
Abstract
Objective:
The prevalence of carbapenem-resistant Acinetobacter baumannii (CRAb) has been increasing globally. This study aimed to investigate the risk factors, resistance gene profiles, and molecular epidemiology of CRAb bloodstream infections (BSIs) among patients in Xi’an, China, to provide evidence for clinical prevention and targeted treatment.
Methods:
We conducted a retrospective study of 139 patients with A. baumannii BSIs. Patients were categorized into a CRAb group (n = 84) and a carbapenem-susceptible A. baumannii (CSAb) group (n = 55). Independent risk factors were identified via multivariate logistic regression analysis. Carbapenemase resistance genes were detected using polymerase chain reaction (PCR), and CRAb isolates were molecularly typed by multilocus sequence typing (MLST).
Results:
Multivariate logistic regression analysis identified the following as independent risk factors for CRAb BSIs: inappropriate empirical antimicrobial therapy (OR = 8.620; 95% CI: 2.078–35.751), deep venous catheterization (OR = 12.625; 95% CI: 2.263–70.429), prolonged hospitalization before the onset of BSIs (OR = 1.467; 95% CI: 1.123–1.915), and ICU admission (OR = 4.981; 95% CI: 1.898–13.065). Antimicrobial susceptibility testing showed that CRAb isolates were multidrug-resistant, exhibiting resistance rates exceeding 70% to most common clinical antibiotics, with the exception of tigecycline (5.95% resistance) and colistin (27.38% resistance). All 84 CRAb isolates carried both blaOXA-51-like and blaOXA-23-like genes, while other carbapenemase genes were not detected. MLST identified 7 sequence types (STs), with ST540 (45.24%, 38/84) being the dominant clone. eBURST analysis indicated that the major STs (ST195, ST208, etc.) belonged to the same clonal complex.
Conclusion:
Inappropriate empirical antimicrobial therapy, deep venous catheterization, prolonged hospitalization before the onset of BSIs and ICU admission are independent risk factors for CRAb BSIs. The prevalent strains produce OXA-23-like carbapenemase, and molecular typing indicates that the ST540 clone and its related clonal complex are predominant, suggesting potential nosocomial clonal spread.
Introduction
Acinetobacter baumannii (A. baumannii) is a non-fermenting, aerobic, Gram-negative coccobacillus. It is highly adaptable to the environment, can persist for long periods, and is frequently isolated from hospital surfaces and colonized patients. 1 A. baumannii is a major pathogen causing various hospital-acquired infections, including ventilator-associated pneumonia, bloodstream infections (BSIs), urinary tract infections, and skin/soft tissue infections. 2 Globally, A. baumannii accounts for approximately 2% of all health care-associated infections, 3 and this proportion rises to 4% in Asia and the Middle East.4–6 The extensive overuse of broad-spectrum antibiotics has led to increasing drug resistance, particularly concerning the rising prevalence of carbapenem-resistant A. baumannii (CRAb). 7 A global study encompassing 46 hospitals reported a 30-day mortality rate of 24% for CRAb infections, underscoring its status as a serious public health threat. 8 Carbapenem antibiotics (e.g., imipenem, meropenem) are often considered the last-line agents for multidrug-resistant Gram-negative bacterial infections. The emergence of CRAb severely limits treatment options and significantly increases patient mortality.4,9
Among hospitalized patients, CRAb most commonly causes respiratory tract infections and BSIs. CRAb BSIs are associated with mortality rates exceeding 40%. 10 The multidrug-resistant nature of CRAb and the scarcity of effective therapeutic regimens contribute to the high incidence and mortality rates of CRAb BSIs, making them a critical clinical challenge. The resistance mechanisms of CRAb are complex, with the production of carbapenemases being the primary molecular mechanism conferring resistance to carbapenems.7,11 Carbapenemases hydrolyze the β-lactam ring of carbapenem antibiotics, thereby inactivating them. The genotypes of carbapenemase genes carried by prevalent CRAb strains vary significantly across different regions and hospitals. For instance, the OXA-23 type is dominant in East Asia, while NDM-1, OXA-237 or OXA-48 types are more frequently detected in some Western countries. 12 Therefore, identifying the types of carbapenemase genes in CRAb strains is crucial for elucidating their resistance mechanisms and guiding precise clinical therapy or antimicrobial selection.
Multilocus sequence typing (MLST) is a DNA sequence-based molecular typing technique. It relies on sequencing the core fragments of multiple housekeeping genes and assigns sequence types (STs) based on sequence differences, thereby elucidating the genetic evolutionary relationships, epidemic clonal lineages, and transmission routes of bacterial strains. 13 Applying MLST to CRAb studies helps identify predominant local clones, trace the origin and spread of infection outbreaks, and provide key insights into the epidemiology and transmission risk of resistant strains within a region. 14
This study aimed to investigate the risk factors for CRAb BSIs in hospitalized patients in Shaanxi Province, China. We also aimed to characterize the carbapenemase gene profiles of CRAb isolates using polymerase chain reaction (PCR) and sequencing, and to analyze their genetic diversity and prevalent clonal characteristics through MLST. The findings will provide data to clarify the molecular resistance mechanisms and genetic background of CRAb in this region, offering a scientific basis for precision clinical treatment, hospital infection control, and the containment of resistance spread.
Materials and Methods
Study design
This single-center retrospective study was conducted at Shaanxi Provincial People’s Hospital. We collected clinical data from hospitalized patients with A. baumannii BSIs between January 2020 and December 2024. Inclusion criteria were: (1) At least one positive blood culture for A. baumannii obtained ≥ 48 hours after admission, and the bloodstream infection was considered primary, not secondary to an infection at another site; (2) Presence of clinical signs and symptoms indicative of infection, meeting the diagnostic criteria for bloodstream infection with evidence of systemic inflammatory response syndrome; (3) For CRAb group inclusion, the isolate had to be resistant to at least one of the following carbapenems: meropenem, imipenem according to CLSI breakpoints; (4) Age ≥ 18 years; and (5) Complete clinical data availability. Exclusion criteria included: (1) Missing clinical data; (2) Duplicate isolates from the same site in consecutive samples from the same patient; (3) Polymicrobial BSIs; (4) Improper preservation of bacterial isolates. All cases were diagnosed based on microbiological culture, biochemical tests, PCR, and clinical assessment. The study was conducted in accordance with the Declaration of Helsinki and Chinese ethical standards. All participants provided written informed consent prior to participation. All procedures were designed to minimize risks to patient privacy, and there were no commercial conflicts of interest existed.
