
Abstract
Breast cancer patients use numerous medications, which include cytotoxic chemotherapy drugs, hormonal agents and supportive medication, so they are more vulnerable to potential adverse drug interactions. This study aimed to evaluate frequency, severity, clinical importance and risk factors responsible for the Drug-drug interactions (DDIs) in a cohort of patients suffering from breast cancer. Data was obtained from 150 patients in the oncology ward (both inpatient and outpatient) with a confirmed diagnosis of breast cancer and currently receiving standard breast cancer-directed treatment. The data was recorded into a pre-designed form specifically made for this study through individual patient interviews and by reviewing the detailed medical chart records of the patients. DDIs were identified by using drug interaction software such as Medscape mobile application and Micromedex version 2.
The results of this study showed that all patients were female. The mean numbers of drugs that patients used were 7. Potential drug interactions were identified in 92% of the patients. When drug groups were overviewed, 32% of interactions were between anti neoplastic drugs, 62.9% interactions were between the anti neoplastic agent and supportive care drugs and 5% of them were between anti-cancer drugs and drugs used to treat comorbidities. Major DDIs were found in 62.2% of patients, 25.3% of DDIs were moderate and 12.4% were minor. The number of drugs, comorbid diseases, and selection of chemo protocols were the risk factors for drug interactions. Most of the DDIs found in breast cancer therapy may have adverse consequences on patient health and therapeutic outcomes. Therefore, health care professionals should review the medication regimen of patients with breast cancer before starting any chemotherapy treatment.
Introduction
Breast cancer is among one of the most commonly observed cancer in women. 1 According to an estimation of World Health organisation (WHO) in 2011 about 508,000 women died worldwide due to breast cancer. 2 In Pakistan, the most common cancer among women is breast cancer. 3
As patients with cancer use numerous medications, such as cancer pharmacotherapy which include cytotoxic chemotherapeutic drugs, hormonal agents and supportive medication, so they are more vulnerable to potential adverse drug-drug interactions (DDIs). 4 In clinical studies, DDIs can be classified as pharmaceutical DDIs, pharmacokinetic (PK) DDIs, and pharmacodynamics DDIs. 5
In patients’ with cancer, drug interactions have particular significance and impact on patient safety because most of the anticancer drugs are cytotoxic and have a narrow therapeutic index, so drug interactions among cancer pharmacotherapy and other adjuvant medications may result in changes in the pharmacodynamics or pharmacokinetic properties of an anticancer agent. Any such DDIs may reduce efficacy or increase the toxicity of anti-cancer medicines.5,6 Hormonal agents like tamoxifen used for long-term treatment of breast cancer are highly metabolized by CYP3A4 into active metabolites; 4-hydroxytamox and CYP2D6 convert it to endoxifen, both of which contribute to the efficacy of tamoxifen. CYP2D6 inhibitors like selective serotonin reuptake inhibitors (SSRI’s) have the potential to lessen tamoxifen’s effectiveness by decreasing production of active metabolites like endoxifen. 5
There are many known risk factors which can lead to the occurrence of drug interactions, such as the number of medications prescribed, older age and individual patient variations, such as age, gender, genetic variations (e.g. fast acetylators vs. slow acetylators), and the existence of different comorbid conditions.5,6 Cancer patients belonging to the age group of 60 and above, have a higher risk of co-morbid diseases such as cardiovascular (CVS) diseases, hypertension, and diabetes, and may require different medications for their treatment. Due to these co-morbid conditions they use multiple medications along with cancer pharmaco-therapeutics, which increases the risk of DDIs in these patients. 7
DDIs in cancer patients is commonly observed and the majority of these interactions have the potential to cause considerable adverse drug reactions (ADRs) and the incidence of ADRs from DDIs is found to be 20–30%. DDIs can become a significant reason for mortality and morbidity in patients with cancer. A study conducted in the oncology ward of Norway stated that 4% of mortality among cancer patients was due to drug interactions. 8
Even though it is common knowledge that drug interactions may harm patients, their frequency in oncology is still high. 9 Furthermore, it was observed that prescribing oncologists may lack in knowledge about the drugs that the patients concomitantly use to treat other co-morbidities. 10 Similarly, at the community level hospitals in developing countries, because of the lack of a centralized patient medical record system, general practitioners and pharmacists may not be aware of patient’s full medications history. Primary health care physicians and pharmacists might not be well-informed by patients or their oncologist about the treatment with anticancer drugs, so they might be not aware of Potential drug interaction of an anticancer agent with other drugs, they may prescribe or dispense for a new complaint. 11 Also, for the pharmacological management of cancer patients, the avoidance of errors is often hindered by a lack of effective communication between prescribing oncologists and cancer patients. 12
Thus, this study aims to gain more insight into the prevalence of DDIs among patients with breast cancer in two cancer hospitals, out of a total six hospitals in the province; INOR (Institute of Nuclear Medicine Oncology and Radiotherapy) Hospital and Ayub Teaching Hospital (ATH) Abbottabad, Pakistan. This study will evaluate severity, clinical significance and risk factors of potential drug interaction in treatment of patients with breast cancer using chemotherapy as well as assess DDIs of chemotherapeutic agents with other routine medicines commonly used to manage other co-morbid conditions.
