isolates harboring MDR, resistant, and susceptible phenotypes identified known sequence types (ST348, ST111, ST1104, ST6394, ST806, ST45, and ST163), as well as seven novel sequence types (ST6917–ST6923). Phylogenetic analysis based on 16S rRNA sequences confirmed Klebsiella genus identity and proved close genetic relatedness among isolates. No clear association between MDR profiles and sequence types was observed. These findings suggest the uncontrolled widespread of MDR K. pneumoniae strains containing multiple virulence determinants in a high-complexity health care setting in Panama. We urge the need to strengthen antimicrobial stewardship programs and reinforce infection prevention strategies to limit the spread of high-risk clones and preserve antimicrobial efficacy.
Klebsiella pneumoniae (K. pneumoniae) remains the main human pathogen in the community and in the nosocomial setting.1,2 According to the World Health Organization (WHO), K. pneumoniae is a leading cause of health care-associated infections worldwide and is recognized as an opportunistic pathogen that primarily affects hospitalized and immunocompromised patients. It is responsible for a range of severe infections, including pneumonia, septicemia, urinary tract infections, and surgical site infections. Clinical management of K. pneumoniae infections has become increasingly challenging due to rising antimicrobial resistance in both health care and community settings, particularly with the emergence of extended-spectrum β-lactamase (ESBL) production, carbapenemase-producing strains, and hypervirulent lineages. 3
The pathogenicity of K. pneumoniae is mediated by multiple virulence factors that enable evasion of host immune responses and contribute to increased disease severity. Key determinants include lipopolysaccharide, capsular polysaccharide, fimbriae, and siderophore production, which collectively enhance bacterial adherence, colonization, iron acquisition, and resistance to host defenses. The expression of these virulence traits, particularly capsule-associated hypermucoviscosity, is associated with heightened virulence and more severe clinical outcomes. 4 Studies show a positive correlation between virulence and antimicrobial resistance genes among K. pneumoniae, with fimbriae factors in 90% of tested isolates. 5 In New York City, the presence of multiple hypervirulent and multidrug resistant (MDR) K. pneumoniae strains increases the relative mortality rate of patients with hepatobiliary disease and diabetes from 19.0% to 29.4%. Consequently, the combination of virulence factors and resistance poses major challenges in hospital settings. 6
Clinical and molecular epidemiology of K. pneumoniae infections has been a subject of studies at a global level. The prevalence of resistance to carbapenems remains in a rising trend, including United States (10.3–58.5%), Latin America (1.3–20%) and Europe (0.2–59%). 7 A recent multicenter study of K. pneumoniae in the Caribbean showed not only carbapenem resistance but also hypervirulent strains. 8 As well as in Jamaica reported a low prevalence of AmpC BL among E. coli and K. pneumoniae, as common urinary pathogens. 9 In Brazil, carbapenem-resistant K. pneumoniae exhibited high mortality rates (36%) in pediatric patients. 10
Limited information remains available about the health burden of infections by K. pneumoniae from patients in Panama. We previously reported an analysis of K. pneumoniae subsp. ozaenae clinical isolates with high resistance levels to antibiotics, including carbapenems, and expressing mechanisms such as ESBL, KPC, and NDM. The presence of these isolates in the hospital setting was involved in the death of nearly 90% (10/11) of patients. 11 Other study in the central region of Panama allowed identified a high-risk emerging clone (ST307) and alerted for potential difficulties in managing K. pneumoniae infections. 12 In this current study, we aim to examine the antimicrobial susceptibility, molecular, and virulence factors of K. pneumoniae strains recovered from inpatients at a tertiary hospital in Panama.
From January to December 2022, a total of 1,425 isolates belonging to the genus Klebsiella were reported at the hospital clinical laboratory as part of the routine standard of care for patients with infections at Complejo Hospitalario Metropolitano Dr. Arnulfo Arias Madrid-Caja de Seguro Social (CHMDrAAM-CSS) in Panama. The species identification procedures yielded 1,067 isolates of K. pneumoniae, 187 K. pneumoniae subsp. ozaenae, 73 K. aerogenes, and 31 K. oxytoca isolates. The overall resistance profiles of K. pneumoniae isolates for each antibiotic were tested (Fig. 1).
