
Abstract
The current study used survey methods to examine initial feasibility and acceptability of a real-world, trauma-informed schools initiative across 15 urban schools and 617 school personnel and classroom teachers. Key indicators included uptake of online asynchronous trauma-informed skills training (TISE) and usage of specific trauma-informed practices by classroom teachers. Approximately 83% of all school personnel completed TISE. Examination of implementation factors revealed organizational health was positively associated with TISE completion, while burnout negatively predicted training completion. Among the subsample of teachers, 76% percent of teachers reported implementing community-building circles, 95% implemented warm and intentional greetings, and 87% implemented mindfulness. For teachers, perceived utility of the practice positively predicted teachers’ implementation of all three skills. Access to practice-focused training at their school predicted community circles implementation, and TISE knowledge predicted intentional greeting implementation. Study results highlight the role of organizational culture, practical support, and usable practices in scaling trauma-informed schools initiatives.
Trauma exposure is a pervasive problem for children and adolescents in the United States, with over 60% of children directly or indirectly exposed to at least one potentially traumatic event (PTE; Finkelhor et al., 2009; McLaughlin et al., 2013). Exposure to PTEs has been linked to increased risk-taking, poor mental and physical health, social maladjustment, and poor educational attainment (Bellis et al., 2014; Hughes et al., 2017; Pechtel & Pizzagalli, 2011). The prevalence of PTEs is heightened among children and adolescents from marginalized communities, thereby increasing risk for associated social, academic, and mental health challenges (e.g., post-traumatic stress, anxiety, and depression; Elkins et al., 2019; Ijadi-Maghsoodi et al., 2022; Milan et al., 2013; Woolgar et al., 2022). Furthermore, youth from low-income, minority, and immigrant backgrounds may be impacted by additionally adverse experiences, such as racial and historical trauma, financial instability, and associated chronic stress (Jaycox et al., 2010; Pumariega et al., 2022; Sacks & Murphey, 2018; Stein et al., 2003). Because of their ability to reduce common barriers to care (e.g., transportation, insurance, cost, stigma), schools have long been key providers of mental health services (Bains & Diallo, 2016). More recently, school-based mental health efforts have expanded to include schoolwide systemic approaches to supporting students exposed to trauma. To this end, the current study used survey methods to examine the initial feasibility and acceptability of an urban school district’s effort to launch a trauma informed care model in schools by investigating uptake of staff-trauma trainings and specific trauma informed practices.
Trauma Informed School Models
School wide approaches to trauma that include prevention, early identification, and intervention can potentially mitigate the impact of PTEs on students’ learning and presentation in the classroom. For example, students with post-traumatic stress symptoms may have trouble concentrating, experience excessive worry, have trouble sleeping, experience mood symptoms, and may be hypervigilant, all of which can affect academics and adult and peer relationships (Bell et al., 2013; Brunzell et al., 2015). Schools can also inadvertently exacerbate some of the negative sequelae of youth trauma exposure. For instance, emotion dysregulation, behavioral challenges, and self-protective behaviors can be interpreted by adults as deliberate misbehavior and defiance, attentional issues, or learning issues (Hobbs et al., 2019). The potential misalignment between students’ trauma responses and how teachers and peers perceive these behaviors can lead to higher use of exclusionary and punitive discipline and negative consequences for students within and outside school (O’Toole & Dobutowitsch, 2023; Zeng et al., 2019).
To facilitate trauma informed systems implementation, the Substance Abuse and Mental Health Services Administration (SAMHSA) developed a trauma informed systems framework via national experts’ input and extensive vetting through federal agencies and public comment. The framework includes four key assumptions and six principles. The four key assumptions are the “Four R’s” of trauma-informed care: realize, recognize, respond, and resist re-traumatization. Realization involves all members of the system understanding the prevalence and impact of trauma on individuals, families, organizations, and communities. Recognizing trauma is the ability to detect post-traumatic stress symptoms. Responding to trauma involves applying the six principles of the trauma-informed approach to all components of a system including policies, language, and behaviors. Finally, resisting re-traumatization involves the understanding that organizations can inadvertently create toxic environments that interfere with their member’s recovery and actively work to prevent this from occurring. The six principles include (1) safety, (2) trustworthiness and transparency, (3) peer support, (4) collaboration and mutuality, (5) empowerment voice, and choice, and (6) cultural, historical, and gender issues (Substance Abuse and Mental Health Services Administration, 2014).
Models of trauma informed schools emphasize training all educators and school staff in the four R’s and integrating the six principles into school practices and policies. Additionally, these models highlight the importance of shifting educators’ mindsets towards a “trauma lens” in which behavioral and academic issues are viewed in the context of what a student or family has been through rather than what is “wrong” with them (Osher et al., 2021). Trauma-informed schools programs typically include at least two of the three following elements: workforce professional development, trauma-sensitive practices, and organizational/environmental changes (Avery et al., 2021; Hanson & Lang, 2016; Maynard et al., 2019).
Workforce professional development typically involves universal staff training that builds awareness of childhood adversity and its sequalae (i.e., Realize and Recognize), provides preventative and restorative behavior management techniques rather than punitive consequences (i.e., Respond and Resist Re-traumatization), and teaches staff emotion regulation skills (i.e., Respond and Resist Re-traumatization). These trainings may also include information about secondary traumatic stress (Hanson & Lang, 2016). Examples of trauma-informed practices or services include evidence-based student interventions and intentionality towards relationships with students (Avery et al., 2021). Organizational or environment change includes restorative discipline policies, protocols for parent communication, physical environment changes, or partnerships with community health agencies (Avery et al., 2021; Hanson & Lang, 2016; Maynard et al., 2019). These three elements theoretically act upon the mechanisms linking exposure to childhood adversity with poor outcomes (e.g., toxic stress response, social information processing deficits, learning and memory deficits, emotion regulation deficits) to reduce the probability or intensity of poor outcomes. For example, developing a trauma-lens among school personnel can promote positive staff-student relationships, increase family engagement, reduce the use of exclusionary discipline practices, and develop children’s practical problem-solving skills (Day et al., 2015; Dorado et al., 2016; Ijadi-Maghsoodi et al., 2017; Perry & Daniels, 2016).
Real World Practice: Implementation of Trauma Informed Schools Within an Urban School District
In the past decade, at least 30 states have enacted policies encouraging schools to provide school staff with professional development on trauma-informed care (Temkin et al., 2021). However, we have very little information about what this looks like in real world practice. The current study examined initial feasibility and acceptability of a real-world, school district wide trauma-informed schools professional development initiative focused on content relevant to the entire school staff. The district, which serves a high number of students from marginalized backgrounds, launched this effort due to concerns over students’ risk for trauma exposure.
They focused on the initial uptake of a trauma-informed knowledge and skills training for all school staff and promoted specific classroom and schoolwide practices aligned with trauma-informed schools. The district’s goals were two-fold: (1) for all school personnel (instructional and non-instructional staff) to receive foundational training in trauma informed skills for educators, and (2) for teachers to use specific classroom and student-focused practices aligned with the trauma informed skills for educators training. To this end, the district adopted an online curriculum called Trauma Informed Schools for Educators (TISE; Wong et al., 2024). TISE was selected because it focused on both knowledge and the application of practical skills in the classroom with students. In addition, the TISE purveyor organization offered training and implementation support options that could be tailored to district needs and existing resources (e.g., asynchronous online training, in-person training, virtual and in-person coaching).
The district chose to promote and support three core practices aligned with TISE course content and districtwide school climate improvement priorities (i.e., community-building circles, warm and intentional greetings, and mindfulness activities). The practices were chosen for their feasibility and potential ability to build relationships, sense of belonging, and regulation skills amongst students (Nilsen & Birken, 2020). Because web-training alone is unlikely to change staff practice (Brownell & Tanner, 2012), local school-based implementation teams were tasked with promoting and supporting teachers to implement the three practices in the context of day-to-day teaching (Fixsen & Blase, 2020). The district deployed a multi-level strategy to achieve their goals: (1) TISE asynchronous, interactive online training for all instructional and non-instructional school staff, and (2) TISE live in-person training for school implementation team members, and (3) live virtual coaching and support for school implementation teams.
The Current Study
Using survey methods, the goal of the current study was to understand the initial feasibility and acceptability of this training and implementation effort mounted across fifteen elementary, middle, and high schools. Specifically, we identified indicators of feasibility and acceptability related to the district’s two primary goals: (a) TISE course completion by all staff and (b) trauma-informed practice use reported by classroom teachers. To design our research questions, the project team relied on conceptual guidance on implementation outcomes (Proctor et al., 2011) and research on theoretically and empirically-based multi-level drivers of implementation success (Aarons et al., 2011; Damschroder et al., 2009; Fixsen & Blase, 2008). Factors at the inner and outer organizational context (i.e., policy, school, district, partnerships, innovation characteristics) and at the individual practitioner-level that can impact implementation success were also examined (Ajzen, 1991; Eccles et al., 2006; Godin et al., 2008; Sanetti et al., 2013). Understanding the connection between these multilevel implementation factors and initial implementation outcomes has practical implications. Implementation support systems, like that mounted by the district, can focus on the most critical organizational drivers (e.g., leadership support, organizational culture, effective implementation teams) and competency drivers (e.g., training, skill development, coaching) for successful implementation (Fixsen & Blase, 2008).
