
Abstract
Administration of chemotherapy is moving into the community as more and more therapies to treat cancer are being developed as oral medications. Patients taking these oral medications still require support, as many of these agents can be toxic. This support could be simple side effect management, compliance issues or even reassurance with regards to their diagnosis as examples. Community pharmacies are ideally placed within the community to help these patients. The purpose of this review is to determine what support community pharmacies are currently providing for patients taking oral anticancer medication and if there is a model that can be adopted or adapted to be used elsewhere. Searches were undertaken using two databases, Medline and Embase. Other evidence-based articles were discovered from other sources. The different services currently available from community pharmacies were largely varied. There are some key aspects to each which could be used in the development of a new model. Further research is required to determine the views of the patients, carers and community pharmacy staff.
Keywords
Introduction
Cancer treatments are increasingly being administered orally rather than the historic route of intravenous administration; this is likely to continue. 1 There is a new scene of oral chemotherapy emerging. Oral chemotherapy agents are no longer limited to cytotoxic drugs but include tyrosine kinase inhibitors and hormonal treatments now becoming available and on the horizon too. The majority of literature currently states that 25% of all antineoplastic drugs in development are oral medications.2,3 This trend is linked to the fact that these treatments are being used for chronic or palliative therapy rather than adjuvant treatment. 4 Attitudes towards cancer are slowly changing as recognition is given to cancer as a chronic condition rather than a life-threatening disease. 5 Administration of anticancer medication orally creates a shift from hospital-based treatment to community-based treatment, as patients are able to administer the doses themselves at home. This shift has already occurred in other disease states such as asthma and diabetes. 6 This brings treatment closer to home for patients providing them with a better treatment experience and also releasing capacity pressures on the hospital. There are many safety benefits such as the fact that patients do not have to attend hospital as frequently, nor do they need intravenous access both of which reduce the risk of a potentially life-threatening infection in already immune-compromised patients. 1 This topic is very relevant currently as cross-sector working, community pharmacy involvement and providing specialist care closer to home have been documented in the following key policy documents: NHS Five Year Forward View (FYFV), 7 Achieving World-Class Cancer Outcomes: A Strategy for England 2015–2020 8 and the two follow-up reports for this: Achieving World-Class Cancer Outcomes: Taking the Strategy forward 9 and Achieving World-Class Cancer Outcomes: One year on 2015–2016. 10 The Sustainability and Transformation Plan for South East London detailing the local implementation plans for the FYFV states specifically that there is not enough investment in community, either preventing illness or encouraging our patients to manage their own health. 11 If better support could be provided in the community then this would reduce patients coming into hospital unnecessarily. 11 The significance of community pharmacy care is also mentioned in Lord Carter’s recent review looking at unwarranted variations in hospital care. 12 The review recognises the importance of community pharmacies, which if utilised properly can ultimately free up hospital clinical pharmacy time to focus on clinical services. At the recent Royal Pharmaceutical Society’s Innovators Forum, they discussed the integration of pharmacists into the new Vanguard models of care. 13 Within the Vanguard models there is a lot of attention around cross-sector working and how hospital pharmacists can work closely with their community counterparts to provide specialist care in the community. 13
Oral anticancer medication does require the patient to be able to self-manage. 14 Adherence becomes a significant issue here. The World Health Organisation estimates that 50% of medicines taken for chronic conditions are not taken as prescribed. 15 A large number of patients who receive oral anticancer medication are older and often have multiple co-morbidities and consequently need more support because of this. 16 Managing toxicities is also a significant challenge for these patients and the teams supporting them. 4 According to Deery 17 patients on oral anticancer therapy need as much support as those receiving chemotherapy via the intravenous route. Ideally this support would be best placed to come from the primary care setting to avoid the patient returning to hospital unnecessarily. Community pharmacies would be an excellent source of expertise to utilise. 18 The contact that community pharmacy staff have with cancer patients will increase as more and more patients are treated with oral therapy over intravenous therapy. 19 Although currently community pharmacy staff may not have direct involvement with cancer care, these patients may well be visiting community pharmacies for advice already. 20 One of the potential barriers to this is that community pharmacies may not want to take on more service-based work. A series of case studies performed to discover the benefits of enhanced skill mix described that the pharmacies they interviewed were patient focused rather than prescription focused and were happy to offer more than just the dispensing service. 21
This review was conducted in order to determine what support is currently provided by community pharmacies for patients receiving oral anticancer therapy. With this information support for these patients in the NHS can be improved and relationships between hospital and community pharmacists strengthened.
