
Abstract
Background
Antineoplastic-induced nausea and vomiting (AINV) is a treatment-related issue that can have significant negative influences on the cancer patient’s quality of life. Assessment of nausea is challenging in children as few studies include the perception of nausea as an outcome, and the severity is rarely evaluated with the use of a validated instrument. We describe our experience of integrating an AINV tool into patient care at the Alberta Children’s Hospital.
Results
AINV tool uptake was low: 47 (22%) eligible chemotherapy cycles utilized the tool (24 (32%) and 23 (16%) cycles of HEC and MEC, respectively, (p < 0.01)). Ifosfamide-containing cycles received the highest nausea ratings, with nausea severity correlated with agent emetogenicity. Mean nausea rating was 2.07 versus 1.76 for patients receiving HEC or MEC, respectively. Clinical pharmacists performed 1.24 AINV interventions per day. Patient satisfaction with AINV care overall was high; however, 51% of patients indicated that the tool led to no changes in nausea symptoms.
Conclusions
AINV tool uptake was low with limited value in improving outcomes. Incorporation of nausea assessment into the electronic health record and potential use of a mobile application may improve uptake.
Keywords
Introduction
Antineoplastic-induced nausea and vomiting (AINV) is a frequent treatment-related issue that has significant negative influences on the cancer patient’s quality of life. 1 The Pediatric Oncology Group of Ontario (POGO) defines optimal control of acute AINV as no vomiting, no retching, no nausea, no use of antiemetic agents other than those given for AINV prevention and no nausea-related change in the child’s usual appetite and diet. 2 Optimal acute AINV control should be achieved on each day that antineoplastic therapy is administered and for 24 h after administration of the last antineoplastic agent of the therapy block. 2 Patients often receive moderately (MEC) or highly emetogenic chemotherapy (HEC), carrying a 30 to 90% or greater than 90% risk of emesis, respectively, in the absence of prophylaxis. 3 Compared to that of adults, overall data about effective antiemetic medication regimens in children are sparse. Pediatric regimens are also typically administered over prolonged periods of time and often employ multiple agents administered over several days.2,4 Although acute antineoplastic-induced vomiting (AIV) may improve over the course of treatment, antineoplastic-induced nausea (AIN) may become more problematic. 2
A recent retrospective review of inpatient chemotherapy regimens at four Canadian pediatric centres reported the majority of patients (87%) received HEC, indicating that many patients receive therapy with a significant risk of emesis. 5 Nausea was not assessed in this report, as the authors were unable to determine its incidence due to the lack of documentation in the health record and participating sites did not use a validated nausea assessment tool. 5
Tool development and implementation
An examination of the literature identified several validated nausea assessment tools. The Multinational Association of Supportive Care in Cancer (MASCC) developed and validated the MASCC Antiemesis Tool (MAT) in adult cancer patients and their caregivers in both the UK and the US.4,6 The MAT is a self-assessment tool that can be integrated into patient care to facilitate discussion between clinicians and patients regarding the experience of nausea and vomiting, but the tool was not designed for use nor validated in pediatric patients. 4 The BARF (Baxter Retching Faces) scale was developed with oncology patients but only validated in non-oncology patients aged 7 to 18 years. 7 The PeNAT (Pediatric Nausea Assessment Tool) was developed and validated in patients aged 4 to 18 years including patients with cancer who have received chemotherapy or a hematopoietic stem cell transplant. 1 The wide use of the PeNAT has thus far not been reported in the literature. Other nausea assessment tools may also be in use, but little information is available describing the tool itself or its use in clinical practice.
The clinical pharmacist team of the Hematology, Oncology, Blood and Marrow Transplant (HOT) program at the Alberta Children’s Hospital (ACH) saw an opportunity to optimize the antiemetic therapy for oncology patients. ACH staff had implemented the use of the POGO guidelines 3 for AINV prevention in 2014 and in 2016 adapted the antiemetic guidelines into institutional guidelines; major changes included a lower initial dose of dexamethasone and increasing use of aprepitant. Independent pharmacist prescribing of antiemetic therapy had been occurring for some time; however, the clinical pharmacists determined that optimal assessment of nausea could improve AINV management. The PeNAT was chosen as the tool for routine assessment of nausea due to its validation in the pediatric oncology patient population. The HOT pharmacy team created a paper-based patient self-documentation tool that integrated the PeNAT with documentation of antiemetic medications and vomiting occurrences to enable expanded use into the ambulatory setting. The tool was trialed with two patients and their caregivers, one in the inpatient setting and the other in the ambulatory clinic while also testing integral age-related differences in PeNAT script and administration. The tool was revised based on the feedback received; ultimately, four individual tools were created to allow for the self-assessment of nausea in the acute and ambulatory settings according to patient age.