Our research questions related to (a) TISE course completion by all staff and (b) trauma-informed practice use reported by classroom teachers are as follows: 1. To what extent were schools able to achieve uptake in TISE course completion for school staff? 2. What individual and organizational level factors are associated with TISE course completion among school staff? 3. With respect to teacher use of trauma-informed practices from the TISE training course, are teachers reporting that their school made them aware of each of the specific trauma informed practices (i.e., community-building circles, warm and intentional greetings, mindfulness)? a. Among teachers with awareness of the practices, did teachers report getting training in these practices at their school, how much are they using the practices, and how useful do they view the practices to be? b .Among teachers with awareness of the practices, what individual, practice-related, and organizational level factors are associated with teacher-reported usage of trauma-informed practices?
With respect to our research our research questions related to TISE uptake (Question 1), we examined course completion rates for the asynchronous, web-based TISE training by all school staff in the building at each school. To address Question 2 related to individual and organizational level factors associated with TISE training uptake among school staff, we selected relevant organizational-level implementation facilitators (Aarons et al., 2011; Damschroder et al., 2009; Fixsen et al., 2013), and individual-level factors associated with implementation and practice change (Ajzen, 1991; Eccles et al., 2006; Godin et al., 2008; Sanetti et al., 2013). For example, burnout has been associated with reduced implementation of new practices by teachers (Holdaway & Owens, 2015; Ouellette et al., 2019). Particularly, relevant to TISE course completion are leadership support and guidance, organizational culture, and individual-level attitudes, self-efficacy, and burnout. The district’s goal was to have as many school staff in the building trained as possible. However, because there was no formal districtwide requirement or professional development time set aside for the training, it was hypothesized that the principal’s implementation leadership support (e.g., making it a priority, setting aside time) would be positively associated with staff members’ TISE course completion. Similarly, we expected staff perceptions of the overall organizational health of their school would relate to TISE course completion, because staff in schools who perceived their school to have institutional integrity, collaboration, connectedness among staff, and mission-driven may be more motivated to complete the TISE training. We also examined the association between TISE completion and individual-level factors that might influence one’s likelihood to complete the training (e.g., years of experience, role, attitudes toward trauma informed care, burnout).
The next set of research questions (Question 3, 3a, and 3b) focused on teachers’ use of specific trauma-informed practices (i.e., community-building circles, warm and intentional greetings, mindfulness). We focused only on the subsample of classroom teachers since they were in the position to use the practices routinely with students. The district’s goal was for local school implementation teams to support usage of three core practices that district leaders felt were aligned with both TISE and other district initiatives (i.e., community-building circles, warm and intentional greetings, and mindfulness). We first examined whether teachers reported awareness of the practice at their school as intended by the district (Question 3).
Among those teachers with awareness of the practice, we examined teacher-reported practice use, teacher-reported information about the implementation supports at their school (i.e., was training provided), and teacher perceived utility of the practices (Question 3a). Among this same group of teachers, Question 3b focused on the relation between teacher’s self-reported practice use, and relevant organizational factors (i.e., training at their school site, leadership implementation support, openness to change), perceived utility of the practice, and individual-level factors (e.g., demographics, attitudes). We hypothesized that teachers who reported higher use of the practice, would be more likely to (a) have received training on the practice at their school, (b) perceive higher levels of implementation leadership support from their principal, (c) perceive greater openness to change among staff in their school, and (d) perceive higher utility of the practice. We also expected that precursors to individual behavior change derived from the theory of planned action (e.g., attitudes toward trauma informed care, TISE-specific trauma knowledge and competence, and teaching self-efficacy) would be associated with greater practice use (Ajzen, 1991; Eccles et al., 2006; Godin et al., 2008; Sanetti et al., 2013). Burnout was expected to be associated with lower usage of the three practices.
Methods
Participants
Descriptive Statistics for Sample Demographics and Key Study Variables
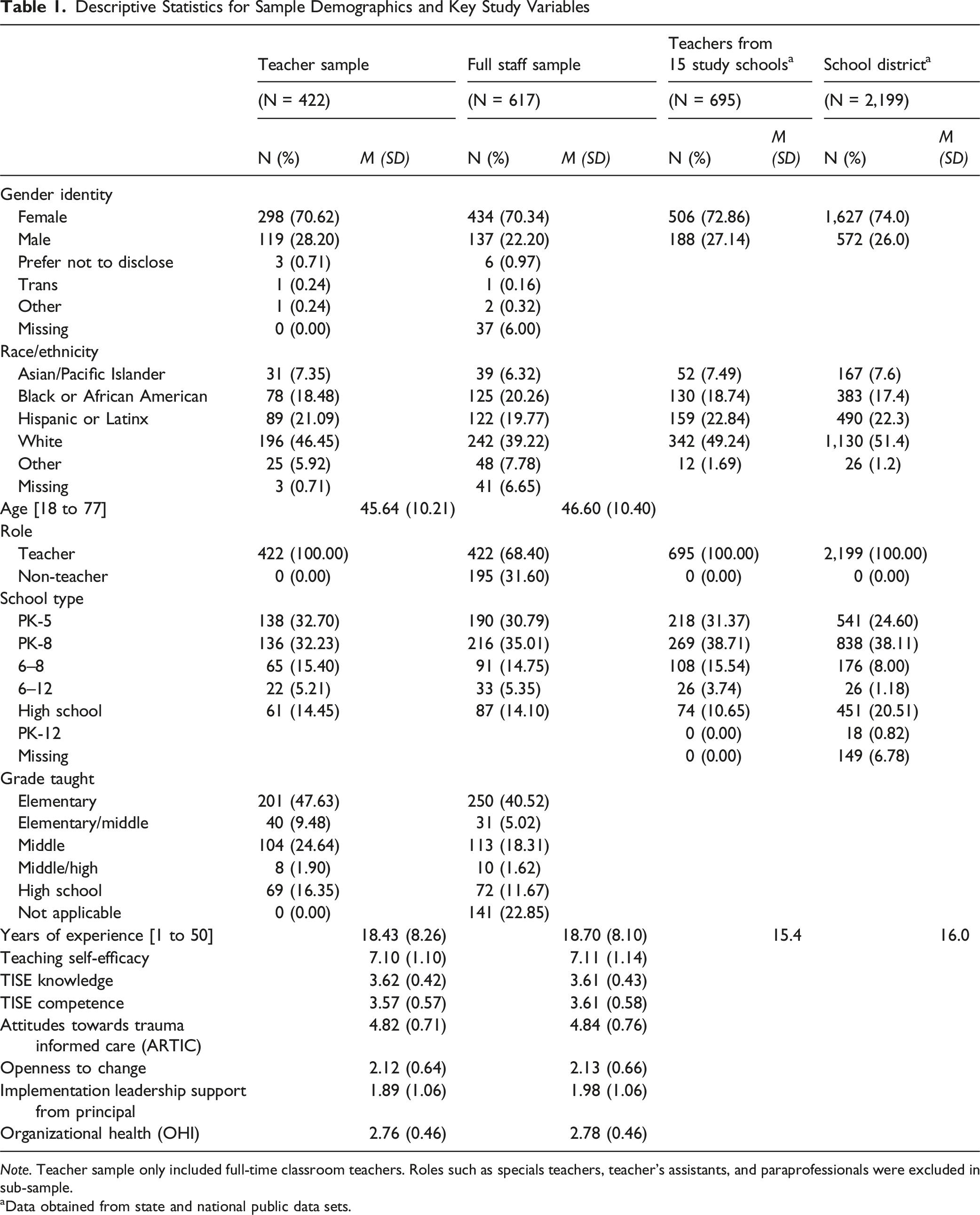
Note. Teacher sample only included full-time classroom teachers. Roles such as specials teachers, teacher’s assistants, and paraprofessionals were excluded in sub-sample.
aData obtained from state and national public data sets.
According to public databases, student demographics for the 15 schools (N = 8,421) were 49.63% Female, 51.37% Male, 29.93% Black, 14.92% White, 34.07% Hispanic, 17.90% Asian, and 3.21% Other, including American Indian/Alaska Native, Native Hawaiian/Pacific Islander, and Two or More Races. Across the 15 schools, 59.88% of students qualified for Free/Reduced Lunch, 14.17% Students with Disabilities, and 13.04% Multilingual Learners.
