
Abstract
Objective
Carboplatin is a cytotoxic chemotherapy drug developed in the 1980s which is still widely used today across various tumour types. Despite its common application, there remains a significant controversy and practice variation on its unique method of dosing by area under the curve (AUC). One potential reason for this variability stems from the reliance of using an estimated glomerular filtration rate (eGFR) as an extrapolation of the measured GFR (mGFR) which the commonly used Calvert equation was originally validated for. This review takes a novel and collaborative nephro-oncology approach to highlight the historical evolution of carboplatin dosing, methods for estimating GFR and its relative performance in the application of carboplatin dosing for adult patients.
Data sources
We reviewed all pertinent publications comparing carboplatin AUC-based dosing in adult patients based on the various methods of GFR measurements or estimations in order to provide a comprehensive description of each method’s advantages and risks.
Data summary and conclusions
The Cockcroft-Gault equation has been widely studied but newer eGFR equations, such as the CKD-Epidemiology Collaboration (CKD-EPI) or Janowitz-Williams equation have outperformed the Cockcroft-Gault in recent studies.
Background
Carboplatin was first developed in 1981 as a less toxic platinum alternative to cisplatin. Early studies with carboplatin demonstrated less nephrotoxicity and ototoxicity with a lower emetogenic potential versus cisplatin.1,2 Its dose limiting toxicity is myelosuppression, with thrombocytopenia being more severe than leukopenia.1,2 Carboplatin is often used in gynecological cancers, but has wide range of activity in other malignancies including lung, breast, genitourinary, germ cell tumours, head and neck and cancers with an unknown primary. 3
Carboplatin was initially dosed by body surface area (BSA) (milligram per m2) with a maximum tolerated dose (MTD) of 400 mg/m2. 1 Carboplatin demonstrates linear pharmacokinetics with a positive correlation between glomerular filtration rate (GFR) and platinum clearance.1,2 The dose of carboplatin and the area under the curve (AUC) is also positively correlated. 1 It has been previously shown that reduced GFR results in unexpectedly high AUC. 1 AUC has been correlated with clinical toxicity, namely thrombocytopenia. 2 Retrospective analyses of BSA-based carboplatin doses resulted in highly variable AUC levels, due to variations in renal function.4,5 Thus, the accurate determination of GFR when dosing carboplatin is essential.
This pharmacokinetic-pharmacodynamic relationship has been previously studied in hopes to improve the dosing accuracy of carboplatin. Several dosing equations have been developed 6 but the most common method has been using the Calvert formula. 7 The uptake of the Calvert formula in practice ranges from 98 to 100% according to surveys conducted in the United States and Spain.8,9 Despite this high degree of consensus among practitioners to use the Calvert equation, the operationalization of this equation remains a highly debated topic.
Much of the controversy is rooted in the reliance of measured GFR (mGFR) within the Calvert equation. In the original Calvert study, mGFR was determined using the 51Cr-EDTA method. 7 The impracticality of this method has led researchers to explore the use of estimated GFR (eGFR) equations. However, these equations often depend on weight and/or creatinine values and lead to significant practice variations. One practice survey conducted in the United States presented a patient case example for which only one of 47 respondents answered with the “correct” dose. 10 The variation in carboplatin doses ranged from 110 to 1,811 mg with the “correct” dose of 721 mg. 10
In the following article, the data presented is exclusively in the adult population and may not apply to pediatric populations. Given the almost exclusive use of AUC dosing based on the aforementioned data, alternative methods of dosing carboplatin (e.g. weight-based) is beyond the scope of this paper.
Carboplatin dosing: Best practice recommendations
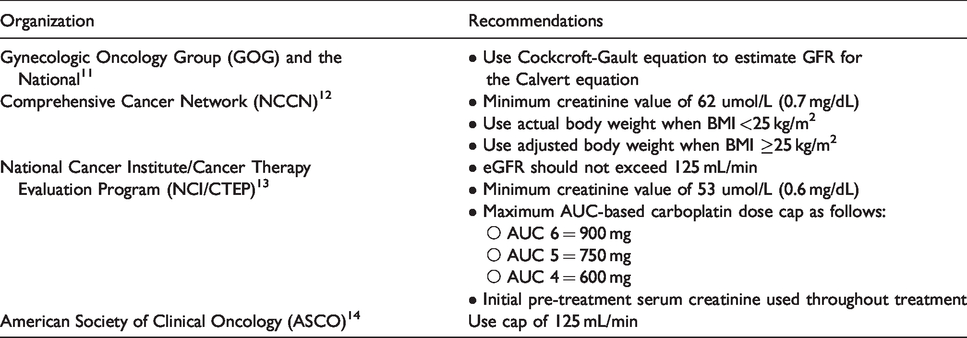
No head-to-head clinical trials currently compare different carboplatin dosing strategies. However, certain groups have made recommendations on the approach to dosing carboplatin. They are summarized below (Table 1).