Bacterial identification and antimicrobial susceptibility testing
Clinical specimens were transported to the microbiology laboratory promptly and inoculated for culture under aseptic conditions within 2 hours. Specimen collection, inoculation, and culture were performed following the standards and operational procedures established by the Clinical and Laboratory Standards Institute (CLSI) M100-S34 (2024) document. 15 Antimicrobial susceptibility testing (AST) was performed using the BD Phoenix M50 automated microbiology system (Becton Dickinson, USA) with its corresponding AST panels. For colistin testing, all isolates with automated minimum inhibitory concentration (MIC) results ≥ 2 mg/L were further verified by the broth microdilution method (BMD), the gold standard recommended by CLSI M07 and EUCAST. The clinical breakpoints for colistin were interpreted according to CLSI guidelines: MIC ≤ 2 mg/L was classified as intermediate, and MIC ≥ 4 mg/L as resistant. Quality control strains included Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853. MIC results were only accepted if they fell within the CLSI-defined ranges for the quality control strains. Tests were repeated if deviations exceeding 10% were observed. The BD Phoenix™ instrument and mass spectrometer (used for bacterial identification) were calibrated monthly according to the manufacturer’s guidelines.
Phenotypic screening for carbapenemase production
Carbapenemase production was detected using the simplified carbapenem inactivation method (sCIM). 16 Briefly, E. coli ATCC 25922 was adjusted to a 0.5 McFarland standard in sterile saline and diluted 1:10. This suspension was swabbed onto Mueller-Hinton agar plates and allowed to dry for 3–10 minutes. Fresh colonies (1–3) from an overnight blood agar plate were smeared onto an imipenem disc (10 μg; Oxoid). This inoculated disc was then placed, smear-side down, onto the pre-inoculated Mueller-Hinton agar plates alongside an uninoculated imipenem disc as a control. Plates were incubated overnight at 35°C. A positive result for carbapenemase production was indicated by an inhibition zone diameter of ≤ 20 mm around the test disc, or the presence of satellite growth of E. coli ATCC 25922 around the disc. An inhibition zone ≥ 26 mm was considered negative, and a zone of 21–25 mm was classified as indeterminate for carbapenemase production.
Based on the carbapenem susceptibility results, patients were categorized into either the CRAb group or the carbapenem-susceptible A. baumannii (CSAb) group.
Detection of carbapenemase genes by PCR
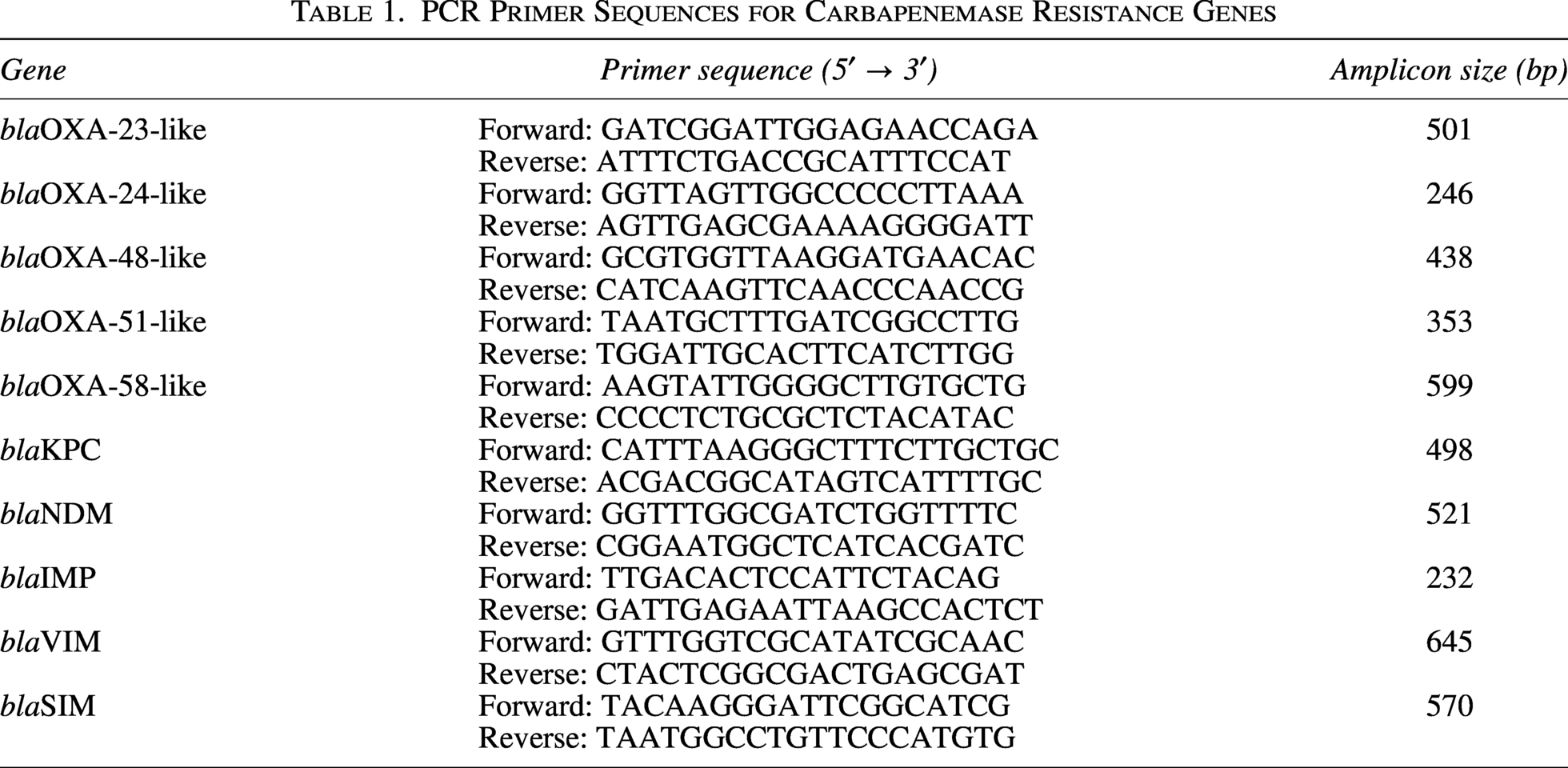
Bacterial DNA was extracted using the boiling method. Briefly, several fresh colonies were suspended in 200 μL of nuclease-free water, heated at 100°C for 10 minutes, followed by centrifugation at 12,000 × g for 5 minutes. The supernatant containing DNA was collected. Nanodrop 2000 spectrophotometer (Thermo Fisher Scientific, USA) was used to evaluate the quality and concentration of DNA. Only samples with A260/A280 ratio between 1.8 and 2.0 were used for subsequent PCR amplification. No amplification failures were observed during the study, indicating that the boiling method provided sufficient DNA quality for PCR detection. Primer sequences for OXA-type carbapenemase genes (blaOXA-23-like, blaOXA-24-like, blaOXA-48-like, blaOXA-51-like, blaOXA-58-like) or non-OXA-type carbapenemase genes (blaKPC, blaNDM, blaIMP, blaVIM, blaSIM) were synthesized based on previously published sequences17,18 (see Table 1).
