
Abstract
Use of telehealth for behavioral health services has rapidly expanded with potential to reduce rural health disparities. Applying evidence-based treatments for problematic sexual behavior (PSB) among youth via telehealth can prevent further sexual harm of children. Successful implementation of telehealth in rural communities requires examining the acceptability, understanding, barriers, and facilitators of the approach. Using a qualitative approach, this study explores family and clinician perception of the utility of telehealth to enhance access to PSB cognitive behavioral group treatment (PSB-CBT) services. Results revealed telehealth provided opportunities to address internal (e.g., shame, stigma) and external barriers (e.g., time, transportation, childcare), as well as impact of unique rural communities’ characteristics. Privacy, safety, reduced isolation and shame, and enhanced sense of community among members were noted as benefits of group telehealth, while technology literacy, device accessibility, and group appropriateness were reported obstacles. Strategies to enhance success included telehealth orientation, loaning secure devices, integrated therapeutic activities, focused efforts on building relationships among members, and augmenting with family sessions. Future research on implementation and treatment outcomes of group telehealth for PSB is recommended.
Child Sexual Abuse and Problematic Sexual Behavior of Youth in Rural Communities
Child sexual abuse (CSA) is a global health concern due to its detrimental outcomes across the lifespan. CSA affects millions of youths, with retrospective research reporting one in five women and one in 13 men reported CSA histories (Evans-Thompson et al., 2017; World Health Organization, 2014). Children who have experienced CSA are at increased risk for maladaptive outcomes in adulthood, such as internalizing and externalizing disorders, suicidality, risky sexual behaviors, and intimate partner violence (Guiney et al., 2024).
Determining CSA rates among rural children can be challenging. Menard and Ruback (2003) found higher CSA rates in rural communities, but noted these rates depended on the data source. More recently, Evans-Thompson et al. (2017) found 57% of children referred to a rural-based Child Advocacy Center (CAC) endorsed CSA histories. Among perpetrator types, CSA incidents committed by other youth are estimated to range from 30% to over 70% of all CSA cases (Finkelhor et al., 2009; Gewirtz-Meydan & Finkelhor, 2020), with the peak offending age occurring between 12 and 14 years (Finkelhor et al., 2009). Of child sexual offenses administratively tracked, the offenders were under 18 years for 20–33% of cases (Finkelhor et al., 2009; National Children’s Alliance [NCA], 2021; NSPCC Learning, 2024).
Thus, sexual harm to children is frequently caused by other youths. Broadly, problematic sexual behaviors (PSBs) are defined as behaviors of youth involving touching, looking, or showing sexual body parts that are developmentally inappropriate and can cause harm to other youth or oneself (Allen, 2023; ATSA, 2023). PSB is a pattern of potentially harmful behaviors that can be associated with or are symptoms of behavioral conditions including diagnoses of oppositional defiant disorder, conduct disorder, and attention-deficit/hyperactivity disorder as well as post-traumatic stress disorder (ATSA, 2023; Gray et al., 1999). PSB can have rippling effects on the youth with PSB, the impacted children, family members, and community. These effects must be addressed through evidence-based treatment (EBT) coordinated processes to enhance the well-being of all the children and prevent any further victimization.
Current State of Rural Mental Health Care for Children
Unfortunately, pediatric mental health remains in a state of national emergency (Children’s Hospital Association, 2025), with particularly noteworthy disparities in rural communities. Current estimates indicate that 14%, or 46 million of the U.S. population, reside in rural areas (Dobis et al., 2021), and 6.5 million rural individuals meet criteria for one or more mental health diagnoses (Morales et al., 2020; SAMHSA, 2017; U.S. Census Bureau, 2016). One in six children in the U.S. is diagnosed with a behavioral, mental, or developmental disorder, with approximately 80% of these children living in areas without available mental health services (Cummings et al., 2013; Ros-DeMarize et al., 2021). These rates, compounded with the mental health provider shortage and rising hospital closures, culminate in the public health crisis facing rural communities (Bureau of Health Workforce, 2021; Weinzimmer et al., 2021).
Beyond shortages, numerous social determinants of health affect rural communities’ ability to access quality mental health care. Logistical barriers frequently reported include a lack of childcare, sustainable transportation, and financial constraints (Alegria et al., 2010; Kapke & Gerdes, 2016; Nicasio et al., 2022). Rural communities report more children per household, higher unemployment rates, lower socioeconomic stability, and are more likely to be uninsured than urban communities (Hart et al., 2005; Simmons et al., 2025). Internal barriers, such as feelings of stigma and shame, and lower mental health literacy are often endorsed (Morales et al., 2020; Shields et al., 2018), but have not been thoroughly explored from the rural community perspective. All of these factors can hinder engagement in services, increasing dropout rates.