Official carboplatin dosing recommendations by organization.
Glomerular filtration rate: Measurements and estimations
GFR, in addition to being traditionally considered the best marker of renal health and function, is critical in its relation to dosing of certain medications like carboplatin. Indeed, therapeutic compounds or their metabolites that are small, heavily water-soluble and polarized are often excreted in urine. 15 Precise measurements of GFR in clinical practice are time consuming, cumbersome and relatively complex. Inulin clearance is usually regarded as the Gold Standard measurement for GFR. 16 However, this method is not applicable in clinical practice as it requires a continuous infusion of inulin intravenously given over a prolonged (i.e. many hours) period of time and concurrent, continuous collection of urine. Other methods of GFR measurement have very close agreement to inulin clearance 17 ; but while technically less complex than inulin clearance, remain impractical. 125-iothalamte or 51Cr-EDTA clearance measurements require a single bolus injection of an exogenous radioactive compound with serial measurements of plasma levels or concurrent and continuous collection of urine. Iohexol single-bolus plasma clearance also requires a single bolus injection of an exogenous compound that is not radioactive, but for which some reports of allergic reactions exist. 18 It also requires multiple plasma measurement levels with complex measurement instruments. Finally, 99mTc-DTPA clearance does not require plasma or urine measurements, but does involve injection of an exogenous radioactive compound and takes many hours to perform. Thus, precise methods of GFR measurement are not routinely used in clinical practice in light of their complexity and cost.
Hence, estimates of GFR are relied upon in clinical practice for both assessment of renal function and dosing of medications. This is done by utilizing plasma measurement of an endogenous marker of kidney function, creatinine, in various methods. Creatinine is formed as a result of the nonenzymatic dehydration of muscle creatine. Creatinine production is fairly constant under normal circumstances and solely cleared by renal excretion. 19 It is readily and reliably measured in clinical laboratories and is by far the most commonly used marker of renal function. 20 There exists many methods to estimate GFR from creatinine measurements, we outline in this manuscript the most common methods used.
GFR estimate equations: Advantages and pitfalls
Creatinine clearance
Creatinine clearance (CrCl) measurements can approximate GFR very closely in right circumstances. 21 It requires both the collection of urine for a defined time period (usually 24 hours) and one serum plasma creatinine concentration measurement, usually collected at the end of the 24 hour period. When performed correctly, this provides a very close estimate of GFR and can be used to dose carboplatin. The major limitation of CrCl in routine practice is the requirement for timed urine collections which are relatively long and often frowned upon by patients. Moreover, timed urine collections are subject to over or under collection (which will lead to under or over estimation of GFR). The correlation between measured GFR and CrCl has been shown to be poor, 22 and caution should be used if relying on creatinine clearance via urine collection for dosing of carboplatin.
eGFR
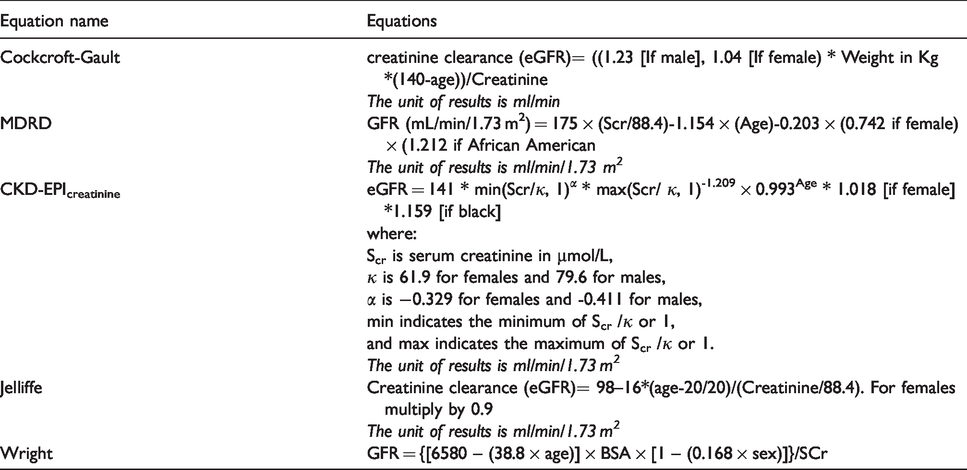
Using one of several formulas, an estimation of GFR can be obtained from a single measurement of serum creatinine (Table 2). This is usually fairly reliable, however there are situations in which serum creatinine is not an accurate representation of the patient's renal function. In very elderly patients or those with very low muscle mass using serum creatinine for estimation of GFR can result in significant overestimation of true GFR. 23 Despite this, formulas using a single creatinine reading to estimate GFR are usually fairly reliable, making them the usual method to establish GFR. 24
Common formulas for estimation of GFR.
