
Abstract
The incorporation of L-asparaginase and pegylated asparaginase into pediatric-inspired regimens has conferred a survival advantage in treatment of adults with acute lymphoblastic leukemia. Use of asparaginase products requires careful prevention, monitoring, and management of adverse effects including hypersensitivity, hepatotoxicity, pancreatitis, coagulopathy, and thrombosis. Currently, there is limited published literature to offer guidance on management of these toxicities. At the University of Maryland Marlene and Stewart Greenebaum Comprehensive Cancer Center, a standard of practice guideline was created to prevent and manage asparaginase-related adverse events. By sharing our long-term experience with asparaginase products and clinical management of asparaginase-induced toxicities, this article aims to improve patient safety and optimize treatment outcomes.
Keywords
Introduction
In 1953, Kidd administered guinea pig serum to rats and mice with lymphoma and observed subsequent tumor regression. The effect was hypothesized to be from a complement immune-mediated effect. 1 Broome and colleagues later negated this theory and found that tumor regression was not caused by complement in the serum, but rather by the enzyme L-asparaginase. 2 The earliest reported use of L-asparaginase for hematologic malignancies in humans was published in the mid-1960s by Dolowy et al. and Hill et al.3,4
L-asparaginase is an enzyme that can be isolated from several bacteria including Escherichia (E.) coli and Erwinia (E.) chrysanthemi. Two Food and Drug Administration (FDA)-approved formulations of asparaginase are commercially available: E. chrysanthemi-derived asparaginase (Erwinaze®), and E. coli polyethylene glycol asparaginase (pegaspargase, Oncaspar®). E. coli L-asparaginase (Elspar®, Kidrolase®), although FDA-approved, is no longer commercially available in the United States. A fourth formulation, L-asparaginase-loaded red blood cells, is currently under investigation. 5 E. coli asparaginase is FDA-approved as a component of multi-agent chemotherapy regimens for treatment of patients with acute lymphoblastic leukemia (ALL).6,7 The FDA-labeled indication for E. chrysanthemi asparaginase is for ALL patients who have developed hypersensitivity to E. coli-derived asparaginase. 8 The pegylated formulation, pegaspargase, was first FDA-approved for use in 1994 for the treatment of ALL patients who were hypersensitive to native forms of L-asparaginase. In 2006, it was granted approval for first-line treatment of patients with ALL as a component of multi-agent chemotherapy.9,10 Even though asparaginase products are currently only FDA-approved for patients with ALL, there are ongoing studies of their use for non-ALL indications such as acute myeloid leukemia including myelosarcoma, non-Hodgkin lymphoma, multiple myeloma, and extranodal natural killer/T-cell lymphoma. 11
An understanding of the pharmacology of L-asparaginase is inherent to gaining perspective on its efficacy and toxicity profile. Asparagine is a non-essential amino acid, critical to protein synthesis and cell survival. In 1961, Haley et al. found that murine L5178Y leukemic lymphoblasts require asparagine for in vitro growth.
12
Asparaginases, as amidohydrolases, also possess glutaminase activity and deplete glutamine. Several studies have highlighted the necessity of glutamine depletion for optimal antileukemic effect of asparaginase.13–15 When asparagine levels are low, the enzyme asparagine synthetase (ASNS) catalyzes transamination of glutamine to aspartate, resulting in production of glutamate and asparagine in an ATP-dependent reaction. ASNS is present in all organs, but basal expression level varies. Primary ALL cells and many ALL cell lines generally exhibit little to no detectable ASNS expression. This makes ALL cells auxotrophs for asparagine and therefore particularly sensitive to asparagine depletion, since they are less likely to regenerate asparagine after use of asparaginase products. As such, administration of an asparaginase product to a patient with ALL rapidly reduces the plasma concentration of asparagine by catalyzing the deamidation of asparagine to aspartate and extracellular efflux of intracellular asparagine, as shown in Figure 1.16,17 This starves the leukemia cells, preventing further cell growth and inducing malignant cell apoptosis.18,19
Administration of asparaginase depletes glutamine and asparagine. When asparagine levels are low, ASNS catalyzes transamination of glutamine to aspartate, resulting in production of glutamate and asparagine. Primary ALL cells and many ALL cell lines generally exhibit little to no detectable ASNS expression, which makes ALL cells auxotrophs for asparagine and renders them particularly sensitive to asparagine depletion.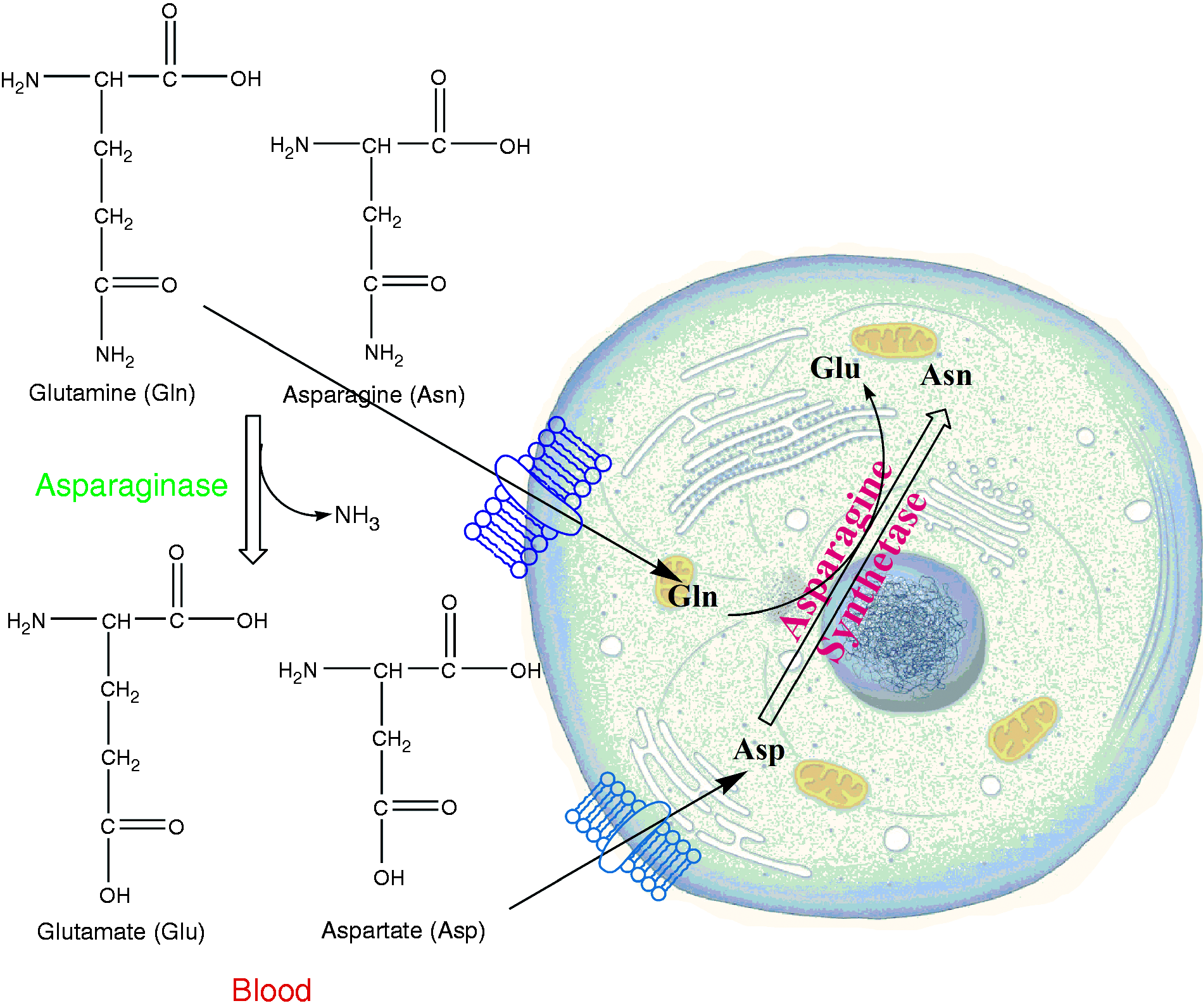
Of note, several mechanisms of resistance may affect the efficacy of asparaginase formulations. Aslanian et al. described elevated ASNS expression as a mechanism of L-asparaginase resistance in ALL cells, 20 but published data directly correlating ASNS activity or upregulation of ASNS mRNA with asparaginase product resistance are limited and conflicting. Another mechanism of resistance is development of neutralizing anti-asparaginase antibodies with repeated exposure to asparaginase, leading to inactivation of the enzyme.21,22
L-asparaginase-based regimens have been a cornerstone of treatment of ALL in the pediatric population since the 1970s. Inclusion of L-asparaginase is a key component of successful pediatric therapy that has produced a marked improvement in survival. The Dana Farber Cancer Institute (DFCI) clinical trial 77-01 randomized pediatric patients with non-T-cell ALL to treatment intensification protocols with or without L-asparaginase. Patients randomized to receive an asparaginase-containing regimen had a significantly higher event-free survival (EFS) of 71% vs. 31% (P = 0.03) and a significantly greater probability of disease-free survival (DFS) (P = 0.04). 23