Use of Telehealth to Reduce Rural Mental Health Care Disparities
Following the COVID-19 pandemic, many practitioners pivoted to telehealth practices to facilitate access to care. Telehealth is a general term encompassing any virtual platform to deliver health services, such as remote patient monitoring or synchronous video conferencing (Cain et al., 2016; Villalobos et al., 2023). A 2021 study reported up to 30% of 16.7 million individuals receiving mental health treatment received care through telehealth (Patel et al., 2021). Pierce et al. (2021) found that therapists rapidly adopted telehealth platforms after the COVID-19 pandemic (7.1% pre-pandemic to 85.5% during the pandemic) to ensure continuity of care. Further, telehealth expansion has seen widespread gains in overcoming traditional barriers. Frye et al. (2022) reported that families engaged in telehealth saved, on average, 132.20 miles of travel round trip and $22.47 dollars per session, while Stewart et al. (2020) reported low dropout rates (11.4%), demonstrating close to 9 out of every 10 youths completed treatment.
Building on this success, telehealth modality may facilitate access to efficacious early interventions for PSB of youth. Successful implementation of these evidence-based treatments (EBTs) can lead to family healing, enhanced child well-being, prevention of additional victimization, and improved community safety (Defending Childhood, 2014; Mundey et al., 2020; Silovsky et al., 2018). EBTs for PSB have been found to yield positive outcomes, with short-term and long-term low recidivism rates, reduced behavioral and trauma symptoms, and enhanced well-being of youth (Borduin et al., 2009, 2021; Carpentier et al., 2006; Mori, 2025; Silovsky et al., 2018, 2025). Unfortunately, EBTs that directly address PSB are not available in many U.S. communities (Dopp et al., 2017). Many states still do not have any teams trained in the EBT (National Center on the Sexual Behavior of Youth, n.d.) leading to recent statewide efforts to enhance availability (e.g., HB4086 Children Exhibiting Complex Sexual Behavior Committee, 2025). Rather than access to EBT, many areas utilize services that have little in common with EBTs for youth with PSB, lack caregiver involvement, and can lead to worsened outcomes for youth (McGrath et al., 2010; National Research Council, 2013).
Telehealth modality could also address barriers that impede families’ ability to engage in evidence-based care. Shields et al. (2020) qualitatively examined family engagement factors affecting retention rates for PSB treatment, identifying delays in receiving treatment, transportation, and childcare, as well as a lack of available services and communication among systems, as significant barriers to care. Other research found that 32% of caregivers reported logistical issues that affected consistent attendance for PSB services (Shields et al., 2018).
North Dakota has notable shortages in mental health providers (Olson, 2023). In 2025, every county except five in North Dakota has been designated as a mental health shortage area (Rural Health Information Hub, n.d.). Recent reports illustrate increasing mental health needs of North Dakota’s children with 23% of youth reported to have at least one mental health condition (The Annie E. Casey Foundation, 2023). Telehealth has been proposed as a strategy to address mental health disparities in rural and frontier communities, such as North Dakota (Center for Social Research, 2023). In response, the North Dakota Telehealth Outreach Program was developed and has systematically worked on telehealth applications for EBTs to increase access to care (Telehealth Outreach Program. n.d.).
When investigating outcomes of telehealth-delivered EBTs, findings have been comparable to those of in-person services. Both Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) and Parent-Child Interactive Therapy (PCIT) have shown positive outcomes, comparable to in-person services (Comer et al., 2021; Nicasio et al., 2022; Ros-DeMarize et al., 2021). Stewart et al. (2020) found 98.6% of the sample no longer met posttraumatic stress disorder criteria after completing telehealth-delivered TF-CBT and one-third of the participants resided in rural areas. One intent-to-treat randomized controlled trial (RCT) of internet-delivered PCIT (I-PCIT) found that 70% of children responded to treatment, compared with 55% for in-person PCIT groups (Comer et al., 2017). While child-focused, telehealth-delivered EBTs consistently demonstrate they can be successfully adapted, research finds rural communities experience obstacles less likely in urban areas, such as lack adequate technological literacy, including acceptability and utilization of telehealth services when available (AkaEze & Nwachukwu, 2025). These obstacles are compounded by addressing sensitive topics, such as PSBs, in rural communities, and the nuances of confidentiality when attempting implementation of telehealth EBTs must be examined for successful adoption of services.
Group-Based PSB-CBT Overview and Research
PSB treatment outcome research has suggested that quality EBTs are short-term, community-based, and involve direct caregiver involvement (Letourneau et al., 2013). One model for PSB, Problematic Sexual Behavior-Cognitive Behavioral Therapy (PSB-CBT™), has been identified as having rigorous scientific support (Dopp et al., 2015). The PSB-CBT model is a family-oriented, CBT intervention model aimed at eliminating or reducing PSB recidivism, reducing behavioral or trauma symptoms, decreasing justice involvement, increasing social skills, improving child-caregiver relationships, and improving parenting skills (Simmons et al., 2025; Theimer et al., 2023). Carpentier et al.’s (2006) ten-year follow-up results found recidivism rates of youth who engaged in PSB-CBT to be 2-3% and significantly lower than those in a comparison play therapy group condition (10% recidivism). Multi-site research implementing PSB-CBT group therapy found a large effect size for reducing PSB (t(126) = 11.69, p < .001, d = 2.08; Silovsky et al., 2018, 2025). Positive findings have been replicated in Canada (Mori et al., 2025) and the United Kingdom (Barry & Harris, 2019). Not only are outcomes promising, but PSB-CBT group therapy is cost-effective and has positive impacts on the community (Dopp et al., 2020; Mundey et al., 2020).
