
Abstract
Introduction
Asparaginase derivatives are essential components of the treatment of acute lymphoblastic leukemia in adolescent and young adult patients. However, their associated toxicities limit wider use in older populations. This study seeks to determine if the practice of capping the pegaspargase dose at 3750 units reduces the risk of related adverse events in adults.
Methods
Adverse event data were retrospectively collected 28 days following each administration of pegaspargase in a single center. Doses were categorized as either capped (≤3750 units) (n = 57, 47.5%) or non-capped (>3750 units) (n = 63, 52.5%). The primary endpoint of this study was the composite incidence of serious pegaspargase-related adverse events, defined as grade 3 or higher.
Results
Of the 120 doses administered, 47 (39.2%) were administered to patients > 39 years. For the primary endpoint, 26 doses (45.6%) in the dose capped group versus 22 doses (34.9%) in the non-dose capped group were associated with serious pegaspargase-related adverse events (p = 0.23). Isolated laboratory abnormalities accounted for all hepatotoxicity and pancreatic toxicity events, while venous thromboembolism and bleeding occurred after 8.3% and 13.3% of doses, respectively. Multivariate analysis of the primary outcome to adjust for differences in baseline characteristics found no difference between groups (OR 2.56 (0.84, 7.77, p = 0.098)).
Conclusions
The incidence of serious clinical toxicities was low in this study, particularly pegaspargase-related venous thromboembolism. This suggests that the practice of capping pegaspargase doses at 3750 units, coupled with vigilant monitoring and prophylaxis for pegaspargase-related adverse events, can allow for the inclusion of this drug in the treatment of older individuals.
Introduction
Asparaginase products are a cornerstone of therapy for acute lymphoblastic leukemia (ALL) and their inclusion in chemotherapeutic regimens has extended event-free and overall survival in both pediatrics and adults.1,2 While older patients still benefit from the use of intensive regimens, they are often unable to tolerate such therapy due to the associated adverse effects (AEs). 3 AEs that occur due to pegaspargase (PEG-ASP) range from relatively benign to potentially life-threatening and include hyperglycemia, hypertriglyceridemia, hypersensitivity, venous thromboembolism (VTE), coagulopathy, hepatotoxicity, and pancreatitis. 4 While the types of AEs are similar between pediatric and adult patients, there appears to be a higher rate of grade 3–4 hepatic dysfunction, pancreatic dysfunction, and thrombosis in adults as compared to pediatrics. 5 Considering the benefit of including asparaginase products in the treatment of adult ALL, studies such as CALGB 9511 4 and a prospective study by Douer et al. 6 have examined utilizing lower doses of PEG-ASP in order to minimize toxicity.
In 2017, the University of Maryland Medical Center implemented a guideline for PEG-ASP-related toxicity monitoring, prevention, and management in adults, which has been described previously. 7 The recommendations in this guideline extend to all non-investigational uses of PEG-ASP in adults, which, in addition to the treatment of ALL, include acute myeloid leukemia utilizing the HAM-pegA regimen8,9 and NK/T-cell lymphoma utilizing the SMILE regimen. 10 This guideline instituted routine monitoring of liver function tests, amylase, lipase, antithrombin III, and fibrinogen, included prophylactic anticoagulation recommendations and recommended management strategies for hypofibrinogenemia, antithrombin III repletion, and hepatotoxicity. In the initial iteration of the guideline, the dose of PEG-ASP was 2500 units/m2 for all patients without an established maximum dose. The 2018 update to these guidelines made changes to antithrombin III repletion thresholds and the dose of levocarnitine used for hepatotoxicity, and, importantly, introduced a dose cap of one vial of PEG-ASP (3750 units). This dose capping practice followed the example of CALGB 9511, which showed adequate depletion of asparagine with PEG-ASP 2000 units/m2 capped at 3750 units per dose. 4 Additionally, doses of PEG-ASP that exceed 3750 units have been associated with higher incidences of toxicities including VTE, pancreatitis, and hyperglycemia, as seen by a previous retrospective study conducted in pediatric B-cell ALL patients. 11 With the growing interest in using lower doses of PEG-ASP and the limited data regarding the practice of capping the dose at one vial size across multiple disease states and regimens, the purpose of this study was to examine the effect of capping PEG-ASP doses at one vial size (3750 units) on asparaginase serious adverse events (SAEs) of interest. We hypothesized that this dosing strategy would result in a favorable safety profile as demonstrated by a decrease in the incidence of PEG-ASP-related SAEs with comparable clinical benefit as non-capped dosing.
