
Abstract
Introduction
Palbociclib is a small-molecule cyclin-dependent kinase 4/6 inhibitor used to treat hormone receptor-positive, human epidermal growth factor receptor-2 negative advanced breast cancer. Patient-specific factors impacting dose reductions or discontinuations are unknown.
Methods
The primary objective was to evaluate the association of age (<60 vs. ≥60 years) with palbociclib dose reductions or discontinuations secondary to neutropenia. This single-center, retrospective chart review included hormone receptor-positive, human epidermal growth factor receptor-2 negative advanced breast cancer patients ≥18 years treated with palbociclib between April 2015 and May 2020. Patients <60 years at the time of palbociclib initiation were in the younger group and patients ≥60 years were in the older group.
Results
Among the 107 patients included, younger patients were less likely than older patients to have a palbociclib starting dose <125 mg (0% vs. 11.9%, p = 0.02). Differences in palbociclib dose reductions or treatment discontinuations secondary to neutropenia were not detected (35.4% vs. 42.4%, p = 0.55). Neither the total number of palbociclib dose reductions (none: 54.2% vs. 49.1%, one: 33.3% vs. 42.4%, two: 12.5% vs. 8.5%, p = 0.61), nor the final dose of palbociclib (125 mg: 54.2% vs. 40.7%, 100 mg: 29.2% vs. 27.1%, 75 mg: 16.7% vs. 32.2%, p = 0.17) differed between younger and older patients.
Conclusions
Age (<60 vs. ≥60 years) was not associated with the rate of palbociclib dose reductions or discontinuations secondary to neutropenia. Older (≥60 years) patients were more likely to start palbociclib at lower doses which may impact neutropenia and non-neutropenic intolerance.
Introduction
Palbociclib is an orally administered, small-molecule inhibitor of cyclin-dependent kinases 4 and 6 (CDK4/6) used for the treatment of hormone receptor-positive (HR+), human epidermal growth factor receptor-2 negative (HER2−) advanced breast cancer.1–3 It is approved for initial therapy in combination with an aromatase inhibitor, and for progressive disease in combination with fulvestrant. 1 For either indication, the starting dose of palbociclib is 125 mg by mouth once daily for 21 days of a 28-day cycle.1–3 Dose reductions are recommended for concurrent use with strong cytochrome 3A inhibitors, and in patients with severe hepatic impairment given palbociclib undergoes extensive hepatic metabolism. 1 Hematologic and non-hematologic toxicities can both require palbociclib dose delays and dose reductions during subsequent cycles.
The most common palbociclib-induced toxicity is neutropenia.1,4–6 PALOMA-1, PALOMA-2, and PALOMA-3 clinical trials evaluated palbociclib in various treatment settings leading to US Food and Drug Administration (FDA) approval in 2015.4–6 The incidence of neutropenia of any grade was 74% in PALOMA-1, 79.5% in PALOMA-2, and 84.1% in PALOMA-3.4–6 Grade 3 or higher neutropenia occurred in >65% of patients in PALOMA-2 and PALOMA-3, necessitating palbociclib dose reductions in more than one-third of patients in PALOMA-2.5,6 Although grade 3 and grade 4 neutropenia were commonly observed, febrile neutropenia was rare and incidence did not exceed 2% in any of the PALOMA trials.4–6 Despite the need for frequent palbociclib dose reductions, few studies have evaluated prognostic factors identifying patients at the highest risk of palbociclib-induced neutropenia and risk factors remain largely unknown. 7
Neutropenia is a class effect with CDK4/6 inhibitors but is biologically distinct from the neutropenia caused by cytotoxic chemotherapy.8–11 Treatment with cytotoxic chemotherapy causes DNA damage that ultimately results in apoptotic cell death. This includes apoptosis of neutrophil precursor cells, which leads to delayed recovery of neutrophils. 10 In contrast, in vitro studies have shown that palbociclib-induced neutropenia is caused by a cell-cycle arrest, but without corresponding senescence of proliferating neutrophil precursor cells. 10 Therefore, palbociclib-induced neutropenia is reversible, and neutrophil count recovery occurs rapidly following therapy discontinuation, often within one week.10,11 The distinct differences in the underlying biological mechanisms of drug-induced neutropenia between cytotoxic chemotherapy and palbociclib prompt different management strategies. Granulocyte colony-stimulating factors can be used for neutropenia caused by cytotoxic chemotherapy, but are not typically used for CDK4/6 inhibitor-induced neutropenia. Instead, neutropenia is preferentially managed by dose interruption and dose modification of the CDK4/6 inhibitor.
At the University of North Carolina (UNC) Medical Center, the UNC Breast Oncology Group has anecdotally observed that younger patients (<60 years) are more likely than older patients (≥60 years) to require palbociclib dose adjustments secondary to neutropenia. Because there is limited published data available describing the association between age and palbociclib-induced toxicities, this study aimed to assess risk factors associated with palbociclib-induced neutropenia, dose reductions, discontinuations, and overall tolerability in patients being treated for HR+, HER2− advanced breast cancer.