Methods
Search strategy used for Medline and Embase.
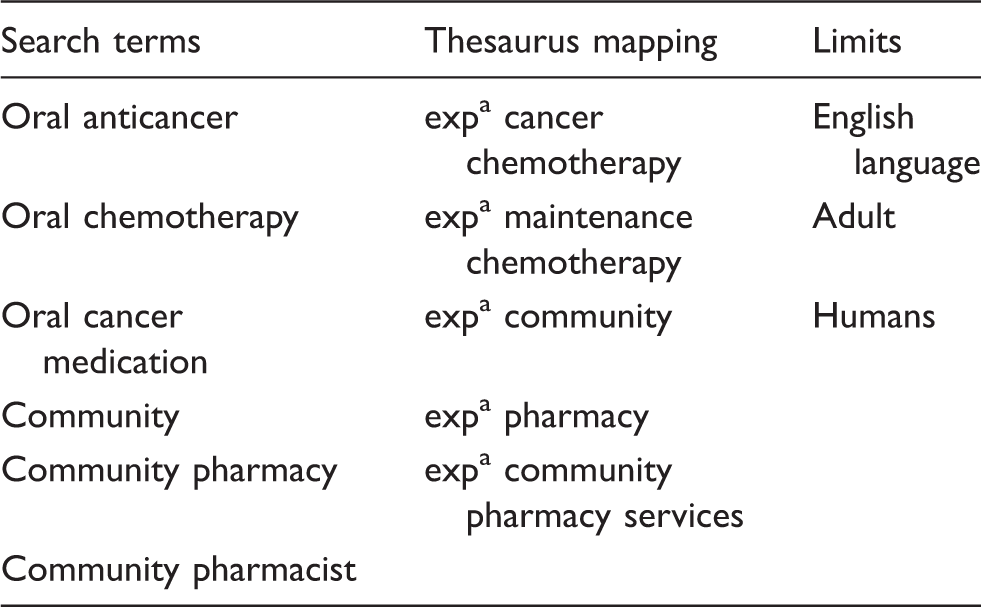
Exploded.
Results
Models of support from community pharmacies to patients on oral anticancer from the published literature.
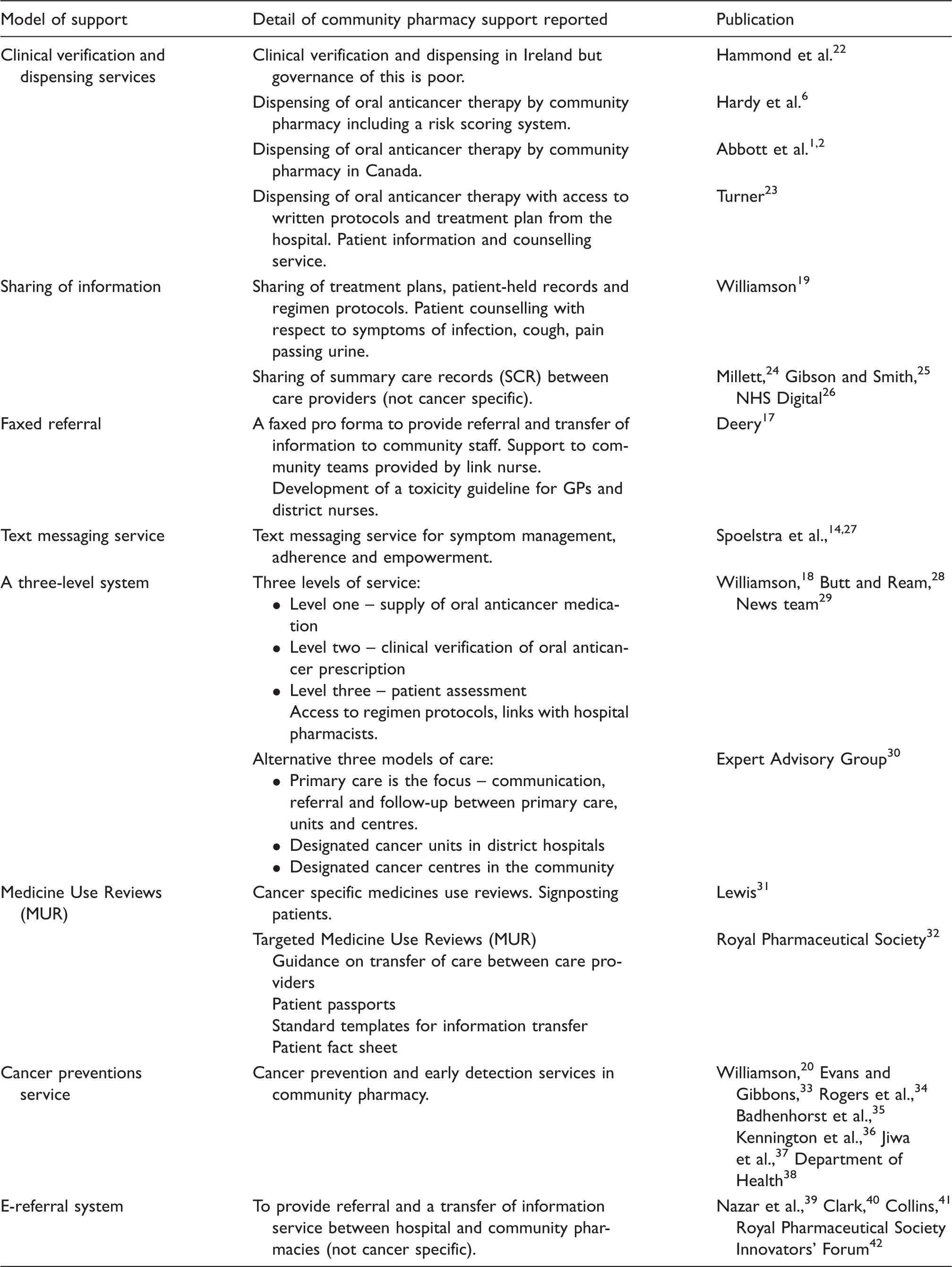
A common barrier to patient care across NHS providers described in multiple articles was the transfer of information from the hospital or General Practitioner (GP) to the community pharmacy. There were quite a few different methods used to solve this challenge. One hospital created a patient passport, which contained details of treatment and diagnosis. 32 Another created a specific pro forma containing patient information that was then faxed to the community pharmacy. Additionally a standard template was used for information transfer.17,32 These methods rely on the patient to transfer the information themselves or the use of fax machines which are fast becoming outdated within the NHS. Sharing of Summary Care Records (SCR) has been shown to reduce the number of calls that a community pharmacy makes to a GP surgery and improves the direct contribution to patient care. 24 In one GP practice, calls were estimated to be reduced by 80%. 24 A third benefit with this is that issues are solved in the pharmacy avoiding the need for patients to return to the GP surgery. In a pilot involving 140 pharmacies, 92% of problems where the SCR was accessed were solved in the pharmacy. 25
A study was conducted on the use of text messaging as a daily reminder to patients to take their medication and a weekly symptom management message to remind them to record their symptoms. 14 The results showed only preliminary efficacy in promoting self-management for patients taking oral anticancer medication. Adherence was improved in the intervention group for only four of the nine weeks that adherence was measured, with one week showing the same adherence levels and the remaining four weeks showing greater adherence in the control group. 14 The summed symptom severity did not significantly differ between study arms. 14 However, 34 patients (n=37) reported satisfaction with receiving text messages and found the texts helpful. 14
Four articles detailed a service or model of care using three levels. Three of the articles relate these levels to the supply of anticancer medication, clinical verification and then lastly patient assessment.18,28,29 The last article relates to where the services will occur such as primary care, cancer units within district hospitals or cancer units within the community. 30 Neither of the articles provide evidence of putting these levels into practice but provide suggestions on how to implement them.