This study seeks to evaluate the use of a validated, standardized tool to assess antineoplastic-induced nausea and vomiting for pediatric oncology patients.
Methods
In February 2017, use of the AINV assessment tool was routinely integrated into the clinical pharmacist assessment of antiemetic therapy for oncology patients in the HOT program. The clinical pharmacists provided and reviewed the tool with patients and their caregivers; patients were instructed to self-report perception of nausea (utilizing the PeNAT) twice daily and document any occurrence of emesis for the duration of and for 24 h after the last dose of antineoplastic therapy (see supplementary material). Clinical pharmacists performed ‘check-ins’ with the patients on each day of therapy, assessing and documenting AINV control. Patients/caregivers were requested to return the AINV tool to the study team at their next assessment.
Patients
A retrospective chart review of acute care and ambulatory clinic patients aged 4 to l7 years receiving their second or greater HEC or MEC course between February and August 2017 were included. Regimen emetogenicity was classified as per the POGO guidelines. 3 Patients were identified through the electronic health record or through pharmacy records; data collected for eligible cycles included patient demographics; location of chemotherapy administration (acute care or ambulatory setting); chemotherapy regimen; antiemetic regimen, emesis as well as nausea ratings per day of therapy. Clinical pharmacist interventions were retrieved from the electronic health record. Patients were excluded if English was not their first language; age was less than four years; if in the opinion of the clinical pharmacist, the patient was unable to complete the AINV tool; or if the patient or caregiver refused to use the AINV tool.
Patients identified through the electronic health record as completing the AINV tool were approached to complete a patient and parent/caregiver satisfaction survey. Surveys questions were created with the assistance of a clinical psychologist, using previous published survey questions8–10 and adopted for appropriate pediatric age ranges based on the format in the PedsQL version 4.0.11–13 Questionnaires were administered by a pharmacy student at the time of follow-up visits.
Written informed consent was provided by all parents and/or caregivers, with patients aged eight years and older providing assent prior to the completion of the survey. This study was approved by the Health Research Ethics Board of Alberta, Cancer Committee.
Outcomes
The primary outcome was the proportion of HEC or MEC cycles where patients received the AINV tool between February and August 2017; to assess impact of time after implementation, the study timeframe was divided into two subgroups (1 February – 31 May and 1 June – 31 August). Secondary outcomes include describing nausea severity, AINV control, as well as the interventions performed by the clinical pharmacist such as the frequency of patient teaching, antiemetic prescribing and response assessment, antiemetic therapy changes, and drug interaction assessments. In addition, patient and caregiver satisfaction with tool utilization will be described.
Statistical analysis
We estimated that of cycles that met the inclusion criteria, the AINV tool would be used on 10 occasions per month, leading to a total of 60 to 70 AINV tool completions throughout the study period, serving as our convenience sample. Descriptive statistics were used to analyze baseline characteristics. The primary outcome is reported as the overall proportion of both HEC and MEC cycles where patients received the AINV tool from the total number of cycles administered, Chi-squared test was used to compare the groups. Pharmacist interventions and nausea ratings were quantified and described. Total acute AINV control (no vomiting, no retching, mean nausea rated as <2 throughout chemotherapy and for 24 h after the completion of chemotherapy and no use of antiemetics other than for prophylaxis) is reported as a proportion of patients (both HEC and MEC) who achieved total control from the total number of patients who completed the AINV tool. The patient and caregiver surveys consisted of questions with responses rated on a modified Likert scale (from 1 for “strongly disagree” to 5 for “strongly agree”). Responses were described, with a paired t-test used to compare the mean response between groups.