PCR Primer Sequences for Carbapenemase Resistance Genes
PCR reaction mixture
The 50 μL PCR mixture contained 25 μL of 2× Taq PCR MasterMix (includes Taq DNA polymerase, dNTPs, MgCl2, and reaction buffer), 1 μL of each forward and reverse primer, 2 μL of DNA template, and nuclease-free water to bring the total volume to 50 μL.
PCR amplification conditions
The amplification protocol consisted of an initial denaturation at 94°C for 5 minutes; followed by 35 cycles of denaturation at 94°C for 25 seconds, annealing at 52°C for 40 seconds, and extension at 72°C for 50 seconds; with a final extension at 72°C for 6 minutes.
Product analysis
PCR amplicons were separated by 1.5% agarose gel electrophoresis (110 V, 35 minutes), visualized using a gel imaging system, and positive amplification products were purified and sequenced. The resulting sequences were compared with known sequences in the NCBI database using BLAST analysis. This study did not generate any new nucleotide or amino acid sequence data.
MLST
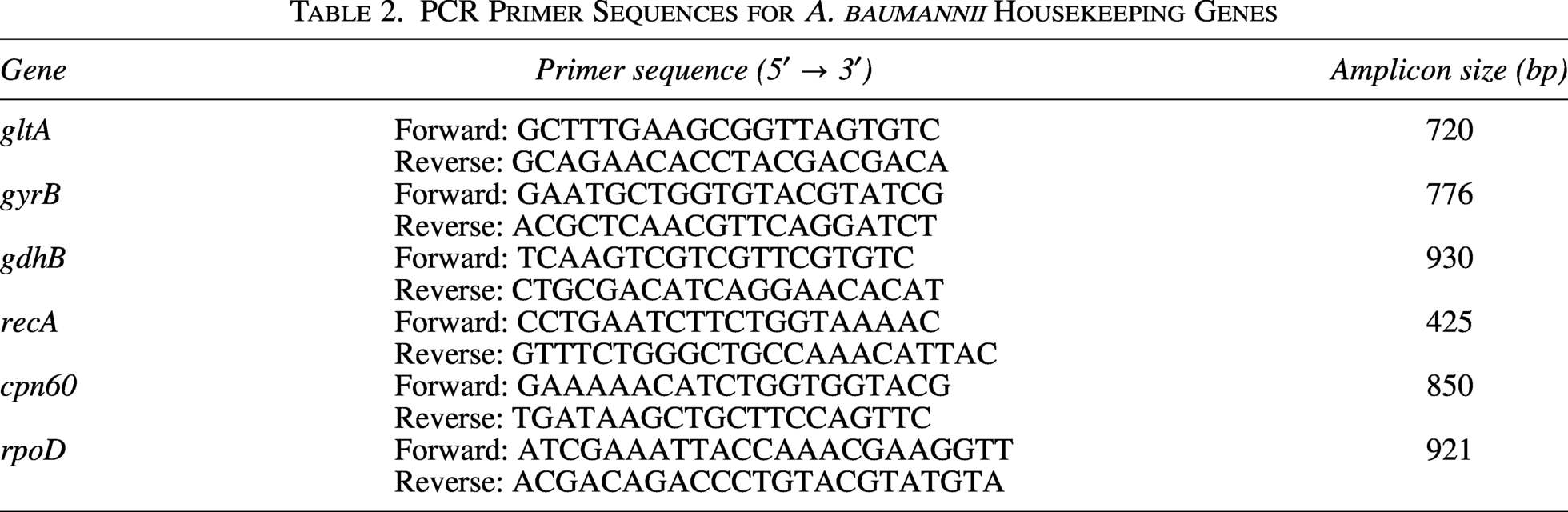
MLST targeting seven housekeeping genes (gltA, gyrB, gdhB, recA, cpn60, gpi, rpoD) was performed using primers synthesized as previously described 19 (see Table 2). For MLST, the 30 μL PCR mixture contained 15 μL of 2× Taq PCR MasterMix, 1 μL of each forward and reverse primer, 1 μL of DNA template, and nuclease-free water to bring the total volume to 30 μL. The thermal cycling conditions were: initial denaturation at 95°C for 5 minutes; 35 cycles of denaturation at 95°C for 30 seconds, annealing at 60°C for 30 seconds, and extension at 72°C for 45 seconds; with a final extension at 72°C for 5 minutes. Sequencing results of the amplified products were compared against the A. baumannii MLST database (https://pubmlst.org/baumannii/) to determine the sequence type (ST). Clonal relatedness among strains was analyzed using eBURST software (Version 3).
PCR Primer Sequences for A. baumannii Housekeeping Genes
Clinical data collection
Clinical data were collected from the medical laboratory information system and electronic medical records, including: (1) Demographic data (sex, age); (2) Comorbidities (categorized as 1 comorbidity or ≥ 2 comorbidities); (3) Total hospital length of stay, hospital stay before the onset of BSIs; ICU admission; (4) Invasive procedures: deep venous catheterization, puncture and drainage, endotracheal intubation, hemodialysis, tracheostomy; (5) Inappropriate empirical antimicrobial therapy, defined as the administration of antimicrobial agents that were later confirmed to be non-susceptible to the isolated pathogen before the availability of blood culture and AST results; (6) Clinical management: blood transfusion, albumin infusion, mechanical ventilation, corticosteroid therapy, immunosuppressive therapy.