The study sample is part of a large urban school district composed of 39 schools, representing twelve PK-5 schools, fourteen PK-8 schools, four 6–8 middle schools, one 6–12 secondary school, seven 9–12 high schools, and one PK-12 special education school. Districtwide student and staff demographics available from public databases are reported in Table 1. According to public datasets, for the entire district, about 60% of students qualify for Free/Reduced Lunch, with 14% of students classified with disabilities, and 13% English Language Learners, speaking over 40 first languages. Approximately 48% of students identify as female and 52% as male. As shown in Table 1, district and study sample characteristics are comparable.
Procedures
Study Context and Partners
Through federal grant funding that was designed to support schools in creating trauma informed systems, the district launched a trauma-informed professional development initiative, the Trauma Informed Skills for Educators (TISE) training, to the district’s first cohort of 15 schools. For the current project, the district was supported by a multiyear research-practice partnership with a local public research university. Research partners were responsible primarily for supporting evaluation efforts and advising on the design of implementation activities. Related to this specific TISE rollout, the research team and the TISE purveyor organization provided consultation on implementation approaches. However, the scale and scope, selection of schools, and final approach to training and implementation support structures were all determined by the district leaders as part of the collaborative design process.
TISE Rollout Structure
TISE and the rollout plan were presented initially to all district principals during a principal’s meeting in the first year of the grant (Winter of the 2022–2023 school year). The plan included sequencing the training and supports across the district via three different cohorts (2023–24, 2024–25, 2025–2026). The cohorts were developed by the district leaders based on preliminary discussions with principals, each schools’ bandwidth based on their involvement in other district initiatives, and a desire to ensure that a range of schools with needs were included across the K-12 grade span. Subsequently, the current study only presents data from the concluded first year of implementation, SY2023–2024.
School administrators were informed that the goal was to have all instructional and non-instructional staff in their schools take part in the TISE online, asynchronous training and to implement some feasible practices linked to TISE. The district also asked each school to identify the members of their school’s implementation team to support this effort. Schools were encouraged to leverage appropriate existing teams embedded within their school structure (e.g., a school climate team or MTSS team) whenever possible. Teams either included an administrator or consulted a school administrator regularly.
To ensure that the implementation team members had sufficient expertise to do this, team members received a full day in-person TISE training in the Spring of 2023, before they were expected to roll out the asynchronous TISE training to their schools in the subsequent Fall 2023 school year. The purpose of this live training was to familiarize team members with the trauma-informed school approach and gain stakeholder buy-in to the concept. The first half of the training-day focused on providing psychoeducation about childhood trauma, its sequelae, and positive childhood experiences that can promote resilience in the face of trauma. The second half of the day focused on presenting specific trauma-informed practices that the implementation teams could turnkey to their school staff.
Implementation Support Structure
Leveraging these teams, the district deployed a multi-level strategy: (1) TISE training for all instructional and non-instructional school staff using an accessible, asynchronous web-based platform, (2) the aforementioned TISE live in-person training for school implementation teams, and (3) live virtual coaching and support for school implementation teams. This approach was intended to achieve the district’s goal of broad reach, while also supporting frontline school-based implementation teams to move knowledge into practice. School administrators and their teams were tasked with supporting their school’s entire staff in completing the web-based TISE course. Administrators were provided with routine progress monitoring data and completion reminders. School implementation teams were also tasked with promoting and supporting practice use by teachers in their school.
TISE Expert Coaching
Implementation teams received monthly virtual coaching from TISE experts, and a yearly in-person site visit co-led by the TISE team and district-level specialists. Beginning in the Fall of 2023, monthly virtual coaching was provided to implementation team members to support the rollout of TISE in their schools. This meant working with team members to support online course completion and helping teachers implement core practices in their classrooms. Of note, administrators were welcome to attend the coaching alongside implementation team members. Coaching was provided by TISE developers from the Center for Safe and Resilient Schools via synchronous video calls. During the 90-min-long coaching sessions, teams received direct instruction on specific trauma-informed skills, developed action plans to facilitate TISE training uptake and trauma-informed practice implementation in their schools, and shared their experiences with implementation.
Finally, each school received in-person support via a formal site visit from TISE coaches, district staff, and university researchers. Schools also received, as requested, in-person implementation support from district personnel and clinicians via in-vivo modeling. For example, at the beginning of the 2023–2024 school year, district-employed clinicians modeled the facilitation of community-building circles in each of the schools. The district also promoted a mindfulness app which was free and available to all district employees. During the 2024–2025 year (after the conclusion of this study), schools in the first cohort could continue to receive support from district staff and TISE experts upon request and maintained access to TISE resources.
Trauma Informed Skills for Educators (TISE)
The TISE online course consists of eight modules and was developed by researchers, mental health personnel, and educators from the RAND Corporation and the University of Southern California. Each module takes about 15–20 minutes to complete, totaling up to 2.5 hours. Modules 1–4 teach school personnel foundational information about childhood trauma and resilience. These modules cover the neurological impacts of trauma, symptoms of trauma, and factors that promote resilience in the face of potentially traumatic events. Modules 5–8 of the TISE curriculum focus on skill building. Specifically, educators are taught how to physically create a trauma-informed classroom, communicate in a trauma-informed manner, de-escalate tense situations, and collaborate with staff in a trauma-informed manner. Not only are educators provided with this information, but they are also able to participate in gamified simulations in which they practice the trauma-informed skills they learned.
While specific skills are taught and practiced in the TISE course, TISE is not a prescriptive or rule-bound approach to developing trauma-informed schools. TISE encourages fidelity to trauma-informed principles rather than adherence to a fixed set of pre-ordained practices, allowing schools the autonomy to adopt or adapt strategies that are responsive to their specific settings. TISE offers a rationale, and examples of practices and skills related to trauma informed concepts, such as building relationships, building community, and supporting mindfulness and emotion regulation.
Trauma Informed Practices
Based on alignment with TISE principles and existing district initiatives, the district decided to roll out three priority practices: community-building circles, warm and intentional greetings, and mindfulness practices. Community-building circles are structured sharing opportunities where school staff and students take turns responding to prompts designed to share experiences and build relationships. Warm and intentional greetings are designed to help staff focus on welcoming each student into the school with a positive relational tone, acknowledging their presence and value (e.g., smiles, high fives, positive comments about seeing the person). The goal of both community circles and warm and intentional greetings are to foster connections and increase students' sense of belonging. Mindfulness activities are designed to support emotional regulation and foster stress reduction. They may involve breathing and grounding exercises and help by allowing students to focus on the here and now, attune to the setting they are in, and increase their awareness of thoughts, feelings, and sensations. Choosing these three practices created a set of concrete actions that school implementation teams and administrators could focus on as they moved their school’s staff from training to practice change. The practices could also be further tailored to each school context. This was further supported in the coaching offered to the implementation teams via action plans and additional training.
Data Collection
All data collection activities were conducted in service of the school district’s internal and external evaluation of the program, as well as funder-required programmatic activities, and IRB approval was obtained. Prior to completing TISE training, participants were asked to complete a baseline survey between Spring 2023 and Spring 2024. After completing the survey, they were given a code to complete the online TISE training modules. A post-training survey was administered in May–June 2024. The overall response rate for the pre and post surveys was 57% of all school personnel in the 15 schools. Due to the variability of time between pre and post measures that occurred because of individual school’s data collection timelines, the primary measures of interest in this study are from the post-test survey. Exceptions include demographics, teacher self-efficacy, organizational health, openness to change, and burnout constructs, which were only administered at baseline. Subsequently, the eligible sample for analysis of research questions related to TISE completion was 617 participants across elementary, middle, and high schools completing the post-test survey in Spring 2024. The eligible teacher subsample examining trauma informed practice usage was 422 participants across elementary, middle, and high schools.
Measures
Implementation Outcomes
TISE Web Course Completion
Completion rates for the online TISE course were collected separately for the eight modules, with each module marked as either “not started”, “started” (i.e., participant began the module but did not complete it) or “finished”. To determine full-course completion rates, each participant’s overall progress was coded as “complete” (i.e., all eight modules were “finished”) or “incomplete”.
Practice Uptake, Acceptability, and Perceived Utility
Several indicators of practice uptake and acceptability were created for the current study related to community building circles, warm and intentional greetings, and mindfulness activities. An initial item was developed to assess whether staff had any awareness about practices being prioritized by the district and school implementation teams. If they did have basic awareness of the practice, they were asked additional questions about training, usage, and utility. Surveys asked the following questions: 1. Has [strategy] been discussed at your school?
If they reported it had been discussed, they were asked: 2. Did you receive any training, modeling, or resources on how to use [strategy]? 3. How often do/did you implement [strategy] in your classroom? 4. How helpful/useful do you find [strategy] for your classroom?
If no, respondents did not see the additional questions.