In response to the need to address service gaps in North Dakota, PSB-CBT group therapy has been adapted for telehealth for implementation in rural areas (Simmons et al., 2025). These group services have been provided to youth across North Dakota for over 6 years, most of whom otherwise would not have access to services (P. Condol & N. Herting, personal communication, September 27, 2023). Moreover, telehealth PSB-CBT has been successfully adopted in urban areas (e.g., Chicago, Atlanta), with positive outcomes (Silovsky et al., 2025).
While urban communities may experience similar challenges, barriers among rural communities are more often pronounced and complex, where limited anonymity, stigma, and strong close-knit social networks are likely to negatively impact ability or willingness to engage in services. Lack of available services for serious behavior concerns, such as PSB, in rural communities is a major concern and warrants unique strategies to reduce future sexual victimization (Russell et al., 2025). Given positive results of the telehealth application of pediatric EBTs and the success in implementing PSB-CBT, research examining the application of PSB-CBT group therapy via telehealth to reduce the more nuanced rural disparities is warranted. Studying the acceptability, utility, barriers and facilitators of the use of telehealth for this sensitive topic is a key next step to assess this approach to reduce rural disparities in EBT for PSB. The perspectives of rural families (caregivers and youth) and of clinicians providing telehealth group PSB-CBT across a rural and frontier state captures the lived experiences to best investigate the use of telehealth in this area. This study sought to provide an initial step toward identifying unique and universal factors, barriers, and perceptions that may affect rural families’ engagement in telehealth-based PSB services through focus group interviews with caregivers, youth, and clinicians.
Method
Study Design
In the present study, we conducted focus groups in North Dakota with caregivers (two focus groups, n = 8), youth (two focus groups, n = 8), and clinicians (one focus group, n = 6). All participants included in the study were actively participating in telehealth PSB-CBT group treatment services. Semi-structured focus group interview guides were designed to obtain in-depth information about participants’ perceptions and experiences with group-based mental health PSB services delivered via a telehealth platform.
Participants
All participants were recruited through Child Advocacy Centers (CACs) in North Dakota. These agencies were identified as ideal candidates for the study due to North Dakota CAC’s extensive history of using telehealth as the primary delivery system for EBTs. All participants were actively engaged in group PSB-CBT telehealth services at the time of the focus groups.
Age of youth who participated in the focus group(s) ranged from 8 to 15 years old (M = 11.75, SD = 2.32); all youth identified as male. Youth race/ethnicity was white (62.5%), Native American (12.5%), Hispanic heritage (12.5%), and one youth preferred not to answer (12.5%). Caregivers in the focus groups were predominantly female (62.5%) and were married or in a long-term partnership (75%). All families had been referred to CACs for PSB treatment. Clinicians providing PSB-CBT group services via telehealth were also recruited for the study. Majority of clinicians reported having a Master’s degree (66.7%) and two participants were clinical interns. All clinicians received specialized training in providing telehealth before conducting the PSB-CBT telehealth group; two-thirds (66.7%) of participants had less than a year of experience with telehealth for mental health services.
Measures
Semi-Structured Focus Group Interview Guide
The qualitative research team developed a semi-structured focus group interview guide to gain a foundational understanding of caregivers’, youth’s, and clinicians’ experiences and perceptions of mental health services for PSB. Caregivers and youth were asked open-ended questions to explore topics including barriers and benefits of telehealth, the effectiveness of group treatment via telehealth, perceptions of therapy, and the use of telehealth platforms to discuss sensitive topics (e.g., PSB histories). Clinicians were asked open-ended questions about perceived barriers and benefits of telehealth for rural communities, difficulties in implementing telehealth, group management, engagement strategies, and lessons learned. For each group, participants were asked to discuss both positive and negative perceptions or experiences they had during telehealth treatment.
Procedures
The University’s Institutional Review Board approved all procedures before implementation of the study. The CACs leadership reviewed and approved all procedures, deferring to the University’s IRB as they did not have an independent IRB established.
Focus Group Procedures
Caregiver and youth participants were recruited through flyers distributed by clinical personnel to families actively participating in group telehealth services at North Dakota CACs. The flyer indicated that the project was recruiting caregivers and youth to share their experiences with telehealth for treatment. If interested in participating, each family was invited to attend their respective focus groups. At the onset of each focus group, the researchers reviewed the purpose, participation, and confidentiality, including that their individual responses would not be disclosed to their respective agencies. Electronic documentation of consent and assent was completed via secure links using the REDCap platform. After caregivers’ consent and the youth’s assent were established, a short demographic form was completed. The caregivers, youth, and clinicians met separately in each focus group, led by two teams of researchers. Each focus group lasted approximately 1 hour on a HIPAA-compliant platform (i.e., Zoom), which was recorded and transcribed. Each transcript was downloaded from the Zoom platform. Two research team members reviewed each transcript while observing the recordings to ensure each transcript captured the discussion accurately.