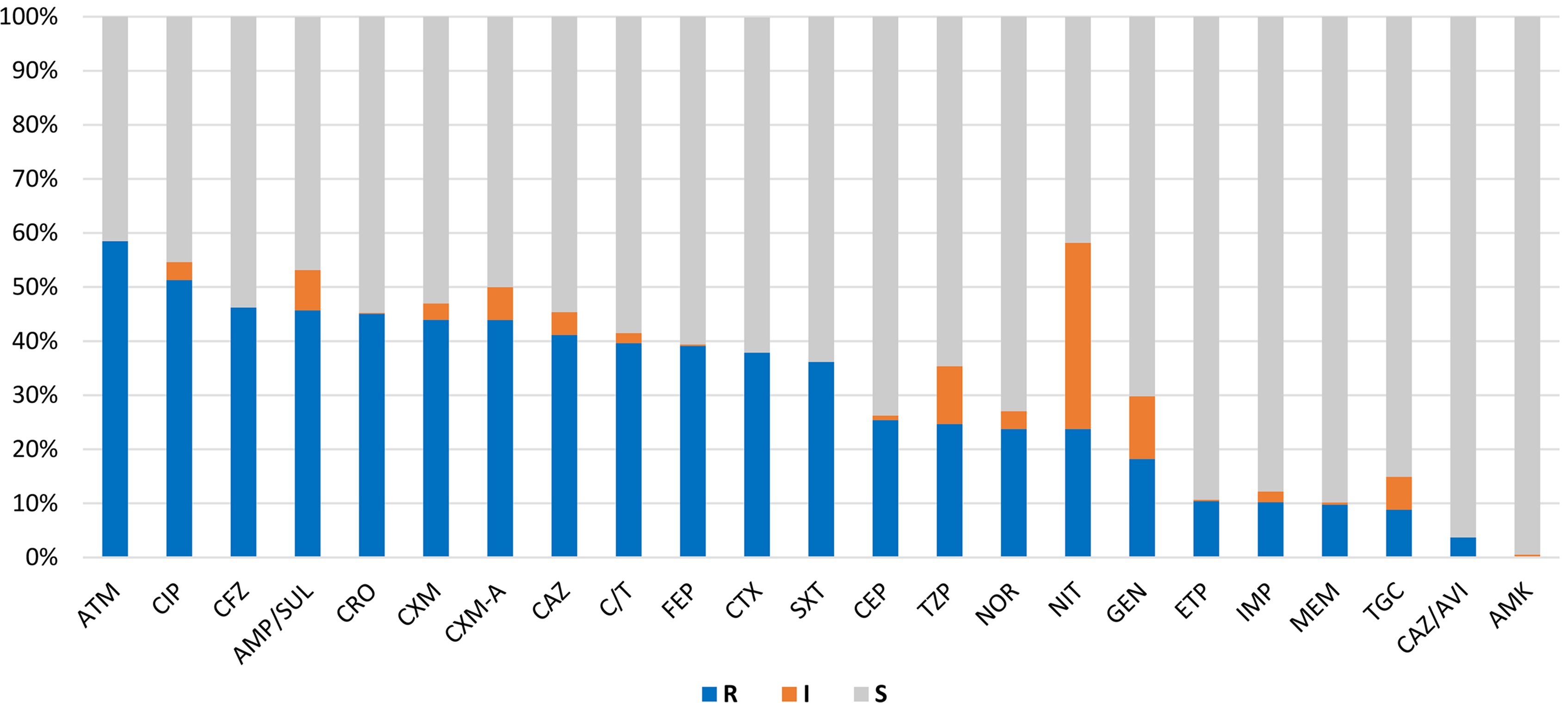
Antimicrobial resistance rates of 1067 K. pneumoniae isolates. AMK, amikacin; AMP/SUL, ampicillin/sulbactam; ATM, aztreonam; C/T, ceftolozane/tazobactam; CAZ, ceftazidime; CAZ/AVI, ceftazidime/avibactam; CEP, cephalothin; CFZ, cefazolin; CIP, ciprofloxacin; CRO, ceftriaxone; CTX, cefotaxime; CXM, cefuroxime; CXM-A, cefuroxime axetil; ETP, ertapenem; FEP, cefepime; GEN, gentamicin; I, intermediate; IMP, imipenem; MEM, meropenem; NIT, nitrofurantoin; NOR, norfloxacin; R, resistance; S, sensitive; SXT, trimethoprim-sulfamethoxazole; TGC, tigecycline; TZP, piperacillin-tazobactam.