Growing evidence suggests that adolescent and young adult (AYA) patients aged 15 to 39 years have improved outcomes, with DFS rates of 60% to 70%, when treated with asparaginase-containing pediatric-based regimens, as compared to adult regimens such as hyper-CVAD. 24 A review published in 2018 by Siegel et al. 25 summarized several studies comparing pediatric-like regimens to hyper-CVAD and showed statistically worse outcomes with hyper-CVAD. In a meta-analysis, Siegel et al. 26 describe 25 studies comparing pediatric vs. adult regimens for treating ALL. All but two of the studies strongly favored the use of pediatric-inspired protocols in the AYA population. 26 It is important to note that there are also studies that suggest that hyper-CVAD is as efficacious as pediatric-inspired regimens and avoids asparaginase toxicities. In a single-center study, Rytting et al. compared 106 patients who received an asparaginase-containing augmented Berlin–Frankfurt–Münster (BFM) regimen to 102 patients who received hyper-CVAD and found no statistical differences in complete remission rates, five-year complete remission duration, and five-year overall survival (OS). The adverse event profile was significantly different between the groups. The augmented BFM group experienced more asparaginase-related severe toxicities, including hepatotoxicity (41%), pancreatitis (11%), and thrombosis (19%). The hyper-CVAD regimen patients experienced significantly more myelosuppression-associated complications, including ≥Grade 3 infections during induction, compared to the augmented BFM group (45% vs. 22%; P < 0.001). 27 The evidence supports the use of pediatric-inspired regimens in the AYA population. However, institutional practices vary and some may still prefer to treat with hyper-CVAD to avoid asparaginase-related toxicities and the complicated administration schedules of pediatric-inspired regimens.
The five-year survival rate of patients with ALL is dramatically lower in older patients.28,29 The OS for adult patients with ALL in the US from 2000–2007 was reported at only 40%. 28 Several factors are thought to contribute to poorer outcomes in the adult population, including increases in the prevalence of genetic abnormalities, socioeconomic factors, and differences in chemotherapy protocols. 30 Despite the OS advantages observed with asparaginase use in pediatric populations, asparaginase was not used consistently for many decades in the AYA and relatively fit adult populations (<65 years old without significant comorbidities). Early adverse experience with asparaginase in the adult population in the late 1960s and early 1970s resulted in subsequent development of ALL protocols containing minimal or no asparaginase. 31 Adult protocols are characterized by greater use of myelosuppressive agents, such as cyclophosphamide and anthracyclines.
With improvement in drug purification, introduction of new long-acting formulations and routes, and familiarity with toxicities, asparaginase use in the adult population has been revisited.29,30 In the Group for Research on Adult Acute Lymphoblastic Leukemia (GRAALL) – 2003 study, investigators studied efficacy and tolerability of pediatric-inspired regimens in adults. In this trial, 225 adults (15 to 60 years old) with newly diagnosed Philadelphia chromosome (Ph)-negative ALL were treated with a pediatric-inspired regimen containing E. coli asparaginase. The results were retrospectively compared with those of the France-Belgium Group for Lymphoblastic Acute Leukemia in Adults (LALA-94). In LALA-94, 922 patients (15 to 55 years old) were treated with cytotoxic chemotherapy and only one dose of L-asparaginase during maintenance therapy. Complete response (CR) rate and OS were higher with the GRAALL-2003 regimen (CR 93% vs. 88%, P = 0.02) and OS at 42 months was 61% (95% confidence interval (CI) 54–68%) vs. 41% (95% CI 37–45%, P < 0.001). 32 The authors concluded that regimens containing multiple doses of L-asparaginase, as compared to single doses, were associated with significant improvement in patient outcomes. DeAngelo et al. treated 92 adults (18 to 50 years old) with newly diagnosed ALL (excluding mature B-cell ALL) with a pediatric-inspired regimen (Dana Farber Cancer Institute Adult ALL Consortium Protocol 01-175) utilizing a 30-week course of pharmacokinetically dose-adjusted E. coli L-asparaginase during consolidation. Disease-free survival at 48 months was 69% (95% CI 56–78%) and four-year OS was 67% (95% CI 56–76%). 33 With improvement in survival with use of pediatric-inspired regimens, asparaginase use has markedly increased.
It is imperative to note that most of the data in ALL are with use of native E. coli or E. chrysanthemi asparaginase short-acting formulations. Pegaspargase was not FDA-approved until at least 20 years after initial incorporation of L-asparaginase into ALL regimens. As such, outcomes for efficacy and adverse events are largely extrapolated from studies using short-acting L-asparaginase products. Pegaspargase has many advantages including longer half-life, decreased immunogenicity, and possibly less pancreatic side effects.9,34 It is produced by joining monomethoxypolyethylene glycol (PEG) to L-asparaginase. Pegylation prolongs plasma retention time and decreases proteolysis and renal excretion. 10 The half-life of pegaspargase is approximately six days, compared to approximately one day with native E. coli and E. chrysanthemi asparaginase preparations.6–9 The duration of effect for each product formulation type determines its dosing frequency. Douer et al. reported pharmacokinetic, pharmacodynamic, and toxicity data after administration of pegaspargase 2000 IU/m2 IV in asparaginase-naive patients with ALL. The kinetic posthoc analyses showed enzymatic activity for three weeks or more. 35 In a group of children with newly diagnosed ALL, the days of asparagine depletion were compared between the three preparations of asparaginase. Asparagine depletion lasted 14–23 days for E. coli asparaginase vs. 7–15 days for E. chrysanthemi asparaginase vs. 26–34 days for pegaspargase (P < 0.01). 36 Due to the longer half-life of pegaspargase, fewer injections are required while still allowing the patient to achieve adequate asparagine depletion.