Qualitative Coding of the Data
Reflexive thematic analysis (Braun & Clarke, 2006) guided the qualitative analyses to generate themes related to services for PSB of youth and the use of telehealth. Reflexive thematic analysis was selected because it integrates themes while considering how the researchers’ perspectives, assumptions, and interactions with the data shape the themes that emerge. Each author reviewed all transcripts independently for familiarization and noted themes and findings that emerged within and across participant groups. The coding process was iterative and emerged from themes in the data, rather than using a pre-developed codebook. The research team met to discuss themes for each participant group separately, developed lists of themes, and then met to examine themes across each participant group. The goal was to identify the themes that best captured and reflected the story told by the data. Interestingly, the themes that emerged resonated across all three participant groups, though the clinicians provided more detail on the clinical decision-making theme. The research team brought their own experience and knowledge related to PSB, trauma, services, and telehealth to the analysis of participants’ responses (experiences of the team members included education, training, and research in child development, trauma, maltreatment, and multiple EBTs; direct in person and telehealth clinical services for child PSB, disruptive behaviors; direct activities and collaborations with multidisciplinary teams).
The research team utilized a reflexive thematic analysis framework and a constructivist approach to epistemology (Hughes, 2014). Analyses procedures recognized our research team’s respective backgrounds in research, clinical, and personal perspectives impact on data interpretation. Throughout coding and theme development, the team engaged in ongoing reflexive discussions regarding assumptions, potential biases, and interpretations with attention to how each researcher’s experience and prior knowledge may influence analytic decisions. These multiple in-depth discussions occurred at all stages of analysis (coding, theme generation, drafting the narrative summation of findings) to ensure their interpretations were grounded in the data.
Results
Overall Themes Among Rural Focus Groups
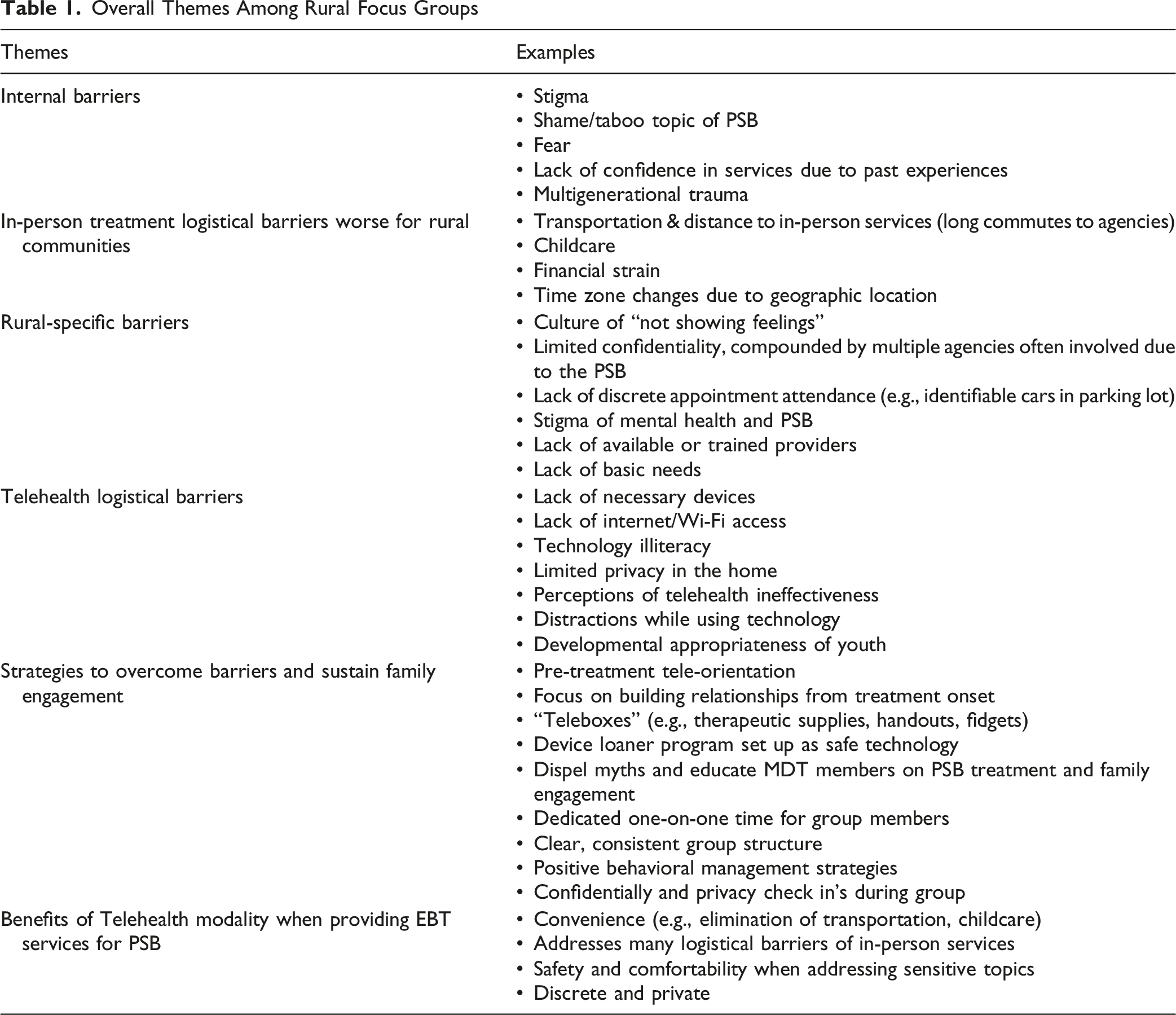
Barriers: Internal, External, and Impact of Rural Culture and Community Characteristics
Participants across all three reporter types (youth, caregiver, and clinician) emphasized experiencing or expressing feelings of stigma/shame and taboo nature of PSB, as significant barriers when families initially engage in services. For example, one clinician shared, “Even in the context of PSB or like sexual abuse, it’s just so taboo. A lot of people don’t want to talk about it. And there’s that stigma against the taboo things” All participant types identified families feeling guarded at the onset of services, noting that in rural communities, discussing and showing emotions is not acceptable. One caregiver stated, “You just hide it. That’s the way I was raised… You hide your feelings, like you’re fine… that’s how I was raised.” This was echoed by a youth “Never talk about it, never anything, just hide it. That’s the way I was raised.”