Methods
A cross-sectional study was conducted on the breast cancer patients visiting or admitted in both, the INOR cancer hospital and oncology ward of ATH for five months from August 2016 to January 2017.This study had ethical approval from the Ethics Committee of ATH Hospital. Patients’ consent was obtained before participation in this study.
In this duration, a total of 150 patients who were either admitted in oncology wards or were visiting the outpatient department (OPD) with a confirmed diagnosis of breast cancer and receiving standard breast cancer-directed treatment, were considered to be eligible for this study. The patient suffering from other types of cancers were excluded from the study.
In this study, we assessed the medical chart records of breast cancer patients receiving systemic anti-cancer therapy. Patient medication charts had demographic and medical information of patients. All prescribed drugs in the patient's medical chart records were noted in the forms specially designed for this study to collect information for analysis of possible drug interactions. Patient individual interviews were also carried out by the researcher RB, in an attempt to get complete information of drugs patients were using for the treatment of other existing co-morbid conditions and any over the counter (OTC) drugs to relieve minor ailments. Drugs used during systemic anti-cancer therapy were classified into 3 groups such as supportive care drugs or pre-medication of chemotherapy, the anticancer agent, and the drugs used for the treatment of the comorbid conditions. Two software such as Medscape Smartphone application and Micromedex (drug interaction) software version 2 were used for screening of potential DDIs. After identification, potential drug interactions were classified by the level of severity to three levels such as:
Major = Drug interactions that have potential to produce serious adverse clinical consequences and can cause permanent damage and such combinations should be avoided.
Moderate = Drug interactions which have potential to produce harm and may require a treatment and there is a need of close monitoring.
Minor = Drug combinations that do not have a significant potential to produce harm and drugs combination can be used together.
Descriptive statistics such as frequencies and percentages were used to represent gender, age group, co-morbidities, cancer disease progression, stage, metastasis, and chemo protocols. A Chi-square test was used to evaluate risk factors for drug interactions.
Result
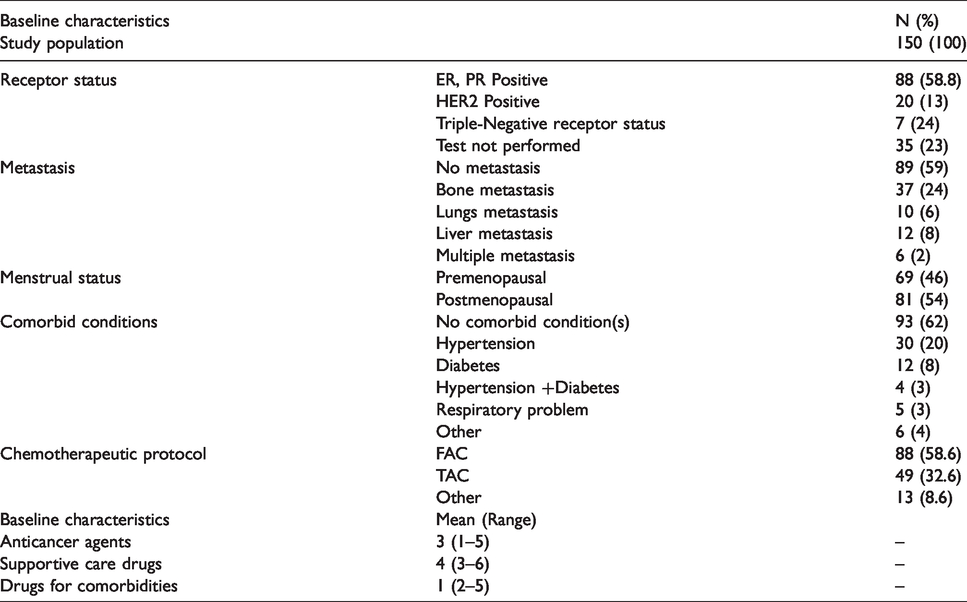