Oral anticancer targeted medicines use reviews (MUR) were discussed in two articles.31,32 As most community pharmacies already provide MUR it was not deemed too much extra work to utilise this method of patient counselling and medicines optimisation to patients taking oral anticancer therapy. Pharmacies were also signposting patients to the relevant care provider in cases where the task was out of their scope of practice. 31 There has also been significant work done with community pharmacies into cancer prevention and early detection services.18,33–38 Recently the Be Clear on Cancer campaign run by the Department of Health is encouraging patients with signs or symptoms of cancer to visit their GP or community pharmacy. 38
More sophisticated systems using digital technology have been suggested for sharing patient information and referring patients. A number of hospitals are using different methods to refer patients to a community pharmacy post discharge. Derby Hospital NHS Foundation Trust, Southport and Ormskirk NHS Trust and Royal Cornwall Hospital fax referrals, Southend University Hospital NHS Foundation Trust email referrals, Newcastle-Upon-Tyne Hospitals have a dedicated e-referral tool through PharmOutcomes and East Lancashire Hospitals NHS Trust have a fully integrated solution through Refer-to-Pharmacy. 32 The e-referral system in Newcastle-Upon-Tyne uses PharmOutcomes which is a web-based platform. 39 A large number of community pharmacies across the UK have access to PharmOutcomes. Therefore, they started using the system in their Trusts and created a referral template in order to refer patients post discharge. This did require a lot if implementation and training with both the hospital staff and community staff involved. A study was done to record the effectiveness of the implementation. Hospital staff identified patients that would benefit from a consultation from a community pharmacist post discharge (not cancer specific). 39 The results showed that hospital staff were able to improve care of patients who were transferring back into the community and indicated that these consultations lowered readmission rates. 39 The number of readmissions post referral in those that received a community pharmacy consultation was 5.8% compared to 16% in those that did not receive a consultation and the number of bed days for readmitted patients receiving a community pharmacy consultation was 7.2 (SD ± 1.0) compared with 13.1 (SD ± 17.4) days for those that did not receive a consultation. 39 This system is now being used in eight other Trusts in the North East and North Cumbria.
The Refer-to-Pharmacy system uses a purpose-built software directly referring patients on discharge to community pharmacies. 40 The community pharmacy receive a discharge summary and a referral note detailing the next steps required by the community pharmacy. 40 A licence fee is needed, however, to be able to purchase the system which was funded by East Lancashire Trust and two Clinical Commissioning Groups (CCGs). 40 The system works by pulling information directly from the Trust’s patient administration system and it is automatically sent when the patient is discharged. This saves a lot of time for the community pharmacist as they don’t need to chase the hospital or GP to get discharge information. 40 The system has shown a reduction of hospital readmissions from 4.2 to 3.2% when compared with the same period the year before. 40 A similar scheme was set up in Wales initially as a paper-based system which was updated to an electronic version. 40 Although this scheme did cost over £1m, around £3m was liberated due to avoided admissions, drug wastage and avoided accident and emergency visits. 40
Discussion
There is very little literature detailing statistically significant data relating specifically to models in place or trialled whereby community pharmacists are supporting patients on oral anticancer therapy. There do seem to be quite a few models however that are being used for post discharge patients not specifically cancer patients that came up from the search databases. To be able to determine whether any of these ideas or models are suitable to be adapted or employed elsewhere the advantages and disadvantages need to be examined. Community pharmacists are already providing a successful service for cancer prevention and there have been a number of campaigns run by Department of Health to help promote this on a National level within the UK; however, this is not necessarily relevant to patients who already have cancer. 38 It does show that pharmacies in the community are already educated in the signs and symptoms to be aware of when their patients present with unusual symptoms or a mixture of specific symptoms. This education could therefore be expanded to include further support advice for patients on oral anticancer treatment provided they are supported by hospital specialist pharmacists. 44 Community pharmacies could then review patients through cancer specific MURs as specified by Lewis. 31 One study did show that community pharmacists are not confident in their knowledge when discussing oral chemotherapy with patients and an educational designed programme was effective at improving their competence and confidence in counselling patients taking these drugs. 45
For those pharmacies that are providing a dispensing service there needs to be a governance structure in place to ensure a safe and efficient service to the patients. Some of the suggested options to ensure a safe, well-governed service include community pharmacist access to chemotherapy hospital protocols, patient treatment plans, clear communication pathways with the hospital and possibly a link pharmacist at the hospital to provide support to the community pharmacy team.19,42 These suggestions should be recommended for any level of service whereby community pharmacists are supporting patients on oral anticancer therapy. The National Patient Safety Agency’s Rapid Report into the risks of incorrect dosing of oral anticancer medicines highlights the potential fatal outcomes if safeguards are not used when non-specialist practitioners prescribe, dispense or administer oral anticancer medicines. 46 Although the four articles detailing the three levelled systems, which included dispensing, were coherently explained, evidence through piloting of these systems is recommended to provide a proof of concept for others to adopt.