Results
Tool use
From February to August 2017, 74 patients receiving 217 cycles of chemotherapy were eligible to receive the AINV tool, Figure 1. Patient characteristics and AINV tool utilization are summarized in Tables 1 and 2, respectively. Chemotherapy cycles were most often administered to patients greater than 13 years of age (97 cycles, 45%). The most common diagnosis was ALL (acute lymphoblastic leukemia, 76 cycles, 35%) followed by Ewing sarcoma (36 cycles, 17%). Overall uptake of the tool was low: 47 (22%) of eligible chemotherapy cycles utilized the AINV tool; 24 cycles of HEC (32%) versus 23 cycles of MEC (16%), p < 0.01. Patients received the majority of their chemotherapy in the ambulatory clinic versus the acute care setting (136 cycles vs. 81 cycles); however, use of the tool was similar with both settings (20% of ambulatory and 25% of acute care cycles, p = 0.41). There was no difference between the proportion of tool used in February–May or June–August timeframes (21% vs. 22%, p = 0.88).
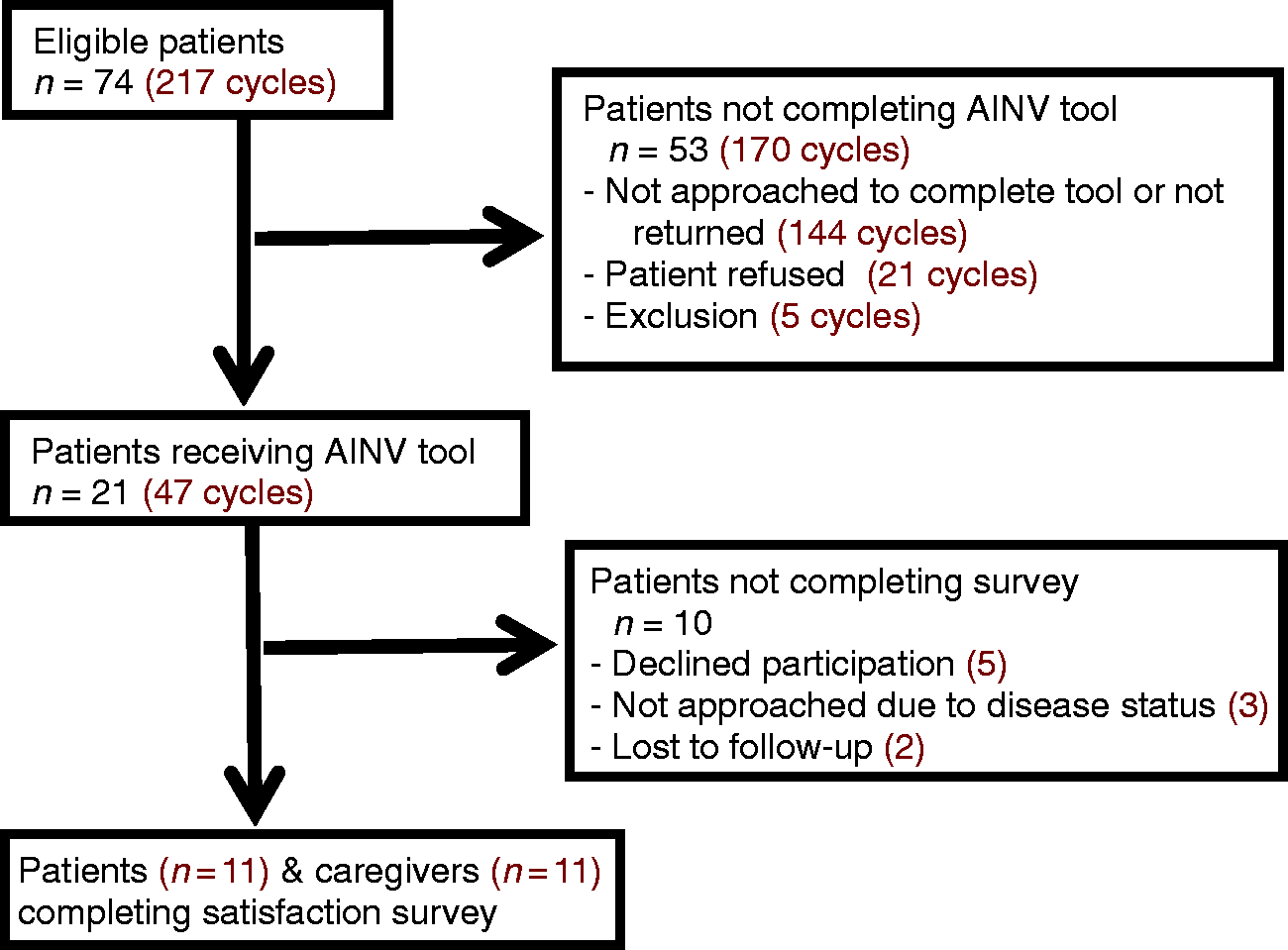
Patient inclusion.
