
Abstract
Filgrastim and pegfilgrastim are granulocyte colony-stimulating factor products, which have been part of the supportive treatment of cancer patients for years to increase the white blood cell count and absolute neutrophil count with the objective of preventing neutropenic fever in patients at risk because of chemotherapy. Pegfilgrastim is a glycosylated form of filgrastim with a prolonged duration of effect, a reduced renal clearance, and relatively fewer side effects. We present a patient with early breast cancer who developed a rash more than a week after the use of pegfilgrastim. Clinicians must be aware of the possibility of a delayed hypersensitivity reaction as the application of this drug is increasing and an adverse event can result in delay of chemotherapy treatment.
Introduction
Pegylated granulocyte colony-stimulating factor (G-CSF) (pegfilgrastim (Neulasta®, Amgen)) is a covalent conjugate of recombinant human G-CSF and monomethoxypolyethyene glycol. While regular G-CSF (filgrastim) has a half-life of 3–4 1 h, pegfilgrastim with its reduced renal clearance and consequent prolonged persistence in vivo has a half-life of 15–80 h. 2 This allows it to be administered as a single subcutaneous injection once per cycle of chemotherapy. It is being used increasingly in oncology as a simple and cost-effective means of maintaining adequate neutrophil levels during intensive combination chemotherapy.
There have been few case reports describing dermatological reactions to filgrastim3–5 and even fewer case reports to pegfilgrastim.6–9 On review of the literature, we found three case reports describing an immediate type hypersensitivity reaction occurring within a day of receiving pegfilgrastim.6–8 Another reports biopsy-proven Sweet syndrome (also known as acute febrile neutrophilic dermatosis—a rare skin condition marked by fever and painful skin lesions) within 3 days of administration. Lastly, there is also a case report with biopsy-proven pyoderma gangrenosum within 3 days of administration. 9
To our knowledge this is the first biopsy-proven case report with a delayed type IV dermatological reaction after the administration of pegfilgrastim.