Results of the study showed that a total of 150 patients were included in this study and all patients were female. The mean age of the patients suffering from breast cancer was 40 and the mean numbers of drugs prescribed to these patients were 7. Among patients with breast cancer, presence of receptor status of estrogen (ER) and progesterone (PR) was evaluated and it was found that among 150 patients, 88(58%) patients had ER and PR positive receptor status. Patients who had human epidermal growth factor receptor 2 (HER2) positive receptor status were 20 (13%) and 7 (4.6%) patients had Triple-Negative receptor status, whereas in 35 (23%) patients, the test for detection of receptor status was not done. Using Tumour, Nodes, Metastasis (TNM) classification system it was observed that among these patients 13.3% patients had Stage 2 breast cancers, 48% had stage 3 breast cancer and 39% had stage 4 cancer. The majority of the patient (74.7%) patients had invasive ductal carcinoma. When metastasis with breast cancer was evaluated, it was found that 59% of patients had no metastasis, 25% patient presented with bone metastasis along with breast cancer, 6% had lung metastasis, 8% had liver metastasis and 6% had multiple metastasis. Co-morbid diseases were evaluated further and it was found that 62% had no co-morbid conditions, while 38% of patients were suffering from co-morbid conditions. Among these 38% of patients with co-morbidities, 20% of patients were suffering from hypertension, 8% of them were suffering from Diabetes Mellitus, 3% had respiratory disorders, 3% had both (Hypertension and Diabetes) and 4% had other co-morbid conditions. Among 150 patients, 88 patients were prescribed FAC (5-Fluorouracil Doxorubicin and Cyclophosphamide) chemo protocol, while 49 patients were prescribed the TAC (Taxane, Doxorubicin, and Cyclophosphamide) chemo protocol. Out of 150 patients, 13 patients were prescribed a combination of other chemo protocols as shown in Table 1.
Baseline characteristics of patients in the study.
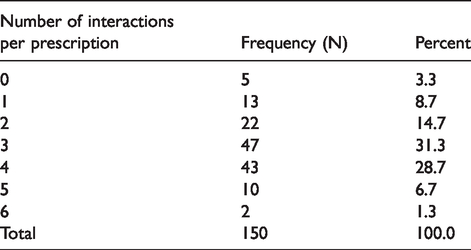
Frequencies of potential drug interactions per patient prescription.
Drug interactions
Potential drug interactions were identified in 96% of patient’sprescriptions.The majority of the patients had at least 3 interactions in their prescription with a percentage of 31.3% (n = 47). The total number of interactions in all patients’ prescriptionsin this study were 437 as shown in Table 2.
Types of interactions based on the severity
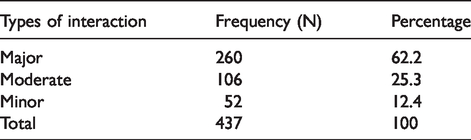
The total number of interactions in all patients’prescriptions were 418. Among these 12.4% were minor interactions, 25.3% were moderate interactions and 62.2% were major interactions as shown in Table 3.
Types of interactions based on the severity.
Interacting drugs
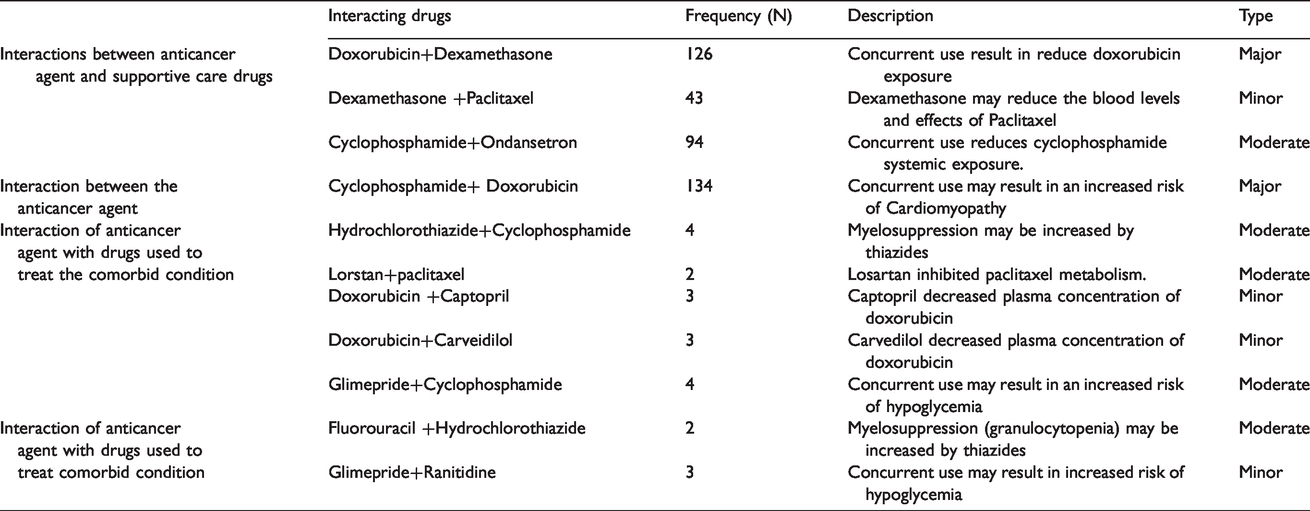
The numbers of interactions between antineoplastic agents were 134 (32%). The number of interactions between the antineoplastic agent and supportive care drugs were 263 (62.9%) and interactions between anticancer agents and drugs used to treat the comorbid conditions were 21 (5%). An overview of interactions between drugs is given in Table 4.
