
Abstract
Purpose
Medication non-adherence to treatment regimens can severely impact the mortality of patients afflicted with breast cancer.The purpose of this study was to identify factors that contribute to non-adherence to endocrine therapy in breast cancer treatment plans.
Methods
Thirty-two women with a breast cancer diagnosis were surveyed by pharmacists and pharmacy students to identify the patient- related factors (e.g. patient personal beliefs, education level), drug-related factors (e.g. patient drug allergies), socio-economic factors (e.g. patient ability to pay for the medication) and healthcare system factors (e.g. poor patient-healthcare provider relationship) that may impact non-adherence to endocrine therapy in breast cancer treatment plans. Medication adherence rates were measured using the Medication Adherence Rating Scale (MARS-8) system. Associations between adherence rate scores and clinical variables (e.g. age, tobacco use, alcohol consumption, cost of treatment, education level, personal beliefs, drug allergies, patient/provider relationship, adverse events) were carried out using Spearman Correlation, T-Test, Mann-Whitney U Test, and X2 tests. A p value of ≤ 0.05 was considered statistically significant.
Results
Our study found that 59% of survey respondents were non-adherent to their endocrine therapy in breast cancer treatment plans. Drug allergies (p = 0.000069), patient ability to pay (p = 0.005), poor personal beliefs about the prescribed therapy (p = 0.009), low education level (p = 0.025), adverse drug events (p = 0.026), and poor patient-provider relationship (p = 0.05) were found to play a role in patient non-adherence to treatment.
Conclusions
Our study found that drug- (e.g. allergies), socio-economic (e.g. patient ability to pay), and patient-related factors (e.g. personal beliefs) are the strongest predictors of adherence among breast cancer patients undergoing endocrine therapy. These findings support the need for a better relationship between breast cancer patients and their healthcare providers, including drug experts such as pharmacists.
Introduction
Breast cancer accounts for 15.3% of all new diagnosed cancers and 7.0% of all cancer deaths in the United States according to 2020 statistics. 1 Tamoxifen (TAM) and aromatase inhibitors (AI) are both endocrine-based treatment options commonly used in patients with estrogen receptor positive breast cancer. 2 While both endocrine-based therapies have been shown to decrease disease recurrence and breast cancer mortality rates, non-adherence continues to be an issue with patients taking either TAM or AI. 3 Tamoxifen (TAM) is a selective estrogen receptor modulator that acts as a competitive antagonist to estrogen, reducing the number of available receptors for endogenous estrogen binding. 4 Aromatase inhibitors (AI) inhibit aromatase, which is the rate limiting enzyme responsible for estrogen production in breast tissues. 4
Medication non-adherence is defined by Nieuwlaat et al. as “taking less than 80% of prescribed doses, although it has to be noted that non-adherence can also include taking too many doses, and it is associated with an increased risk for poor health, adverse clinical events, and mortality.” 5 Previous studies have shown that there was a 90% median patient adherence rate to TAM or AI treatments during the first year of therapy, but by the fifth year, the median patient adherence rate was 51%. 6 Adherence to TAM or AI treatment plans is paramount for patients with estrogen receptor positive breast cancer. Hershman et al found that the 10-year survival rate of patients who adhered to their prescribed treatment plan was 80.7%. Patients who were nonadherent to their treatment plan had a lower survival rate of 77.8%. Also, the patients who discontinued their treatment earlyhad an even lower survival rate of 73.6%. 7 This study showed that non-adherence to endocrine therapy increased the likelihood of mortality among patients with estrogen receptor positive breast cancer.
Many studies have attempted to identify factors associated with poor adherence. 2 Sawesi et al. have reviewed published literature and compiled data from 26 studies to identify reasons for poor medication adherence. 2 According to their study, those factors can be classified into five main categories (patient- related factors, therapy- related factors, healthcare system factors, socioeconomic factors, and disease-related factors). They found that the most significant predictors of medication adherence were forgetfulness (patient- related factor), the patient-provider relationship (healthcare system factor), and fear of side effects (therapy related factor). 2
Previous studies that have been conducted to identify the factors associated with non-adherence to endocrine-based breast cancer treatments were mostly designed, carried out, analyzed, and interpreted from a non-pharmacist perspective. In this study, pharmacists and pharmacy students aimed to illuminate previously unknown factors that could contribute to patient non-adherence to endocrine-based breast cancer treatments. Under- investigated therapy-related factors such as drug-drug interactions, drug-herb interactions, and drug allergies were the primary focus herein.