Patient characteristics.
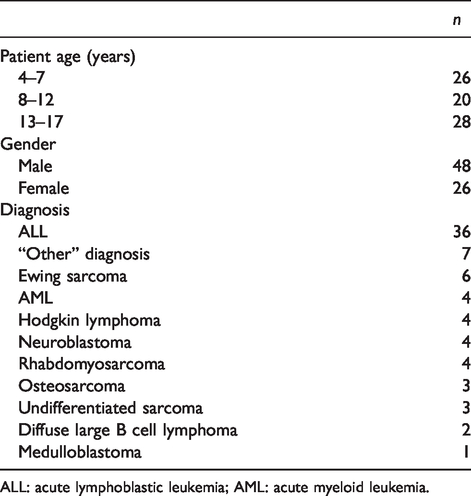
ALL: acute lymphoblastic leukemia; AML: acute myeloid leukemia.
AINV tool utilization.
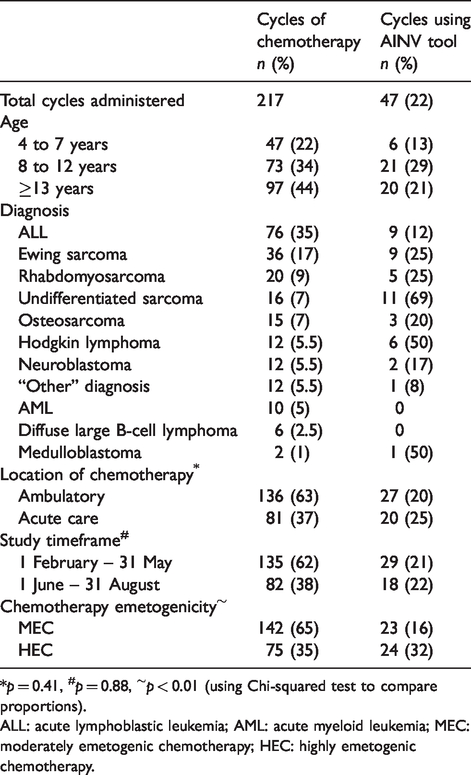
*p = 0.41, #p = 0.88, ∼p < 0.01 (using Chi-squared test to compare proportions).
ALL: acute lymphoblastic leukemia; AML: acute myeloid leukemia; MEC: moderately emetogenic chemotherapy; HEC: highly emetogenic chemotherapy.
Nausea severity and AINV control
Complete AINV data were available for the analysis for 21 cycles of chemotherapy (8 HEC and 13 MEC). The mean nausea rating over the entire course was higher for patients receiving HEC (2.07) than MEC (1.76), see Table 3. The most nauseating chemotherapy regimens, as outlined in Table 4, were ifosfamide-containing combination regimens that received maximum nausea rating of 4. Maximum nausea ratings of 3 were reported for patients receiving: doxorubicin and cisplatin; intravenous (IV) methotrexate (MTX) 5 g/m2/dose; vincristine and irinotecan; and ifosfamide. Total acute AINV control was achieved in six cycles (29%), all in patients receiving MEC with IV MTX 5 g/m2/dose.
Nausea severity and total control by chemotherapy emetogenicity. a
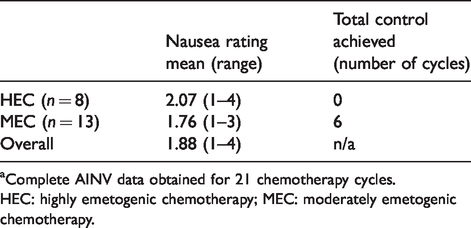
aComplete AINV data obtained for 21 chemotherapy cycles.
HEC: highly emetogenic chemotherapy; MEC: moderately emetogenic chemotherapy.
Nausea severity by chemotherapy regimen.