Interestingly, caregivers and clinicians both highlighted perceptions of power dynamics and the family’s previous experiences within the rural communities and service agencies (e.g., law enforcement, child protective services, juvenile services) as barriers to service engagement. Families receiving PSB services are often referred to or even mandated by local and state agencies. Caregivers and clinicians noted that poor interactions with agency systems before beginning services can cause families to enter therapy with negative expectations and an initial lack of genuine internal motivation and commitment. One clinician noted, “Sometimes I think caregivers are angry with other systems…so [caregivers] being let down by other systems creates barriers or challenges.” Negative past experiences in therapy also hinder initial engagement in mental health treatment, for example, one caregiver noted, “I’ve also had very horrible… horrible experiences with therapy. So…I’m okay with him doing it…But you know, I also am scared of it.”
Among the barriers expressed, unique themes emerged specific to rural communities of limited resources, culture (e.g., everyone knows each other, family and religious values), and the impact of multigenerational/historical trauma. Unsurprisingly, lack of trained and available providers with specialized training to address PSB was endorsed by the caregivers and clinicians. A clinician noted, “Another barrier is a lack of trained providers in our area, or clinicians to do group [therapy]. So training more people, I think, could overcome a lot of barriers as well.” Participants reported inadequate internet access as a common barrier in rural areas. Perhaps the most illuminating point identified by all groups was the lack of privacy and confidentiality in rural communities. One clinician shared, “Small communities operate like they kind of feel like they’re always knowing what’s up and are the talk of the town… like everyone knows everyone and everything about everyone sometimes.” One youth shared, “It kind of feels weird, you just met these people and you can’t really trust them… you don’t really want to share any private information with them…they could start sharing with other people that could start being posted all over the world.” Participants also noted strong religious and unique cultural values as factors impacting engagement in their rural communities. One clinician shared, “Culture and religion can affect treatment. Sometimes you have clients who don’t want to open up…They [youth] say in my family it’s not okay to cry, we don’t talk about our feelings.” Multi-generational trauma, particularly related to sexual abuse, was reported to influence pre-treatment perceptions. “I grew up in a very abusive, physically abusive, mentally abusive home… and my child went through something similar, so I would rather him get through it [treatment] and work through it.” Many families must navigate requirements and expectations across multiple agencies (e.g., juvenile probation) which can cause the family unit to be in crisis. Both caregivers and clinicians both reflected this sense of crisis as a significant barrier to active participation.
Unaddressed basic needs and lack of community support (e.g., extended family, neighbors) who could provide assistance (e.g., childcare during services) caused significant strain for many participants. “Supervision of childcare, especially if there is not a lot of natural supports in the home or outside the home or community, even… it can be challenging [for families],” one clinician shared.
Barriers to In-Person Services Among Rural Communities
Participants identified multiple barriers they would face if only in-person services were available, including time, transportation, location, and costs. Most notable among the groups was the time needed to travel from their communities to agencies for in-person services. Long commutes were discussed, particularly their added stress on caregiver work responsibilities and family finances. When asked how telehealth impacted their commute, one caregiver shared, “…where I live [town] is 3 hours from here.” Another caregiver noted, “The time zone change, if it’s four o’clock down that way [CAC location], I would have to leave at one o’clock from my house to go over that way.”
Telehealth Benefits for Enhancing Engagement and Overcoming Barriers in Rural Areas
All participant groups shared the ability to be seen via telehealth overcame numerous logistical barriers, such as transportation, time to and from appointments, and childcare burdens commonly reported as in-person barriers. Beyond logistics, all groups described a sense of safety from participating in services from home. Telehealth was frequently described as promoting a “safe space” and enhancing a sense of privacy when discussing uncomfortable topics in both caregiver and youth groups. One caregiver noted, “You’re not comfortable. You’re already in that tense, tight kind of feeling when you walk in [in-person services], and then you don’t want to say the wrong thing while you’re in their office, you know…. yeah, I feel like I’m more me while I’m home.” One youth shared, “What I like about [telehealth] is I don’t have to be in person ‘cause I get nervous sometimes [discussing PSB].” A clinician emphasized privacy, stating, “Telehealth is nice because it is discreet, more discreet than going into an office or having to take off two hours of school or work for travel and people asking where they go every week.”