Methodology
Study design and patient selection
Thirty-two women with a breast cancer diagnosis were recruited to our non-randomized prospective study over a two-year period. The study was approved by the Harding University Institutional Review Board and the patients involved in the study gave written informed consent.The patients in this study were selected based on a diagnosis with estrogen-receptor positive breast cancer between 2010 and 2017. The patients selected were asked to participate in a survey in which they were asked to identify which medication they were prescribed, including: Tamoxifen, Letrozole, Anastrozole, or Exemestane.
Clinical variables
Several patient- related factors were ascertained by the survey (e.g. race or ethnic group, gender, tobacco usage, alcohol consumption, education level, diagnosis stage, co-morbidities, and personal beliefs and knowledge). Personal beliefs were assessed using three questions: “How much trust do you have in your current treatment?”, “How much belief do you have that your current treatment will be effective?”, and “How much do you understand about your current treatment?”. Patients were asked to answer with one of three answers: “a little bit”, “some of it”, or “A lot of it”. Education level was assessed using check boxes for the patient to choose one of five different educational levels they had achieved: (I: middle school or lower, II: high school, III: Some college, IV: college degree, V: professional degree). There was also a category listed as “other” for patients to write in an educational level that wasn’t represented in the five categories. The survey also collected therapy-related factors (e.g. medication allergies, prescription and over the counter (OTC) medications, herbal or dietary supplement use, side effects, and medication adherence). Lastly, the survey asked several questions related to healthcare-system factors (e.g. health insurance status, medication cost with insurance, out-of-pocket expenses, and patient-provider relationship).
Medication adherence
Medication adherence was measured as previously described by the MARS-8 methodology. 8 Patients were asked eight questions pertaining to medication adherence and for each question were given a point, totaling eight points. An 8 out of 8 on the scoring system yielded a 100% adherence score. The survey questions used to measure adherence can be found in Table 1. If a patient answered “No” to question number one, for instance, that was considered adherent and given a point. A “No” answer to question number five, however, would be non-adherent and wouldn’t be scored a point toward the total score.
Medication adherence questions.
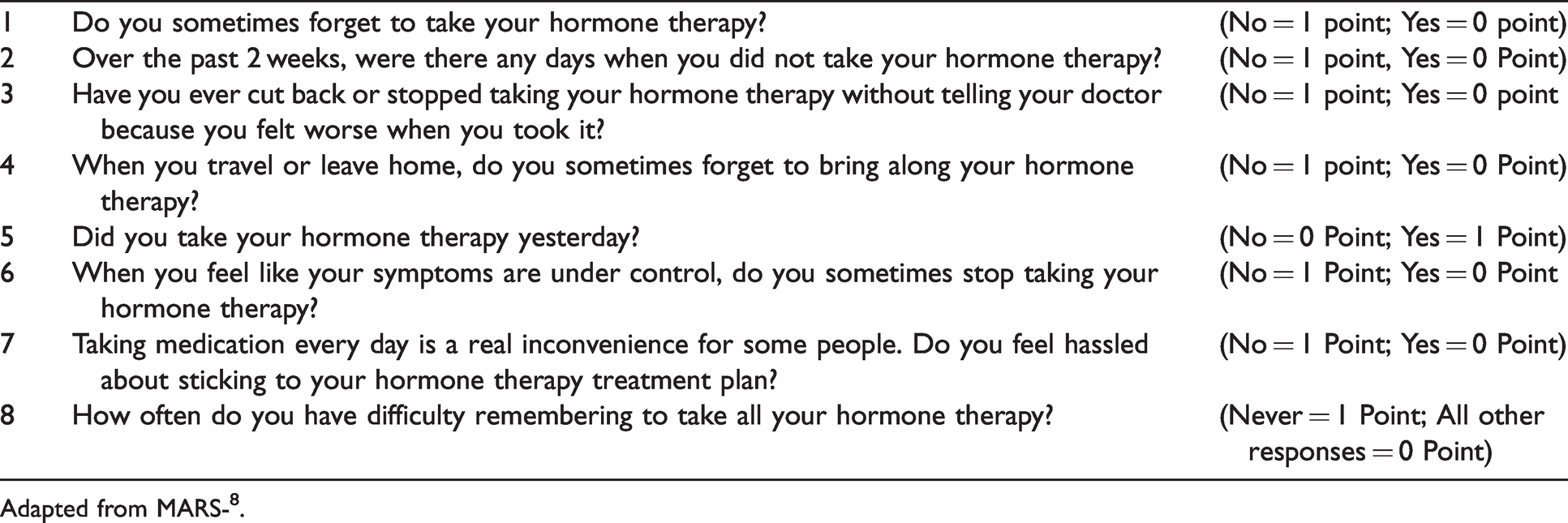
Adapted from MARS-8.