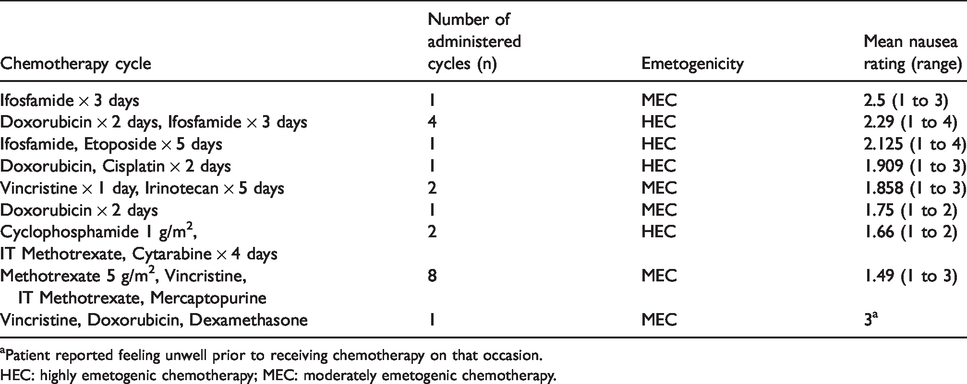
aPatient reported feeling unwell prior to receiving chemotherapy on that occasion.
HEC: highly emetogenic chemotherapy; MEC: moderately emetogenic chemotherapy.
Pharmacist interventions
Pharmacists performed a mean of 1.24 documented clinical intervention related to AINV per weekday over the course of the study period. There were 117 drug therapy assessments, with prescribing (97), patient and/or caregiver teaching (66) and assessing for drug interactions (13) occurring most frequently (Table 5). Antiemetic modifications were made in response to inadequate therapy, as assessed by patient response to antiemetics and antiemetic ordering in relation to chemotherapy emetogenicity (37); family request (3); or adverse event (2); and no modifications were required after assessment in 31 instances.
Documented pharmacist clinical interventions related to AINV care.
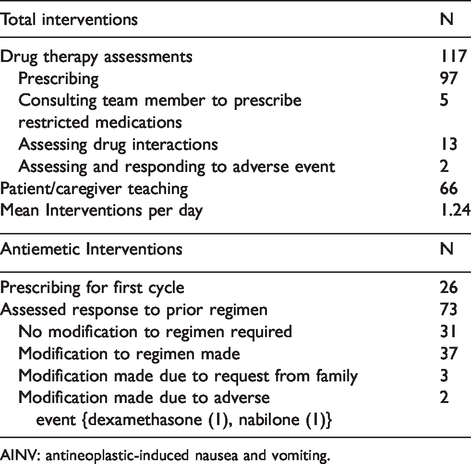
AINV: antineoplastic-induced nausea and vomiting.
Satisfaction surveys
Of the 21 patients who were identified as receiving the AINV tool, 11 patients and 11 caregivers completed the AINV satisfaction surveys for a total of 22 survey responses. Ten patients did not complete the survey: patient/caregiver declined (5), patient not approached due to a change in clinical status (3) or patient was lost to follow-up (2). Surveys were completed by patients aged 4–7 (5), aged 8–12 (1) and aged 13–17 (5) and parents/caregivers (11). Survey questions and Likert scale responses for parents/caregivers and children aged 8 to 17 (17 responses total) are collated in Table 6, while mean responses are available in supplementary material. There was no statistical difference between the mean scores for any survey statements from the patient or caregiver groups. Overall, those surveyed strongly agreed that patients were able to understand the concept of nausea, that the tool was easy to use and that they knew who to contact if there were concerns about nausea and/or vomiting. Patients did not feel that the tool took too much time to use and parents felt the time it took to complete the tool each day was acceptable. However, use of the tool was not felt to help control nausea, increase knowledge about antiemetic medications, or increase the dialogue about nausea with the care team. Finally, overall care provided by the health care team in regards to nausea and vomiting control was reported as good (2), very good (7) or excellent (8).