Barriers to Engagement Among Rural Participants in Telehealth Group Services
Telehealth was not without barriers. Participants reported an initial hesitancy to use telehealth for treatment or a lack of technology literacy in rural communities as barriers to effective engagement in telehealth at the onset of services. One caregiver stated, “I have the computer skills of a wet paper towel. So you know, getting things turned on… is difficult. But it is worth it, and I mean anything worth doing generally is difficult.”
Per PSB-CBT treatment requirements, caregivers and youth must have separate devices and be in separate rooms to participate in group services. If the program did not have a technology loaner program, access to necessary devices and privacy concerns were noted as barriers across all participant types. Prior misconceptions about telehealth treatment were also highlighted. One caregiver shared, “Before I found out that this was all telehealth, I was very against it. I didn’t think telehealth would actually be meaningful.”
Considerations of the length of the group and the developmental appropriateness of telehealth were expressed. A caregiver shared, “It’s more about my child’s ability to sit still and pay attention for that long.” Clinicians highlighted, “One thing we discussed recently that makes doing therapy on Zoom challenging in group is we have a lot of kiddos with ADHD, some with Autism diagnosis, and it’s challenging to get them engaged and sit still long enough to actually be able to absorb the material during session.”
Engagement Strategies to Overcome Barriers for Rural Families
Themes on strategies to facilitate understanding and engagement in telehealth services were notable. All participant types shared the importance of engagement strategies and dedicating time to the family before initiating group services. Topics for this one-on-one time with the families included orienting to therapy, orientation to the technology, case management, and resource provision. Due to the sensitive nature of the referral, many emphasized the need for time to develop relationships, validation, genuineness, and empathy, and displaying respect in initial interactions.
Implementation of a technology orientation, described as a “tele-orientation,” was a critical strategy for new families. Creating a tech-loaner program for families lacking internet-capable devices was noted as a significant burden lifted from caregivers’ many responsibilities. Alongside assessing for device and internet access, implementing a screener addressing logistical barriers for the family was recommended to identify potential barriers to service engagement. One clinician shared, “We go over the treatment of what’s expected… We review when the group is, how long, a lot of logistical things…and then for people who have never done telehealth therapy, it [orientation] allows them to log in with less people.” Additionally, it was noted that clinicians must evaluate the youth’s electronic or online sexual behavior (EOSB) histories, provide education on equipment supervision and rules, and then use devices approved and monitored by the treatment agency to ensure safe use. A clinician noted, “Being able to provide them [families] with technology, especially for PSB groups. You worry that they’ll be on other sites and maybe their PSB involves technology… so being able to provide them with safe technology seems to be helpful [in reducing barriers].”
Outside direct work with families, clinicians reflected that misconceptions and myths regarding PSBs and treatment outcomes held by multidisciplinary team (MDT) members (e.g., juvenile justice professionals, law enforcement, pediatricians, social workers) hindered families’ motivation to engage in treatment. One clinician shared, “I think that’s a lot of the time, like however treatment was presented to the family, then it’s already setting us up for failure sometimes. If we take the time and educate our team members (MDT members) on what the treatment is and what it should look like, and what they should be saying to families…that will overcome that barrier.” Education of agency partners in the community about PSB in youth was recommended.
Dedicated time for one-on-one sessions with families and clinicians outside of the group was reported as important for engagement. One caregiver noted, “The people, the counselors themselves, have been really…great. They stay after the group to talk privately, or if we need assistance or anything…It’s been really nice that they’ve made themselves available for any help.” Families may come into treatment with previous negative experiences, which can be misconstrued as defensive or disengaged. One clinician reflected, “as [clinician participant] was saying about sometimes clients coming off as defensive, I think sometimes they’re [families] new to this process right? Sometimes they’ve never done therapy before, they don’t know what to expect. I think it’s very important starting off by validating those feelings and addressing those feelings of being uncomfortable.”
Setting expectations and treatment structure for telehealth groups, such as setting rules similar to in-person services (e.g., being in a private space), limiting distractions (e.g., using a space with no TV), and incorporating behavior charts was noted as important. The youth participants had varied views of distractions during telehealth. One youth reported finding telehealth helpful because it reduces distractions, while another reported that some youth take advantage of the platform’s special features, which can be distracting. Caregivers and youth shared that incorporating interactive activities (e.g., games, videos) and visual materials during the telehealth sessions enhanced engagement. Implementation of group activities to achieve therapeutic impact and to avoid an atmosphere of a “class” was noted. Provision of “Teleboxes” (mailed boxes that include supplies for therapy, including workbooks of handouts, headphones, fidgets, reinforcers) was identified as extremely helpful for engaging families and providing a similar experience to in-person services.
Lastly, participants noted privacy and confidentiality check-ins and rule reviews facilitated a sense of safety and promoted understanding requirements for therapy (e.g., privacy, focused attention). Some caregivers were noted to initially not understand telehealth sessions “like almost like it isn’t always treated like it’s a separate appointment, … Like a phone call during a break at work.” Setting limits and expectations and reviewing group etiquette were noted as important to keep the group focused on therapeutic activities. Youth voice noted the importance of pacing and not getting stuck on one topic. Check-ins with caregivers to praise youth progress and dedicated time for family sessions were highlighted as important factors that facilitate stronger family connections.