Statistical analysis
The association between clinical variables and adherence rate scores were carried out using Spearman Correlation, T-Test, Mann-Whitney U Test, and X2 tests. A p value of ≤0.05 was considered significant.
Results
Study participants
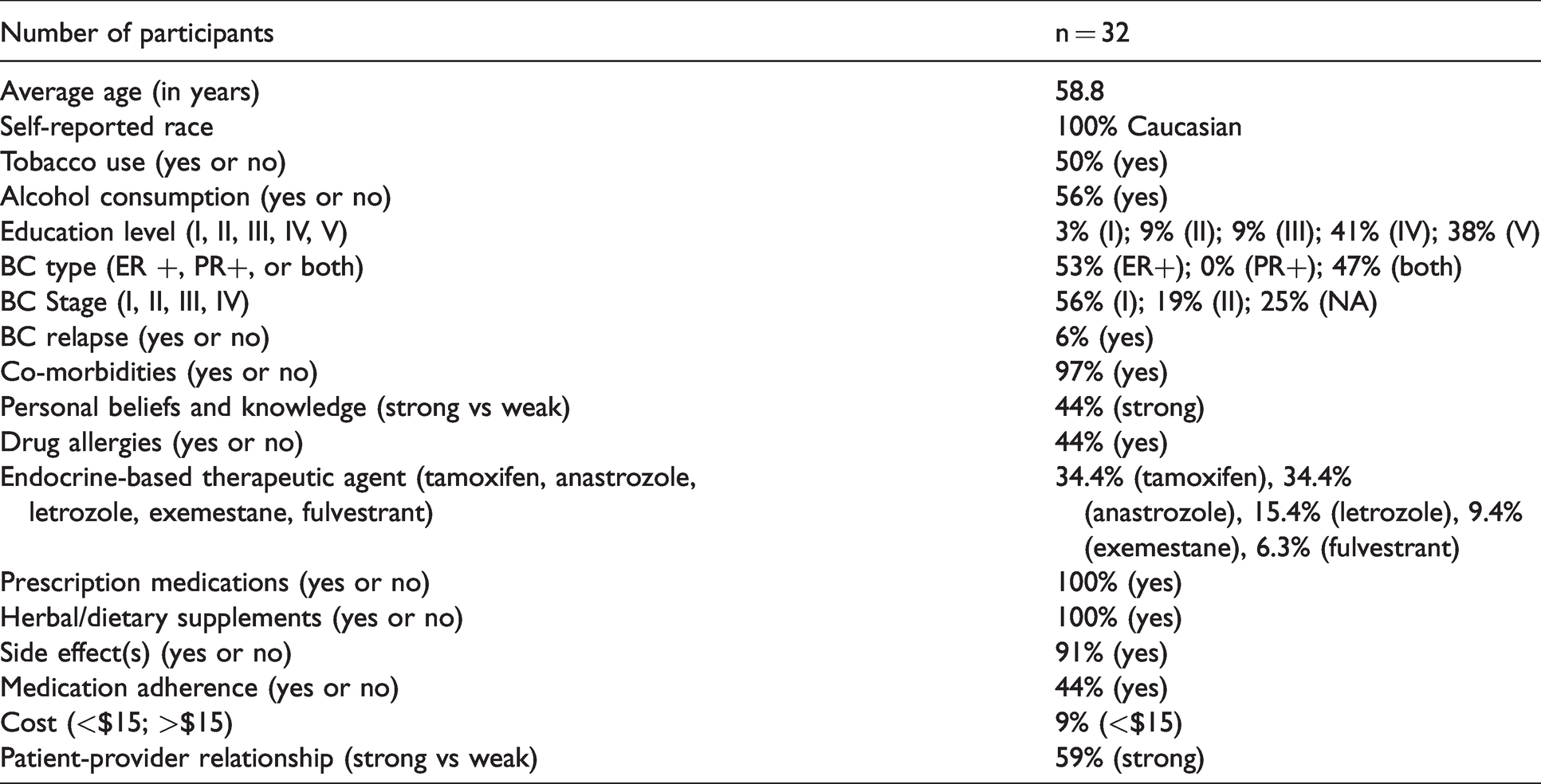
The combined results of the demographic and clinical variables for the 32 participants are summarized and reported in numerical form above (Table 2).