Summarized patient (ages 8 to 17) and caregiver satisfaction survey results. Patients and caregivers were provided with 12 statements and response ranking performed utilizing a Likert Scale, where 1 is strongly disagree and 5 is strongly agree. a
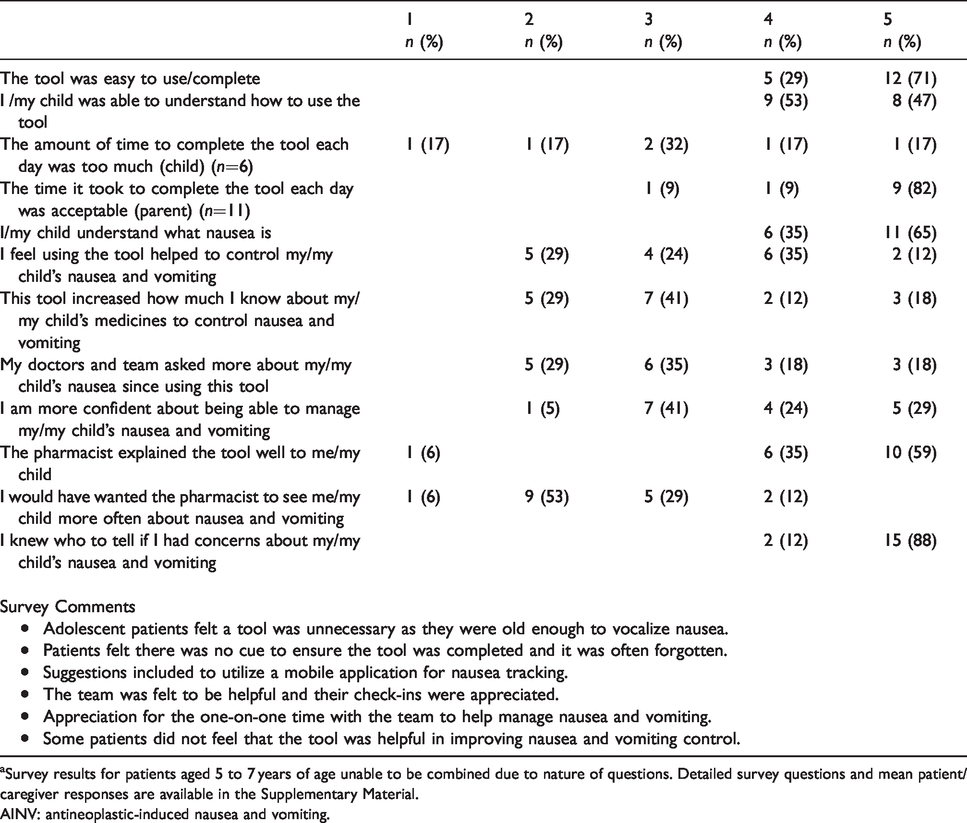
aSurvey results for patients aged 5 to 7 years of age unable to be combined due to nature of questions. Detailed survey questions and mean patient/caregiver responses are available in the Supplementary Material.
AINV: antineoplastic-induced nausea and vomiting.
Discussion
The AINV tool was developed, trialed, and revised with a simplified patient script and modified for the ambulatory setting after feedback from patients. It was then implemented into clinical care in February 2017 after training was provided to clinical pharmacists at ACH. Our experience indicates that incorporating an AINV tool into practice was difficult, in that only 22% of eligible chemotherapy cycles received the AINV tool. Identification of emetogenicity, practice differences between prescribers and the guidelines when rating emetogenicity, and time constraints due to workload were identified as challenges that limited the use of the AINV tool. When analyzed by emetogenicity, a statistically greater proportion of HEC cycles utilized the tool (32% vs. 16%), which may be related to the clinical pharmacist perception that HEC regimens were more likely to lead to nausea and thus the tool would be more useful. Of the 142 cycles that were classified as MEC, 60 (42%) contained intrathecal (IT) chemotherapy as the only moderately emetogenic agent and the ACH clinical pharmacists did not distribute the tools to these patients. Excluding IT only cycles led to 28% of MEC cycles receiving the tool, demonstrating more consistency with tool utilization with HEC cycles. Although POGO guidelines classify IT chemotherapy as MEC, 3 there are various clinical factors that may also contribute to nausea and vomiting, for example fasting prior to the lumbar puncture procedure or the sedation agents used. 14 A recent report found that IT MTX-induced vomiting was well controlled with 5-HT3 receptor antagonists but nausea still occurred in 49% of patients receiving IT MTX, indicating an ongoing unmet need for some patients. 14
Patients receiving HEC reported a higher mean and range for nausea severity over the entire course versus patients who received MEC, suggesting that risk of nausea may be in part related to risk of emesis. The highest nausea rating of 4 was reported in patients who received ifosfamide-containing chemotherapy combinations. At ACH, patients who receive ifosfamide are not eligible to receive aprepitant due to risks of neurotoxicity as the metabolites of ifosfamide (both active and toxic) are produced after metabolism by CYP3A4, of which aprepitant is a substrate and an inhibitor. 2 Patients instead receive a 5HT3 receptor antagonist, dexamethasone, and an additional agent such as olanzapine, lorazepam, or nabilone as dictated by prescriber preference. Aprepitant has been shown to improve AIV control in children receiving HEC or MEC who were given ondansetron with or without dexamethasone15–17; however, due to gaps in evidence regarding the impact of the interaction of aprepitant with ifosfamide and other common pediatric chemotherapy agents,2,15–17 it is likely patients administered ifosfamide experience poorer control.