An exploration study was conducted in which a subset of K. pneumoniae isolates was selected from the hospital microbiology laboratory database. A total of 27 isolates, representing 2.5% (27/1,067) of all K. pneumoniae isolates recovered during the study period, were randomly selected to ensure representation of diverse antimicrobial resistance phenotypes. Isolates were obtained from clinically significant specimens, including urine, endotracheal secretions, blood, and pleural effusion. K. pneumoniae isolates were analyzed using a combination of phenotypic and molecular approaches to generate baseline data on antimicrobial resistance and virulence characteristics (Table 1).
Microbiological Characteristics of 27 Klebsiella pneumoniae Isolates
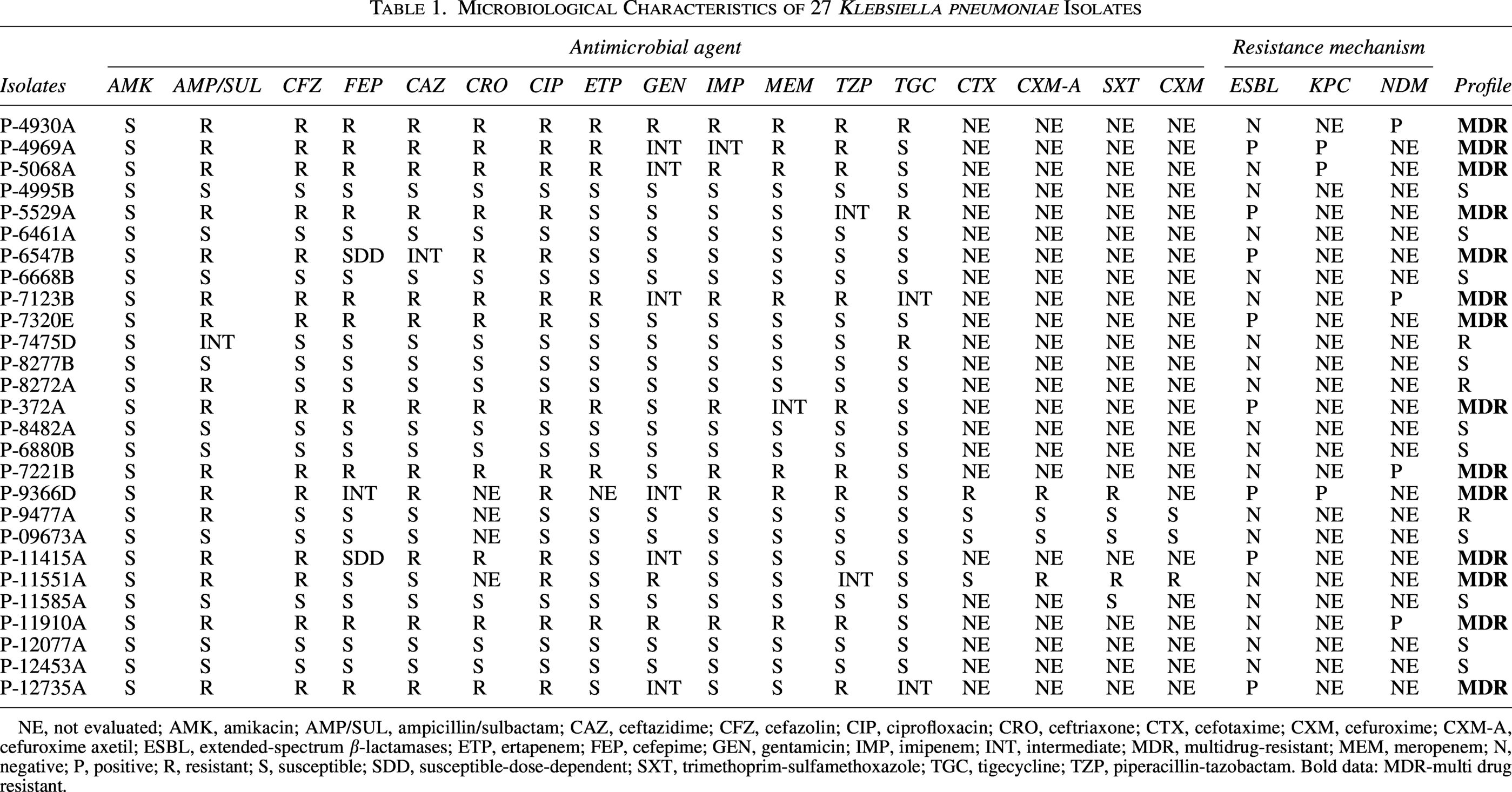
NE, not evaluated; AMK, amikacin; AMP/SUL, ampicillin/sulbactam; CAZ, ceftazidime; CFZ, cefazolin; CIP, ciprofloxacin; CRO, ceftriaxone; CTX, cefotaxime; CXM, cefuroxime; CXM-A, cefuroxime axetil; ESBL, extended-spectrum β-lactamases; ETP, ertapenem; FEP, cefepime; GEN, gentamicin; IMP, imipenem; INT, intermediate; MDR, multidrug-resistant; MEM, meropenem; N, negative; P, positive; R, resistant; S, susceptible; SDD, susceptible-dose-dependent; SXT, trimethoprim-sulfamethoxazole; TGC, tigecycline; TZP, piperacillin-tazobactam. Bold data: MDR-multi drug resistant.