The last two questions were answered with a five-point scale ranging from 1 (never) to 5 (daily). Anchors were recoded to “no use,” “inconsistent use,” and “consistent use.” “Inconsistent use” was defined as Monthly, Once a week, or Multiple times per week for warm/intentional greetings, and “consistent use” was defined as Daily. This is because educators were trained to engage in intentional greetings at least once per day and encouraged to intentionally greet students before each class in grades that rotate classrooms. Thus, anything less than daily application of this skill would be considered inconsistent use. However, educators were encouraged to engage in community circles and mindfulness at least once a week. Thus, “consistent use” for the skills of mindfulness and community circles was considered “once a week,” “multiple times per week,” or “daily,” and “inconsistent use” was defined as “monthly.”
Individual Factors
Demographics
General demographic data were collected from all participants as part of the baseline survey administered prior to the TISE training. This encompassed participants’ school name, school type (e.g., K-5, middle school), gender, age, race/ethnicity, school position (e.g., full-time teacher), current grade(s) taught, if applicable (e.g., 3rd grade, “all grades”, “not in a teaching role”), and total years of experience as an educator.
Attitudes Towards Trauma Informed Care
The educator version of the Attitudes Towards Trauma-Informed Care (ARTIC) is a 35-item bipolar survey intended to capture participants’ favorable versus unfavorable attitudes towards TIC (Baker et al., 2016). Participants indicated where their belief lay on a bipolar 7-point Likert between two statements to best represent their personal beliefs during the past two months. One statement captures favorable trauma-informed attitudes, and the second statement captures unfavorable trauma-informed attitudes. An example item asks respondents to rate their belief between the two statements of “Students’ learning and behavior problems are rooted in their behavioral or mental health condition” versus “Students’ learning and behavior problems are rooted in their history of difficult life event.” For this example, a score of 1 represents the responders’ full belief of the first statement, and a score of 7 represents the responders’ full belief of the second statement. The ARTIC is composed of a total score and five subscales (underlying causes of problem behaviors, responses to those behaviors on-the-job behavior, self-efficacy, and reactions to the work). The current study only utilized the total score. Cronbach’s alpha in the current study for the ARTIC total scale score was .89.
TISE-Specific Knowledge
A 23-item knowledge scale was developed by TISE creators (Wong et al., 2024). Participants were asked to rate 23 items on how much they agreed with each statement on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Example items include “Encountering reminders of a traumatic experience can elicit the fight, flight or freeze response in a student” and “Highlighting and celebrating students’ diversity can increase traumatized students’ sense of belonging.” Higher mean scores reflect more TISE knowledge. Cronbach’s alpha for the TISE knowledge questions in the current study was .84.
TISE-Specific Perceived Competence
An eight question perceived competence rating scale was developed by TISE creators (Wong et al., 2024). The scale was used to capture the perceived competence in carrying out trauma-related practices taught in the TISE training. Participants read a statement and were asked to indicate how effective they feel addressing trauma-related issues with students on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Example items include “I am able to recognize when a student’s behavior may be a sign of stress or trauma” and “I know how educators can help students bounce back from trauma.” Cronbach’s alpha in the current study was .88.
Teacher Self-Efficacy
The Teachers’ Sense of Efficacy Scale Short Form was used to capture participants’ self-efficacy, or belief in one’s ability to succeed in their job (Tschannen-Moran & Hoy, 2001). This 12-item scale was administered to all staff in the pre-training survey, and contains three 4-item subscales: student engagement, classroom management, and instructional strategies. Participants responded to each item, with the item stem “How much can you do?” using a 9-point Likert scale ranging from 1 (nothing) to 9 (a great deal). Example items from each subscale, respectively, include “How much can you do to help your students think critically?”, “How much can you do to get through to the most difficult students?”, and “To what extent can you craft good questions for your students?”. This scale was given to teacher respondents only. Cronbach’s alpha in the current study was .94.
Teacher Burnout
The Maslach Burnout Inventory—Educators Survey (Maslach et al., 1996) was used to assess levels of burnout among survey participants. The scale has 22-items related to burnout across three different dimensions (i.e. Emotional Exhaustion, Depersonal-ization, and Personal Accomplishment). Items are answered on a 4-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). For the current study, a total MBI score was calculated using the sum of the subscale scores. Cronbach’s alpha for the current study was .89.
Organizational Factors
Implementation Leadership Support from Principals
We adapted six items from Lyon et al.’s (2022) School Implementation Leadership Scale (SILS). These questions were used to capture a participant’s perception of how their school principal was doing at supporting and leading the implementation of trauma-informed practices. One item was selected from each of the following six subscales: knowledgeable, supportive, perseverance, communication, vision, and availability to fit this project’s purpose. Participants were asked to rate their principal’s leadership on a 5-point Likert scale ranging from 0 (not at all) to 4 (a very great extent). Example items include “Our principal talks about trauma-informed practices” and “Our principal is accessible if I have a problem or concern, or if I need help with implementing trauma informed practices.” Cronbach’s alpha was .97.
Organizational Health
The current study used an abbreviated version of the Organizational Health Inventory (Hoy et al., 2002). The OHI is designed to measure five dimensions of school climate (institutional integrity, collegial leadership, resource influence, teacher affiliation, academic emphasis). The OHI includes versions for elementary, middle, and high schools and ranges from 37 to 44 items depending on the version. Respondents are asked to rate each item on a scale of 1 (rarely occurs) to 4 (very frequently occurs). An abbreviated version of the OHI was developed for the current study based on district feedback regarding participant burden and the need for a single version of the OHI (in lieu of elementary, middle, and high school versions). To create the modified OHI, the researchers selected four items within each subscale based on the following criteria: (1) the items best captured the different dimensions of the construct while minimizing redundancy, and (2) the items applied across all ages. The current study utilized the overall organizational health score (alpha was .84). This measure was used in the analysis of TISE completion only.
Openness to Change
The Openness to Change questions were adapted from Bryk & Schenider’s (2002) and Cramer et al.’s (2023) orientation to innovation measure. These questions measured participants’ perspectives of how change is accepted and supported by all staff members. This measure was administered pre-training to participants only and contains six items with two 3-item subscales: Learning and Innovation. For the Learning subscale, participants were asked to rate on a 5-point Likert scale ranging from 0 (none) to 4 (nearly all). An example item of this subscale is “how many staff in the school are eager to try new things”. The Innovation subscale used a 4-point Likert scale ranging from 0 (strongly disagree) to 3 (strongly agree) and asked how much they agreed with statements such as “in this school all staff are encouraged to ‘stretch and grow’”. Cronbach’s alpha in the current study was .88. This variable was used in the analysis of specific teachers practices due to its practice focused quality.
Analysis
TISE Uptake (Research Questions 1 and 2)
All analysis was conducted using SPSS Version 26. To answer Question 1 regarding the rates of TISE course completion across all school staff (n = 617), descriptive statistics tabulated the frequency count and percent completion for all study participants, for each school, and for the subsample of teachers. Question 2 focused on examining multi-level factors that might be associated with TISE completion. For the full sample of instructional and non-instructional school staff, we first conducted bivariate analyses to evaluate the extent to which hypothesized predictor variables were related to TISE completion. We then conducted a logistic regression predicting completion of TISE training. Individual-level predictor variables included race/ethnicity, total years of teaching experience, attitudes towards trauma-informed care, burnout, and job role (i.e., teacher or non-teacher). Organizational factors included organizational health, principals’ implementation leadership, and grade level taught (i.e., elementary, middle, or high school).
Trauma-Informed Practice Use by Teachers (Research Questions 3, 3a, and 3b)
Our next research questions were focused on teachers’ (n = 422) use of trauma-informed practices aligned with TISE. As noted above, we focused this analysis on teachers only because practice use was most clearly aligned with their role in the school. To assess teachers’ awareness of practices (Question 3), we calculated the appropriate descriptive statistics (frequencies, percentages, means, and standard deviations) to determine how many teachers said their school had discussed each of the three practices they were being asked to use (i.e., community-building circles, warm and intentional greetings, mindfulness activities).
Question 3a focused only teachers that responded “yes” the practice was discussed in their school, to assess training received at the school, perceived utility, and practice usage. Appropriate descriptive statistics (frequencies, percentages, means and standard deviations) were calculated to assess whether they received any training at their school, how often they implemented the practice, and how helpful/useful they found the practice.
To examine organizational, practice-related, and individual factors associate with trauma-informed practice use by teachers (Question 3b), we conducted three regressions focused on practice use (i.e., community-building circles, warm and intentional greetings, mindfulness activities). As above, analysis included only teachers who indicated a given practice had been discussed at their school. Prior to conducting the regressions, we conducted bivariate analyses to evaluate the extent to which hypothesized predictors variables were related to TISE completion. For continuous variables, bivariate correlations were conducted. To determine whether the categorical variables of gender, race/ethnicity, and school level were associated with skill use, independent samples t-tests and one-way ANOVAs were conducted. Factors that had both theoretical rationale for predicting skill use and statistical rationale based on preliminary analyses were included in the regression models. Demographic variables (race/ethnicity, gender) were included if it was determined that they were related to the dependent variable.