The last common theme that appears in this literature search is the importance of sharing the right information. There are some potentially outdated models suggested. The use of faxing information across to community pharmacies is potentially an information governance risk as well as not supporting a paperless NHS. There are risks associated with emails and text messaging. There is a potential that patient information is sent to the wrong person. This of course applies to faxes also. If an email is sent to a particular community pharmacist who perhaps doesn’t check that email account for a number of days then a patient who has been identified for follow-up could be missed. There is also an information governance risk again if information is not shared through an nhs.net email account. The use of a patient passport or booklet requires the patient to bring it to each hospital appointment and for a health care professional at that appointment to complete it each time. The patient would then have to remember to take it to the community pharmacy to provide them with the required information. In a digital world, is this sustainable?
Further research into the use of text messaging patients for adherence and symptom management needs to be conducted to show statistical significance of this method before it is implemented. The sharing of the SCR has clearly shown benefits between GP surgeries and community pharmacies but this does only include the medication that the GP surgery prescribes. Unless the hospital can access it with write access to include the anticancer medication, this system will not provide a comprehensive drug history for these patients.
Two systems that have shown reduced hospital readmissions are PharmOutcomes and the Refer-to-Pharmacy systems as described by Nazar et al., 39 Clark, 40 Collins 41 and the Royal Pharmaceutical Society Innovators’ Forum. 42 Both provide a direct referral to the community pharmacist. The referral system using PharmOutcomes first requires access to the system for the hospital staff. The literature is unclear what cost was involved with this and also if there was a cost where the funding came from. Hospital staff needed training in order to be able to use the system and community pharmacies needed to be encouraged to check the system on a regular basis in order to receive the referrals. Hospital staff had to complete a template referral form with the patient details once they had received consent from the patient. The Trust did work to quality improve the system to allow for easier use and to include data collection. 39 The use of PharmOutcomes for referring patients post discharge to the community pharmacies lowered the rate of readmission and resulted in shorter hospital stays. 39
The Refer-to-Pharmacy system is a system that appears to have been well thought out. Patients are shown a short film about it before consenting and then the patient’s hospital number, reason for referral and community pharmacy is entered. Once the patient has been discharged the system automatically sends the referral. If the community pharmacist do not pick up the referral a notification is sent back to the hospital recommending them to contact the community pharmacist directly. The system also allows information to be sent back to the hospital if required.
Based on the literature described above the following key points have been utilised in order for community pharmacies to safely provide a support service to patients receiving oral anticancer therapy:
Training on cancer and oral anticancer medications for community pharmacy staff Community pharmacy access to chemotherapy protocols and patient treatment plans Good communication between the hospital and the community pharmacy Integrated working between the hospital and community pharmacies A key link person at the hospital that the community pharmacy staff can contact A referral system that safely delivers key patient information in a confidential way that involves a closed loop, i.e. information back to the hospital Patient consent Cancer targeted MUR Information for community pharmacy staff for signposting
Organisations wishing to develop a system to integrate secondary care with community pharmacies to support this patient group may benefit from using a combination of these points. An addition to this that none of these models currently show would be if all the NHS care providers were able to connect to a system that stored all the information for a given patient and each provider could update that system. This is a big vision that is a long way off but is not impossible with the digital technology available and with appropriate investment.
Conclusion
Even though some of these models do not relate specifically to patients on oral anticancer therapy, there is a potential that these could be adapted to create a system that would work for patients taking oral anticancer medication. The next steps are to find out more information from patients on oral anticancer therapy, specifically what support they require in between their hospital visits and explore their perceptions of community pharmacies and then determine what education is required to ensure community pharmacy staff feel competent and confident to provide this service.
Footnotes
Acknowledgements
Dr Vivian Auyeung, Institute of Pharmaceutical Science, King’s College London.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received funding from the King’s Health Partners Pharmaceutical Science Clinical Academic Group.