All 27 K. pneumoniae isolates included in this study were collected as part of routine clinical diagnostics in the hospital’s clinical microbiology laboratory. Antimicrobial susceptibility testing was performed using the automated VITEK® 2 AST Compact system (Cat—N250, BioMerieux, Spain), the same procedure as the susceptibility tests described in Figure 1. Phenotypic antimicrobial susceptibility was determined against 24 antimicrobial agents according to M39 guideline (CLSI, 2022, 5th edition) (Table 1). We also investigated the presence of carbapenem resistance using Xpert Carba-R (Cat. GXCARBAR-CE-10, Cepheid, USA) to determine the most prevalent carbapenemase families, including New Delhi metallo-β-lactamase (NDM), imipenemase (IMP), Verona integron-encoded metallo-β-lactamase (VIM), Oxacillinase-48 (OXA-48), and K. pneumoniae carbapenemase (KPC).The consensus to define the grade of resistance (R) categorize and notify multidrug-resistant, extensively drug-resistant, or pandrug-resistant bacteria was applied according to standard definitions for acquired resistance. 13
DNA extraction from 27 K. pneumoniae isolates was done using the conventional cetyltrimethylammonium bromide method previously described by Van Soolingen et al. 14 Resistance genes were determined using specific set primers to quinolones [aac(6’)-Ib-cr, qnrB], aminoglycosides (aadb), and sulfonamides (sul1 and sul2), as described previously.4,15 Furthermore, we explored virulence genes associated with fimbriae (fimD, fimH, and mrkD), capsule-associated genes (ycfM and wabG), siderophores (entB, iucA, and irp2), colibactin genes (clbA) and capsular serotypes (K1 and K2) genes. 16 The PCR products were analyzed by gel electrophoresis (2.5% agarose gel) and visualized using ChemiDoc Image System (Bio-Rad, USA).
DNA sequencing of the 16S rRNA gene was performed on a subset of 14 K. pneumoniae isolates to confirm species identification previously obtained using the VITEK® 2 automated system. 17 This subset was selected with an emphasis on antimicrobial resistance profiles, reflecting the clinical complexity of hospital management. This subset included 10 multidrug-resistant (MDR), two resistant, and two susceptible K. pneumoniae isolates (Table 1). Genetic relationships were assessed by sequencing the 16S rRNA gene using universal primers 337 F and 1100 R, as specified in the Macrogen primer list (Macrogen Inc., South Korea). Resulting sequences were compared with reference K. pneumoniae strains from the ATCC database. The remaining four MDR isolates had low DNA quantity and quality; therefore, we were only able to analyze those ten MDR isolates. This molecular typing was performed to complement bacterial identification using the NCBI database and to evaluate the genetic relatedness among MDR K. pneumoniae isolates through phylogenetic analysis. Additionally, molecular typing was performed using multilocus sequence typing (MLST) 18 (Macrogen Inc.; Seoul, Korea). MLST profiles and allelic definitions were analyzed using the BIGSdb-Pasteur database (https://bigsdb.pasteur.fr/) for the K. pneumoniae complex.
Our results show a total of 1,067 K. pneumoniae isolates recovered during the study period, predominantly from blood 36% (388/1,067), urine 28% (300/1,067), and respiratory secretions 25%; (260/1,067). Antimicrobial susceptibility data were not uniformly available for all isolates, resulting in variable denominators across antibiotic classes. Among isolates with available resistance data, elevated resistance rates were observed for aztreonam 58% (31/53) and ampicillin/sulbactam 47% (18/38). Resistance to cephalosporins was also frequent, including cefazolin 46.2% (335/725) and ceftazidime 41.3% (320/778). Within the carbapenem class, resistance was detected for ertapenem 10.4% (81/778), imipenem 10.2% (65/656), and meropenem 9.8% (76/776), whereas resistance to amikacin remained low at 0.5% (1/778) (Fig. 1). Molecular data available for the full collection indicated a high prevalence of ESBL and carbapenemase-associated genes, with bla_CTX-M detected in a substantial proportion of isolates. Carbapenemase genes included bla_KPC 48% (512/1,067), bla_NDM 34% (363/1,067), and the combined presence of bla_KPC and bla_NDM 3% (28/1,067).