Patients and methods
Patients and study design
This was a single-center, retrospective study that included adult females diagnosed with HR+, HER2− advanced breast cancer (stage III or IV) treated with palbociclib at UNC Medical Center between 10 April 2015 (the first-day palbociclib was prescribed at UNC Medical Center) and 31 May 2020 (UNC IRB 20-1360 approval). To ensure data regarding palbociclib therapy was complete, patients were only analyzed if they had stopped palbociclib treatment by 31 May 2020. Major exclusion criteria included patients on a clinical trial with palbociclib, patients who were prescribed but never initiated palbociclib, patients not followed longitudinally at UNC Medical Center for management of their breast cancer, and patients with HR negative (HR−) or HER2 positive (HER2+) breast cancer. Patients were divided into two groups by age, <60 years versus ≥60 years. Select demographic data collected included age, race, menopausal status, previous treatments (i.e. endocrine, chemotherapy, and radiation), disease stage, baseline labs, and therapies given concurrently with palbociclib, as well as date and dose of treatment initiation.
Primary and secondary objectives
The primary objective of this study was to compare the composite incidence of palbociclib-induced neutropenia that led to a dose reduction or discontinuation between the younger (<60 years) and older (≥60 years) study groups. Palbociclib-induced neutropenia was defined as an absolute neutrophil count (ANC) <1 × 10 9 /L after palbociclib treatment initiation. Secondary objectives included differences in the total number of dose reductions, final palbociclib dose, final palbociclib administration frequency, time to first neutropenia-induced dose reduction or discontinuation, ANC at the time of first neutropenia-induced dose reduction or discontinuation, and the composite incidence of palbociclib dose reduction or discontinuation not attributable to neutropenia. The rationale for dose reductions or palbociclib discontinuation was confirmed by provider documentation in the electronic health record (EHR). Time to neutropenia-induced dose reduction was defined as the time between initiation of palbociclib and the date a new prescription with a lower dose of palbociclib was e-scribed. Time to neutropenia-induced dose discontinuation was defined as the time between the initiation of palbociclib and the date when the treating provider documented instructions to discontinue palbociclib. Patients were counted as having an