Demographics and clinical variables.
Medication adherence
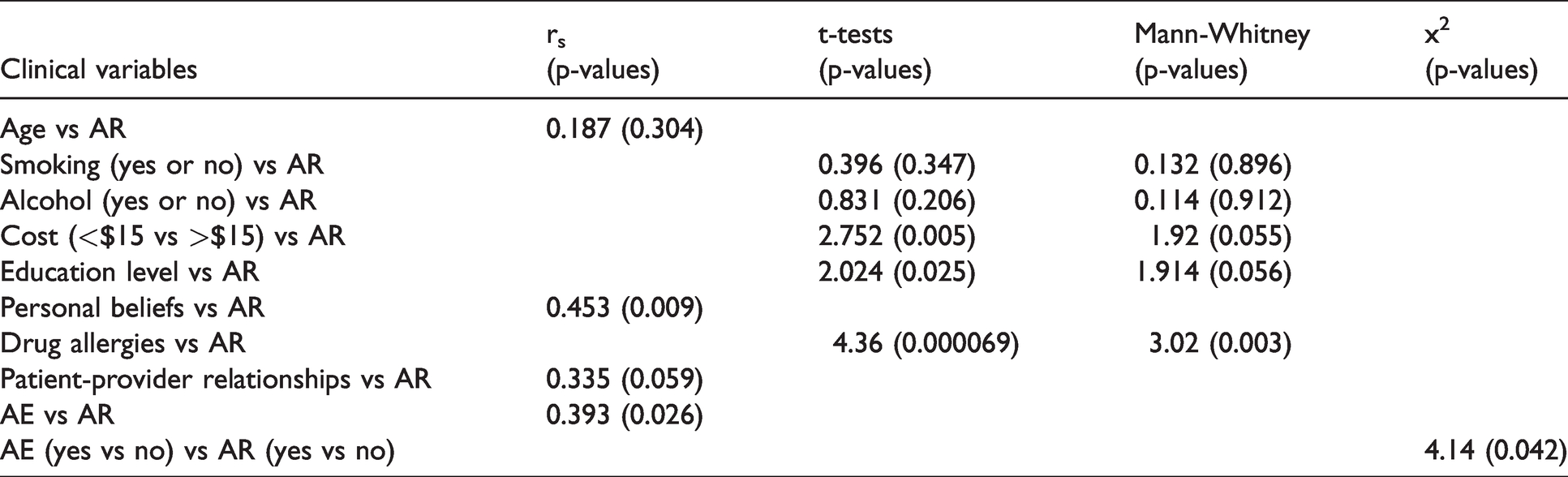
Medication adherence scores were given using MARS-8 8 adapted questions (Table 1). From those questions, 59% of the participants in our study were scored as non-adherent to their endocrine-based breast cancer therapy (Figure 1). Any score less than 100% on our modified MARS-8 scoring system was considered non-adherent, as 87.5% would be the next highest score that you could receive and that would imply some level of non-adherence. Among clinical variables and demographics tested (Table 2), statistical analysis (Table 3) revealed that patients in our study with known drug allergies (p = 0.000069), with out-of-pocket expenses of more than $15 per month (p = 0.005), with poor personal beliefs (p = 0.009), with low education level (p = 0.025), with more adverse events (p = 0.026), and with poor provider relationship (p = 0.05) were found to be possible reasons for poor medication adherence to endocrine-based breast cancer therapy. Patient personal beliefs were found to correlate with patient adherence scores (Figure 2). As patient personal belief scores increase, so do adherence rates among the participants.