Avramis et al. published an open-label, randomized, multicenter trial supporting pegaspargase efficacy. It included 118 children (one to nine years old) with previously untreated standard-risk ALL. Patients received either E. coli asparaginase or pegaspargase with multiagent chemotherapy during the remission induction and delayed intensification phases of treatment. E. coli asparaginase was administered three times weekly for nine doses during intensification and six doses during each delayed intensification phase. In contrast, pegaspargase was only administered once during induction and again during each delayed intensification phase. The three-year EFS rates were approximately 80% in both arms, which suggests that efficacy was not compromised by using pegaspargase. Of note, the study was underpowered to assess for efficacy; this was not the study's primary endpoint. 21
An important challenge that complicates drug effectiveness is the development of antibodies to the asparaginase product. Studies have previously shown that asparaginase activity is low when the antibody titer is high. 37 The previously mentioned Avramis et al. study evaluated asparaginase antibody ratios for both native and pegaspargase during induction, delayed intensification #1, and delayed intensification #2. They also evaluated the fraction of samples collected 3 to 14 days after administration with asparaginase activity above 0.1 IU/mL, which is the level above which asparagine depletion is considered to occur. The antibody ratio mean±standard error of the mean (SEM) was 3 ± 0.7 for E. coli asparaginase arm vs. 1.9 ± 0.8 for those treated with pegaspargase. Additionally, patients treated with pegaspargase had fewer samples with elevated antibody ratios and all pegaspargase samples with antibody ratios ≥1.5 showed adequate asparaginase activity. As such, the use of pegaspargase resulted in less antibody formation and even patients who had high antibody ratios showed adequate asparaginase activity. 21 Antibody inactivation of E. coli asparaginase has shown worse outcomes. Vrooman et al. evaluated patients 1 to 18 years old with ALL randomized to fixed dose (FD) weekly E. coli asparaginase or individualized dose (ID) E. coli asparaginase adjusted every three weeks based on nadir serum asparaginase activity (NSAA) to maintain a nadir between 0.10 and 0.14 IU/mL. FD patients switched asparaginase preparation for clinical allergic reaction; ID patients with NSAA <0.1 IU/mL despite dose adjustment or when coupled with antibody positivity were considered to have “silent inactivation” and switched to E. chrysanthemi or pegylated-asparaginase. They found that ID patients who switched preparations for silent inactivation had five-year EFS of 95% compared to 76% for FD patients with NSAA level <0.1 IU/mL who never switched preparations. The difference in five-year EFS result was attributed to silent inactivation that was identified in the ID arm, but not in the FD arm.38
At our institution, pegaspargase is incorporated as part of ALL treatment in the Cancer and Leukemia Group B (CALGB) 10403 regimen and in AML treatment using the HAM-pegA regimen (high-dose cytarabine, mitoxantrone, pegaspargase). In the AYA population, the choice of regimen for ALL varies considerably in the United States depending on physician's preference and availability of clinical trials. Typical treatment of ALL includes a backbone of multi-agent chemotherapy consisting of vincristine, anthracyclines, and steroids. Regimens may also include cyclophosphamide and asparaginase products. There are many variations in ALL treatment regimens, but in general all use the same multi-agent backbone. Some common regimens include ALL-96, BFM, DFCI ALL 01-175, and CALGB 10403. To date, CALGB 10403, which enrolled 295 patients aged 16 to 39 years, is the largest prospective study evaluating the use of a pediatric-inspired regimen in adults. Compared to historical controls, patients treated on the CALGB 10403 protocol experienced higher EFS with median EFS of 78.1 months (95% CI, 41.8–not reached) vs. 30 months (95% CI, 22–38). The three-year EFS was 59% (95% CI, 54–65%). Although accrual to the trial is closed, we treat our patients according to regimen in CALGB 10403. 39
For relapsed or refractory AML patients, salvage therapy includes regimens containing cytarabine and anthracyclines. A single-center study retrospectively evaluated HAMA in 94 relapsed or refractory AML patients aged 20 to 84 years. The CR or complete response with incomplete count recovery (CRi) rate was 41% (61% < 60 years old; 33% ≥60 years old). In patients < 60 years old, 50% proceeded to allogeneic hematologic stem cell transplant (HSCT), whereas for patients ≥60 years old, 14% proceeded to HSCT. We use HAM-pegA as an asparaginase-containing AML salvage regimen at our institution. HAM-pegA regimen is given over four days and consists of high-dose cytarabine 3 g/m2 IV over 3 h every 12 hs for five doses on days 1, 2, 3, mitoxantrone 6 mg/m2 IV over 1 h once daily for three doses on days 1, 2, 3 immediately following doses 1, 3, 5 of cytarabine, and pegaspargase 2500 mg/m2 IV over 2 h (with dose cap of 3750 IU) for one dose on day 4. The dose of cytarabine is reduced to 1 g/m2 for renal dysfunction or age ≥60 years old. Of note, the original study uses 6000 units/m2 L-asparaginase IM, whereas our institution substitutes pegaspargase 2500 mg/m2 IV with a dose cap of 3750 IU. 40
While asparaginase use confers a survival advantage in both pediatric and adult populations, its use requires careful prevention and management of a range of possible toxicities. Asparaginase appears to cause more toxicities in adults than in children, with an increased trend with age. 29 While toxicities are generally manageable and do not warrant omitting this key chemotherapy agent from standard ALL regimens, it is critically important to be able to prevent, recognize, and manage asparaginase-related toxicities.
The use of pegaspargase is challenging and the risks must always be weighed against the benefit of its use. We created a standard of practice guideline focusing on prevention, monitoring, and management of pegaspargase-related adverse events. Reasons prompting us to create this guideline included increased institutional and national use of pegaspargase, known frequency and severity of pegaspargase-related adverse events (especially in older adults), and absence of detailed best practice consensus or evidence-based guidelines for pegaspargase use and monitoring since Stock et al. published their recommendations in 2011. 29 Here we share our single center's guide to adverse event management in order to optimize treatment outcomes without compromising patient safety.
Materials and methods
A working group of physicians and oncology clinical pharmacy specialists at the University of Maryland Greenebaum Comprehensive Cancer Center (UMGCCC) performed a PubMed literature search to identify current and best practices surrounding pegaspargase-related toxicity prevention and management. An informal survey was also conducted to understand other institutions' practices surrounding antithrombin repletion and dosing of anticoagulants for venous thromboembolism (VTE) prophylaxis in patients receiving pegaspargase, given clinical controversy and financial implications of implementing these practices. Survey questions included whether antithrombin repletion is used for prevention of pegaspargase-related thrombosis, whether antithrombin repletion is used during treatment of active thrombosis during pegaspargase treatment, and what dosing strategy is used for LMWH in the prophylactic setting. Information from the literature search and the survey was compiled to modify our single institution's pegaspargase guidelines, which were initially adopted in April 2017 and formally implemented in an updated version in February 2018. These guidelines are intended for any non-study use of pegaspargase in the AYA and adult populations.
Management of pegaspargase toxicities
As previously stated, the frequency of pegaspargase toxicities increases with patient age. A study compared the incidence of ≥Grade 3 pegaspargase toxicities in AYA and adults (14 to 68 years old) versus pediatric patients (0 to 18 years old). Seventy-six patients with newly diagnosed ALL were treated with IV pegaspargase. The adult population experienced higher incidences of elevated liver enzymes (36%), hyperbilirubinemia (14%), hypofibrinogenemia (16%), pancreatitis (5%), and thrombosis (8%) compared to children, but a lower incidence of hypersensitivity (1%) and bleeding (0%). 41
Dosing strategies
We recommend pegaspargase 2500 IU/m2 IV capped at 1 vial (3750 IU) for all non-study adult patients.
Because pegaspargase-induced toxicities may be life-threatening, approaches to toxicities include interruption of therapy or discontinuation of future pegaspargase doses. Douer et al. found that 20% of previously untreated ALL patients aged 18 to 57 years did not complete all planned doses of pegaspargase because of pancreatitis, severe allergy or deep vein thrombosis. 35 Thus providers must weigh the risk of dangerous adverse effects with each dose versus the benefit of improved OS seen with completing all doses of therapy.
The challenge is to identify the dosing strategy that optimizes disease control while minimizing the risk of toxicities that would preclude patients from receiving the full number of pegaspargase doses or delay administration of subsequent cytotoxic agents. The pharmacokinetics of pegaspargase have been extensively studied in pediatric patients, but studies in AYA and adults are limited.42–44 Pegaspargase doses of 2500 IU/m2 are used in the Children's Oncology Group (COG) ALL 0232 and CALGB 10403 protocols and appear to have greater hepatotoxicity in the AYA population during induction therapy. 45 This may be due to the higher body surface area-based doses in AYA patients.