Statistical analysis
Antimicrobial resistance data were analyzed using WHONET 5.6 software. Statistical analysis of clinical data was performed using SPSS Statistics Version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables with a normal distribution were expressed as mean ± standard deviation and compared using the independent samples t-test. Non-normally distributed continuous variables were expressed as median (interquartile range) [M (P25, P75)] and compared using the Mann-Whitney U test. Categorical variables were presented as numbers (percentages) and compared using the Chi-square test or Fisher’s exact test, as appropriate. Binary logistic regression analysis was performed to identify independent risk factors for CRAb bloodstream infection. Statistical significance was defined as a two-tailed p value <0.05.
Results
Baseline characteristics of patients with A. baumannii BSIs
A total of 139 patients with A. baumannii BSIs were enrolled. Among them, 84 patients (60.43%) were categorized into the CRAb group, and 55 patients (39.56%) into the CSAb group.
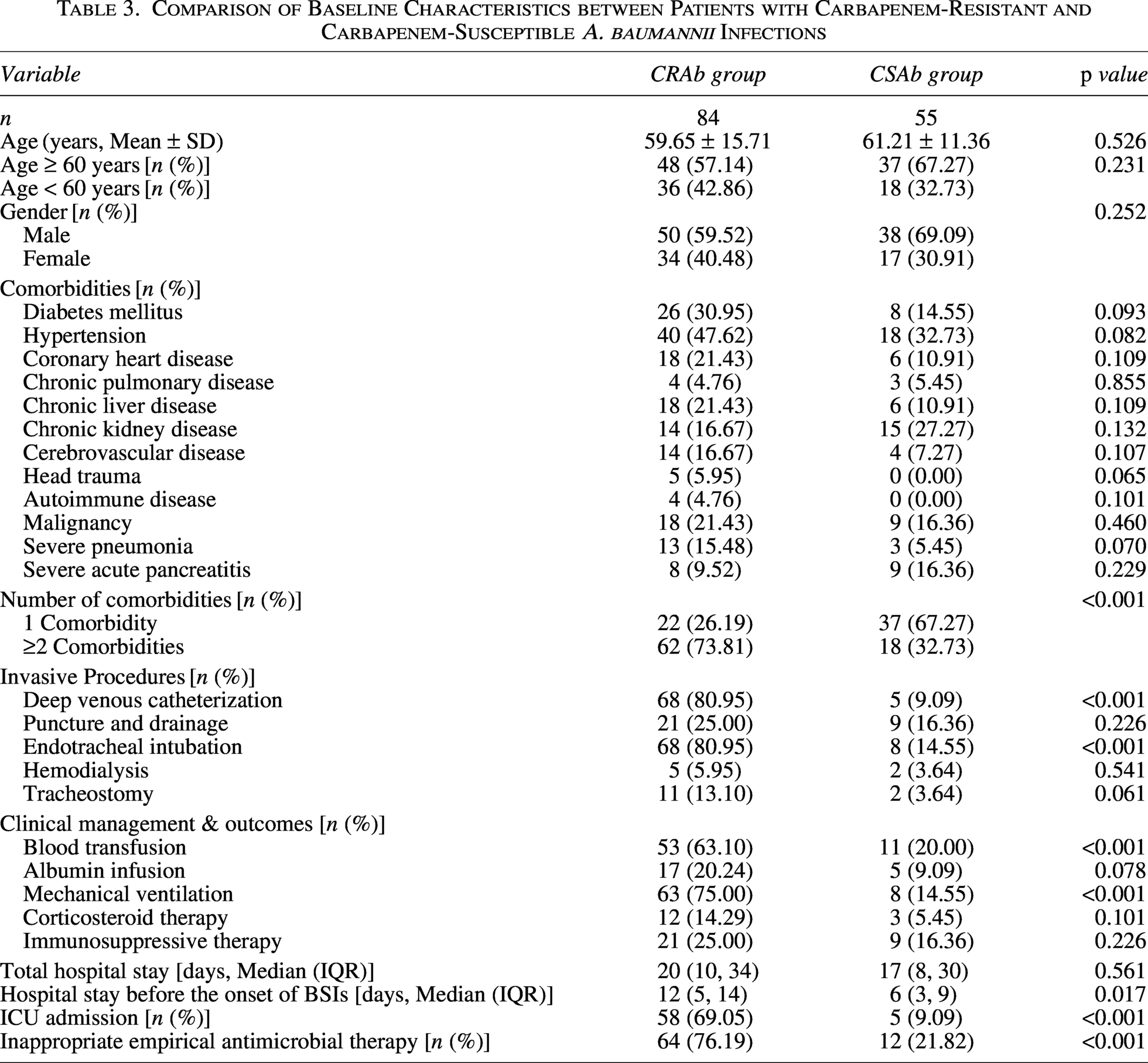
There were no significant differences between the two groups in age, sex, or specific comorbidities. However, the CRAb group had a significantly higher proportion of patients with ≥2 comorbidities and a higher rate of ICU admission (p < 0.05 for all).
Regarding invasive procedures, the CRAb group exhibited significantly higher proportions of deep venous catheterization, tracheal intubation, mechanical ventilation, and blood transfusion therapy. Furthermore, inappropriate empirical antimicrobial therapy was more frequently administered in the CRAb group, and the length of hospital stay before the onset of bloodstream infection was significantly longer compared with the CSAb group (p < 0.05 for all). Detailed characteristics are presented in Table 3.
Comparison of Baseline Characteristics between Patients with Carbapenem-Resistant and Carbapenem-Susceptible A. baumannii Infections
Multivariate logistic regression analysis of CRAb BSIs
Multivariate logistic regression analysis was performed using the forward method, incorporating variables with p < 0.1 from the univariate analysis. All variables had a variance inflation factor of less than 5, demonstrating no substantial collinearity. Multivariate logistic regression analysis identified the following factors as independent risk factors for CRAb BSIs: inappropriate empirical antimicrobial therapy (OR = 8.620; 95% CI: 2.078–35.751), deep venous catheterization (OR = 12.625; 95% CI: 2.263–70.429), prolonged hospitalization before the onset of BSIs (OR = 1.467; 95% CI: 1.123–1.915), and ICU admission (OR = 4.981; 95% CI: 1.898–13.065). The results are presented as a forest plot in Figure 1.