An exploratory subset of 27 K. pneumoniae isolates was analyzed. Of these, 63% (17/27) were recovered from male patients and 37% (10/27) from female patients, with the majority, 81% (22/27), derived from individuals aged 57–88 years. The most frequent clinical specimens were urine in 33% (9/27), endotracheal secretions 30% (8/27), and sputum 27% (7/27) (Table 1). Antimicrobial susceptibility testing showed the highest rate of susceptibility to ampicillin/sulbactam 59% (16/27). Resistance mechanisms included ESBL production in 26% (7/27), NDM in 15% (4/27), and KPC in 11% (3/27) of isolates. Genes conferring quinolone resistance were also detected, including aac(6′)-Ib-cr in 30% (8/27) and qnrB in 41% (11/27). Additional resistance determinants included aadB associated with aminoglycoside resistance (7%) and sul1 linked to sulfonamide resistance (37%).
The presence of virulence genes was determined (Fig. 2). The fimbriae genes fimD and fimH were present in 96% (26/27) of the strains, and for mrkD and ycfM genes 93% (25/27) were found in almost all strains, while the numbers varied for the other genes entB 83% (22/27), iucA 3% (1/27), irp2 60% (16/27), and wabG 52% (14/27). The clbA gen was not found in the strains tested. The K1 capsular serotype was determined in only two strains. When we focus only on