event at the time of first palbociclib dose reduction or discontinuation due to neutropenia. Patients who did not experience a palbociclib dose reduction nor neutropenia-induced discontinuation (but discontinued palbociclib for another reason) were censored at the time of discontinuation. Frequency changes were defined as any change in the palbociclib administration schedule that differed from taking palbociclib for 21 days followed by 7 days off to complete a 28-day cycle. Palbociclib dose reduction and discontinuation not attributable to neutropenia were determined to be due to medication intolerance, disease progression, loss to follow-up, patient death, or palbociclib discontinuation for other reasons.
Statistical analyses
Descriptive statistics were used to assess baseline clinical and demographic data. Fisher's exact tests were used to compare differences in categorical variables between the two study groups, and Wilcoxon rank-sum tests were used to compare differences in continuous variables between the groups. Kaplan–Meier analyses were used to assess time-to-event endpoints. A P-value <0.05 was considered statistically significant. Time-to-event graphics were created with R version 3.6.0 software as well as R packages ggplot2, survival, and survminer (R Core Team, Vienna, Austria). All other statistical analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results
Patient characteristics
A total of 312 patients prescribed palbociclib at UNC Medical Center for HR+ and HER2− advanced breast cancer were reviewed for eligibility in this single-center, retrospective chart review. Of the initial 312 patients, 107 patients (48 patients in the <60 years study group and 59 patients in the ≥60 years group) were included in the final analyses (Figure 1). Baseline clinical and demographic characteristics were similar between the two study groups (Table 1).
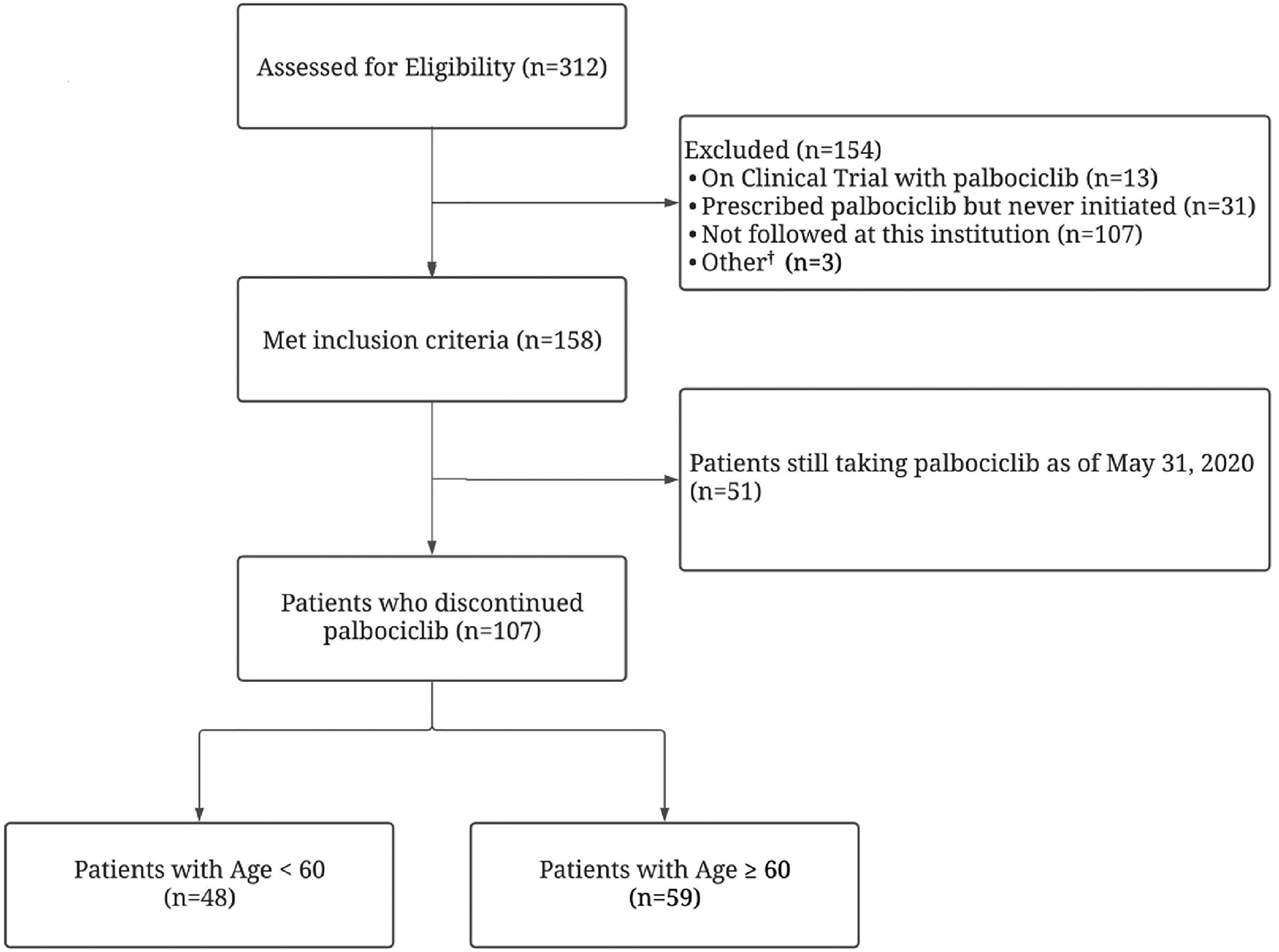
Enrollment diagram. †Other reasons for exclusion: palbociclib prescribed for liposarcoma (n = 1), palbociclib prescribed for bladder cancer (n = 1), palbociclib prescribed in a human epidermal growth factor receptor-2 positive patient (n = 1).
Patient demographic characteristics.
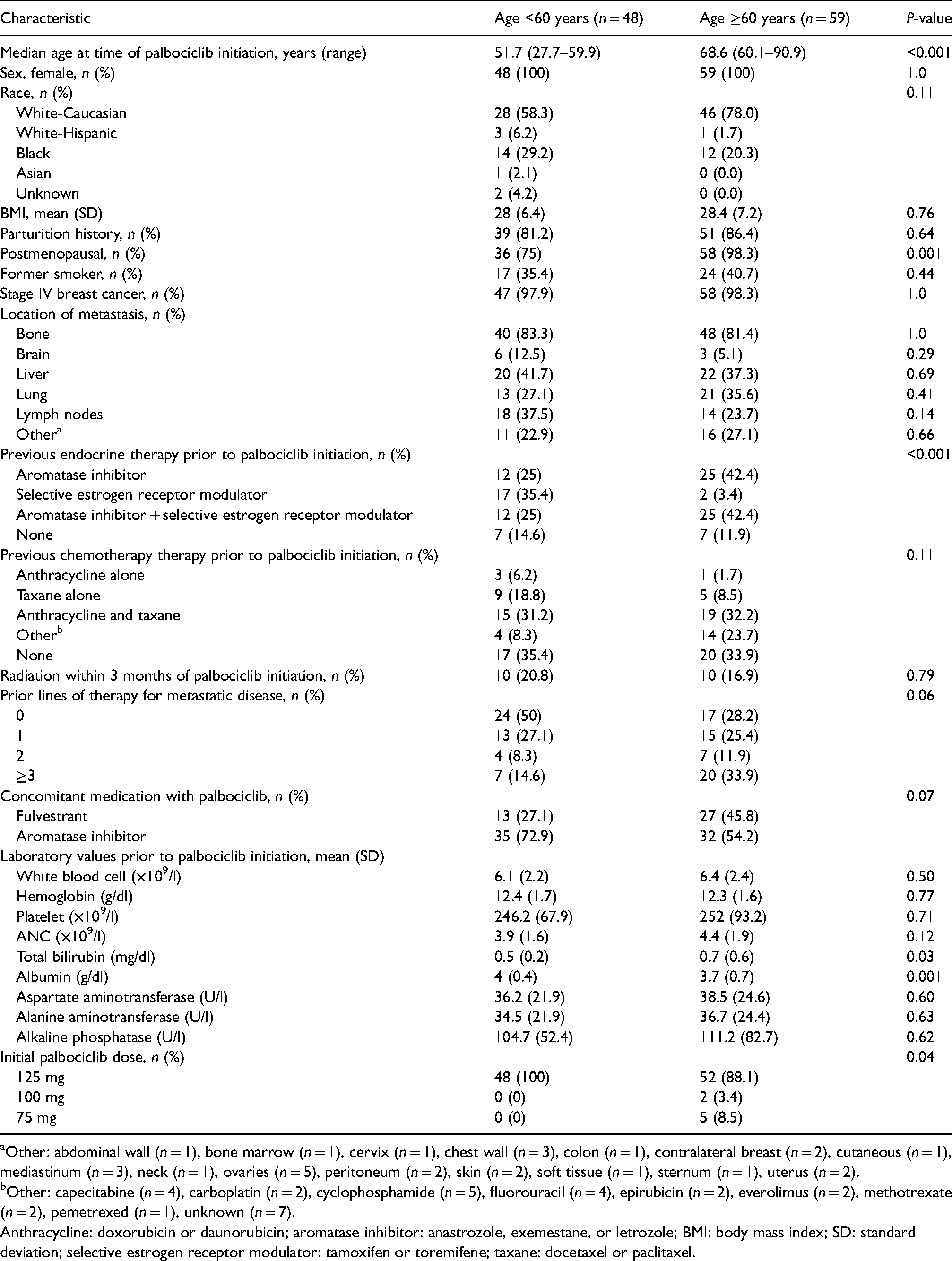
Other: abdominal wall (n = 1), bone marrow (n = 1), cervix (n = 1), chest wall (n = 3), colon (n = 1), contralateral breast (n = 2), cutaneous (n = 1), mediastinum (n = 3), neck (n = 1), ovaries (n = 5), peritoneum (n = 2), skin (n = 2), soft tissue (n = 1), sternum (n = 1), uterus (n = 2).