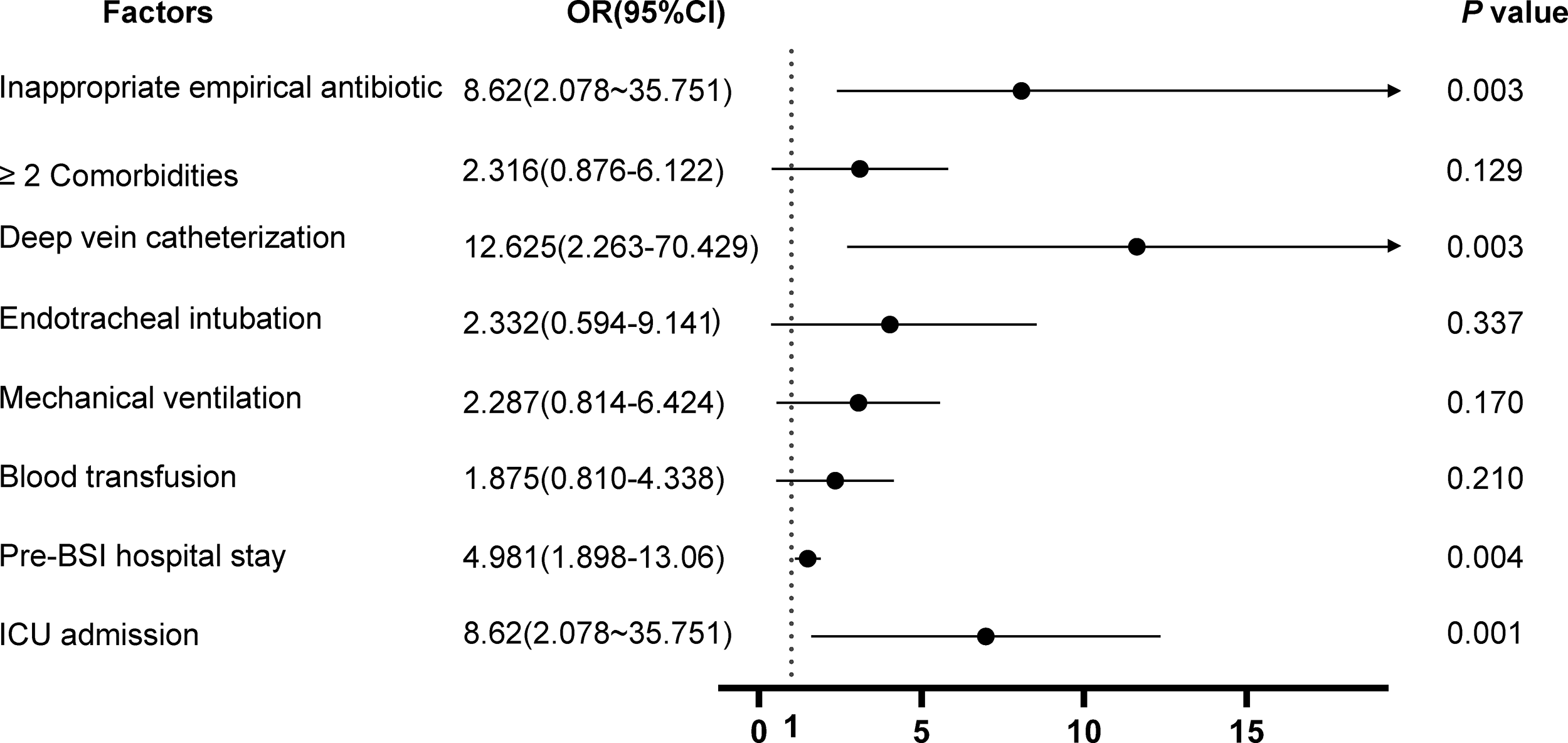
Forest plot of multivariate logistic regression analysis for CRAb bloodstream infections.
In vitro antimicrobial susceptibility testing
From 2020 to 2024, a total of 139 non-duplicate A. baumannii isolates were collected from blood specimens in our hospital. The antimicrobial susceptibility testing results for the 84 CRAb isolates included in this study are shown in Figure 2. These isolates exhibited resistance rates exceeding 70% to most tested common clinical antibiotics. In contrast, resistance rates to tigecycline and colistin were 5.95% and 27.38%, respectively.