In the three multiple regressions (Community Circles, n = 256; Warm Greetings, n = 182; Mindfulness, n = 270), individual factors included gender, total years of teaching experience, teaching self-efficacy, trauma related knowledge, beliefs about their competence to engage in trauma-informed practices, attitudes towards trauma-informed care, burnout, and perceived utility of the skill. Organizational factors included whether training was provided on the skill, organizational openness to change, grade level taught (i.e., elementary, middle, or high school) and perceived implementation leadership support. A multiple regression analysis was conducted for each dependent variable: (i.e., community circles, warm and intentional greetings, mindfulness). To account for potential Type I error arising from multiple comparisons, a Bonferroni correction was applied to the multiple regressions examining predictors of trauma-informed practice use among teachers. The adjusted significance threshold was set at α = 0.0167 (0.05 ÷ 3).
Results
School Staff TISE Course Completion Among School Staff (Question 1)
TISE Web Course Completion by All School Staff
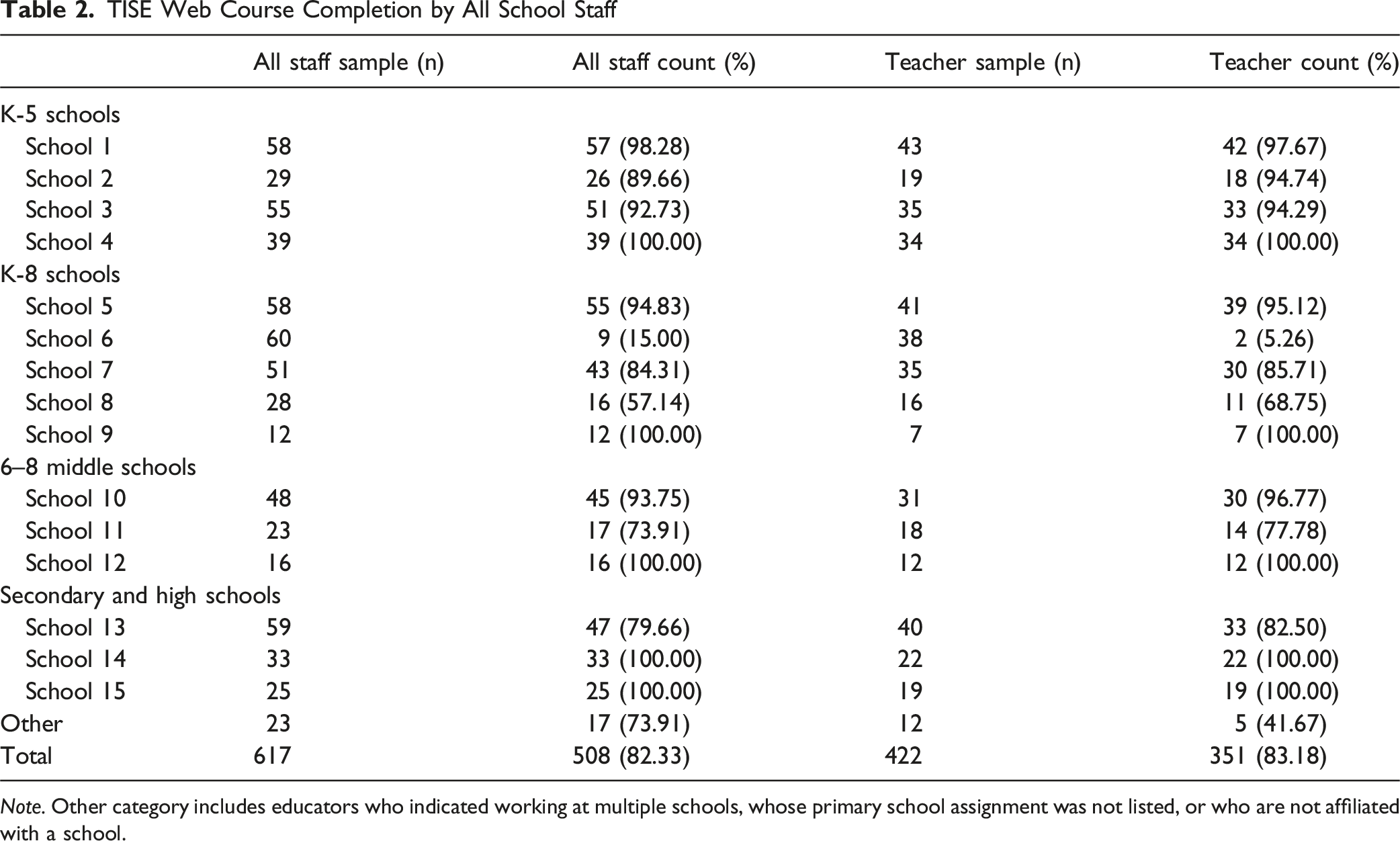
Note. Other category includes educators who indicated working at multiple schools, whose primary school assignment was not listed, or who are not affiliated with a school.
Multilevel Predictors of TISE Uptake Among School Staff (Question 2)
Bivariate Associations Between Individual and Organizational Factors TISE Completion for All School Personnel
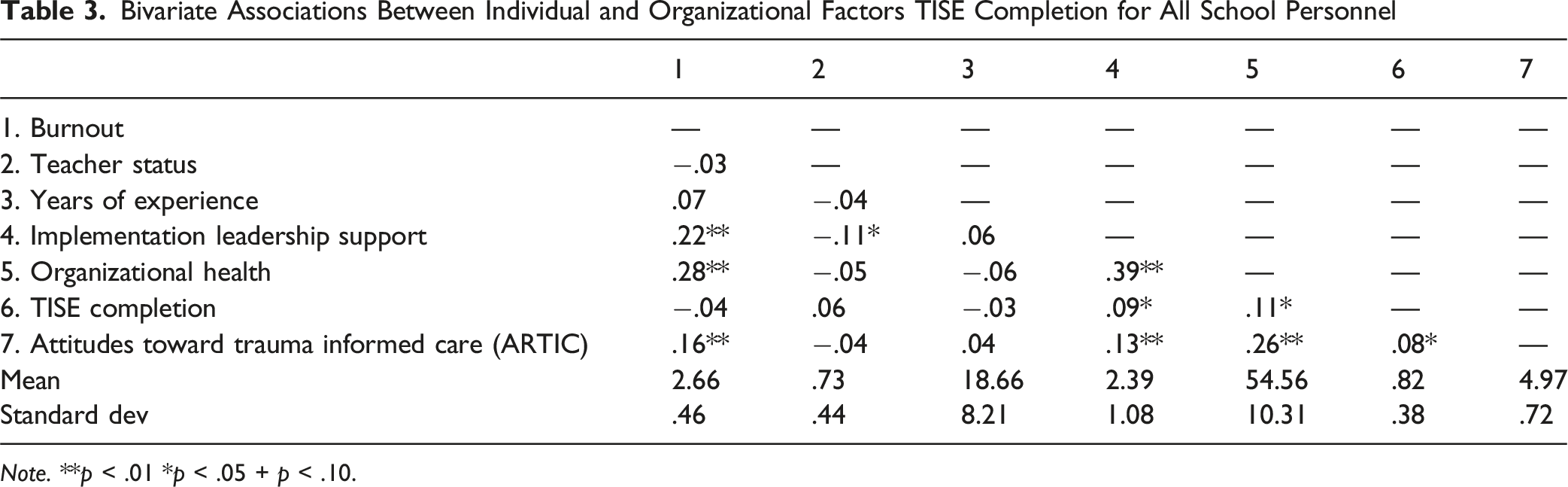
Note. **p < .01 *p < .05 + p < .10.