Cockcroft-Gault (CG)
The CG equation, developed in 1976, remains a widely used method of estimating GFR for dosing of carboplatin in the clinical setting. 9 The CG formula estimates creatinine clearance (CrCl) in mL/min from age, sex, body weight, and serum creatinine. 25 Use of the CG formula for carboplatin dosing can be problematic given its limitations. Indeed, using modern standardized serum creatinine assays, it systematically overestimates true GFR. In addition, the age coefficient is too large, thus, it underestimates true CrCl in elderly persons. 26 It includes weight, so it systematically overestimates true CrCl in people who are obese or edematous. 26 Moreover, determining the accurate adjustments to body weight can in of itself be challenging as it is not clear how body weight should be adjusted to be used within the formula. The original CG formula was not developed to take into account the concept of adjusted ideal body weight, yet in light of the rapidly increasing obesity rates, 27 this becomes necessary. The precision of the formula appears to be somewhat preserved when using adjusted ideal body weight but does not exceed 80%. 28 Finally, the cutoff at which one should use adjusted ideal body weight is not known.
Modification of diet in renal disease (MDRD)
In the late 1990s, a new equation to estimate GFR was derived from the MDRD Study cohort. 29 While the original equation contained 6 variables, it was later abbreviated to a simple 4 variable equation containing age, gender, serum creatinine and race (limited to African or non-African descent). 29 Owing to its simplicity and precision, it was rapidly adopted in clinical practice and in clinical practice guidelines. 30 One of its most important limitation is a very imprecise estimation of GFR at values above 60 mL/min/1.73 m2 and its tendency to underestimate GFR in that same range. 31 Therefore, its utility is confined to patients with CKD.
CKD-Epidemiology Collaboration (CKD-EPI)
The CKD-EPI equation, first reported in 2007, addresses the shortcomings of the MDRD formula. 32 The reported accuracy of the CKD-EPI equation in patients with GFR >60 mL/min/1.73 m2 is 89% for an estimate within +/−30% of the measured GFR result. Because the reported GFR with the CKD-EPI formula is adjusted to 1.73 m2 of body surface area (BSA), for drug dosing, the result must be readjusted to the patient's BSA. With this method, the CKD-EPI formula is very precise and outperforms the CG GFR and MDRD eGFR formula in almost all settings,33,34 even in the elderly population. 35 When this is done, the BSA adjusted CKD-EPI eGFR is very reliable to dose carboplatin. 36 Since most laboratories now report CKD-EPI eGFR when serum creatinine is ordered, and BSA is very simple to calculate, this proves to be a reliable and simple method to approximate GFR for drug dosing.
Jelliffe
The Jellife GFR formula, originally described in 2002, was developed with the aim to estimate creatinine clearance easily in acutely ill patients with unstable renal function, who have rapidly changing serum creatinine values and who need careful individualization of drug dosage. 37 Owing to its relative complexity and fairly narrow application, it is not commonly used.
Wright
Wright et al. developed four formulae for estimating renal function specifically in cancer patients. One of the formula derived provides accurate and assay-specific predictions for accurate dosing of carboplatin. 38 However, the formula was derived form a small cohort of patients and its performance patients across the full range of renal function, and particularly those with poor renal function, is not well documented. 39
Janowitz-Williams
Janowitz et al recently published a new model for GFR calculation using a cohort of more than 2000 patients. 36 This model appears to be particularly precise at estimating GFR for carboplatin dosing when compared to 51Cr-EDTA GFR. However, it has not been extensively studied, and it requires an online tool to calculate GFR, something which may limit widespread adoption.