Other: capecitabine (n = 4), carboplatin (n = 2), cyclophosphamide (n = 5), fluorouracil (n = 4), epirubicin (n = 2), everolimus (n = 2), methotrexate (n = 2), pemetrexed (n = 1), unknown (n = 7).
Anthracycline: doxorubicin or daunorubicin; aromatase inhibitor: anastrozole, exemestane, or letrozole; BMI: body mass index; SD: standard deviation; selective estrogen receptor modulator: tamoxifen or toremifene; taxane: docetaxel or paclitaxel.
The majority of patients were postmenopausal (87.9%) and had stage IV breast cancer (98.1%) that had metastasized to the bone (82.2%). Endocrine therapy prescribed prior to palbociclib initiation was statistically significantly different between groups (p < 0.001), with a greater proportion of younger patients (35.4%) receiving monotherapy with tamoxifen than older patients (3.4%). Compared to younger patients (50.0%), older patients (71.8%) were more likely to have received at least one previous line of therapy for stage IV, although this was not statistically significant between the groups (p = 0.06). Younger patients (27.1%) were also prescribed fulvestrant as concomitant therapy with palbociclib less often than older patients (45.8%), although this was also not statistically significantly different between the groups (p = 0.07). Patients in the younger study group were more likely to be prescribed an initial palbociclib dose of 125 mg compared to patients in the older study group (100% vs. 88.1%, p = 0.04).
Palbociclib tolerability
For the study primary endpoint, a statistically significant difference in palbociclib dose reductions and treatment discontinuations due to treatment-emergent neutropenia was not observed between the two study groups (Table 2).
Palbociclib tolerability.
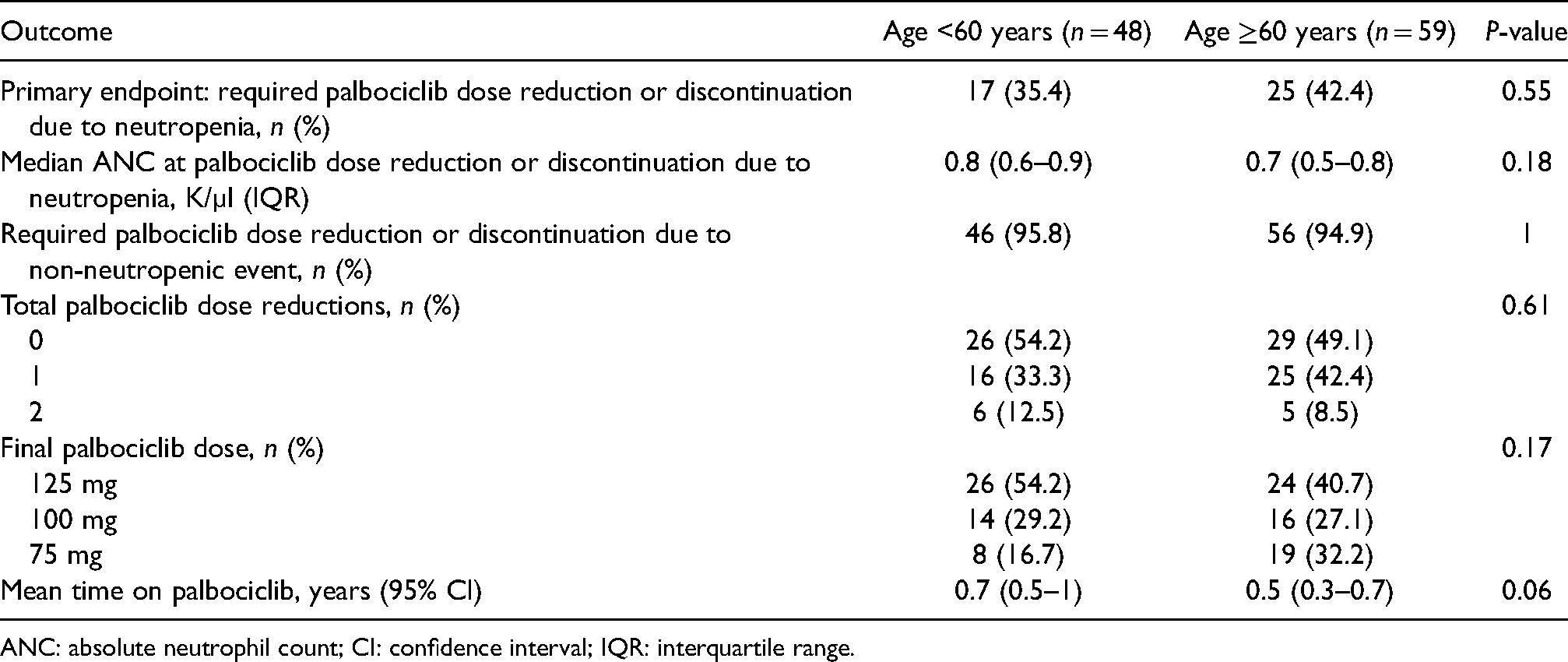
ANC: absolute neutrophil count; CI: confidence interval; IQR: interquartile range.