Frequency of interaction and detail of interacting drugs.
Risk factors for drug interaction.
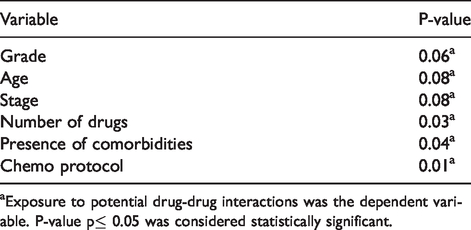
aExposure to potential drug-drug interactions was the dependent variable. P-value p≤ 0.05 was considered statistically significant.
Risk factors
The presence of comorbid diseases, the number of drugs used, and the selection of chemo protocol used for the treatment of breast cancer were found to have a relationship with the number of interactions. Drug interactions were more common while using TAC (Taxane, Doxorubicin, and Cyclophosphamide) chemo protocol as compared with other chemo protocol used for the treatment of breast cancer. The number of interactions per prescription did not correlate with age, stage, type and receptor status and the P-value was not significant as shown in Table 5.
Discussion
Breast cancer patients are prescribed different drugs such as cancer pharmacotherapy, drugs used for their prolonged survival and for the treatment of their comorbid diseases so potential drug interactions are commonly observed in these patients. 13 The prevalence of DDIs in general medicine has been evaluated in several studies. 14 but studies evaluating the prevalence of drug interactions with anticancer agents are limited especially in breast cancer. This study highlights the incidence of drug interaction and determines relationship of significant risk factors responsible for drug interactions in breast cancer treatment. This study results can be utilized to decrease the frequency of DDIs in breast cancer patients as there is limited research regarding drug interaction in breast cancer patient receiving systemic anti-cancer therapy.
The results of this study showed that in breast cancer patients the prevalence of DDIs was high and majority of the patients had at least one DDIs. More than half of the study participants had major DDIs and those patients were at high risk of developing serious clinical consequences. Our findings were similar to a study conducted in Turkey, which showed that the prevalence of drug interaction in breast cancer patients was 86%. 1 The study results are similar to two other studies, performed on ambulatory cancer patients, showing 27–58% of all patients in those studies had at least one DDI.11,15
The high frequency and occurrence of major DDIs can produce serious adverse reactions, such as increase risk of cardiotoxicity, gastrointestinal (GI) toxicity, increasing or decreasing the desired level of drug concentrations in blood and enhancing the toxicity of anticancer agents or decreasing the clinical effectiveness of the drugs. 10 The most frequent drug interaction found in our study was an interaction between cyclophosphamide and doxorubicin in 134 individual patient prescriptions. The interaction between cyclophosphamide and doxorubicin is a major interaction and it increases the risk of cardiomyopathy, so care should be taken while designing a therapeutic regimen of the patient with heart disease or patients who are at risk of developing heart diseases. 16 From our study results, it is also recommended that close clinical monitoring of patients for signs and symptoms of cardiac dysfunction should be carried out in all patients taking this drug combination. For patients who have an existing cardiac dysfunction, it would be better to avoid this protocol or use doxorubicin analogs like epirubicin as epirubicin does not have interaction with cyclophosphamide and additionally epirubicin have less cardiotoxicity as compared to doxorubicin. 17 Our study also showed that interaction between paclitaxel and dexamethasone is frequent in the treatment of patients with breast cancer and according to literature, this interaction decreases therapeutic efficacy of paclitaxel. 16 Another significant interaction was observed by the concurrent use of hydrochlorothiazide with 5-fluorouracil and cyclophosphamide. This pharmacodynamics interaction can cause prolonged and severe neutropenia. As myelosuppression is also common with cancer treatment so to avoid febrile neutropenia this combination should be avoided. 18
This study also showed that the number of drugs used by the patients could be a risk factor for DDIs. This finding that drug interactions may increase by increasing the number of medications in cancer patients is consistent with the results of a previous study. 19 Our study also provides evidence, that presence of co-morbid conditions is associated with an increased number of interactions, so co-morbidities are also a risk factor for the occurrence of DDIs in breast cancer patients which is similar to findings from another study. 1 Our study highlights that drug interactions were more common with taxane, doxorubicin and cyclophosphamide (TAC) chemo protocol as compared to FAC chemo protocol and highlights the fact that the selection of chemo protocol may also be a risk factor for possible drug interactions.