Performance of various GFR estimate equations in the Calvert equation
Cockcroft-Gault (CG)
The CG equation consistently shows the lowest comparative accuracy and precision in estimating GFR;36,38,40–42 low concordance of carboplatin dosing 43 or AUC. 5 The CG underestimated the carboplatin dose in four studies36,40,42,43 and overestimated the dose in two studies.41,44
The precision and bias of the equation is commonly expressed using the absolute percentage error (APE) and percentage error (PE), respectively. The APE of CG was 23% and the bias (a measurement of accuracy) was −7% in one small study. 42 Other studies used a proportion of patients above a threshold APE. Two larger studies demonstrated that 25% to 35% of patients would have a dose APE > 20%.36,43 If a more conservative threshold of dose variance of 5% is selected, the percentage of patients may increase to 85% when using any formulae compared with mGFR. 42 All studies had an acceptable patient demographic population with included patients of all ages, weights and mGFR values, which may partially explain the high amount of discordance when considering the above stated limitations of the formula. The evolution and changing standards of creatinine assays may also account for differences in results. 41 Interestingly, underestimation of dose was most common in those with BMI <25, compared to BMI ≥30. 43
In van Warmerdam et al., the mean BSA was 1.9 and all patients had a creatinine clearance ≥60 mL/min. 44 Increased weight and creatinine clearances may have led to overestimations in carboplatin dosing due to the inaccuracy of the CG in these populations. Using various weight corrections (e.g. ideal body weight, IBW) have been studied to attempt to improve the accuracy of the CG equation with some success but issues remain of when and which weight correction to use. These concepts are briefly exemplified in Dooley et al. where the rate of underdosing is more prevalent among BMI <25 compared to BMI ≥30 and the rate of overdosing has the opposite result. 43 When using IBW as a correction, the rate of overdose is decreased in the BMI ≥30 group compared to no weight adjustment, but it introduces a very significant underdose problem in this group, where it did not previously exist without the weight adjustment. 43
In another study, a modified CG was concluded to provide better carboplatin dosing accuracy compared to the CKD-EPI and MDRD. 45 This study is limited by the use of weight indexing, where eGFR is reported on a standardized BSA per 1.73 m2. While this is useful for the purposes of CKD staging, it is not recommended for the purposes of drug dosing.
MDRD
The MDRD underestimated GFR and/or carboplatin dose in three studies36,42,43 and was overestimated 40 in one study. Relative to the other eGFR equations, it has a high discordant rate to carboplatin dosing and similar precision and bias of the Cockcroft-Gault.36,42 The outlier GFR overestimation finding may be a result of the study a 24-hour creatinine clearance, whereas previous studies have used some form of exogenous marker to measure GFR. No clear differences between subgroups (e.g. age, sex, BMI) were shown. 43 However, in comparison to the other equations, the MDRD produced the largest bias and lowest precision amount multiple subgroups of GFR, age and BMI. 46
CKD-EPI
The CKD-EPI underestimated GFR and/or carboplatin dose in one study 43 and it overestimated in two studies.36,40 It has demonstrated consistently high concordance to mGFR.36,40,43 The proportion of patients experiencing a >20% underdose is 20.7% in one study. 43
In the study with the largest data set, the CKD-EPI was found to be the most accurate in eGFR determination with a root-mean-square-error (RMSE) of 16.3 mL/min compared to 23.75 mL/min for CG and MDRD. 36 Consequently, this led to a much lower proportion of patients having an absolute percentage error > 20% at approximately 20% when compared to 25 to 40% with CG and 30 to over 40% with MDRD. 36 No subgroup analysis has been conducted to date.