There were 17 patients in the younger study group (35.4%; 95% confidence interval [CI] 22.1–50.5%) and 25 patients in the older group (42.4%; 95% CI 29.6–55.9%) who required a dose reduction or discontinued palbociclib secondary to neutropenia (p = 0.55). There was an observed difference of 7.0% (95% CI −13.4% to 27.3%) in the rates of patients who required palbociclib dose reduction or discontinuation secondary to neutropenia between age groups. At the first palbociclib dose reduction or discontinuation due to neutropenia, median ANC was not different between the younger and older study groups (0.8 × 10 9 /l vs. 0.7 × 10 9 /l, p = 0.18). The median time to first palbociclib dose reduction or discontinuation due to treatment-emergent neutropenia was 0.13 years (range 0.02–3.21 years) in the younger treatment group versus 0.1 years (range 0.04–0.69 years) in the older treatment group. However, this was not statistically significantly different between study groups (p = 0.29) (Figure 2). Of all included patients, the majority (95.3%) required a palbociclib dose reduction or discontinued palbociclib due to a non-neutropenic event.
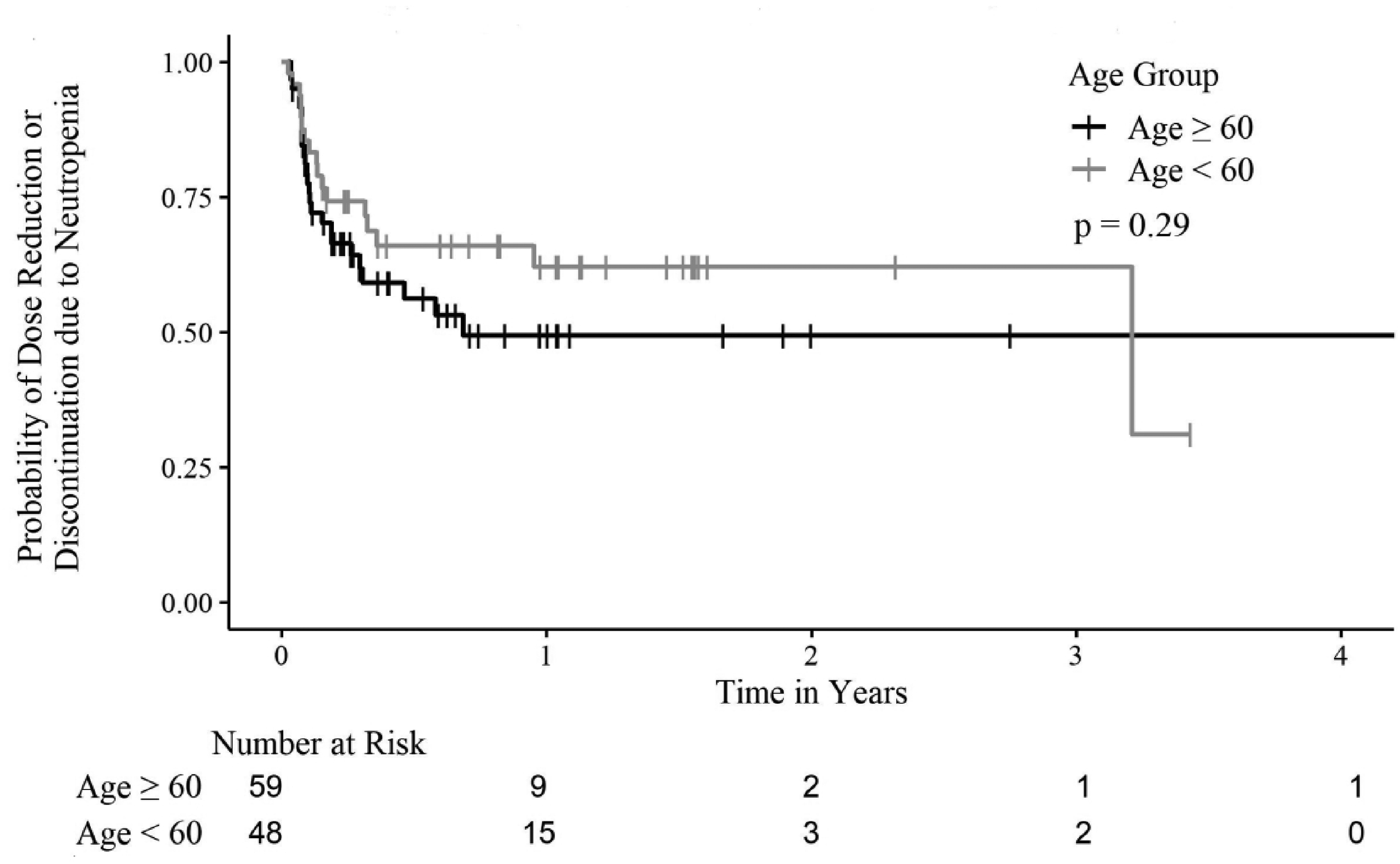
Time to first palbociclib dose reduction or discontinuation due to neutropenia. An event was recorded at the time of first palbociclib dose reduction or discontinuation due to neutropenia. Patients who neither had a palbociclib dose reduction nor discontinued palbociclib due to neutropenia, but discontinued palbociclib for another reason, were censored at the time of discontinuation (n = 65).