There is limited literature on different dosing strategies in adults. The dose of 2500 IU/m2 is used in pediatric-inspired adult ALL protocols such as CALGB 10403 and is the dose approved by the US Food and Drug Administration. 9 Some published studies have evaluated lower doses of 2000 IU/m2 uncapped or at 3750 IU (one vial) arbitrarily capped because of higher bioavailability after IV compared to IM dosing and possibly greater toxicity in adults. Douer et al. conducted two separate studies in newly diagnosed adult ALL patients treated per the BFM protocol with substitution of a single dose of pegaspargase 2000 IU/m2 IV without a dose cap on day 16 for 14 injections of E. Coli asparaginase. The first study enrolled 25 newly diagnosed ALL patients aged 17 to 55 years, while the second evaluated 55 adults aged 18 to 57 years. The CR rate was 96% in both studies. Grade 3 and greater toxicities included transaminitis (12% vs. 63%), hyperbilirubinemia (8% vs. 31%), deep vein thrombosis (4% vs. 14%), and pancreatitis (0% vs. 14%).35,43 In contrast, the original BFM protocol included 162 patients with ALL or acute undifferentiated leukemia (AUL) aged 15 to 65 years old, with 77.8% achieving complete response. 46 A study by Wetzler et al. evaluated doses of 2000 IU/m2 but capped at 3750 IU. This was a multicenter trial evaluating 85 patients with untreated ALL (excluding Burkitt-type) or AUL treated per CALGB 8811. Patients were initially given pegaspargase 2000 IU/m2 subcutaneously (capped at 3750 IU) on day 5 of induction and day 15 of early intensification. The protocol was later modified to give patients pegaspargase 2000 IU/m2 on days 5 and 22 of induction and days 15 and 43 of first intensification. The overall CR rate was 77%, which was lower than the CR rates reported in the Douer studies without dose capping. 43
Recently, the United Kingdom Acute Lymphoblastic Leukaemia (UKALL) trials have focused on administering smaller doses of pegaspargase at 1000 IU/m2, with dosing frequency depending on patient age, treatment phase, and length of treatment phase. The UKALL study enrolled patients 25 to 65 years old with newly diagnosed ALL regardless of Philadelphia chromosome status. Patients received a dexamethasone prephase, then two sequential courses of induction therapy. Pegaspargase was administered at 1000 IU/m2 on Days 4 and 18. The UKALL14 trial had a higher mortality rate than the previous UKALL12. Asparaginase activity was monitored via a trough level assessed 14 days after the first dose in 49 patients. Enzyme activity was therapeutic (enzyme level >0.1 IU/mL) in 42 of 49 (86%), thus suggesting that a dose of 1000 IU/m2 is effective. However, induction deaths occurred in 16 of 90 patients (18%). Of those deaths, 15 of the first 59 (25%) were in patients >40 years old. The causes of death were often multifactorial; however, the most common was concurrent sepsis and hepatotoxicity in 8 of 16 (50%). The authors noted that induction deaths occurred after the day 4 pegapargase dose, also in the setting of myelosuppressive toxicities of anthracycline given on days 1, 8, 15, and 22. As a result, the protocol was amended to omit the day 4 pegaspargase dose for patients >40 years old, decrease daunorubicin doses by half to 30 mg/m2 on days 1, 8, 15, 22, and omit pegaspargase from induction treatment for patients with Philadelphia chromosome-positive ALL. Following the amendment, 302 patients were recruited with 244 assessable for induction death and induction deaths occurred in only 6 (2.5%). 47 In summary, optimal pegaspargase dose and frequency are still debated. Timing in relation to myelosuppressive agents also affects toxicities and treatment-related death.
At our institution, we dose pegaspargase at 2500 IU/m2 with a dose cap of 3750 IU for all patients not enrolled on a clinical trial. As previously mentioned, our institution's pediatric-inspired ALL regimen of choice is CALGB 10403, and we have used the treatment scheme in that trial since the trial stopped enrollment. It includes pegaspargase 2500 IU/m2 once or twice within each phase, with a minimum of 14 days between doses. Our rationale for using 2500 IU/m2 with a dose cap of 3750 IU was to follow the dosing scheme of CALGB 10403 per protocol, but capped the dose at 3750IU, which follows the practices of many clinical trials and institutions, in order to minimize drug-induced toxicities. Although the choice to select one vial (3750IU) is arbitrary and based on vial size, our group thought it best to cap doses so that patients would be more likely to be able to receive all planned doses. Current literature describing lower doses consists of single-arm studies with unclear comparisons in describing asparagine depletion and asparaginase activity. CALGB 10403 is used for patients 16 to 39 years old at our institution, using the inclusion criteria outlined in the trial. For patients who are not candidates for pegaspargase due to comorbidities or older age, a non-asparaginase regimen such as hyper-CVAD is considered. As previously mentioned, relapsed or refractory AML patients may receive HAM-pegA, which contains one pegaspargase dose of 2500 IU/m2 with a dose cap of 3750 IU on day 4. The choice of whether to use this reinduction regimen or another regimen such as CLAG-M is dependent on patient-specific factors and preference of the treating oncologist. If patients are not candidates for pegaspargase due to comorbidities, a regimen not containing pegaspargase is used. There is not a strict age cut-off for patients to receive pegaspargase, as the literature does not strongly support specific ages at which patients are at increased risk for toxicity or lack of efficacy.
Hypersensitivity reactions
We recommend intravenous pegaspargase administration and premedication with acetaminophen, hydrocortisone, and diphenhydramine for prevention of hypersensitivity reactions.
We recommend permanent discontinuation of pegaspargase and switching to Erwinase (Erwinia chrysanthemi) for patients who experience a ≥Grade 3 severe hypersensitivity reaction.
Asparaginase is a foreign protein and therefore there is a risk of hypersensitivity reactions, ranging from mild infusion-related reactions to fatal anaphylaxis. The incidence of hypersensitivity to asparaginase reported in the literature is 10% to 15% in adults.29,47 The risk of hypersensitivity is dependent on the number of previous exposures to asparaginase, the type of asparaginase, the patient's immunocompetence, and the use of corticosteroids during treatment. 48
The effect of IV versus IM delivery of pegaspargase on hypersensitivity reactions has been a topic of clinical controversy. In a study of 318 children receiving pegaspargase, there was a 9% greater incidence of hypersensitivity with IV compared to IM drug delivery. 49 The Dana Farber Cancer Institute identified an 11% incidence of hypersensitivity with pegaspargase IV compared to 9% with IM. 50 Recently, Burke et al. 51 found that the rate of ≥Grade 3 hypersensitivity reactions was 5.4% with IM injections compared to 3.2% for IV administration (P < 0.001) in six COG leukemia trials (2003-2015). 51 No deaths were reported from hypersensitivity reactions with either formulation. Higher-grade reactions appear to be less frequent with IV administration, while lower grade reactions are more commonly seen. It is unclear to what degree infusion-related reactions are being interpreted as hypersensitivity reactions.
Repeated exposure to asparaginase products increases the risk of developing neutralizing anti-asparaginase antibodies that may not produce clinical symptoms of allergic reaction, but may reduce the overall efficacy of the medication by inhibiting the enzymatic activity (“silent hypersensitivity” or “deactivation”).
Compared to L-asparaginase, pegaspargase is associated with a lower incidence of developing anti-asparaginase antibodies. In 2002, Avramis et al. 21 published a randomized study of L-asparaginase vs. pegaspargase in children. High-titer anti-asparaginase antibodies were present in 26% of patients treated with L-asparaginase, compared to only 2% in those treated with pegaspargase. Of note, the immune system can also produce antibodies that specifically recognize and bind to PEG. These anti-PEG antibodies have been correlated with loss of therapeutic efficacy and increase in adverse effects such as injection site reactions and dizziness.52,53 Armstrong et al. 54 analyzed blood samples from 28 patients receiving pegaspargase. Among 15 patients with undetectable asparaginase activity after receiving pegaspargase, 9 had anti-PEG antibodies detected by serology and 12 by flow cytometry. They concluded that anti-PEG antibodies were closely associated with the drug's rapid clearance. 54
Premedication strategies have proven successful in decreasing the incidence of hypersensitivity reactions. In the CALGB 10403 trial, 9 of the first 61 adult patients receiving IV pegaspargase without premedication (15%) experienced ≥Grade 3 hypersensitivity reactions. 29 Subsequently, premedication was implemented, including hydrocortisone, diphenhydramine and acetaminophen. At the University of Michigan, the switch rate to E. chrysanthemi due to hypersensitivity reactions was 24% in 2016 prior to implementing a premedication protocol, and it decreased to 6% in 2017 after implementing the protocol. 55 A similar premedication policy was established at Johns Hopkins Hospital, resulting in a lower switch rate to E. chrysanthemi (from 17% to 8% after policy implementation). 56 Premedication is currently not an established standard of practice. The main concern is that administration of premedications may mask symptoms that may correlate with silent inactivation. To adequately assess for silent inactivation, especially when premedications are used, asparaginase activity levels should be measured. 57 Asparaginase activity levels have been correlated with identification of silent inactivation and outcomes. 58 Use of premedications minimizes hypersensitivity reaction rates and unnecessary switching to the E. chrysanthemi formulation, and measurement of asparaginase activity levels enhances the ability to identify silent inactivation. 59
We developed a standard order set for pegaspargase that includes premedication with acetaminophen 650 mg PO, hydrocortisone 100 mg IV, and diphenhydramine 25 or 50 mg IV prior to pegaspargase administration, and pegaspargase administration restriction to day shift time frame to allow for appropriate staff oversight if a hypersensitivity reaction occurs. Additionally, it is preferred that pegaspargase be given IV instead of IM. If a hypersensitivity reaction occurs, nurses are instructed to stop the infusion and notify the covering physician. Diphenhydramine 50 mg IV, famotidine 20 mg IV, hydrocortisone 100 mg IV, and epinephrine 0.3 mg SQ are available at the bedside and can be given according to a standardized hypersensitivity management protocol. Patients who experience a ≥Grade 3 hypersensitivity reaction to pegaspargase, including anaphylaxis, should not be re-challenged with pegaspargase. Patients may be switched to asparaginase E. chrysanthemi, which has no known cross-reactivity with E. coli-derived products and is FDA-approved for this indication.