Logistic Regression Predicting TISE Training Completion for All School Personnel
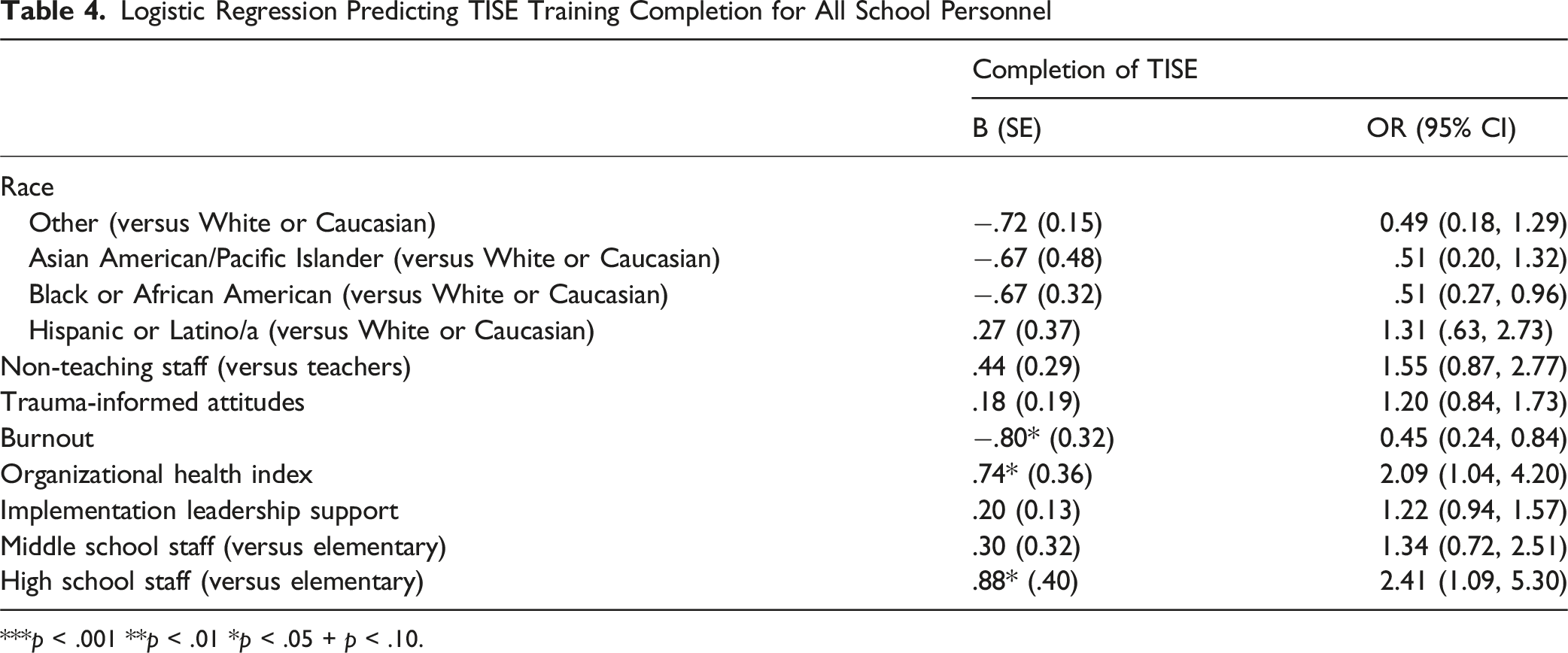
***p < .001 **p < .01 *p < .05 + p < .10.
Teachers’ Awareness of Trauma-Informed Practices at Their Schools (Question 3)
Teacher Report on School Supports, Practice Use, and Practice Utility
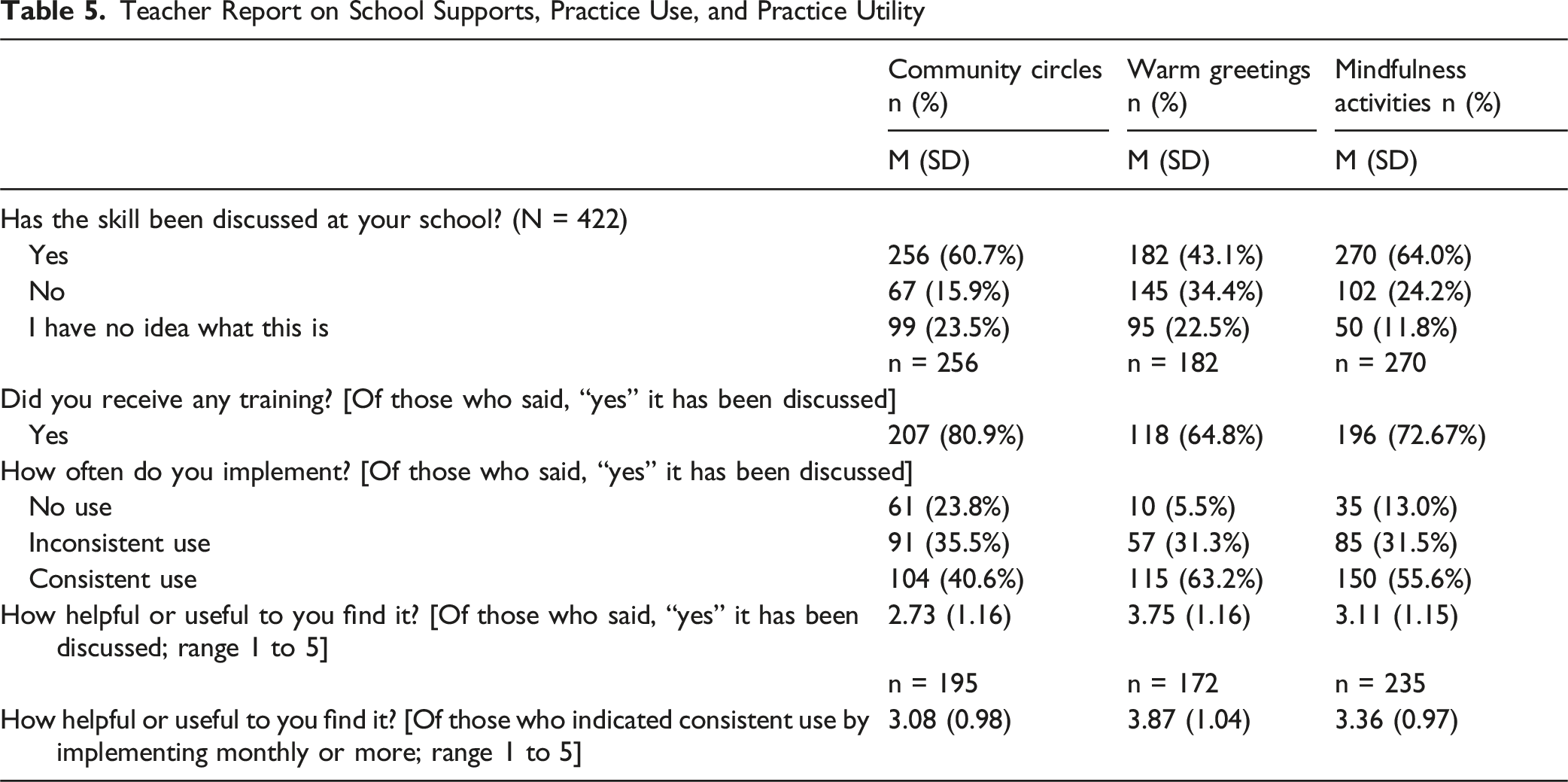
Teachers’ Reported Implementation Support, Practice Use, and Practice Utility (Question 3a)
Among teachers with awareness of the practices, Question 3a addressed whether teachers reported getting training in these practices at their school, how much are they using the practices, and how useful do they view the practices to be. As shown in Table 5, among teachers who said the skill had been discussed at their school, the skill in which the most educators were trained was community circles with 80.90% of teachers reporting receiving training. The most consistently used skill among school staff was intentional/warm greetings (63.2%) followed by mindfulness (55.6%) and community circles (40.6%). Intentional/warm greetings were reported to be the most useful or helpful skill (M = 3.75). Finally, among teachers who engaged consistently in each of the skills, all were reported to be, on average, moderately to greatly helpful or useful.