Case
Informed consent was obtained from the patient to report this case and present accompanying photographs.
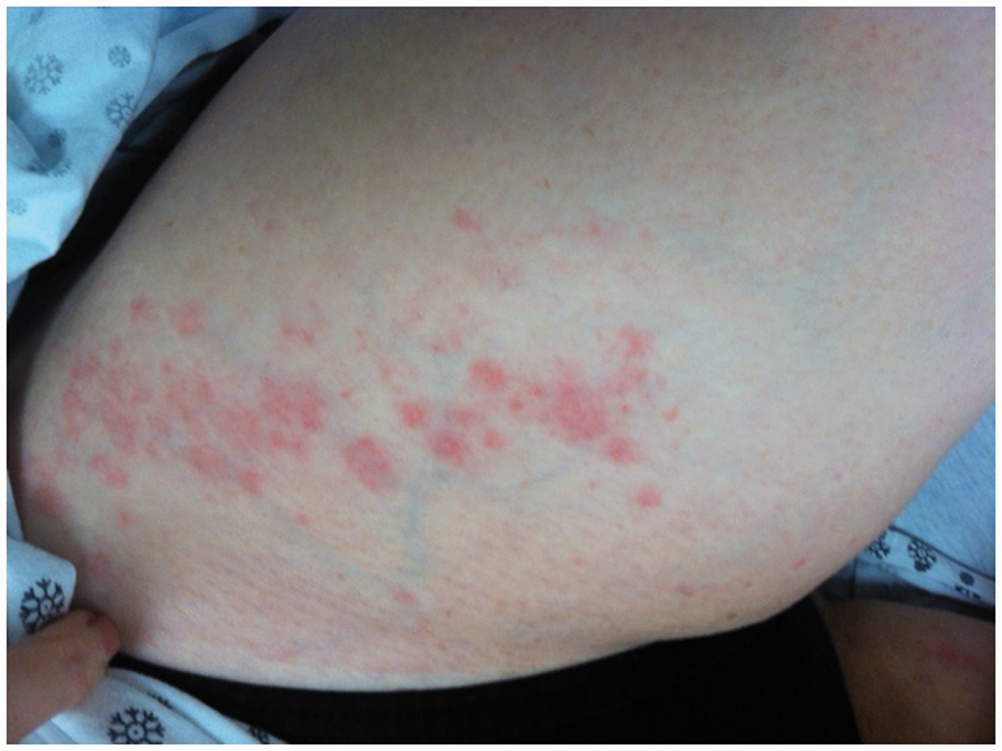
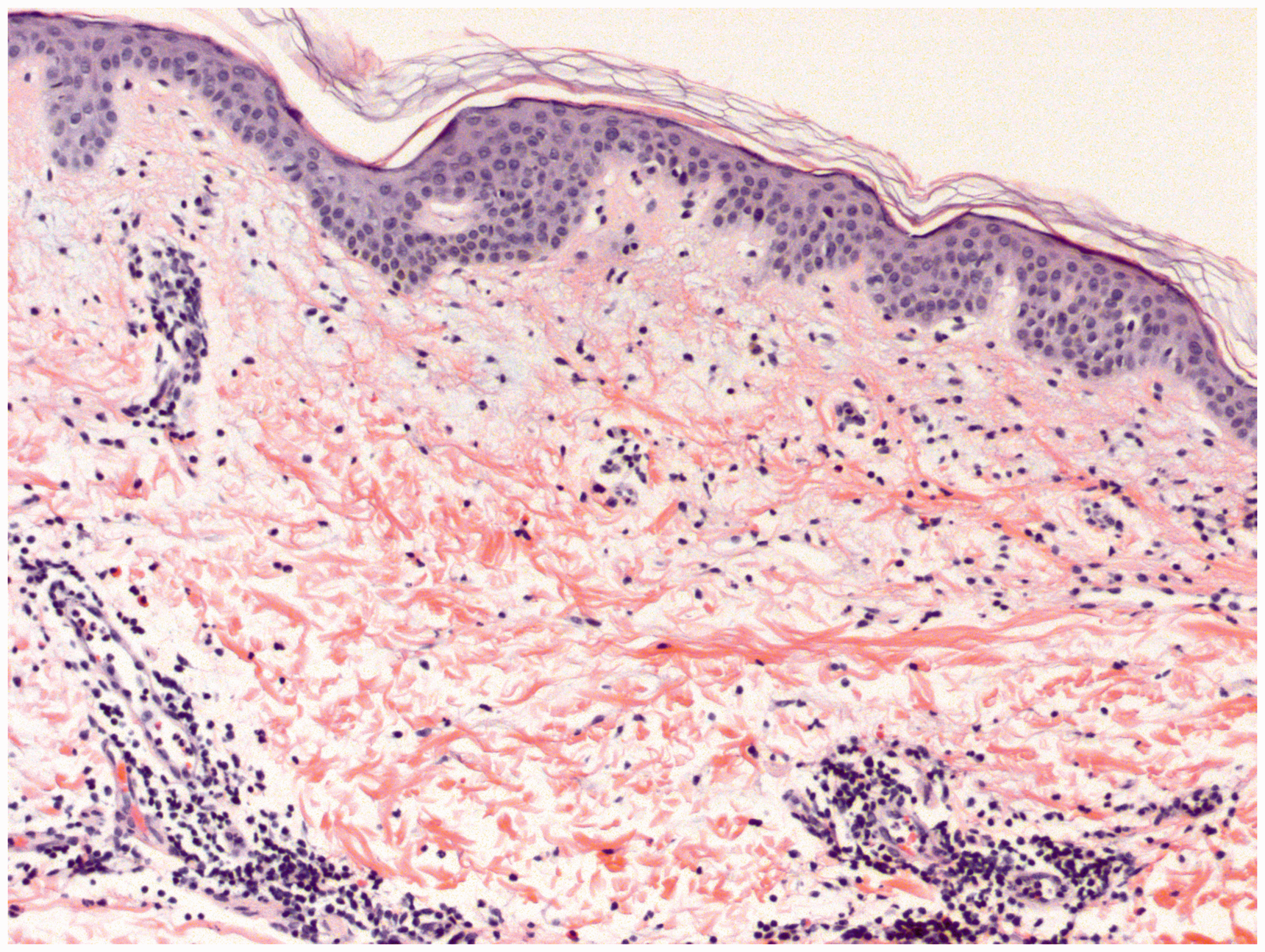
We present the case of a 52-year-old Caucasian woman with a T1bN0 infiltrating ductal carcinoma of the right breast, which was estrogen receptor- and progesterone receptor-positive, HER2 (Human epidermal growth factor receptor 2)/neu negative with a high-intermediate Oncotype Dx® (Genomic Health) score of 27. She received her first cycle of chemotherapy with docetaxel 75 mg/m2 and cyclophosphamide 600 mg/m2 intravenously on day 1 (TC) followed by day 2 pegfilgrastim 6 mg subcutaneously, and did well. The patient was scheduled to receive this regimen once every 3 weeks. Concurrent medications were valacyclovir, multivitamin, vitamin C, vitamin D, probiotic, senokot, and lorazepam (as needed). Eight days after her 2nd cycle of chemotherapy (TC (same doses day 1) + day 2 pegfilgrastim), the patient developed minimal rash on her arms and abdomen as well as a sore throat, which was self-limiting. The same occurred again 8 days after the 3rd cycle of chemotherapy (TC (same doses day 1) + day 2 pegfilgrastim) when the patient developed a sore throat. On day 9 after the 3rd cycle, the patient developed a rash on her face, scalp, back of her neck, lower abdomen, and hands (Figures 1 to 3). She presented to the emergency department and was sent home on oral corticosteroids and diphenhydramine but came back the next day with lip swelling and a more severe rash. The rash was pruritic, not painful, and described as diffuse, erythematous, maculopapular, and raised. Other than the lip swelling she denied any shortness of breath, wheeze, cough, phlegm, fever, or chills. She was admitted for further work up and a punch biopsy of one of her abdominal lesions was obtained. The skin biopsy (Figure 4) showed perivascular and interstitial inflammatory cell infiltrate of lymphocytes, histiocytes, and eosinophils in the dermis with PAS (Periodic acid-Schiff) stain negative for fungal