Pharmacists at ACH are directly involved in patient teaching, antiemetic prescribing, assessment, and managing drug interactions and adverse effects for patients receiving chemotherapy. Over the study period, pharmacists performed a mean of 1.24 clinical interventions per day. This is likely an underestimation of interventions, as recommendations made by the pharmacist to the healthcare team may not have been documented in clinical pharmacy notes, while interventions made during chemotherapy order review were also not included. Patient response to antiemetic regimen was documented on 73 occasions, with no adjustment required in 42% of cases.
As the return rate for the paper AINV tool was less than half of the cycles, (45%) complete data were only available for 21 cycles. Total complete acute AINV control was achieved in 6 (ALL patients administered IV MTX 5 g/m2) of 21 evaluable cycles (29%) (Table 3).
Satisfaction surveys were completed by 11 patients and their caregivers. Responses were collated and summarized in Table 5, with no statistical difference in mean scores between the two groups. All patients refusing the tool were between 13 and 17 years of age, perhaps indicating that nausea assessment and documentation in this age group could be better achieved by utilizing an adult tool such as the MAT, or on a mobile platform. Validation of that tool in this age group should be undertaken.
Respondents indicated that the use of the tool itself was not felt to assist in nausea control or improve knowledge about antiemetic regimens. This is likely due to the fact that nausea is only one element of the AINV continuum, and that a paper assessment tool does not replace the need for directed patient-care team assessment and re-assessment of AINV each time a new cycle of chemotherapy is planned. Tool uptake was lower than expected, and feedback from patients, caregivers, and team members indicated that the use of the paper form for nausea reporting, emesis and antiemetic documentation was onerous. While reporting and tracking patient reported nausea is essential to assess the entirety of the AINV experience, communicating the patient experience to the health care team will allow for more timely management of AINV. The use of mobile applications or electronic health records should be explored to enable better sharing of patient symptoms.
Limitations of our study include the single institution design and the convenience sample utilized. Use of a paper AINV tool contributed to less nausea data collected in this study. An AINV tool that could be better included into clinical care; utilized by many members of the health care team; integrated into existing technology to facilitate information collection and assessment; and improved sharing of patient self-reported outcomes will allow for better data in future studies.
Summary
Despite a perceived ease of use and acceptable time commitment for completion of the AINV tool, uptake was low with limited value in improving AINV outcomes. Future studies should focus on ifosfamide-containing regimens, management of MEC, identifying and managing the emetogenic risk of IT chemotherapy, as well as instances when overall emetogenicity changes mid-chemotherapy cycle. Exploration of innovative methods to track and assess AINV will allow for better real-time personalization of antiemetic regimens. As only 61% of patients reported time spent with pharmacists was sufficient, pharmacist assessment of AINV should include ongoing real-time assessment of symptoms, either in-person, on the phone, or via secure online questionnaires to ensure ongoing AINV control.
Supplemental Material
OPP892666 Supplemental Material - Supplemental material for Integration of a nausea and vomiting assessment tool into antineoplastic management of pediatric oncology patients
Supplemental material, OPP892666 Supplemental Material for Integration of a nausea and vomiting assessment tool into antineoplastic management of pediatric oncology patients by Krista McKinnon and Jennifer Jupp in Journal of Oncology Pharmacy Practice
Footnotes
Acknowledgements
The involvement of patients and their caregivers is acknowledged with thanks. The authors are grateful to Dr. Fiona Schulte for her assistance in developing the patient and caregiver satisfaction surveys. They are also grateful to Chen Shen and Alysha Wong for their assistance with data collection and analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.