Logistical Strategies for Clinicians Utilizing Telehealth in Rural Communities
Clinicians shared lessons learned and strategies they believe make telehealth group services successful. A “pre-planning” stage was recommended before launching the telehealth clinical program to review and select a telehealth platform that has appropriate control settings, chat functions, and to educate all clinicians on how to operate it. Flexibility and having a co-facilitator to manage children with behavior problems and a team member who can troubleshoot any technical issues were viewed as critical for success and maintaining the flow of the group session.
Benefits of Telehealth Modality When Providing EBT Services for PSB
Consistently, clinicians, caregivers, and youths noted that the most impactful aspect of participating in virtual group therapy was hearing and learning from others dealing with similar sensitive issues. Caregivers and youth reported feeling less isolation, shame, and judgment from their group members and a new sense of community, a sense echoed by clinicians. One youth stated, “I thought I was going to be judged and all that but in reality, we are all there for something similar. Nobody’s going to judge you.” A caregiver shared, “Coming into [therapy], I was a little worried the things I was going through were just me, but…knowing that other people are going through similar things with their children definitely helps. It’s kind of an ease of mind, letting me know that there’s things we can work through and get past and we can overcome.” A unique theme identified was related to the open group format, and that having group members at different points in treatment inspired hope as members graduate from the treatment program. A caregiver shared, “Participation is key. If you don’t participate, you don’t get the full grasp of all of it… Before they [previous group members] graduated, they opened up to me about why they were there. I felt like that [participation] helped me be able to share with them.”
Caregivers and youth reported that being part of a group enhanced their ability to express feelings, manage their own/child’s coping, relationship skills, and that getting advice directly from group members. Creating friendships, feeling connected, and sharing advice among members was noted by multiple participants. When asked by the interviewer what makes discussing sensitive topics easier, a youth shared, “Cause I’m not alone.” Youth also reported that the group aspect enhanced accountability and a desire to maintain healthy sexual boundaries. “There are other people that…have similar problems [PSB]. So I can give advice, and you can give them advice…It’s just stuff like, I'm not the only one with stuff like that [PSB].”
Discussion
The results provide insights in strategies to reduce mental health disparities in rural communities through telehealth group services designed to prevent child sexual abuse (CSA) by targeting problematic sexual behaviors (PSBs) among youth. The group telehealth approach is designed to increase access, reduce stigma, shame, and isolation in rural communities during the implementation of PSB-CBT to eliminate PSB, enhance behavior and emotional well-being, and facilitate healthy relationships. The current study examined implementation barriers, facilitators and acceptability of telehealth services for PSB through the lived experiences of caregivers, youth, and clinicians in North Dakota. This work helps to fill a gap in the research literature by identifying factors that can impact treatment engagement among underserved rural communities. Results highlight unique considerations when implementing telehealth in rural communities and the benefits of telehealth when specific strategies to facilitate its success are applied to address internal and logistical barriers.
Families shared that sexual violence and specifically youths’ PSBs, and related traumas is surrounded by a sense of stigma and shame, causing isolation and seclusion consistent with previous research (e.g., Shields et al., 2018; Yoder & Brown, 2015). Living in isolated rural communities compounded these concerns, noting heightened challenges to confidentiality when everyone knows each other, lack of acceptability of mental health services, and the culture where vulnerability can be scrutinized. The healing aspects of creating community, being connected, and knowing others with PSB histories was highlighted by the youth, caregivers, and clinician in the current study. Thus, the group aspect of services appears important for families’ healing.
Prior to the availability of telehealth groups, members in rural communities often did not have access to group services due to not having enough local families to form a group as well as due to confidentiality and privacy concerns. When telehealth group programs serve a larger region (in this case statewide), families in small communities can experience the power of group and access trained clinicians all while reducing privacy concerns. Clinicians implementing telehealth groups will need to proactively integrate strategies that facilitate connection among caregivers and youth group members (Simmons et al., 2025). Deliberately exploring commonalities, providing a safe space to share struggles, and encouraging support and advice among members can enhance interpersonal connections. Care must be taken to avoid creating a “classroom” atmosphere and instead maintain the therapeutic approaches.
Telehealth was viewed as having multiple advantages to reduce barriers of in person therapy sessions in rural communities. In person service barriers of financial burden (e.g., gas), transportation, time, impact of time zone change, childcare, and other logistics described in these rural communities were found to be even more pronounced (e.g., three-hour commutes) than previous research (e.g., Frye et al., 2022; Stewart et al., 2020).
A unique way telehealth was recognized as facilitating engagement in services was how it allowed addressing “uncomfortable topics in the comfort of the home.” Talking about the youths’ PSB and related topics is quite personal, sensitive, and anxiety-provoking. Beyond the stigma of mental health overall, the issues of PSB of youth brings added burden. Programs providing telehealth may want to consider how to more deliberately lean into comfort in the home. The process of identifying safe places in the home during sessions can be integrated in the orientation of services. It is important to also note that not everyone feels safe in their own home nor have clear areas of privacy. Integrating discussions about safety and well-being in the home, including case management, is key.