Of the 52 total patients who required palbociclib dose reductions, 25% (n = 13) had their first palbociclib dose reduced secondary to a non-neutropenic event, the remaining 75% (n = 39) had a dose reduction secondary to neutropenia. A greater proportion of patients in the older group (50.8%; n = 30) than the younger group (45.8%; n = 22) required a palbociclib dose reduction, but this was not a statistically significant difference between the younger and older study groups (p = 0.61). Similarly, although a statistically significant difference in final palbociclib dose was not observed between the study groups (p = 0.17), fewer patients in the younger group had a final palbociclib dose of 75 mg (16.7%) compared to the older group (32.2%). The time to first palbociclib dose reduction or discontinuation for any reason was not statistically significantly different between the older and younger age groups (p = 0.37). The median time to first palbociclib dose reduction or discontinuation for any reason was 0.25 years (range 0.02–3.43 years) in the younger treatment group versus 0.22 years (range 0.04–4.3 years) in the older treatment group (Figure 3). Most commonly, patients in both the younger and older study groups discontinued palbociclib secondary to disease progression (85.4% vs. 66.1%, respectively). Among the older study group, 20.3% (n = 12) of patients discontinued palbociclib due to medication intolerance for reasons other than neutropenia, including fatigue (n = 3; 5.1%) (Figure 4).
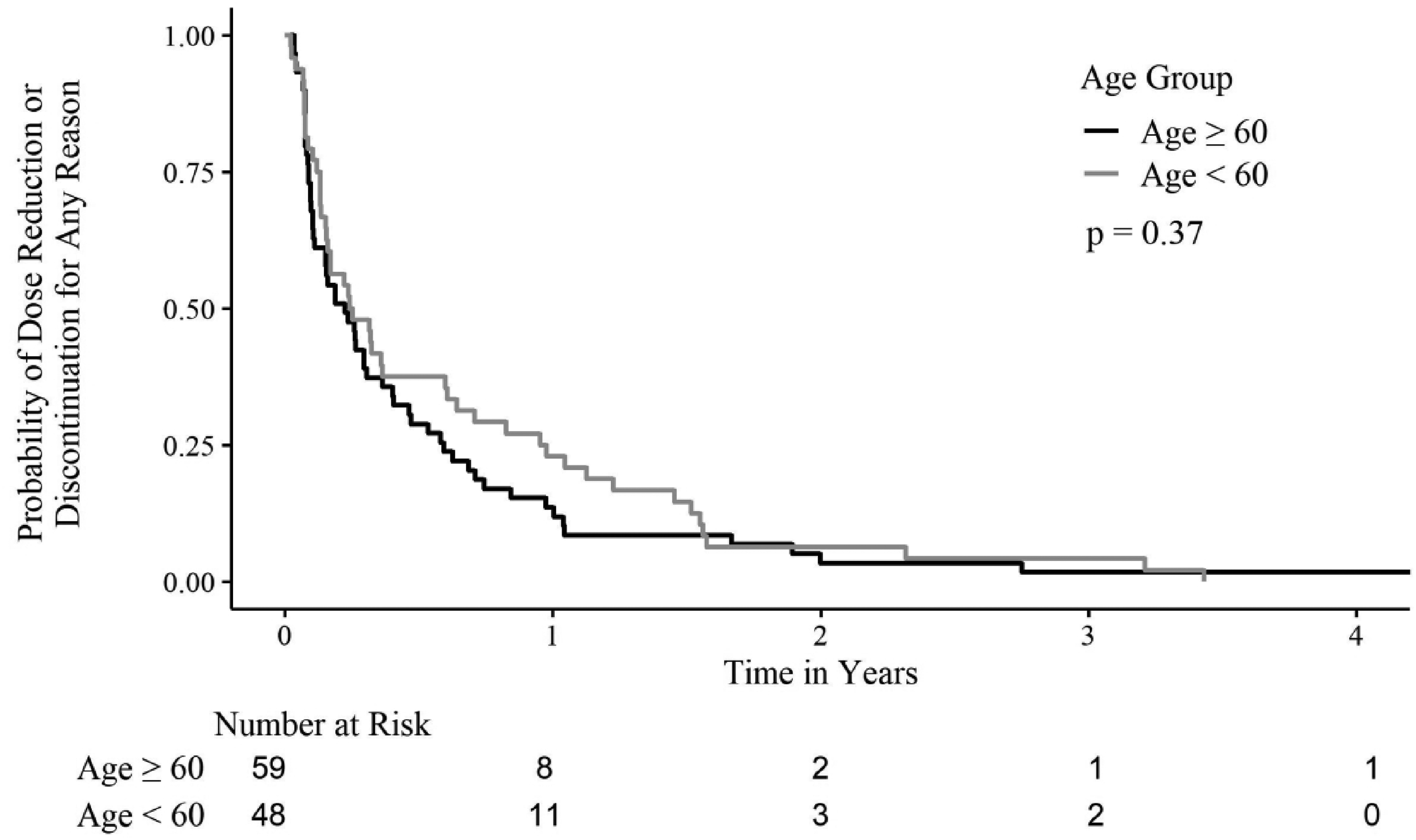
Time to first palbociclib dose reduction or discontinuation for any reason. Patients were counted as having an event at the time of first palbociclib dose reduction or discontinuation. All 107 patients discontinued palbociclib by the study end date; therefore, no patients were censored in this plot.