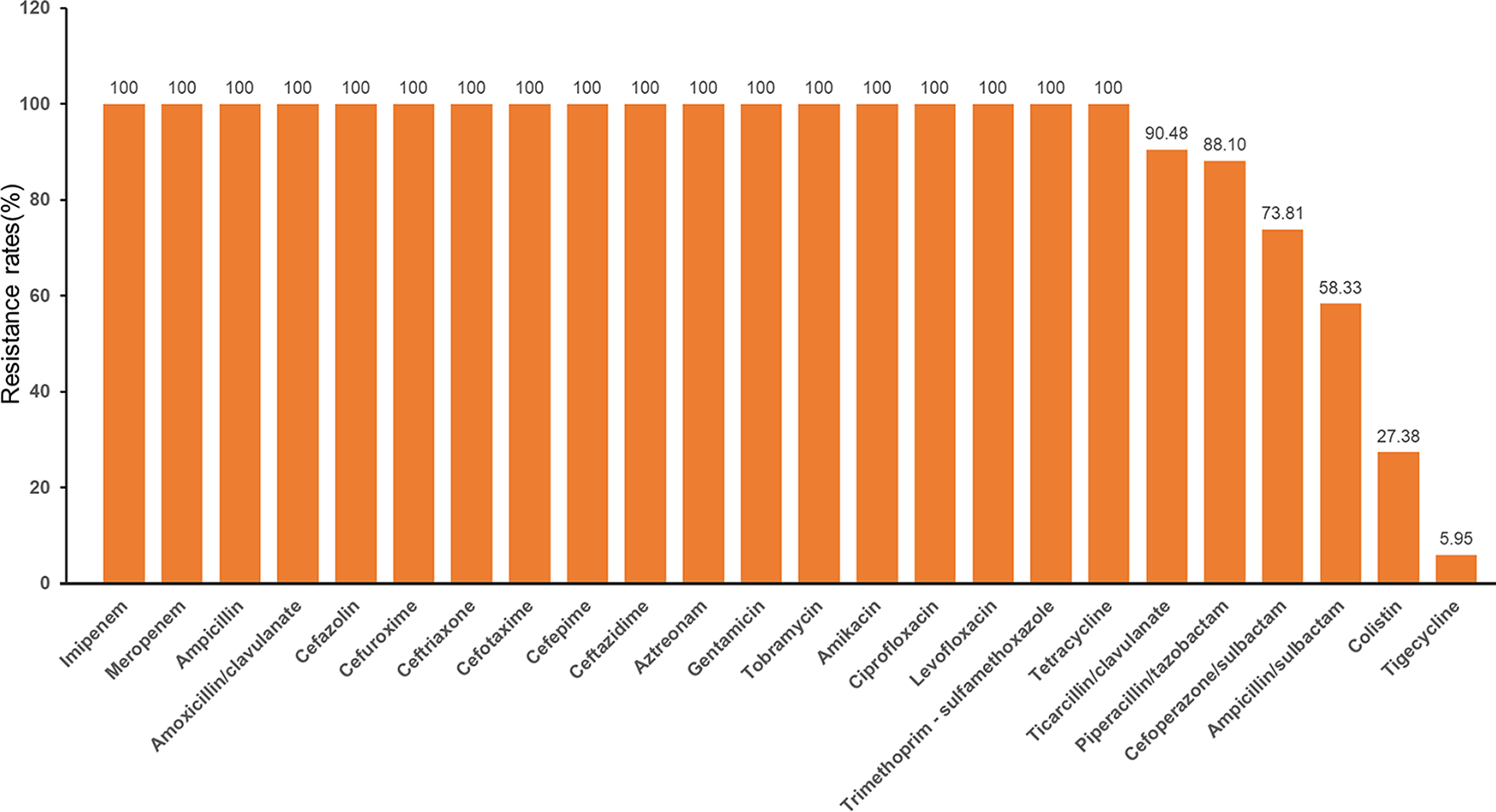
Antibiotic resistance rates of 84 CRAb isolates from blood specimens.
Detection of carbapenemase genes
All 84 CRAb isolates were positive for both the blaOXA-23-like and blaOXA-51-like genes. None of the isolates tested positive for the blaOXA-24-like, blaOXA-48-like, blaOXA-58-like genes, and non-OXA-type carbapenemase genes. DNA sequencing and BLAST alignment confirmed the presence of blaOXA-23-like and blaOXA-51-like genes in all 84 isolates. The concordance rate between phenotypic screening and genotypic detection for carbapenemase production was 100.00%.
Multilocus sequence typing results
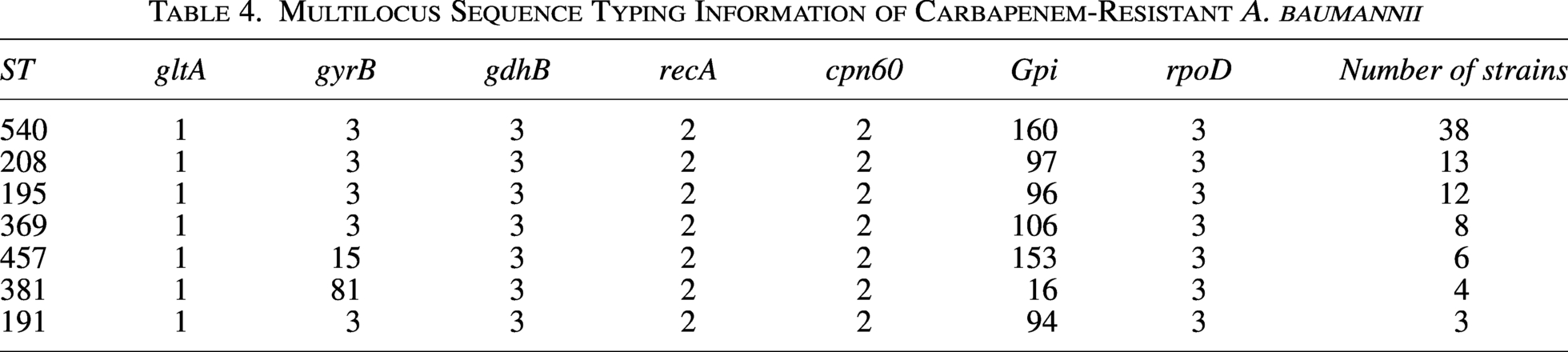
Multilocus sequence typing analysis of the 84 CRAb isolates revealed 7 different sequence types. The distribution was as follows: ST540 (38 isolates, 45.24%); ST208 (13 isolates, 15.48%); ST195 (12 isolates, 14.29%); ST369 (8 isolates, 9.52%); ST457 (6 isolates, 7.14%); ST381 (4 isolates, 4.76%); and ST191 (3 isolates, 3.57%). The detailed results are shown in Table 4.
Multilocus Sequence Typing Information of Carbapenem-Resistant A. baumannii
Phylogenetic analysis
eBURST analysis demonstrated that at the single-locus variant level, ST195, ST208, ST191, and ST369 formed a clonal complex with ST540 as the putative founder. The genetic differences among these sequence types were minimal, with differences in only one allele (the gpi gene), thus classifying them as single-locus variants. This suggests that they belong to the same clonal complex and are closely genetically related, as shown in Figure 3.