Another method of decreasing the risk of pegaspargase-related infusion reaction has been to increase the duration of IV infusion, with 10% of pegaspargase infused over the first hour and remaining 90% infused over the second hour. This has been shown to decrease “allergic-like” reactions. It is postulated that these “allergic-like” reactions are mediated by the known increase in ammonia levels, which can lead to nausea, vomiting, and rash. 60
At the time that Stock et al. 29 published guideline recommendations, the availability of therapeutic monitoring was limited. The asparaginase activity assay has become available at outside clinical laboratories that can provide a value within a few days, making therapeutic drug monitoring viable for identifying silent inactivity due to neutralizing antibodies, especially in the setting of using an H1 blocker to prevent hypersensitivity reactions. Based on consensus expert recommendations from van der Sluis et al., 59 our institution is planning to incorporate an asparaginase activity level seven days after each dose of pegaspargase to assess for silent inactivation. 59 Activity levels < 0.1 IU/mL would necessitate a switch to the E. chrysanthemi formulation. Additional consideration may be given to using this assay to modify subsequent doses to allow for maximum efficacy.
Hepatotoxicity
We recommend to monitor AST, ALT, total bilirubin, and direct bilirubin at baseline and weekly for at least four weeks after each pegaspargase dose.
We recommend administration of vitamin B complex 1 tablet PO twice daily and L-carnitine 50 mg/kg/day IV in six divided doses to patients who develop direct bilirubin >3 mg/dL or transaminase(s) > 3 × ULN. Patients who develop hyperbilirubinemia or transaminitis may receive pegaspargase in future cycles of treatment if the bilirubin/AST/ALT return to normal range and potential clinical benefit is thought to outweigh risk.
Hepatotoxicity is the most common adverse event associated with asparaginase use in adults. Asparaginase hepatotoxicity most commonly manifests as transaminitis and/or hyperbilirubinemia. A commonly described mechanism of drug-induced hepatotoxicity involves induction of oxidative stress. Asparaginase causes oxidative stress by increasing reactive oxygen species (ROS) and causing enhanced mitochondrial permeabilization and subsequent cell apoptosis. For example, in a recent pharmacogenomic study, Alachkar et al. 61 showed that a polymorphism (rs4880) in the superoxide dismutase 2 gene, which is located in the mitochondrial matrix and catalyzes detoxification of mitochondrial superoxide, results in the CC genotype, which was associated with increased asparaginase-related hepatotoxicity, likely due to its effect on mitochondria and subsequent apoptosis of cells. 61 In animal models, L-asparaginase-induced hepatotoxicity occurs more frequently in the setting of hepatic steatosis than in normal livers. 62 In a study looking at four human patients who developed hepatomegaly and abnormal LFTs following L-asparaginase administration, the most consistent pathological change in all cases was diffuse steatosis. 63
Hepatotoxicity is usually reversible and infrequently leads to fulminant hepatic failure. In a single-center study of adult ALL patients, ≥Grade 3 transaminitis and hyperbilirubinemia occurred in 54% and 24% of patients, respectively, and none developed fulminant hepatic failure. The incidence of transaminitis did not vary by cycle, while hyperbilirubinemia was found to be inversely related with cumulative dose. 64 In the UKALL14 trial, fulminant hepatic failure was implicated in mortality. Sixteen of 90 patients died during induction therapy and half of these patients died with sepsis in combination with ≥Grade 3 hepatotoxicity. Other risk factors associated with hyperbilirubinemia included prior-cycle bilirubin elevation, older age, obesity (BMI > 30 kg/m2), BSA > 2 m2, albumin < 3 mg/dL and platelet count <50 K/mm3.48,65
Data were recently published on the incidence of hepatotoxicity in 51 patients who received up to 6 doses of pegaspargase (2000 IU/m2/dose) at least 4 weeks apart as part of a pediatric-inspired ALL regimen, for a total of 192 pegaspargase doses. 66 In this retrospective analysis, high-grade hyperbilirubinemia was more likely to occur during the initial induction phase (19.7%, 10 of the 51 patients). The median time from pegaspargase dosing to onset of hyperbilirubinemia was 13 days and the median time to recovery was 34 days. Hyperbilirubinemia associated with the initial induction dose took longer to recover (45.5 days) than in other phases. While hyperbilirubinemia did delay the next phase of chemotherapy after 12 of the 192 pegaspargase doses administered (6.5%), 11 of the 16 patients who experienced ≥Grade 3 hyperbilirubinemia went on to receive an additional 39 doses of pegaspargase (median 3.5 doses per patient). Per the protocol, these additional doses were not reduced. Only 7 of these 39 additional doses (17.9%) caused recurrence of high-grade hyperbilirubinemia. Similar results were found for patients who developed high-grade transaminitis. Twenty-four of 33 patients (72.7%) who experienced ≥Grade 3 transaminitis went on to receive a total of 78 additional doses of pegaspargase (median 3.3 doses per patient). Fifteen of these 24 patients (62.5%) had at least one recurrence of transaminitis, but only 29 of the total 78 doses administered (37.2%) caused high-grade transaminitis. None of the patients who were re-challenged developed fulminant liver failure. Although the sample size is too limited to draw a definitive recommendation from these data, these results may support administration of additional unreduced doses of pegaspargase in patients with previous pegaspargase-induced hepatotoxicity. This recommendation is in line with the guideline recommendations published by Stock et al. in 2011. 29
As much of the data regarding treatment of hepatotoxicity are anecdotal, no formal recommendations exist for the management of hepatotoxicity due to asparaginase use beyond avoiding alcohol and hepatotoxic drugs during and after treatment. Given the theoretical mechanism of impaired mitochondrial β-oxidation, L-carnitine and vitamin B complex have been proposed as potential agents to reduce the severity and duration of hepatotoxicity. Components of vitamin B complex are precursors of mitochondrial β-oxidation. L-carnitine is an amino acid derivative compound that facilitates the transport of long-chain fatty acids into mitochondria to allow for β-oxidation and has been used to limit the hepatotoxic effects of other medications, such as valproic acid.67,68 Based on published case reports, the use of L-carnitine and vitamin B complex may aid in recovery of hepatic injury from asparaginase without deleterious side effects. In these reports, hepatotoxicity occurred within 28 days of asparaginase administration. Patients presented with significant elevation of total bilirubin and, in three of the six cases, with AST and ALT >3 × ULN. Intravenous L-carnitine was administered at doses ranging from 50 to 450 mg/kg/day in six divided doses. Five of six reports also included vitamin B complex administered PO twice daily. Formulations and doses of vitamin B complex vary among case reports, including niacin (20–50 mg), pantothenic acid (10 mg), pyridoxine (5–10 mg), riboflavin (1.7–10 mg), and thiamine (1.5–15 mg). Five of the six patients survived, and the adverse event profiles of L-carnitine and vitamin B complex were modest.67–70
Our guidelines recommend the use of both L-carnitine and vitamin B complex in the management of asparaginase-induced hepatotoxicity as defined by direct bilirubin >3 mg/dL and/or AST/ALT > 3 × ULN. Intravenous L-carnitine is stable at concentrations from 0.5 to 8 mg/mL. Treatment with the maximum studied dose of 450 mg/kg/day could lead to a total administered volume of 8 L daily. Therefore, given the lack of proven benefit and the risk of fluid overload with higher doses, our institution recommends intravenous L-carnitine dosed at 50 mg/kg/day in six divided doses with duration determined by improvement of hepatic injury and physician discretion. Given the poor bioavailability (∼15%) reported in the package insert, oral L-carnitine is not recommended for initial management of hepatotoxicity unless the patient is not able to tolerate the fluid burden of IV dosing. Doses of L-carnitine may be escalated to 100 mg/kg/day based on ability to tolerate the associated fluid load. Patients with hyperbilirubinemia or transaminitis associated with pegaspargase administration may receive pegaspargase in future cycles of treatment if the bilirubin/AST/ALT return to normal range and potential clinical benefit is thought to outweigh risk.