In the process of designing the therapeutic regime for the patients, DDIs should be given important consideration, because of the possible risk of DDIs to produce adverse consequences on the desired therapeutic outcomes and may affect patient quality of life. Drug interactions also have the potential to increase treatment costs 12 which should be given special emphasis in countries and health care systems with lesser resources.
The medication review process in daily practice is not common in developing countries due to a lack of clinical pharmacists in oncology ward, although it is a common fact that many combinations of drugs in different treatment chemo protocols for breast cancer may produce interactions and are unavoidable. Interacting drugs may be administered together if proper precautions and appropriate monitoring such as dose adjustment, plasma concentration monitoring, and outcome monitoring could be done. Clinical judgments of risk vs benefit ratio of the possible adverse impacts of drug interactions and beneficial effect of combination medicines on patient treatment and quality of life could be helpful in the management of DDIs in treatment of breast cancer patients. However, all these process needs a proper medication review process of all drugs used in treatment of patients withbreast cancer performed by a specialized oncology health care team.
Therefore, in an ideal condition in developing countries, all drugs prescribed to breast cancer patients should be electronically documented, including a patient's full medication record, to recognize and prevent drug interactions that have the potential to produce the unintended harmful effects.
The study was carried out in two different hospitals therefore the representativeness and generalisability of the data strengthens. We also used an advanced screening method for the detection of DDIs, which led to more valuable data on the occurrence of DDIs. A major limitation due to the lack of a centralised electronic system was that there was a risk of missing patient medications not recorded in the patient record form however, the data collection method was designed as individual patient interviews, which was able to overcome that limitation and provide detailed medication history. Another possible limitation of the study could be lack of inclusion of novel treatment protocols and novel targeted therapies, as they were not being used in hospital settings where study was conducted due to financial constraints.
Conclusions
Breast cancer patients use different drugs and therefore, potential drug interactions are commonly observed in these patients. DDIs can produce adverse consequences on the desired therapeutic outcomes and patient quality of life. Therefore, the medication regimen should be investigated according to patient needs before starting any treatment. The number of drugs that are being used, the existence of comorbidities and the selection of chemo protocols are the major risk factors for drug interactions. Cardiac monitoring of patients with risk of heart diseases should be done as most of the interactions found in conventional systemic breast cancer therapy may potentiate cardiotoxicity in patients.
Novelty and impact
Our study shows the risk factors responsible for drug interaction in breast cancer patients using chemotherapeutic standard protocols, which were consistent with other studies. Our study identified a new risk factor of drug–drug interaction (DDI) in breast cancer i.e. the selection of chemo protocol for treatment. The DDI interactions were found to be more common while using TAC chemoprotocol. Our study results suggest that cardiac monitoring of patients, with risk of heart diseases, should be performed with regular intervals as DDI in breast cancer therapy may increase the risk of cardio toxicity.
Footnotes
Authors’ Note
Ayesha Iqbal is also affiliated with Division of Pharmacy Practice and Policy, School of Pharmacy, University of Nottingham, University Park Campus, Nottingham, RD, UK. Muhammad M Iqbal is also affiliated with Department of Internal Medicine, Leicester Royal Infirmary, University Hospitals Leicester, Leicester, UK.
Acknowledgments
We are grateful to the hospital administration of INOR, and Ayub Teaching Hospital Abbottabad and all the staff. We acknowledge Dr. Javed, Head of Department INOR hospital for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.