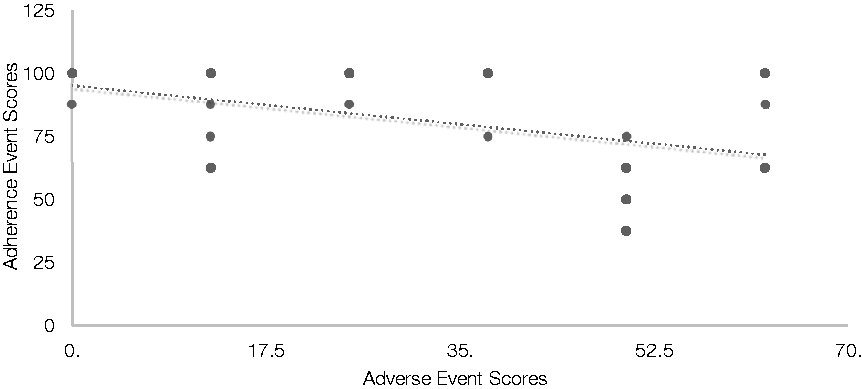
Adverse event scores versus patient adherence scores to endocrine-based breast cancer therapy.
Statistical analysis between adherence rates and clinical variables.
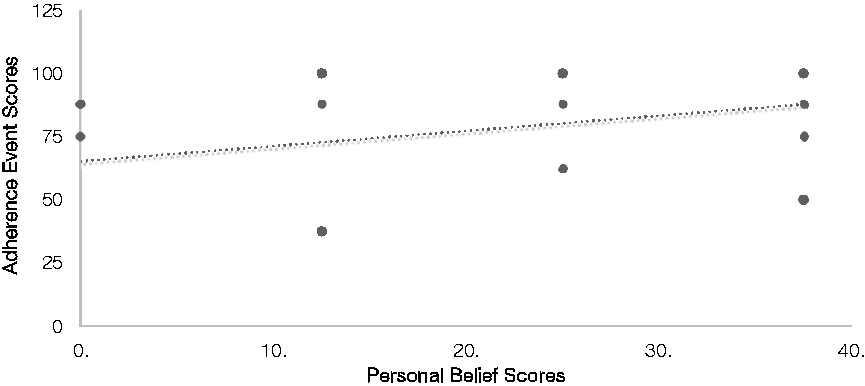
Personal belief scores versus patient adherence scores to endocrine-based breast cancer therapy.
Adverse events
Adverse events ranging from vaginal itching to pain occurred in 91% of study participants. The most common adverse event reported was hot flushes. Adverse event scores were found to correlate to decreasing adherence rates among the patient participants (Figure 1). 2 x 2 Chi Square analysis of adverse events further showed a significant correlation (p = 0.042) between medication adherence scores and adverse events (Table 3).
Discussion
Our study identified several factors that could explain the lack of patient adherence to Tamoxifen (TAM) and aromatase inhibitors (AI). Poor patient-provider relationship (p = 0.05), adverse drug events (p = 0.026), low education level (p = 0.025), poor personal beliefs about treatment (p = 0.009), the cost of medications (p = 0.005), and previous drug allergies (p = 0.000069) were all shown to be significant factors relating to adherence to endocrine-based breast cancer therapy. Each of the identified factors allows us to better understand the plight of a patient with breast cancer from their perspective. Since medication adherence is paramount in preventing breast cancer relapse and mortality, we believe that the additional information we attained through this study could be significantly impactful to patient outcomes.
A poor patient-provider relationship has previously been identified as a barrier to patient medication adherence. 10 Our study also found a relationship between the patient and the provider to be of vital importance. Liu et al. found that poor communication within the patient-provider relationship was as significant barrier to patient medication adherence to oral endocrine therapy. 10 We believe patient-provider relationship greatly impacts the well- being and overall health of patients treating breast cancer with tamoxifen or aromatase inhibitors.
Previous published papers assessed the effect adverse events have on medication adherence. 11 Our study also found that adverse events, including but not limited to vaginal pain, itching, and hot flushes were barriers to patient adherence to their prescribed AI or TAM. Medication side effects are common, and we believe that patient education on the known side effects for TAM and AI is key in improving medication adherence. A study published in 2011 by Brown et al. showed that drug- related adverse effects was the most common concern among patients they surveyed in their study. 9 Side effects of TAM and AI can often be detrimental to patient's overall health and well- being. It isn't surprising that these adverse events can prevent patients from adhering to their prescribed treatment.
Our study asked participants to select their highest education level. The adherence rate of patients who reported a lower education level was worse compared to those with higher education levels. The link between patient education level and medication adherence was found to be significant in our study. A previous study of patients with breast cancer showed that education level impacted patient adherence to medication therapy. 12 It is possible that patients with lower education levels weren't able to fully comprehend the importance of adherence to their prescribed AI or TAM. Prescribed instructions found on patient medication labels have been found to be confusing to the average patient. 13 We believe that patients with lower education levels need more medication counseling and better relationships with their providers.