Pancreatitis
We recommend monitoring amylase and lipase levels at baseline, two to three days after administration of pegaspargase, and then weekly for at least 4 weeks after each pegaspargase dose.
We recommend permanent discontinuation of pegaspargase in patients who develop clinical pancreatitis (i.e. vomiting or severe abdominal pain) with amylase/lipase elevation > 3 × ULN for > 3 days and/or develop a pancreatic pseudocyst. These patients should not receive any other asparaginase products.
Asparaginase-associated pancreatitis is the most common reason for termination of asparaginase treatment. It occurs early during the course of therapy, which suggests that it does not correlate with cumulative dose. 71 Asparaginase products are classified as Class I medications for suspicion of causing pancreatitis, based on more than 20 reported cases of acute pancreatitis with at least one documented recurrence following re-exposure. 72 The incidence of ≥Grade 3 pancreatitis in the pediatric and adolescent population ranges from 2% to 18%. 71 In the adult population, the risk of ≥Grade 2 pancreatitis is estimated to be 13%. 64 In a single-center prospective study of children with ALL at the Dana-Farber Cancer Institute/Boston Children's Hospital between 1987 and 2003, 28 of 403 patients (7%) were diagnosed with acute pancreatitis, which typically occurred early during the course of therapy. Sixteen (57%) of those patients were retreated with asparaginase after recovery from pancreatitis and 10 (63%) had another episode of acute pancreatitis, suggesting a high risk of recurrence with re-exposure to the drug. However, no patient had long-term sequelae. 71
Acute pancreatitis is a reversible process characterized by interstitial edema, infiltration by inflammatory cells, and varying degrees of apoptosis, necrosis, and hemorrhage. Asparaginase-associated pancreatitis has been recognized for more than 30 years, but its mechanism is unknown. 73 We theorize that the injury is due to asparagine and glutamine depletion and subsequent reduction of protein synthesis, particularly in organs such as the liver and pancreas that have high protein turnover.12,14–15,19
Pancreatitis can be classified as either chemical or clinical. Chemical pancreatitis presents as elevation in serum amylase and/or lipase. Clinical pancreatitis is defined by symptomatic manifestations including nausea, vomiting, and epigastric abdominal pain. Tachycardia, hypotension, and fever can also be present. 74 Diagnosis of pancreatitis is based on a combination of clinical, biochemical, and radiographic evidence. In general, pancreatitis can present with mild to severe symptoms, with mortality rates as high as 30% in patients with severe pancreatitis. 74
Management of drug-induced pancreatitis depends on its severity. If clinical manifestations are absent, asparaginase therapy may be continued in the setting of mildly elevated amylase and lipase values, as long as they do not exceed 3 × ULN. Asparaginase therapy should be permanently discontinued for clinical pancreatitis with amylase or lipase elevation >3 × ULN for > 3 days and/or development of pancreatic pseudocyst. Management of pancreatitis includes nothing-by-mouth status, nasogastric decompression, hydration and, in some instances, antibiotics.
Case reports describe the use of octreotide for both treatment and prevention of pancreatitis related to asparaginase or other causes. Somatostatin inhibits secretion of pancreatic digestive enzymes and decreases pancreatic inflammation.75–77 Continuous regional arterial infusion (CRAI) with antibiotics has been shown to prevent complications and reduce mortality in non-asparaginase-related severe acute pancreatitis. Piascik et al. 74 conducted a randomized controlled trial in 78 patients with severe acute pancreatitis. The mortality rate and urgent surgical intervention rate were statistically lower in the CRAI group at 5.1% vs. 23.1% (ITT, P = 0.02) and 10.3% vs. 33.3% (ITT, P = 0.01), respectively. 74 Despite reports of successful use of this treatment for non-asparaginase-related severe acute pancreatitis, data on managing asparaginase-induced acute pancreatitis are limited, and the immunocompromised state of these patients may limit options.
We recommend monitoring amylase and lipase at baseline, two to three days after administration of pegaspargase, and then weekly for at least 4 weeks after each pegaspargase dose. Asparaginase-containing products should be permanently discontinued for clinical pancreatitis (ie. vomiting or severe abdominal pain) with amylase/lipase elevation > 3 × ULN for > 3 days and/or development of pancreatic pseudocyst.
Coagulopathy and thrombosis
Asparaginase-induced coagulopathy presents with varying incidence and severity. The predominant clinical manifestations are serious hemorrhage and thrombotic complications. Coagulopathy occurs due to alterations in procoagulant, anticoagulant, and fibrinolytic factors. The general proposed mechanism of both bleeding and thrombosis is asparaginase-induced endothelial cell and neutrophil activation, leading to increased tissue factor expression. This in turn causes thrombin generation, consumption of coagulation factors and physiological anticoagulants which leads to hypofibrinogenemia, reduced antithrombin and other physiologic anticoagulants, and prolongation of activated partial thromboplastin time (APTT) and prothrombin time (PT). 78
Hemorrhage
We recommend monitoring fibrinogen levels at baseline and three times per week for at least four weeks after the initial dose of pegaspargase and up to three times weekly for at least four weeks for each subsequent dose. If fibrinogen is < 80 mg/dL, replete with 1 unit of cryoprecipitate and ensure adequate repletion by measuring post-repletion fibrinogen level within 24 h. If fibrinogen 80–150 mg/dL and TT > 1.5 × ULN, replete with 1 unit of cryoprecipitate.
We recommend withholding subsequent pegaspargase doses for ≥Grade 2 hemorrhage in conjunction with hypofibrinogenemia until toxicity grade decreases to ≤1 as defined by CTCAE.
Hemorrhage is thought to occur due to low fibrinogen levels. Fibrinogen is critical for clot formation and adequate hemostasis. The mechanism of fibrinogen depletion is unclear and may be either decreased production or excessive fibrinolytic activity (i.e. consumption). 79 Dysfibrinogenemia may contribute to hemorrhage.
Fibrinogen levels were measured serially in 20 children receiving induction chemotherapy including asparaginase for newly diagnosed ALL; the mean level was found to decrease from 290.5 mg/dL pre-treatment to 75 mg/dL two days post asparaginase. 79 In 152 adults receiving repeated pegylated asparaginase doses, fibrinogen levels <100 mg/dL occurred in 48% of patients. 64 In another study, fibrinogen levels were found to be <100 mg/dL in 73% of adult patients who received L-asparaginase; there were 42 bleeding episodes in 31 patients who had a median fibrinogen level of 130 mg/dL. 80
The incidence of all-grade central nervous system (CNS) and non-CNS bleeding reported in the literature ranges from 2% to 12%.46,64,81 Incidence of bleeding was comparable in patients treated with E. coli asparaginase and pegaspargase, but patients treated with pegaspargase had longer durations of coagulation dysfunction. 82 In a study by Aldoss et al., bleeding of any grade occurred in 5% of patients; 75% of those patients were continued on pegaspargase in subsequent cycles without recurrence of bleeding. Bleeding was more likely to occur after the first cycle of therapy, as opposed to subsequent cycles. 64
Fresh frozen plasma (FFP), cryoprecipitate, or fibrinogen concentrate (not readily available in the US) are used for repletion of fibrinogen.