Multilevel Predictors of Trauma Informed Practice Usage Among Teachers (Question 3b)
Bivariate Associations Between Individual and Organizational Factors and Implementation Outcomes for Teachers
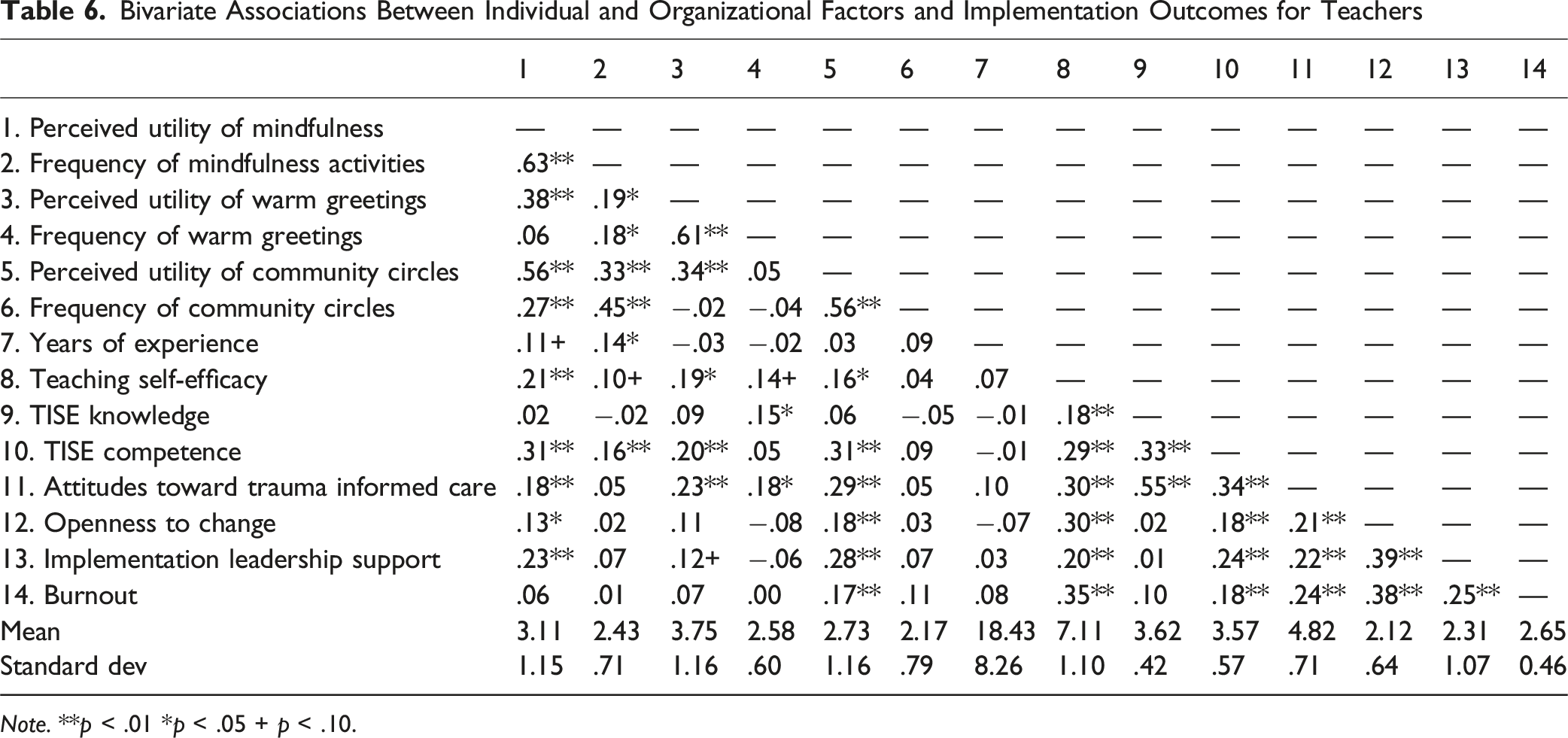
Note. **p < .01 *p < .05 + p < .10.
Multiple Regression Analyzing Association of Individual and System-Level Predictors With Teachers’ Use of Community Circles, Warm and Intentional Greetings, and Mindfulness Activities
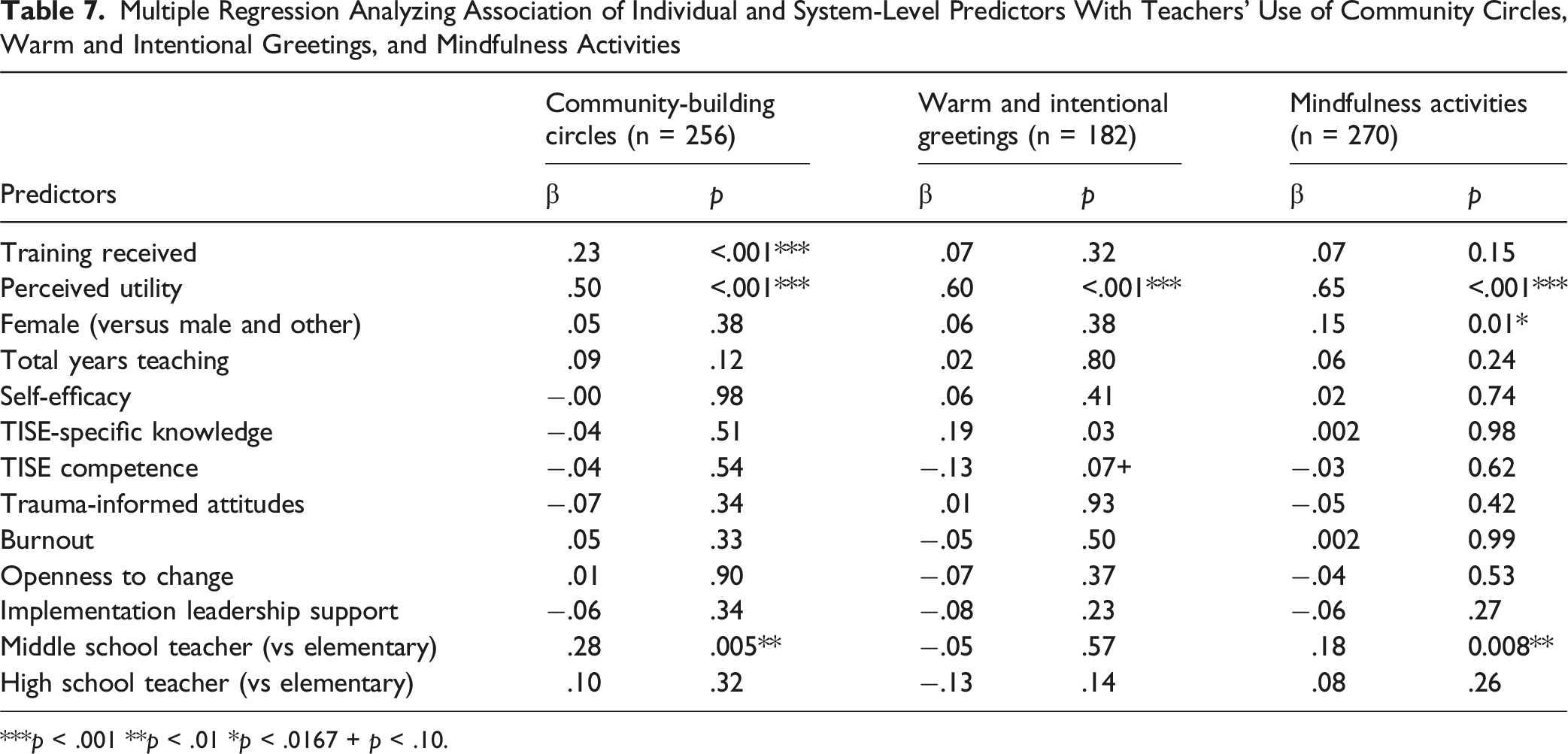
***p < .001 **p < .01 *p < .0167 + p < .10.
Community Circles
The overall fit of the model for community circles was significant (F [13, 214] = 11.63, p < .001, R2 = .44, R2adjusted = .39). Organizational contributors to community circles use included receiving training in the practice (β = .23, t (214) = 3.98, p < .001) and being a middle school teacher as compared to an elementary school teacher (β = .28, t (214) = 2.82, p = .005). The individual factor that contributed to community circle use was perceived utility of the skill (β = .50, t (214) = 8.29, p < .001).
Warm and Intentional Greetings
The overall fit of the model for warm and intentional greetings was significant (F [13, 148] = 8.97, p < .001, R2 = .41, R2adjusted = .38). Organizational factors did not significantly contribute to intentional greeting use. The individual factor that contributed to use of intentional greetings was perceived utility of the skill (β = .60, t [148] = 9.11, p < .001).
Mindfulness Practices
The overall fit of the model for mindfulness was significant (F [13, 222] = 15.72, p < .001, R2 = .48, R2adjusted = .45). The organizational factor that significantly contributed to mindfulness use was teaching middle school compared teaching elementary school (β = .18, t [222] = 2.68, p = .008). Individual factors that contributed to use of mindfulness were perceived utility of the skill (β = .65, t [222] = 12.20, p < .001) and being female (β = .15, t [222] = 2.78, p = .006).
Discussion
The goal of the current study was to provide descriptive information and initial implementation outcomes for a trauma-informed professional development initiative in a large, diverse urban school district. As part of this initiative, the school district focused on developing staff’s trauma awareness and knowledge, and the implementation of three trauma informed practices in classrooms across the first cohort of fifteen elementary, middle, and high schools. To assess feasibility and acceptability of the initiative, we examined overall uptake rates of the TISE training by the entire school staff, and uptake of specific practices by the teachers (i.e., community-building circles, warm and intentional greetings, mindfulness). We also examined the potential role of theoretical drivers of implementation behavior change based on multi-level implementation theories (Aarons et al., 2011; Damschroder et al., 2009; Fixsen et al., 2013) and individual-level focused drivers based on the theory of planned behavior (Eccles et al., 2006; Godin et al., 2008; Sanetti et al., 2013).