The link between poor health beliefs and medication non-adherence to AI has been previously studied by Brier et al. 14 Our study echoed the previously found significance of patient personal beliefs on medication adherence. In our study, the survey sought to determine how much trust the patients had in their treatment plan, as well as how effective their treatment would be in preventing cancer relapse. The patients that responded negatively had worse adherence rates than those that responded positively.
Like personal beliefs, the effects of medication cost on patient adherence to AI or TAM are well documented. 15 Sedjo et al. found that AI non-adherence was directly related to drug costs exceeding $30. In our study, the copay breakpoint was set at $15 for statistical analysis purposes. Our study found that medication cost, specifically cost exceeding $15 to be a significant contributing factor in patient non-adherence to AI or TAM. The difference in cost between the Sedjo et al. study and ours can be attributed to differences in income levels in different geographic locations of the country. As expected, those patients with a higher cost burden were less adherent to their prescribed medications. Cost of medications was found to be the second most significant factor in patient adherence to endocrine-based breast cancer therapy.
The most significant factor we found to be a barrier to patient medication adherence to TAM and AI was drug allergies. To our knowledge, this is the first time that drug allergies have been identified as a significant patient barrier in terms of medication adherence to endocrine-based breast cancer treatment. We believe that patients with previous drug allergies could be wary of taking medications such as AI or TAM since they have had negative reactions to other medications. Even patients with a belief that they are allergic to a medication may be negatively affected, even if they do not possess a true allergy to the said medication in question.
Several limitations were found in this study. The adapted MARS-8 questionnaire was chosen for the first phase of this study due to its accessibility and affordability. This system was originally developed and validated to assess adherence with psychoactive medications and has not yet been validated for use in breast cancer medication adherence assessment. 8 More sophisticated tools will ideally be used in later phases of this study. Other limitations include, but are not limited to, the relatively small sample size, the lack of diversity in the patient population, and the failure of 25% of our participants to report the stage of their disease progression. The small sample size and lack of diversity in the patient population limits the generalizability of the results of this study to a larger group of individuals. A larger sample size with a wider range of diversity will ideally be utilized in the next phases of this study. While there were limitations to this study, the results are significant enough to warrant further investigation.
All of the significant factors found in our study (i-poor patient-provider relationship, ii-adverse drug events, iii-low education level, iv- poor personal beliefs about treatment, v-medication cost, and vi-previous drug allergies) could be affected positively by drug experts, also known as pharmacists, assuming a greater role in managing medications for patients on AI or TAM. Pharmacists are easily accessible to patients and have been trained not only to be experts in the field of pharmacology and pharmacotherapy, but also in the area of patient-centered care that includes patient counseling and relationship building. Recently, the Joint Commission of Pharmacy Practitioners created a standard care process for pharmacists to employ when treating patients. 16 This patient-centered process has been added to the curriculum of many colleges of pharmacy across the nation. The patient care process developed by the JCPP has elevated pharmacy practice by emphasizing the patient role in decision making and treatment planning. While it is known that pharmacists could have a profound impact on improving medication adherence in breast cancer patients, research studies aimed at identifying and validating factors underlying poor medication adherence should be continued.
Overall, our study suggests that drug allergies appear to be a significant determinant of endocrine therapy adherence. Therefore, future studies aimed at validating the importance of known drug allergies in endocrine therapy adherence are warranted. This data will help a great deal in improving medication adherence measuring tools in order to personalize endocrine therapy among postmenopausal women with hormone-receptor positive breast cancers, which will ultimately improve breast cancer patient outcomes.
Footnotes
Compliance with ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Author contributions
All authors discussed the results and reviewed and approved the manuscript.
Data sharing statement
All data requests should be submitted to the corresponding author at
Ethical approval
All procedures performed in this study were in accordance with the ethical standards of Harding University Institutional Review Board (which reviewed and approved the protocol for this study) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Institutional Review Board approval number is 2016-006.
Informed consent statement
All volunteers signed written informed consent under said protocol.
Acknowledgments
The authors would like to acknowledge the breast cancer patients and survivors for their participation, the Arkansas Cancer Coalition team, KAITV8, The Broadway Joe morning show, Sara E. Goodson, Morgan A. Nicholson, Susana P. Villalba, Travis S. Ezell, Paola L. Quijano, Queenie H. Y. Wan and Khuong Q. Ly.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.