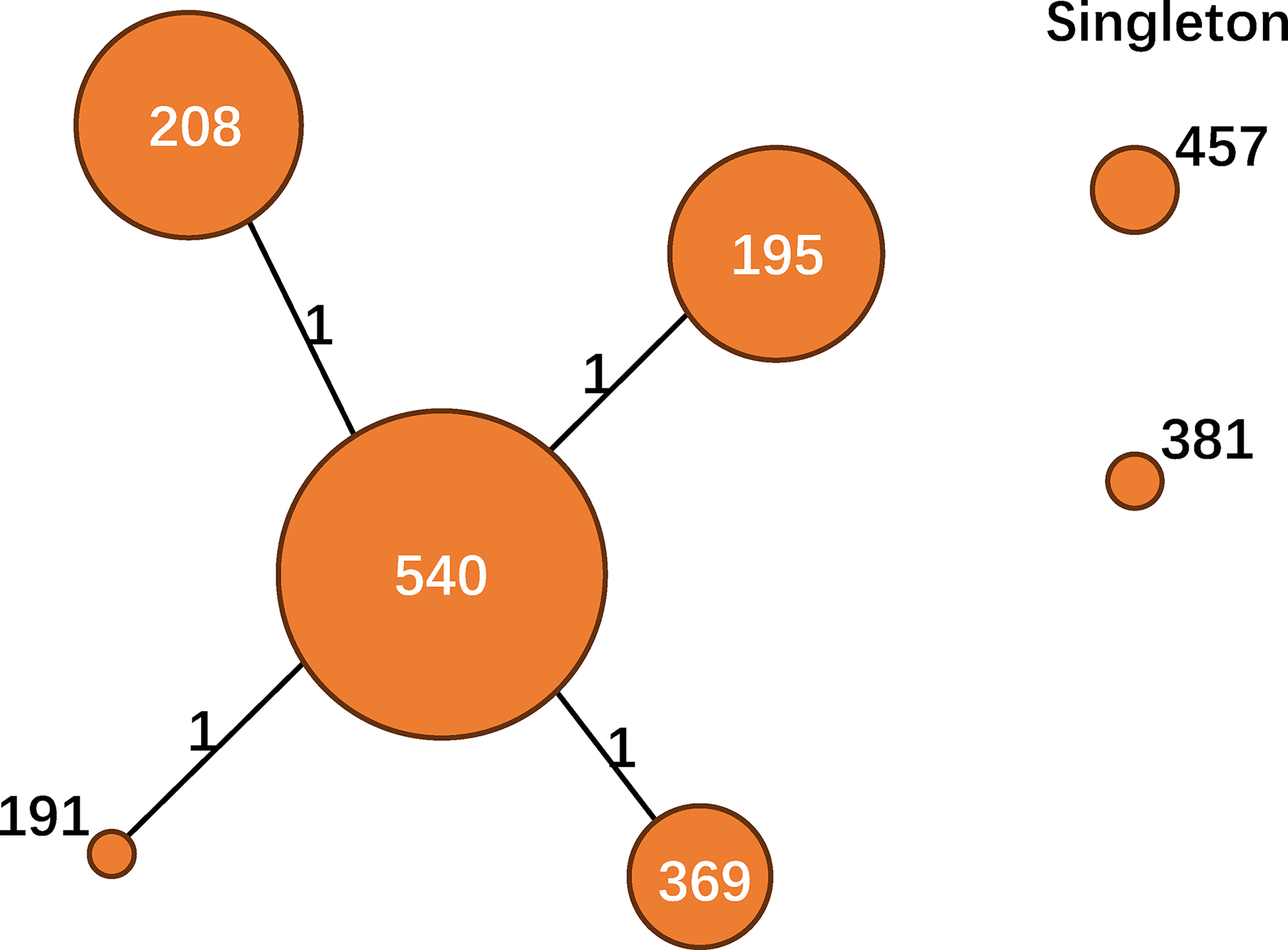
Phylogenetic analysis by eBURST. Each circle represents a unique sequence type, with the circle size corresponding to the number of isolates. The numbers on the lines connecting circles indicate the number of allele differences.
Discussion
In this single-center retrospective study, we investigated the risk factors, resistance genes, and molecular epidemiology of CRAb BSIs in hospitalized patients in Xi’an, China. Our findings indicate that ICU admission, prolonged hospitalization before BSIs onset, deep venous catheterization, and inappropriate empirical antimicrobial therapy were independent risk factors for CRAb BSIs. The blaOXA-23-like gene was identified as the predominant mechanism conferring carbapenem resistance. Molecular typing revealed ST540 as the dominant clone, suggesting potential clonal dissemination within the health care setting.
Our study helps to clarify the risk factors for CRAb BSIs. ICU admission (OR = 4.981), prolonged hospitalization before the onset of BSIs (OR = 1.467), deep venous catheterization (OR = 12.625), and inappropriate empirical antimicrobial therapy (OR = 8.620) were all confirmed as significant risk factors for CRAb BSIs. The identified risk factors are consistent with global reports on CRAb infections.20–22 Patients with ICU admission are more susceptible to CRAb colonization and subsequent infection due to severe underlying conditions, frequent invasive procedures, and extensive exposure to broad-spectrum antimicrobials. 22 Recent studies suggest that CRAb may originate from the patient’s own gut microbiota, where commensal A. baumannii proliferates under the selective pressure of antibiotics. 23 The high infection risk of deep venous catheterization is primarily attributed to biofilm formation on catheter surfaces, which allows A. baumannii to evade host immunity and antimicrobial agents, ultimately causing BSIs. 24 Therefore, strengthening antimicrobial stewardship programs and ensuring appropriate empirical antimicrobial therapy are critical for controlling CRAb spread.
Antimicrobial susceptibility testing showed that the CRAb isolates were resistant to most tested antibiotics except tigecycline and colistin, which reflects the typical multidrug-resistant phenotype of CRAb. Although the clinical use of colistin and tigecycline remains debated, they are currently among the limited therapeutic options for CRAb infections.25,26 In our study, CRAb exhibited 100% resistance to several β-lactam antibiotics, including ticarcillin/clavulanate, piperacillin/tazobactam, ceftazidime, imipenem, and meropenem. This underscores the significant role of β-lactamase production in mediating resistance in these isolates. 27 CRAb resistance mechanisms are complex, involving not only carbapenemase production but also decreased outer membrane permeability, efflux pump overexpression, and target site modifications. 28
The colistin resistance rate of 27.38% observed in our study is higher than both the global average (approximately 5%–15%) and the rates reported in most regions of China. All resistance results have been validated using the gold standard method, thereby ruling out false resistance due to automated testing systems. The fact that 84.2% of colistin-resistant isolates belonged to ST540 suggests a potential clonal outbreak rather than independent acquisition of resistance mechanisms. Further genomic investigations are warranted to elucidate the mechanisms underlying colistin resistance in these isolates, such as the presence of the mcr gene or chromosomal mutations in the pmrAB and lpxACD operons.