Successful implementation of telehealth for PSB of youth in rural communities requires consideration of heightened technology barriers. Our results found limited access to technology (e.g., electronic devices, Wi-Fi) and concerns about technology literacy and acceptability as barriers, consistent with research in rural communities (AkaEze & Nwachukwu, 2025). Successful implementation of telehealth programs serving rural communities require integrating strategies to address access (e.g., technology loaner programs) and integrate methods to build knowledge and comfort in the use of technology for mental health services. Orientation sessions and technology support built in throughout services were noted as benefits.
In addition to safety considerations, telehealth sessions and treatment materials need to support active engagement, emotional safety, privacy, and community connection. The youth participants indicated how important the use of therapeutic activities is to help with their attention and focus. Recommendations noted in the literature have included using visual supports (e.g., Power Points, Google Slides, brief videos), creating games to encourage participation and reduce anxiety, using platforms that allow direct participation (e.g., whiteboard, chat features), including culturally relevant activities, and integrating visual charts to reinforce active participation and appropriate behavior (Geary et al., 2011; Simmons et al., 2025).
Specific and careful consideration of online safety are required when applying these promising results to group telehealth to address PSB of youth as a modality to prevent CSA and enhance family well-being (Simmons et al., 2025). PSB among youth is increasingly shaped by and expressed in the digital environment. Youth are exposed to sexually explicit media at younger ages, and this exposure impacts their own behavior. Caution is required when the modality of therapy is in the digital environment, potentially increasing the risk of youth access to sexually explicit media. Clinicians, caregivers, and youth shared the importance of safety planning, technology orientation, and control of any devices used for telehealth therapy. A device loaner program facilitated agency-controlled restriction of devices for participants’ safety as well as provided access for families without sufficient technology.
Families are frequently referred or mandated to services to address PSB of youth by public agencies (e.g., child protective services, juvenile justice). Results uncovered how previous negative experiences (e.g., threats, fears, misinformation) experiences with these systems and the process of referral interfered with therapeutic engagement. The clinician participants noted the importance of educating the community professionals to improve engagement by dispelling myths and replacing these with accurate information about youth with PSB, vulnerabilities and protective factors, and the impact of treatment. As often the first contacts with families when PSB of youth is identified, such public agencies are in a distinct position to provide the family with the messages of seriousness and hope. By sharing their role in keeping all children safe, how the recent behavior is unsafe, and how the family’s participation in therapeutic services can facilitate well-being, the professional is supporting motivation to follow up with services (Taylor et al., 2023). Additionally, these community partners may have hesitations regarding the impact of telehealth services, particularly how well the modality can engage and impact youth. When educating MDT partners about treatment via telehealth may benefit from addressing safety procedures, therapeutic processes, as well as treatment impact.
Limitations and Future Directions
This study represents an initial exploration of youth, caregiver, and clinician lived experiences with group telehealth to address PSB of youth. Characteristics of this specific sample must be considered when interpreting the findings. The youth participants in this study all identified as male. Although the vast majority of teenagers with PSB are male, females are not uncommon samples of 7–12-year-olds with PSB (Allen, 2023; Friedrich et al., 2001). Further, while the sample was representative of North Dakota’s population in terms of race and ethnicity, the lived experiences of Black, Asian, and other cultural groups require additional research. Further, all participants were involved in the same program, in North Dakota, and the groups included clinicians and family members who were relatively recent to the program. Follow up studies of additional populations can enrich understanding of themes that are both universal and unique to specific rural communities. Capturing the insights of families who were referred for services but failed to engage could elucidate additional barriers and notably is a particularly challenging population to engage in research. Additionally, the authors opted to utilize focus groups to facilitate the process of the members ability to express beliefs, perceptions, and recommendations in a manner that facilitates connections to ideas and deeper discussion (Onwuegbuzie et al., 2009). However, by not using an individual interview format, some unique messaging may have been missed, and future research would benefit from allowing individual time for each participant. Given the concerns raised about families’ previous experiences with agencies and services, expanding research on perspectives of key professionals in the rural communities (e.g., child protective services, law enforcement, schools) on telehealth and PSB is recommended.
Direct evaluation of outcomes of group telehealth services to address PSB of youth are needed. Similar programs of research examining telehealth outcomes for TF-CBT and PCIT (Comer et al., 2021; Nicasio et al., 2022; Ros-DeMarize et al., 2021) are quite promising for the impact of EBT through the telehealth modality. Treatment outcome research on group CBT for PSB of youth via telehealth is a critical next step, examining impact not only on future PSB, but also impact on co-occurring issues (e.g., trauma and general behavior problems) as well as vulnerability and protective factors (e.g., parental stress, support, and behavioral management skills). Assessment of PSB types should include electronic and online sexual behaviors and interpersonal in-person PSB (Allen et al., 2026). Testing telehealth strategies to facilitate engagement and impact with youth who have developmental or behavioral challenges, similar to work being conducted with TF-CBT is warranted (McDonnell et al., 2026).
Conclusions
In summary, telehealth group treatment for PSB of youth has great potential for preventing CSA across rural communities. Findings support telehealth to reduce barriers across internal, logistical, and clinical factors associated with rural areas. While promising, further research on telehealth implementation of PSB-CBT and similar programs is needed to examine engagement, barriers, and treatment outcomes with diverse and special populations.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Oklahoma Children’s Health Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.