elements consistent with an allergic reaction, such as to a drug. On treatment with intravenous corticosteroids and diphenhydramine her rash improved significantly. She was discharged the same day with oral corticosteroid taper. Despite her corticosteroid taper, her rash waxed and waned until day 18 at which time it resolved completely.
Rash on forehead. Rash on posterior aspect of the scalp and neck. Rash on outer aspect of thigh. Skin biopsy perivascular and interstitial inflammatory cell infiltrate in the dermis.

The patient made an informed decision to proceed with her fourth and final cycle of chemotherapy (TC (same doses day 1)) without pegfilgrastim. At the time of the last treatment (9 weeks from the start of chemotherapy), the total white blood cell count was 10,600 K/µl (neutrophils 76%) and declined to 3000 K/µl (neutrophils 38.8%) 2 weeks posttreatment; the rash did not reoccur.
Discussion
Adjuvant chemotherapy with TC for early breast cancer has improved survival.10–12 According to one trial with 506 patients receiving TC, rates for febrile neutropenia (FN) were 8% for older patients (age >65 years) and 4% for younger patients. 11 In a recent meta-analysis evaluating 902 patients treated with TC, the FN rate was 29% without primary prophylaxis, and therefore it is a standard part of treatment with TC. 13
Filgrastim and pegfilgrastim have been part of the supportive treatment of cancer patients for years. Their main use is to increase the absolute neutrophil count with the primary objective of preventing the appearance of FN in patients at risk. Risk is dictated by the chemotherapeutic regimen itself and due to patient factors, including comorbidities such as age of the patient and diabetes. 14 There have been case reports of immediate hypersensitivity reactions to both docetaxel as well as cyclophosphamide, with most cases occurring with docetaxel. Typically these occur with or soon after drug administration.15–18 The time course of the reaction in our patient and the fact that the rash did not return when it was withheld from the last cycle points to this rash being due to the pegfilgrastim.