The use of cryoprecipitate for fibrinogen replacement is not based on rigorous evidence and because it contains fibrinogen, von Willebrand factor and factors VIII and XIII and is a multi-donor product, it must be used with caution. There is certainly a theoretical risk of thromboembolic events associated with cryoprecipitate supplementation. This effect may be counteracted by use of recommendation of prophylactic anticoagulation in patients receiving pegaspargase. The International Society on Thrombosis and Haemostasis (ISTH) Scientific and Standardization Committee recommends use of cryoprecipitate in bleeding-predominant disseminated intravascular coagulation (DIC) with low fibrinogen levels, but notes that the recommendation is based on low quality of evidence. 83 FFP is not routinely used because it contains asparagine and could theoretically counteract the benefit of asparaginase. It must be acknowledged that there are other exogenous sources of asparagine, including foods, that are not routinely avoided. 84 A prospective study in children receiving ALL induction therapy including L-asparaginase evaluated the use of prophylactic FFP when fibrinogen levels fell below 60 mg/dL. FFP (5–20 mL/kg) only minimally increased fibrinogen levels. 85 The volume of FFP required to increase fibrinogen levels is greater than that of cryoprecipitate. Fibrinogen concentrates, which are not readily available in the US, are indicated for prophylaxis and treatment of bleeding in congenital and acquired fibrinogen deficiency states; efficacy of these products in preventing bleeding has been documented in several acquired settings including DIC.86,87 Despite a measurable correctable fibrinogen level with replacement, there is an absence of data on whether use of replacement therapy actually decreases the incidence of bleeding in ALL patients who receive asparaginase.
Recommendations for bleeding prophylaxis vary, including use of cryoprecipitate repletion based on differing fibrinogen levels or based on bleeding only. GRAALL recommends that adult patients receive cryoprecipitate prophylactically when fibrinogen levels are <50 mg/dL.80,88 The Mayo Clinic recommends repletion when fibrinogen levels are <100 mg/dL. 29 Those who recommend only using repletion if bleeding is noted may be basing their recommendations on the fact that repletion of fibrinogen has not been proven to decrease the incidence of bleeding, and that pegaspargase-induced coagulopathy tends to promote thrombosis rather than hemorrhage.
Our guideline recommends that fibrinogen levels be monitored three times weekly after pegaspargase administration. If levels are < 80 mg/dL or if fibrinogen is 80 to 150 mg/dL with TT > 1.5 × ULN, 1 unit of cryoprecipitate is administered with the goal of preventing hemorrhage. We based our selection of 80 mg/dL on international guidelines of minimal fibrinogen concentration above 80–100 mg/dL, despite paucity of information to support various levels. 89 Active hemorrhage due to low fibrinogen levels is also treated with fibrinogen repletion with cryoprecipitate. However, this is done cautiously due to the high concentrations of factor VIII, which is considered thrombogenic, in cryoprecipitate.
Thrombosis
Thromboprophylaxis
We recommend administering enoxaparin to all patients for at least four weeks after each pegaspargase dose – enoxaparin 40 mg SQ daily for patients <80 kg and 60 mg SQ daily for patients ≥80 kg. Patients must meet the following criteria: not already receiving therapeutic anticoagulation; platelet count ≥30 K/μL; absence of significant bleeding; creatinine clearance ≥30 mL/min.
We recommend monitoring antithrombin III levels at baseline and twice weekly for at least four weeks after each pegaspargase dose (or until two sequential levels normalize to >50%). Replete antithrombin III when level is ≤50%.

Treatment of thrombosis
In patients who are hospitalized with tenuous clinical status, we recommend using UFH for treatment of thrombosis:
PTT goal 1.5–2 × ULN for upper extremity or line-associated DVT PTT goal 2–3 × ULN for all other thromboses if platelets ≥30 K/μL. In patients with stable clinical status, including outpatients, we recommend the use of LMWH at the provider's discretion: Enoxaparin 1 mg/kg twice daily if platelet count is >50 K/μL Enoxaparin 0.5 mg/kg twice daily if platelet count is 30–50 K/μL
If platelet < 30 K/μL, the risk of bleeding versus the benefit of anticoagulation is determined per discretion of the treating physician.
Antithrombin (AT) is a circulating factor belonging to the serine protease inhibitor family that is responsible for up to 60% of the plasma anticoagulant activity.90,91 The effect of asparaginase on antithrombin synthesis is more profound than for other coagulation proteins, and this can explain why thrombotic complications occur more frequently than bleeding. 92 Clinically, AT levels were shown to be markedly lower after L-asparaginase administration, with median AT levels of 59% after the fourth infusion, decreased from 120% prior to the first infusion. 80
The reported incidence of thrombotic complications in adult patients receiving asparaginase has ranged from 6% to 34%.81,92,93 This large variation is due to inclusion of reports of both symptomatic thrombosis and thrombotic events identified by screening. The CAPELAL study reported low antithrombin levels after the fourth infusion of asparaginase, with thrombotic events in 9% of patients. 80 In a meta-analysis, the incidence of clinically apparent events was 6%. 94 In one multivariate model, age was found to be the only predictor of increased incidence of VTE. 90 Other contributing factors implicated include presence of an indwelling venous catheter and use of steroids, with lower thrombosis rates in patients receiving dexamethasone compared to prednisone.93,94 Additionally, external prothrombotic factors (immobility, malignancy, age, etc.) contribute to thrombotic events.
Given the high incidence of thrombotic events with asparaginase use, thromboprophylaxis is a key concept. Thromboprophylaxis has been described with use of LMWH alone, in combination with antithrombin, or solely with antithrombin. Most of the data for thromboprophylaxis come from the pediatric literature and from patients receiving L-asparaginase rather than pegaspargase. In one prospective single-center study, children received prophylactic LMWH every 24 h throughout the entire duration of asparaginase therapy. No patients developed thrombosis while receiving LMWH. This was informally compared to a historical cohort of patients who did not receive prophylaxis, which experienced a 4% thrombotic rate. Furthermore, no patients had bleeding from use of anticoagulation. 95 A second study evaluating the use of DFCI-based treatment regimen in adults observed a high incidence of thrombosis, warranting a protocol amendment to include routine thromboprophylaxis with LMWH. Thrombosis rates in patients treated post-amendment were 6% during induction therapy and 29% during consolidation, compared to 10% and 41% in the pre-amendment patients. This study also did not identify any ≥Grade 3 bleeding in the patients receiving LMWH. 96 A third retrospective study evaluated the use of enoxaparin in adults receiving intensification phase of the DFCI 91-01 protocol. Compared to a historical cohort of no thromboprophylaxis, rates of thrombosis were 18.9% in the enoxaparin group and 21.7% in the historical cohort. Minor bleeding occurred in 8% of patients receiving enoxaparin, but no major bleeding was identified. 97 Of note, these studies evaluating LMWH alone as thromboprophylaxis did not detect a statistically significant decrease in thrombosis rates, although a numerical reduction was seen. Importantly, these studies showed the practice using LMWH prophylaxis was safe with low rates of minor bleeding. The authors additionally acknowledge the limitation of prolonged daily injections of LMWH and potential added cost to the patient; however, we believe that reducing the risk of thrombosis outweighs these limitations.
Regarding the use of AT, the PARKAA trial was a prospective single-center study that assigned children to receive or not receive AT. Thrombotic events occurred in 28% vs. 37%, respectively. Though an absolute reduction in thrombosis was seen, these results were not statistically significant. 98 In a single-center prospective study of patients receiving asparaginase-based therapy for ALL, antithrombin replacement was initiated at AT levels <70%. There was a significant reduction in the incidence of thrombosis from 33% to 0% with replacement therapy. 99 In contrast, a recently published single center retrospective study of adult patients with ALL who received pegaspargase showed there was no significant decrease in thrombotic events in patients who received AT replacement. 100 In the CAPELAL trial, adults received AT if their measured level was <60%. The rate of thrombosis in AT-treated vs. non-AT treated patients was 5% vs. 12% (P = 0.04). However, the design of these comparator arms may have been improved by comparing AT repletion vs. no AT repletion at similar antithrombin levels. 80 The most robust study to date is a single-center study that assigned children to receive AT along or in combination with LMWH. In the AT alone group, there was a 13% incidence of thrombosis compared to the AT + LMWH group, which had a 0% rate of thrombosis (P < 0.05). 101 This trial serves as the basis of our thromboprophylaxis recommendation, as it is one of the few prospective comparator trials evaluating thromboprophylaxis and has a remarkable thrombosis rate of 0% in the combination therapy arm.