The district’s first goal was to ensure that all school district personnel were given the opportunity to acquire foundational knowledge on trauma as it relates to teaching and learning, resiliency building in schools, and how to engage in trauma-informed practices to support students at the school wide and classroom level. The platform used by the district was TISE, a web-based asynchronous training that includes the use of interactive lessons and practical materials (Wong et al., 2024). While there was variability across schools in rates of TISE training participation and completion, it is noteworthy that the district was able to achieve a course completion rate of 82% across the 617 personnel who responded to the survey from 15 schools. This included not only classroom teachers, but student support staff, nurses, administrative and clerical support staff, and others. This was accomplished with minimal mandated professional development time allocation and appears to reflect a strong level of district messaging, buy-in, and support for trauma informed schools. Specifically, the district engaged principals directly, provided live training to implementation team members, and were available for coaching, on-the-ground support, and providing feedback to principals on their school’s progress. Although beyond the scope of the current study, it will be important to unpack the school-by-school variance in the completion rates. Because of the complexities in survey timing and the lack of a comparison condition, we were also unable to reliably examine the direct impact of the course itself on knowledge, attitudes, and behavior change.
With respect to the multivariate predictors of TISE course completion, logistic regression analysis revealed that teachers with higher burnout scores had lower odds of completing the TISE course, and those who perceived a stronger organizational climate and culture had higher odds of completing TISE. The emergence of these two variables as the strongest predictors in our regression analysis is noteworthy. Put simply, if you are burnt out, it may be difficult to find the time or bandwidth to complete an online course. This finding builds on the emergent literature on burnout in school mental health (Holdaway, 2015; Ouellette et al., 2019), which suggests that staff who are overloaded or exhausted are less likely to engage in novel efforts and activities. However, if you are in a healthy work environment characterized by integrity, support, strong academics, and positive morale, you might find it more feasible to complete a course. For example, you may be more motivated to comply with the directive to complete a course because you feel valued, respected, and supported in your position. Or pragmatically, you may have been given the support necessary (e.g., time) required to complete the course during the workday. This is consistent with research on organizational health in education which suggests that schools with better organizational health have more efficacious educators (Mehta et al., 2013). Interestingly, in the present sample, burnout and organizational health were positively correlated, indicating that the more burnt out a staff member felt, the more likely they were to work in a healthy organizational environment. One possible explanation for this relationship is that as school staff experience increased levels of burnout, the school increases their responsiveness to these staff by becoming more protective of their staff and increasing resources. Burned out staff may also unite in solidarity with each other and experience organizational cohesion. Alternatively, depending on the context and staff perceptions about the meaning of work, burnout could reflect a heavy investment and commitment (Suyatno et al., 2022).
The next set of research questions focused on teachers’ use of key practices aligned with trauma informed schools and school district priorities. These include the use of community-building circles, warm and intentional greetings to students, and mindfulness activities. Given the scale and scope of the district’s effort and support structure focused on implementation teams, we were first interested in knowing whether teachers reported that the practice had ever been discussed at their school and then, if they received training in the practice. Because the TISE training itself includes more than three trauma-informed practices, knowing if a practice was being discussed at the school was an indicator that the teachers had some awareness of the expectations around practice application. Except for the discussion of warm and intentional greetings, over 60% of teachers noted each practice had been discussed at their school, and the vast majority noted that they had been provided with training, modeling, or resources to implement. Overall, teachers reported consistently using warm and intentional greetings (63%) and mindfulness activities (56%) more than they did community circles (41%). This ordering is also aligned with teachers’ ratings of each practices’ perceived helpfulness. This is not surprising given their relative ease of use compared to community circles. The pattern in our findings is also aligned with prior research suggesting that teachers are most likely to use those practices that are relatively easy to implement (e.g., Kassab et al., 2023; Washington-Nortey et al., 2023). Of note, practices that are more complex may still be highly impactful for student outcomes. Community-building circles and similar practices are a core component of several evidence-based SEL programs and classroom climate models (Durlak et al., 2024). Their implementation may warrant additional focus and targeting coaching and training to support practice and enhance the perceived benefit. Nonetheless, it is still encouraging that 41% of teachers reported consistent use.
With respect to the multivariate predictors of self-reported practice use among teachers, we found that teachers’ perceived usefulness was consistently associated with more frequent practice use for all three practices. This is not surprising given that perceived utility is highlighted in theoretical models of implementation (Aarons et al., 2011; Damschroder et al., 2009) and has been identified as a predictor in teacher use of practices (Kassab et al., 2023; Washington-Nortey et al., 2023). Interestingly, for community circles, there was also an association between teacher-reported access to the training and modeling and more consistent usage. This makes sense given that community circles are more complex to use, require planning and scheduling, and may require practice. What is also interesting is that utility-related factors emerged as being more consistently associated with practice use in the regressions than other hypothesized implementation factors such as implementation leadership support from principals, perceptions about openness to innovation, and teacher self-efficacy (Aarons & Sommerfeld, 2012; Benjamin Wolk et al., 2015; Lyon et al., 2018). Some of these variables were associated with practice use in our correlational analysis. While these constructs will continue to be important to explore in school-based implementation research, our findings point to the unique role that teacher perceptions about the practice may have.
There are several limitations to the current study, which also have implications for future research. The study provides preliminary evidence of the feasibility and acceptability of a real-world large-scale effort to launch trauma-informed schools in an urban school district. However, because it is a correlational self-report survey study, the results should be interpreted with caution. The lack of a comparison group and data about the specific activities conducted by each school’s implementation team limits our ability to link the TISE training curriculum or the district’s implementation support structures to the specific outcomes reported in this study. Not all staff in the 15 schools responded to the survey. Although our response rate (57%) is in line with or stronger than what might be expected in an online survey with educators (Wu et al., 2022), it may not represent the perspectives of all school staff. In addition, there were complexities in the timeline of survey administration and variability across schools with respect to their implementation structures that was difficult to account for in the current study. Also, like other research on trauma-informed schools (Avery et al., 2021; Maynard et al., 2019), we did not have observational data on classroom or school practices or student outcomes related to their perceptions of the school or their academics. Future research should include randomized control trials or matched control designs and should include additional indicators of successful outcomes. Moreover, while the study used existing measures wherever possible, some of the survey items related to practice use and supports provided to teachers and staff were developed for the current study. This is a strength in that we were able to share feedback with stakeholders using measures with high face validity and feasibility; however, it is also a notable limitation in that our measures may not generalize to others’ efforts. Future research should work towards common metrics or indicators of trauma-informed schools practice change. Finally, the current study took place in the context of a research-practice partnership and represented an effort that was supported by external funding to the district. The school district population and characteristics, and these larger contextual factors may not generalize to other settings. However, it is noteworthy that the district’s commitment and high-level buy-in at the district and school level appears to yield initial success in uptake of trauma-informed systems change.
The current study has practical implications. Efforts to launch trauma informed schools have grown exponentially (Temkin et al., 2021), with little research providing insight into how school districts are structuring their efforts and if these approaches hold promise. The current study contributes to the literature by describing a large-scale implementation support structure that involves training, engagement of leadership, and the use of implementation teams to support practice use by school staff. It also highlights that schools should likely focus on engagement and buy-in, support schools to create a conducive implementation environment, use implementation teams, and ensure that practices are perceived as useful and usable for staff.
Decision-makers should also recognize that the kind of systemic change needed for trauma-informed schools takes intentional and sustained effort (Fullan, 2016). As schools do this work, they must also contend with the burden of multiple initiatives and can experience implementation fatigue, which can impact efforts for sustained and scalable change (Coburn, 2003; Coburn, 2003; Hamilton et al., 2023; Hamilton et al., 2023). Organizational and leadership factors, diverse workforce needs, regulations, mandates, complex funding streams, and the relative cost/benefits must also be considered (Lyon et al., 2024). The district in the current study made efforts to tailor their implementation effort to existing structures, priorities, and initiatives. Districts and schools could benefit from organizational frameworks that can help them do this effectively. Multi-tiered systems of support (MTSS) may be helpful in this context. MTSS is, “an evidence-based model of education that employs data-based problem-solving techniques to integrate academic and behavioral instruction and intervention’’ (Gamm et al., 2012). Typically using three tiers of support focused on prevention, targeted interventions, and intensive interventions, MTSS has been used to varying degrees as a model of trauma-informed schools (Berger, 2019). MTSS provides a structure though which school teams can integrate trauma-informed care with social emotional learning programs, school climate initiatives, classroom strategies, and mental health supports. Future research, practice, and policy efforts should continue to examine implementation strategies and sustainable models for the integration and application of trauma-informed schools.
Integration of a trauma-lens and practices in schools is often discussed, but we have little research that unpacks the processes at work in real world contexts. The current study contributes to the literature by highlighting some of the processes, initial outcomes, and associated implementation factors that may be important in developing trauma informed schools. As the field moves forward, it will be essential to delineate core strategies, indicators of successful implementation, and most importantly the long-term impact on student well-being and academics.
Footnotes
Acknowledgement
We would like to express our deep gratitude to the teachers, administrators, student support staff, and all school personnel who have dedicated their time to this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the funding from the Substance Abuse and Mental Health Services Administration (1H79SM088082 and 1H79SM087194).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.