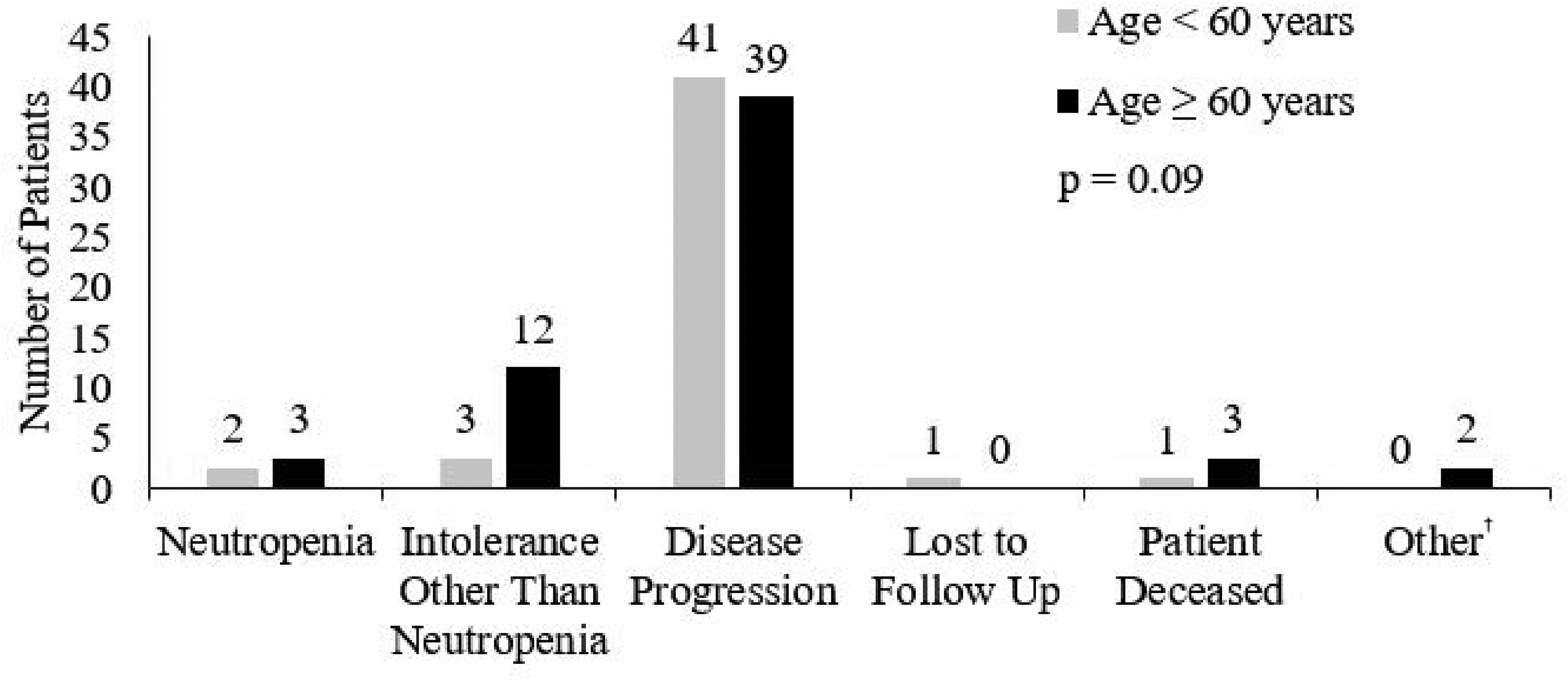
Reason for palbociclib discontinuation. †Other reasons for discontinuation included non-adherence (n = 1) and clinical status secondary to concomitant comorbidities (n = 1).
While there was a trend toward a longer mean time spent taking palbociclib among the younger study group (0.74 years; 95% CI 0.5–0.97) than the older group (0.52 years; 95% CI 0.33–0.71), this observation was not statistically significant (p = 0.06).
Discussion
Excluding non-melanoma skin cancer, breast cancer is the most common cancer in women in the US and worldwide.2,12 The majority of these women present with HR+ and HER2− disease. 13 When studied in these patients with advanced disease, the first-in-class CDK4/6 inhibitor palbociclib has been shown to prolong progression-free survival when combined with letrozole in previously untreated patients, and prolong both progression-free survival and overall survival when combined with fulvestrant in patients previously treated with endocrine therapy.5,6,14 Given these promising results from phase III clinical trials, it is essential to understand how these findings translate to real-world patients. While palbociclib toxicities and dose modifications have been studied previously, there is no literature primarily evaluating the impact of age on palbociclib tolerability of clinic patients. 13 Therefore, the primary goal of this retrospective study was to evaluate differences in palbociclib-induced neutropenia, dose reductions, dose discontinuations, and tolerability between younger (<60 years) and older patients (≥60 years).