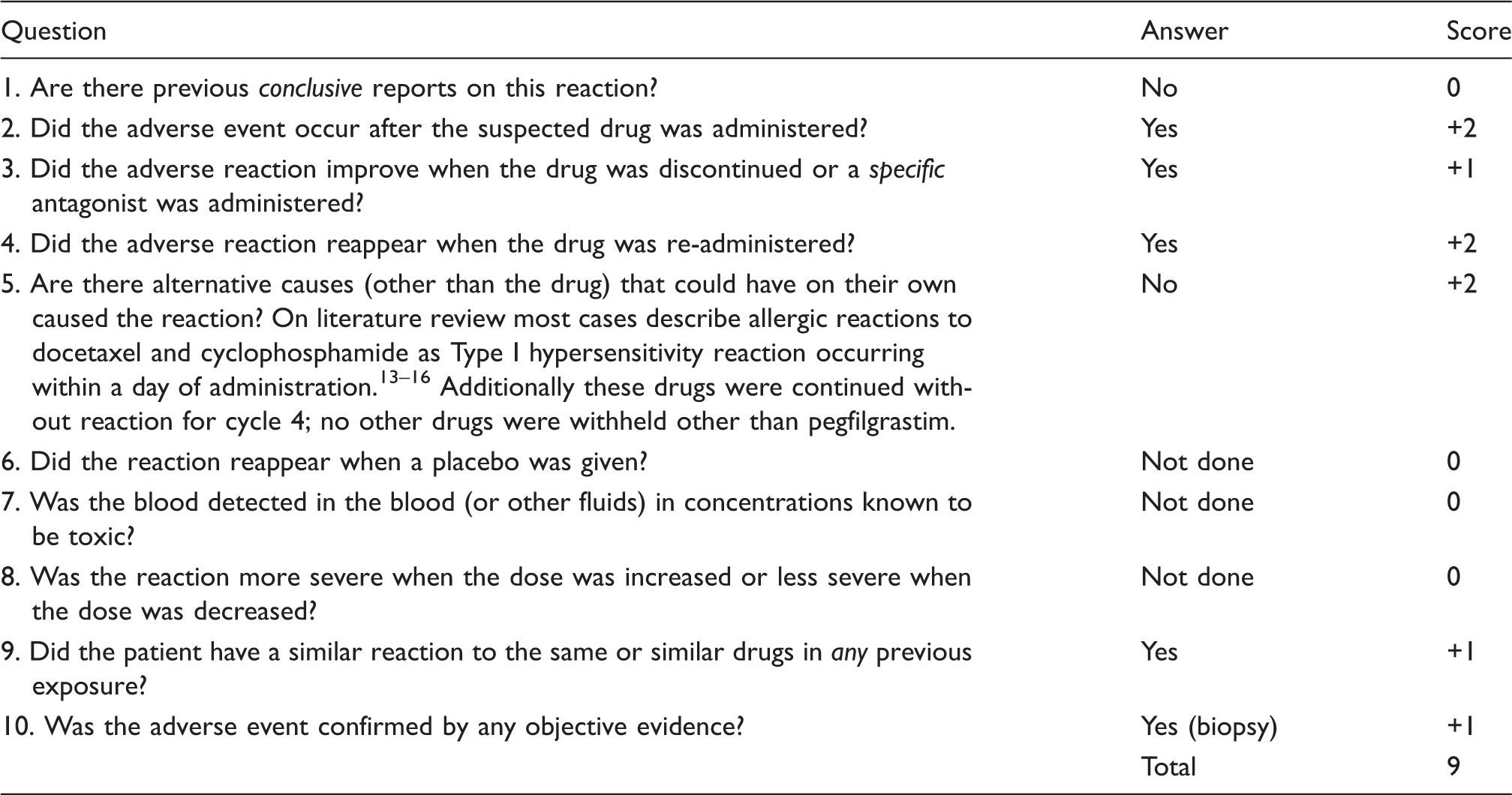
Naranjo adverse drug reaction scale for this reaction.
In the case of pegfilgrastim, a 20-kDa polyethylene glycol molecule is covalently conjugated to the N-terminal methionine residue of filgrastim. This results in a long-acting drug with a half-life of 15–80 h. 2 The polyethylene glycol moiety renders pegfilgrastim too large for renal clearance, thus leaving neutrophil receptor-mediated clearance as the primary mechanism of removal. 9 One paper postulates that since pegfilgrastim requires receptor-mediated clearance, it may trigger an abnormally high neutrophil proliferation beyond its intended action. Some of these neutrophils then deposit in the skin causing dermatological reactions. 9
Another paper with a case of advanced pancreatic cancer postulates that the tumor itself may produce its own G-CSF, which leads to production of antibodies that cross react with exogenous G-CSF, 6 though that patient only received pegfilgrastim and filgrastim was not administered. At this point we cannot be sure if our case involved the above mechanisms or rather was an idiosyncratic reaction as seen with other commonly used medications.
We alert clinicians to the possibility of delayed hypersensitivity reactions to pegfilgrastim due to its purposefully slow clearance as a result of its drug design. The use of this drug is critical to the timely and safe delivery of chemotherapy and awareness of this potential toxicity is important.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.