With the high incidence of thrombocytopenia in patients receiving leukemia treatment, the benefit of thromboprophylaxis with LMWH must be weighed against the risk of bleeding. The use of prophylactic doses of enoxaparin is described in a recent publication by Sibai et al. In this retrospective study, subjects <80 kg received enoxaparin 40 mg daily, while those ≥80 kg received enoxaparin 60 mg daily during intensification chemotherapy that included asparaginase. Subjects who had a platelet count < 30 K/μL had their anticoagulation temporarily stopped. No patients reported clinically significant bleeding, and the incidence of minor bleeding was low (8%). 97
Low-molecular-weight heparin remains the preferred anticoagulant for the acute management of cancer-related thrombosis, given its superiority over warfarin and ability to be administered in the outpatient setting, in contrast to UFH.102,103 However, in patients with tenuous clinical status who are hospitalized, UFH may be preferable, given a much shorter half-life. In the inpatient setting, we use UFH as the anticoagulation agent of choice, with LMWH as an alternative in patients who are clinically stable and have appropriate renal function.
Frequent thrombocytopenia in this patient population also creates a challenge for safe anticoagulation of an acute thrombosis, given the increased risk of bleeding from two independent processes. Current guidelines consider platelets <50 K/μL as a relative contraindication to anticoagulation, but the risk of progressive or recurrent thrombosis without anticoagulation remains, despite thrombocytopenia. 102 A recent publication from Memorial Sloan Kettering Cancer Center describes success with enoxaparin dose reduction in the setting of thrombocytopenia. In this study, patients received full-dose enoxaparin (1 mg/kg twice daily, or 1.5 mg/kg daily) for platelets >50 K/μL, 50% dose-reduced enoxaparin for platelets 25 to 50 K/μL, and no anticoagulation for platelets <25 K/μL. No recurrent thrombosis and no major bleeding occurred. 104 Oliver et al. published retrospective experience with patients with acute leukemia and central venous catheter VTE at our institution. Venous thrombosis resolved in 80% in the anticoagulation (AC) group vs. 45% in the non-anticoagulation group (P = 0.11). Of the AC group, 67% were alive compared to 29% in the non-AC group (median survival nine months, HR 0.32, P = 0.015). This study highlights both the efficacy and mortality benefit of treating thrombosis. 105 These results serve as the basis for our enoxaparin dosing for acute thrombosis in our institution's guidelines.
Heparin-based products cause a conformational change in antithrombin which significantly enhances antithrombin activity. 106 Therefore, without adequate levels of antithrombin, patients may have inadequate benefit from heparin. Asparaginase-based products can induce an acquired antithrombin deficiency. 78 Therefore, the role of antithrombin repletion in the management of an acute thrombosis due to pegaspargase should be considered. In a description of thrombosis management practices at the Dana Farber Cancer Institute, all pediatric patients with an active thrombosis in AT-treated versus non-AT treated patients had antithrombin activity monitored at least once weekly and had repletion when activity was lower than 50% to 75%, in addition to receiving anticoagulation therapy with either warfarin or LMWH. 81 Antithrombin monitoring did not occur as frequently in the adult population in this observational study, with antithrombin monitoring in only 1 of 14 adults. However, it is acknowledged that the adult population may benefit from monitoring and replacement, particularly due to their overall increased risk of thrombosis compared to children. It was noted that the adult population had an increased risk of VTE recurrence, though it is difficult to attribute this to lack of antithrombin monitoring and replacement since other confounders were also present. None of the patients receiving anticoagulation with antithrombin repletion experienced major bleeding events.
Current recommendations suggest an antithrombin repletion threshold of <60% in the setting of both prevention and active management of thrombosis, but the optimal level of repletion is unknown. Additionally, the high cost of antithrombin therapy is noted, with average wholesale price of $4.66 per unit and typical doses >1000 units.
107
In a study by Barreto et al. evaluating antithrombin repletion thresholds, the authors noted no difference in thrombosis incidence with repletion at <80% versus < 60%.
108
With these repletion thresholds, median expenditure was $35,000 per patient, and median cost $118,000 per patient receiving pegaspargase on the CALGB 10403 protocol. In an effort to contain this cost, our institution adopted the lower antithrombin threshold of 50%, with a repletion goal of 80%. This lower threshold is the physiologic threshold used to define type I antithrombin deficiency per laboratory reference range and is the repletion threshold used by Meister et al.,
101
upon which our prevention practices are based. Antithrombin repletion is calculated as follows
109

Conclusion
This guideline was created and implemented at the University of Maryland Marlene and Stewart Greenebaum Comprehensive Cancer Center to standardize toxicity prevention and management and improve patient safety. We are prospectively monitoring the impact of implementation of this guideline and outcomes will be reported at a later date.
Recommendations
Dosing strategies
Pegaspargase 2500 IU/m2 intravenously (IV) capped at 1 vial (3750 IU) for all non-study adult patients.
Hypersensitivity reactions
Intravenous administration and premedication with acetaminophen, hydrocortisone, and diphenhydramine to prevent hypersensitivity reactions. Permanent discontinuation of pegaspargase and switching to Erwinase® (Erwinia chrysanthemi) for patients who experience a ≥Grade 3 severe hypersensitivity reaction.
Hepatotoxicity
Monitor aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin, and direct bilirubin at baseline and weekly for at least four weeks after each pegaspargase dose. If direct bilirubin > 3 mg/dL or liver function tests (LFTs) > 3 × upper limit of normal (ULN) administer vitamin B complex one tablet by mouth (PO) twice daily and L-carnitine 50 mg/kg/day IV in six divided doses. Patients with pegaspargase-induced hyperbilirubinemia or transaminitis may receive pegaspargase in subsequent cycles of treatment if the bilirubin/AST/ALT return to normal range and potential clinical benefit outweighs risk.
Pancreatitis
Monitor amylase and lipase at baseline, two to three days after administration of pegaspargase, then weekly for at least four weeks after each pegaspargase dose. Permanently discontinue pegaspargase in patients who develop clinical pancreatitis (e.g., vomiting or severe abdominal pain) with amylase/lipase elevation > 3 × ULN for > 3 days and/or develop pancreatic pseudocyst. These patients should not receive any other asparaginase products.
Hemorrhage
Monitor fibrinogen at baseline and three times per week for at least four weeks after the initial dose of pegaspargase and up to three times per week as needed for at least four weeks for each subsequent dose. If fibrinogen < 80 mg/dL, replete with 1 unit of cryoprecipitate and ensure adequate repletion by measuring post-repletion level within 24 h. If fibrinogen 80–150 mg/dL and thrombin time (TT) > 1.5 × ULN, replete with 1 unit of cryoprecipitate. Withhold subsequent pegaspargase doses for ≥Grade 2 hemorrhage in conjunction with hypofibrinogenemia until toxicity ≤Grade 1 as defined by Common Terminology Criteria for Adverse Events (CTCAE).
Thromboprophylaxis
Administration of enoxaparin to all patients for at least four weeks after each pegaspargase dose-enoxaparin 40 mg subcutaneously (SQ) daily for patients <80 kg; enoxaparin 60 mg SQ daily for patients ≥80 kg. Patients must meet the following criteria: not already receiving therapeutic anticoagulation; platelet count ≥30 K/μL; absence of significant bleeding; creatinine clearance ≥30 mL/min. Monitor antithrombin III level at baseline and twice weekly for at least four weeks after each pegaspargase dose (or until two sequential levels normalize to >50%). Replete antithrombin III when level is ≤50%.

Treatment of thrombosis
In patients who are hospitalized with tenuous clinical status, we recommend using unfractionated heparin (UFH) for treatment of thrombosis:
·PTT goal 1.5–2 × ULN for upper extremity or line-associated deep vein thrombosis (DVT) ·PTT goal 2–3 × ULN for all other thromboses if platelets ≥30 K/μL. In patients with stable clinical status, including outpatients, we recommend the use of low-molecular-weight heparin (LMWH) at the provider's discretion:
·Enoxaparin 1 mg/kg SQ twice daily if platelet count is >50 K/μL ·Enoxaparin 0.5 mg/kg SQ twice daily if platelet count is 30–50 K/μL ·If platelet < 30 K/μL, the risk of bleeding versus the benefit of anticoagulation is determined per discretion of the treating physician.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.