MDR isolates, we found a similar proportion including, fimbriae 93% (25/27) for all genes fimD, fimH, mrkD, capsule-associated genes ycfM 93% (25/27), wabG 59% (16/27) and siderophores entB 81% (22/27), irp2 55% (15/27) and capsular serotypes with K1 7% (2/27). Only one MDR isolate (P-9366) did not show the presence of any of the genes analyzed.
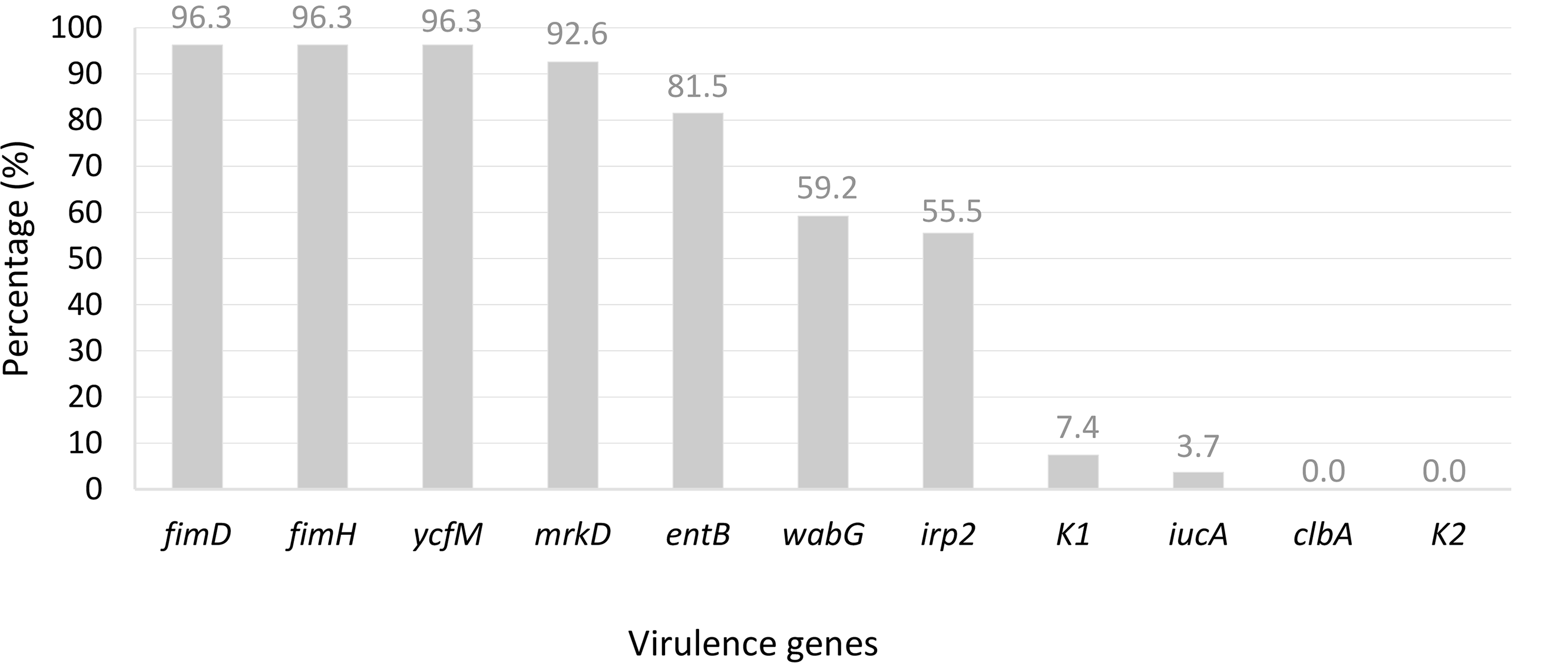
Percentage of virulence genes detected in 27 K. pneumoniae isolates. Overall virulence genes were represented in percentage. All strains in which the respective gene is not present are assigned to “not detected”. Fimbriae genes (fimD, fimH, mrkD); capsule (ycfM, wabG); siderophores (entB, irp2, icuA); capsular serotypes (K1, K2); colibactin (clbA). 4
We confirmed the taxa of K. pneumoniae with 100% sequence similarity with the reference from the NCBI database. MLST typing of these 14 K. pneumoniae isolates showed heterogenous clonal distribution and seven new ST types (ST6917–ST6923) were assigned and deposited in the Pasteur Institute MLST database https://bigsdb.pasteur.fr/ with registration ID numbers 58913–58919, Table 2.
MLST Of Selected Klebsiella pneumoniae Isolates
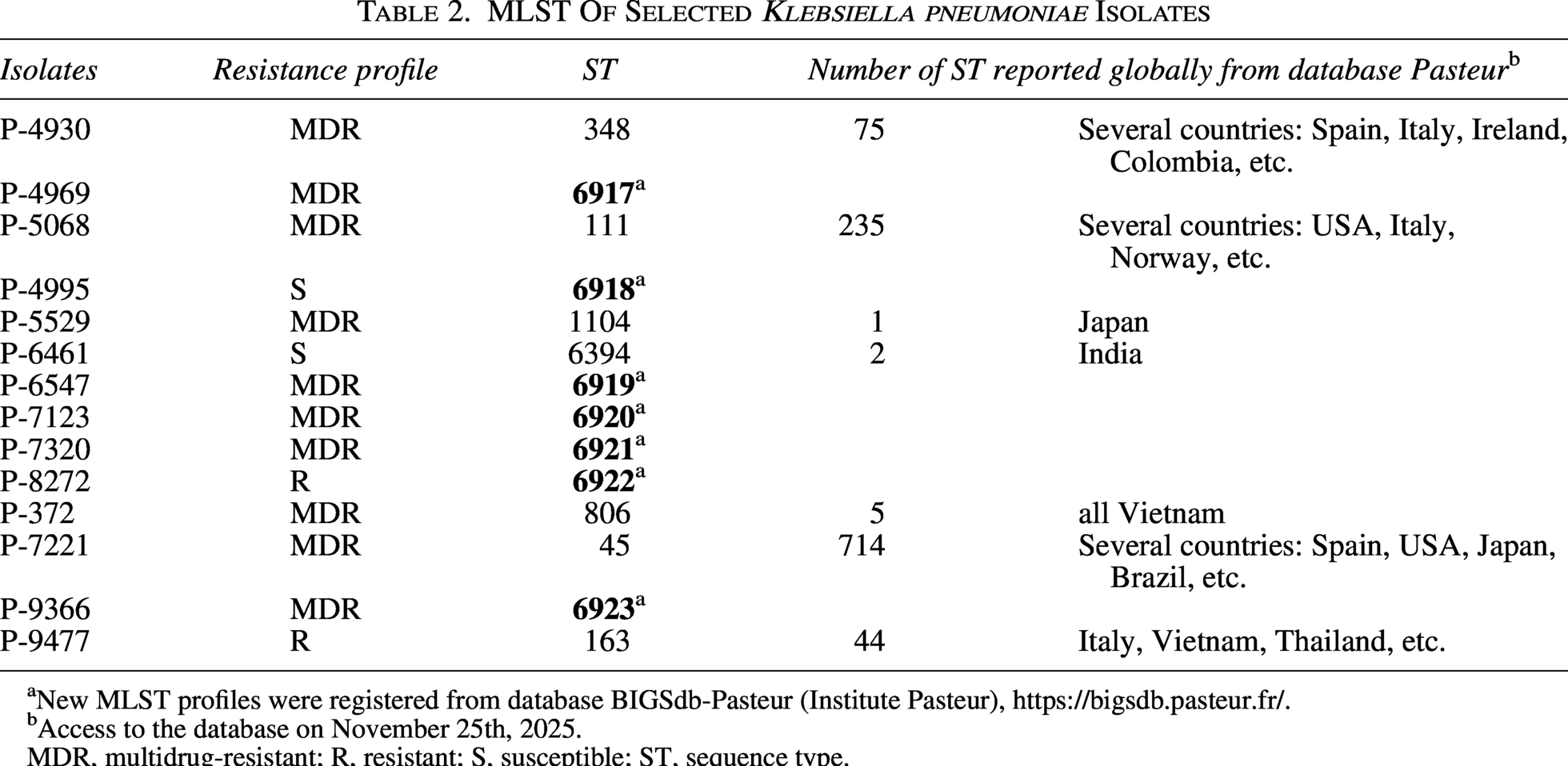
New MLST profiles were registered from database BIGSdb-Pasteur (Institute Pasteur), https://bigsdb.pasteur.fr/.