Jelliffe
The Jelliffe was historically recommended by the GOG, but has since fallen out of favour since the NCI/CTEP released a statement warning practitioners of potential carboplatin overdosing due to IDMS standardization. 11 In three studies, the Jelliffe underestimated the GFR and/or carboplatin dose.40,42,47 The mean percentage underestimation was estimated at 14 to 20% in two small studies.40,47 In another study, the Jelliffe both under- and over-estimated the dose, but overestimated the dose more frequently. 40 There remains very limited data in different subgroup populations where the Jelliffe equation may be beneficial. For example, a common clinical challenge is selecting the correct equation and/or weight adjustment for obesity. In one study, patients greater than 30% of their IBW, the Jelliffe underestimated the GFR by greater than 10%, regardless of the weight correction applied. Over the entire study population, it was the most biased. 46
Wright
The Wright formula was specifically derived in a cohort of cancer patients. 38 In three studies the Wright formula underestimated the GFR and/or carboplatin dose.38,42,43 In two studies the GFR and/or carboplatin dose was overestimated.36,42 The mean APE was 12 to 13% and the PE was −3 to −5%. 38 These results were similar in a small study limited to patients with gynecological malignancies with an APE of 19% and PE of −2%. 42 However in a subsequent larger study, the proportion of patients with dose APE > 20% was higher than the CKD-EPI and Janowitz-Williams. 36 Of note, the Wright formula was found to have to the highest concordance for carboplatin dosing when compared to the MDRD, CKD-EPI and CG equation. 43 In patients greater than 30% of their IBW, the Wright equation using ABW was the most accurate. However, the Wright equation performed poorly overall, when compared to the Cockcroft-Gault or MDRD. 46
Janowitz-Williams (JW)
Janowitz et al recently published a new model for GFR calculation using a cohort of more than 2000 patients. 36 This model appears to be particularly precise at estimating GFR for carboplatin dosing when compared to 51Cr-EDTA GFR. Precision and bias were exceptional at 11.2% (median APE) and 1.39%, respectively. 36 This model had the lowest proportion of dose APE >20% at 14.17%, compared to 18.62% for CKD-EPI and 25.51% for the CG. 36 Despite its relatively large sample size for development, the model only included all white participants from a single center with a majority mGFR of >60 mL/min. No subgroup analyses were conducted. This limits the generalizability of the model. No clinical studies have been published to date evaluating the model and it requires an online tool to calculate GFR, something which may limit widespread adoption.
Summary of the evidence and its implication to practice
The studies presented above are mostly uncontrolled and retrospective in design. This may lead to a number of selection, reporting and other biases. Therefore, caution must always be exercised when applying these results in clinical practice. However, despite the limitation in study design, many of the studies do generally agree in the direction and to a lesser extent, the degree of bias. There have not been any robust investigations into subgroups that would inform and support the use of one equation over another. Without any clinical outcome data to support one of the equations over another, we must rely on the current data that suggests the CKD-EPI or Janowitz-Williams has the greatest concordance to mGFR with the lowest PE and APE. The CKD-EPI has an advantage in its familiarity to clinicians and standard reporting in certain institutions. Clinicians should take note that any equation that relies on eGFR for AUC-based dosing will inherent the limitations of the estimation notwithstanding the potential limitations of the equation itself.
Conclusions
While the CG GFR remains frequently utilized, it shows significant limitations in its applicability for accurate estimation of renal function and thus carboplatin dosing. We recommend it no longer be the preferred method utilized in the Calvert equation. Alternatively, we suggest that the body surface area adjusted CKD-EPI method or JW equation.
The adjusted CKD-EPI is advantageous in its simplicity and precision since clinical laboratories frequently report the CKD-EPI eGFR with all creatinine measurements, and BSA adjustment is extremely simple and easily calculated. The body surface adjusted CKD-EPI eGFR formula matches or outperforms the CG GFR in almost all clinical circumstances encountered, with the rare exception of patients marked obesity, abnormal body composition such as amputees, paraplegia, in patients with severe liver disease and for pregnant women. In these situations, none of the formulas accurately estimate renal function and a GFR measurement (e.g. 99mTc-DTPA clearance) should be used. Importantly, CKD-EPI performs well in elderly patients and those with significant deviation from an ideal body weight (with the exception of extreme obesity), something the CG GFR formula does not.
While a bit more cumbersome, the JW equation can also be easily used with a simple web browser. Its robust sample size for model development as well as internal and external validation sets is promising. The reported bias and precision are similar to the BSA-adjusted CKD-EPI and its estimates with the other equations are in line with previous reported studies, which is encouraging.
Both methods offer precise methods of GFR assessment and carboplatin dosing to ensure safe and effective patient care. Given the widespread use of carboplatin across diverse tumour sites and its strong positive correlation between renal function and drug exposure; and thus toxicity, it is imperative that estimations in GFR be as accurate as possible. We suggest that given the current evidence, moving beyond the CG formula is warranted. Future prospective clinical trials comparing different methods of eGFR measurements for carboplatin AUC dosing are needed to validate this recommendation. Importantly, trials exploring non AUC carboplatin dosing methods are also needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.