In this study, all isolates carried both blaOXA-51-like and blaOXA-23-like genes, while other carbapenemase genes such as blaOXA-24-like, blaOXA-58-like, blaNDM, and blaKPC were not detected. Notably, blaOXA-51-like is an intrinsic gene of A. baumannii, while blaOXA-23-like is acquired. Their co-carriage is consistent with the known resistance profile of CRAb in East Asia. This suggests that OXA-23-type carbapenemase is the primary resistance mechanism in this region, aligning with the prevalent resistance profile of CRAb in East Asia.29,30 The absence of other major carbapenemase genes indicates a relatively singular resistance mechanism, providing a clear target for localized infection control and molecular diagnostics. 31
MLST analysis of the 84 CRAb isolates identified seven sequence types, with ST540 (45.24%) being the predominant clone, followed by ST195 and ST208. eBURST analysis confirmed that ST195, ST208, ST191, and ST369 formed a clonal complex with ST540 as the putative founder. The dominance of the ST540 clone in our center, contrasting with the ST208 clone reported by Xiong et al., 32 underscores that specific CRAb clones can become established and transmitted within individual hospitals. The limited genetic diversity suggests that the horizontal acquisition of new resistance genes may not be the primary driver of CRAb spread. Instead, the persistence and cross-transmission of successful clones, such as ST540, within the hospital environment likely contribute to the clustering of CRAb-associated BSIs. 33 The predominance of the ST540 clone in our hospital may be attributed to the following factors: (1) A total of 84.2% of ST540 isolates co-carry blaOXA-23-like and colistin resistance determinants, allowing them to survive under multidrug selective pressure in ICUs; (2) The ST540 clone exhibits stronger environmental persistence than ST208 on dry surfaces. A. baumannii has been recognized for its remarkable ability to persist in hospital environments under harsh conditions, with desiccation resistance serving as a key determinant of its adaptive success in health care settings. Although direct comparative survival data for ST540 versus ST208 are lacking, the dominance of ST540 across multiple hospitals in China suggests enhanced environmental persistence and clonal transmissibility;2,34 (3) The ST540 clone has superior biofilm-forming capabilities. It facilitates bacterial transmission via invasive medical devices, which helps explain its close association with deep venous catheterization.
Although all 84 CRAb isolates in this study carried blaOXA-23-like and blaOXA-51-like genes, we observed that the MIC of carbapenem antibiotics and the resistance profiles to other antibiotics varied considerably. This phenotypic heterogeneity might be attributed to factors beyond these genes. When the insertion sequence ISAba1 is positioned upstream of blaOXA-23-like or blaOXA-51-like, it can act as a potent promoter, significantly boosting gene expression and resulting in high levels of carbapenem resistance. Moreover, the overexpression of efflux pumps and loss of outer membrane porins are key contributors to the multidrug resistance observed in A. baumannii. The current study did not evaluate these mechanisms, which is a limitation. Future research should incorporate quantitative gene expression analysis, ISAba1 mapping, and whole genome sequencing to fully elucidate the regulatory network driving the resistance phenotype in local CRAb populations.
The identification of inappropriate empirical antimicrobial therapy as an independent risk factor, with an odds ratio as high as 8.620, underscores a critical gap in current clinical practice that is directly amenable to intervention. To mitigate this risk, we propose the following actionable measures for our hospital: (1) implement a pre-prescription review system for broad-spectrum antibiotics (including carbapenems) in the ICU, requiring approval from infectious disease specialists before carbapenem prescription; (2) establish a rapid molecular diagnostic platform for CRAb to obtain carbapenemase gene results within 4 hours after positive blood culture; (3) provide regular training for clinicians on the local CRAb resistance spectrum and rational empirical antibiotic selection for bloodstream infections; (4) monitor the rate of inappropriate empirical therapy quarterly and provide feedback to each department for continuous improvement.
This study has several limitations. First, its single-center retrospective design and limited sample size may introduce selection bias; the CSAb group was relatively small. Second, we focused solely on carbapenemase genes and did not explore the contribution of other mechanisms, such as loss of outer membrane proteins or overexpression of efflux pumps to the multidrug-resistant phenotype. Third, the impact of molecular typing and resistance gene profiles on clinical outcomes, such as mortality or prolonged hospitalization, remains unclear. Fourth, the generalizability of our findings to other geographical regions or institutions is limited. Finally, although MLST suggested clonal spread, higher-resolution typing techniques, such as whole-genome sequencing, would be required to precisely delineate transmission routes and micro-evolution. Future studies should involve multi-center prospective designs with larger sample sizes, incorporate analysis of other resistance mechanisms, and correlate risk factors and molecular characteristics with patient outcomes (e.g., 30-day mortality, total length of hospital stay) to better assess the efficacy of clinical interventions.
In conclusion, ICU admission, prolonged hospitalization before BSIs onset, deep venous catheterization, and inappropriate empirical antimicrobial therapy are independent risk factors for CRAb BSIs. The OXA-23 carbapenemase is the primary resistance mechanism in CRAb isolates from Xi’an, China. The ST540 clone and its related clonal complex were the dominant lineages, indicating potential ongoing nosocomial clonal transmission. These findings underscore the need for enhanced infection control measures targeting high-risk patients and procedures, along with vigilant antimicrobial stewardship.
Authors’ Contributions
J.G. and L.Z. contributed to the conception designed the study. J.G. and Y.R. performed the data analysis. J.G., X.D., and Z.L. were responsible for the draft of the article. Y.R. and Q.G. helped with the analysis through constructive discussions. All authors have contributed to the revision of the article and have read and approved the submitted version.
Availability of Data and Materials
This article does not report any new nucleotide or amino acid sequences. Therefore, no accession numbers were deposited. All data generated or analyzed in the study are included in the article and further inquiries can be directly contacted with the corresponding author Lixia Zhang via e-mail.
Ethics Approval and Consent to Participate
This study was approved by the Medical Ethics Review Committee of Shaanxi Provincial People’s Hospital. All participants provided written informed consent prior to participation. All procedures were conducted in accordance with the Declaration of Helsinki and its later amendments.
Footnotes
Acknowledgments
We would like to thank all the clinical laboratory staff for their technical assistance and the participants and families who participated in the study.
Disclosure Statement
The authors declare that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This work was supported by the