Access to the database on November 25th, 2025.
MDR, multidrug-resistant; R, resistant; S, susceptible; ST, sequence type.
In this study, a high prevalence of antimicrobial resistance was observed among the 1,067 K. pneumoniae isolates analyzed. This finding is consistent with previous reports from tertiary-care hospitals, where up to 90% of MDR organisms causing health care-associated infections exhibited resistance to commonly used β-lactam antibiotics, including ampicillin, amoxicillin, ceftriaxone, and cefuroxime. 19 Such patterns reflect the well-recognized capacity of K. pneumoniae to rapidly acquire and accumulate resistance determinants, contributing to its prominence as a high-risk MDR pathogen in hospital settings.
In our exploratory subset of 27 K. pneumoniae isolates, our analysis revealed substantial diversity in antimicrobial resistance profiles, virulence gene content, key β-lactamase determinants, and MLST profiles. Notably, approximately half of the isolates met the criteria for MDR, as defined by established classification standards. Although the limited number of isolates, this rapid screening alerts us to the presence of high-risk strains in the nosocomial setting. The anatomical origin of clinical isolates, together with their associated molecular characteristics, may serve as a proxy for infection severity. For example, Zhao et al., isolated carbapenem hypervirulence K. pneumoniae from surgery and pulmonary specimens which resulted in total mortality of the cases; the patient deaths were attributed to complications arising from clone CR-hvKP infections. 16 In fact, infections caused by multidrug-resistant or highly virulent bacteria are associated with increased mortality and prolonged hospital stays, resulting in substantial economic burden, with costs related to antibacterial therapy rising by up to two-thirds. 20
In this exploratory subset, resistance genes associated with quinolones, aminoglycosides, and sulfonamides were detected. These genetic determinants remain a robust indicator of antimicrobial resistance in this hospital and could facilitate the rapid emergence and dissemination of resistance among other bacterial populations. Thus, we urge the implementation of sustained and effective antimicrobial stewardship programs (ASPs) to mitigate selective pressure, limit resistance spread and optimize antibiotic use. 21 The correct use of antibiotics in the clinical management of hospitalized patients suffering chronic diseases will aid in preventing the emergence of resistance.
We also found a high diversity of virulent genes among K. pneumoniae isolates. Most of the isolates had genes for fimbriae and capsule, lipopolysaccharides, and for siderophores (Fig. 2). The fimH gen fimbriae encodes the end of the fimbria that connects to the capsule and facilitates adhesion to the cell, that is, adhesion to the urinary tract. These virulence genes have been detected in nearly all K. pneumoniae isolates from clinical samples including urine, sputum, and blood. Our data suggest a similar and positive correlation between virulence and antimicrobial resistance genes among K. pneumoniae, which could contribute to the adaptation of the pathogen. 5
The virulence determinants found here are consistent with previous studies reporting that K. pneumoniae clinical strains were producers of virulence factors. 15 Analysis of capsular determinants revealed the presence of the ycfM gene, associated with capsule production and the K1 capsular serotype, while no evidence of the K2 capsular serotype was detected in the isolates examined. In addition, we observed irp2 gene, encoding parts of the siderophore system for iron acquisition and conferring hypermucoviscosity. Although we only determined the presence of the K1 capsular serotype in two isolates, this suggests the presence of hypervirulent isolates with hypermucoviscosity which is associated with invasive infections and high resistance. We also identified virulence genes in both MDR and susceptible isolates. Although some strains are susceptible to antibiotics, they carry genes that may enhance their capacity to cause severe infections. 5 The presence of mobile genetic elements in these isolates may facilitate the dissemination of not only antimicrobial resistance genes but also virulence factors. From a public health perspective, the increasing coexistence of these traits is particularly concerning, as it could lead to difficult-to-treat or untreatable K. pneumoniae infections.