This retrospective review of patients with advanced breast cancer prescribed palbociclib at a single medical center found that there was not a difference of palbociclib-induced neutropenia that led to a dose reduction or discontinuation between younger and older patients (35.4% vs. 42.4%, p = 0.55). Additionally, there was not a statistically significant difference between the number of dose reductions, final dose or dose frequency, ANC at the first dose reduction or discontinuation, or dose reduction or discontinuation for a non-neutropenic event for younger and older patients.
Our findings on the similar tolerability of palbociclib in younger versus older patients are supported in other trials. Three studies have assessed the impact of age on palbociclib tolerability. In a single-institution retrospective review by Gong et al., 15 29% of patients treated with palbociclib required dose reductions due to treatment-emergent toxicities. Of the 31 patients who were ≥65 years, 32.3% required a palbociclib dose reduction due to toxicities. Given the similar rates of palbociclib discontinuations between the overall cohort and those patients ≥65 years, the authors concluded older age did not impact palbociclib tolerability. These findings are consistent with palbociclib tolerability in our study as we also did not observe differences in tolerability between the younger and older groups. Although it must be noted that in contrast to our study where 11.9% of patients ≥60 years received a starting palbociclib dose of <125 mg, only 2% of their patients received palbociclib at a starting dose proactively reduced for anticipated intolerance due to age. In addition, a retrospective study completed by Pizzuti et al. 16 that evaluated palbociclib use did not detect significant differences in rates of toxicities between patients <75 years (n = 379) and ≥75 years of age (n = 44). In a pooled analysis of the PALOMA studies evaluating patients ≥65 years, 304 patients were treated with palbociclib in combination with letrozole or fulvestrant. 17 Rates of grade 3 or greater neutropenia were similar across age groups and older patients did not demonstrate any new safety concerns prompting the authors to conclude no palbociclib dose adjustments were required based on age. Nonetheless, our study demonstrated that older patients were more likely to have a reduced palbociclib starting dose in a real-world clinical practice which likely impacts subsequent palbociclib tolerability.
In one of the largest retrospective reviews of patients treated with palbociclib (n = 763), 79.9% of their patients received a palbociclib starting dose of 125 mg, while 93.5% of our patients started with the standard starting dose of 125 mg. 18 In this large retrospective review, with over half of them being >65 years, 20.1% of their patients required a palbociclib dose reduction, compared to the 48.6% of women in our study who required a dose reduction. Another study of patients treated with palbociclib by Bui et al. 19 found only 21.7% of patients required a palbociclib dose reduction and only 4.3% of patients required palbociclib discontinuation due to adverse effects. In comparison, our study found that 18.7% of the 107 included patients had palbociclib discontinued due to adverse events - neutropenia or intolerances other than neutropenia. Our retrospective review includes patients who initiated palbociclib soon after the FDA approved the medication. At that time, data was not available on the tolerance of this novel CDK4/6 inhibitor in younger versus older populations. Without information regarding the tolerability of palbociclib by older patients, providers at our institution took a conservative approach in prescribing this medication. This conservative approach could have led to differences in starting dose, dose reductions, and discontinuations. This prescribing practice was different than that of the Gong et al. 15 study where all patients were initially prescribed palbociclib 125 mg orally daily which may reflect real-world experiences. However, our results along with others indicate that older patients tolerate palbociclib similarly to younger patients.
This study directly compared toxicities and tolerability of palbociclib between two age groups of women with advanced breast cancer over a 5-year period at a single institution. One strength of this study is the enhanced understanding of common initial and sustained prescribing practices in a real-world breast cancer practice, which included information about palbociclib starting doses, the frequency of palbociclib dose reductions, and final palbociclib dose prescribed over a prolonged period. Additionally, beyond assessing the frequency of common toxicities such as neutropenia, this study evaluated time to treatment-emergent toxicity and the reasons for palbociclib discontinuation. Unlike the studies by Pizzuti et al. 16 and Gong et al., 15 which looked at real-world use of palbociclib for only one year, our study evaluated data over a 5-year period. 17 Five years of following-up women who were prescribed palbociclib demonstrated that the majority of patients discontinued this medication due to disease progression rather than intolerance. This finding importantly indicates that similarly to young patients, our older patients were able to tolerate palbociclib and continue the medication until disease progression. There are also limitations to this retrospective study. The sample size was based on a convenience sample and no formal a prior power calculation was done. Notably, there was only an observed difference of 7.0% (95% CI −13.4% to 27.3%) in the rates of patients who required palbociclib dose reduction or discontinuation secondary to neutropenia between age groups. Furthermore, data were collected via manual chart review from the electronic medical record, and inconsistency between provider documentation could have introduced selection bias. The timing and rationale of dose reductions subsequent to the first dose reduction, as well as the incidence and duration of palbociclib treatment delays due to toxicities, were not collected.
Conclusions
Age (<60 years vs. ≥60 years) was not associated with the rate of palbociclib dose reductions or discontinuations secondary to neutropenia, palbociclib dose reductions or discontinuations secondary to non-neutropenic events, total number of palbociclib dose reductions, or final palbociclib dose. Palbociclib was most often discontinued due to disease progression. Older patients were more likely to start palbociclib at lower doses, potentially reducing the frequency of neutropenic and non-neutropenic events. Future prospective trials are needed to understand the tolerability and safety of palbociclib in older patients. Additionally, future studies should investigate the effect of palbociclib starting dose on tolerability.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.