MLST typing showed heterogeneity STs of MDR isolates (Table 2), just one strain (ST6922) had resistance to ampicillin/sulbactam, and another one was sensitive (ST6918). According to the MLST database (https://bigsdb.pasteur.fr/), ST45 is the one that has been reported the most globally, including in Spain, the United States, and Japan, while ST1104 is a rare lineage that has only been isolated in Japan, and ST6359 has only been identified in India. 2 The ST45 variant was implicated in an outbreak in a pediatric unit in Italy and China, which involved the clonal spread of K. pneumoniae with production of ESBL.3,22 In turn, ST111 is a genotype present worldwide and has been reported in healthy animals with characteristic virulence genes and drug resistance. A new ST6917 strain isolated in this study showed an MDR profile associated with ESBL and KPC, suggesting a high capacity to acquire resistance to carbapenems and cephalosporins. This finding, the high genetic diversity or not clonal profile among the isolates suggests their endogenous origin as in another. 23
This study is limited by the relatively small number of isolates analyzed and by its focus on MDR K. pneumoniae strains selected for genetic characterization. As a result, the findings may not be fully generalizable to the broader K. pneumoniae population circulating in different clinical settings or geographic regions. Second, as this was an anonymized study, we focused exclusively on the resistance and virulence mechanisms of the bacteria; patient clinical records were not available. As a result, we were unable to correlate bacterial genotypes with patient outcomes or clinical severity. Nevertheless, this study provides valuable baseline information on the genotypic diversity, resistance profiles, and virulence factors of K. pneumoniae isolates circulating within this hospital setting and underscores the need for expanded genomic surveillance studies with larger sample sizes.
In summary, this exploratory study reveals a high genetic variability among K. pneumoniae isolates with resistance patterns. This finding alerts the presence of high-risk strains in the hospital setting. Also, they are prone to the appearance of diverse clones that acquire resistance and with the remarkable presence of virulent factors associated with fimbriae, capsule, siderophores and lipopolysaccharide genes in nosocomial infections. We recommend increasing the number of K. pneumoniae clinical isolates (from multicenter or national sources) to enable genotyping of circulating strains and to assess the correlation between virulence genes and antimicrobial resistance. Finally, reinforcing hospital biosafety measures to prevent the arrival of MDR K. pneumoniae with higher proportions of virulent gene profiles. Together with the expansion of an antimicrobial stewardship program will aid to avoid the activation of other resistant genes and mechanisms among these MDR K. pneumoniae.
Authors’ Contributions
S.V.: Project administration, formal analysis, data curation, writing—original draft, and writing—review and editing. F.A.: Formal analysis, data curation, validation, funding acquisition, and writing—review and editing. J.G.: Conceptualization, methodology, investigation, and writing—review and editing. M.M.: Methodology, validation, investigation, data curation, and writing—review and editing. A.G.: Resources, writing—original draft, writing—review and editing, supervision, and investigation.
Data Availability Statement
The authors confirm that all the data in this study are available in the main article and supplementary materials.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
The authors declare they have not used artificial intelligence (AI) tools in the creation of this article.
Ethics Approval of Research
Bacterial strains were previously obtained as part of standard care in Panama. The authors analyzed an anonymized bacterial strain collection. This information was anonymized by hospital laboratory staff who worked independently from the author team. No patient data was obtained for this study.
Footnotes
Acknowledgments
The authors would like to acknowledge the support of the nurses, physicians and laboratory staff of CHMDrAAM-CSS involved in the diagnosis and management of the patients where these strains were obtained. The authors thank Colleen Goodridge and Simone Simionatto for their critical review of this article and valuable suggestions. Also, we thank the Institute Pasteur teams for the curation and maintenance of BIGSdb-Pasteur databases at ![]()
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
SV, FA, and AG were supported by the Sistema Nacional de Investigación (SNI) of the Secretaría Nacional de Ciencia, Tecnología e Innovación (SENACYT) of Panama.