Methods
This was an IRB-approved, single-site retrospective chart review of all doses of PEG-ASP administered to adult patients (≥18 years of age) at the University of Maryland Medical Center, a National Cancer Institute-designated comprehensive cancer center, from 15 November 2015 to 15 November 2019. The primary endpoint of this study was the composite incidence of SAEs in adult patients receiving dose capped versus non-dose capped PEG-ASP within 28 days of PEG-ASP administration. This composite endpoint was defined as the occurrence of any grade 3 or higher PEG-ASP-related hepatotoxicity, pancreatic toxicity (both clinical pancreatitis and isolated lab abnormalities), VTE, or hemorrhage. Secondary endpoints included the incidence of each individual component of the composite endpoint, time to event, and peak values of relevant laboratory parameters (i.e. hepatic transaminases, bilirubin, amylase, and lipase). Exploratory endpoints included overall response rate (ORR), rate of complete response (CR), rate of complete response with incomplete hematologic recovery (CRi), the rate of minimal residual disease (MRD), the incidence of hypersensitivity to PEG-ASP necessitating switching of therapy to Erwinia asparaginase (Erwinaze®), as well as the incidence of 28-day mortality between groups.
Administrations of PEG-ASP were excluded if they were given within 28 days of a previous dose of PEG-ASP. For patients who received a subsequent dose of PEG-ASP within the 28-day period, data collection for adverse events halted on the day the subsequent dose of PEG-ASP was administered. Baseline demographics, relevant baseline labs, and oncologic history were collected. Chemotherapeutic regimens were divided into three broad categories based on structure of the regimen and overall dose-intensity. High intensity regimens had structures similar to those of pediatric-inspired ALL protocols, or had doses of glucocorticoids or vincristine characteristic of pediatric regimens (i.e. CALGB10403, COG protocols, augmented Hyper-CVAD, and MOpAD). Reduced intensity regimens included ALL regimens designated for older adults, or which utilized a lower dose-intensity of glucocorticoids or vincristine. The last category of “miscellaneous” regimens included those that did not meet the above criteria, or were regimens typically used in diseases other than ALL (e.g. HAM-pegA and SMILE).
The dose capped and non-dosed capped groups were distinguished by the amount of PEG-ASP received and were defined as doses of PEG-ASP ≤ 3750 units and >3750 units, respectively. Grading of toxicity was defined as per the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Toxicity data were collected for all grades of VTE, and grade 3 or higher hepatotoxicity, pancreatic toxicity, and bleeding. Hepatotoxicity was defined by laboratory values only; pancreatic toxicity was defined by both laboratory values and by clinical evidence of pancreatitis via note documentation. CR, CRi, and MRD data were collected following completion of remission induction chemotherapy, and until initiation of consolidation or disease progression.
Statistical analysis
Each dose of PEG-ASP administered was treated as an individual instance. Therefore, patients who received multiple doses of PEG-ASP were potentially included multiple times as a separate subject within our analysis due to their receiving multiple PEG-ASP-containing cycles of treatment. Previous exposure to PEG-ASP was recorded, and data were also analyzed on a per-patient basis to account for these instances of patients who received multiple doses of PEG-ASP. This was a convenience sample over the pre-specified time period, for which power was retrospectively calculated. To detect a difference in proportions of 0.25 with 80% power, the total sample size required was 134 doses. Descriptive statistics were used to measure and quantify characteristics of the study population. Differences between non-dose capped and dose capped groups were analyzed using chi-square test or Fisher's exact for categorical variables, and t-test or Wilcoxon rank-sum test for continuous variables. The association between the outcome variable, composite toxicity, and various factors was analyzed using multivariate analysis. For multivariate analysis, a multiple logistic regression model was conducted to evaluate for independent factors. The odds ratio with 95% confidence interval (CI) was used to measure the magnitude of association. The variance inflation factor and correlation coefficients were used to identify multicollinearity. The Hosmer–Lemeshow test and the area under the receiver operating characteristics (ROC) curve were used to assure goodness-of-fit and the discriminatory power. The association between the secondary outcome variables and various factors were analyzed using bivariate analysis. Analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC).
Results
During the study period, a total of 129 doses of PEG-ASP were identified, nine of which were excluded due to being administered within 28 days of the previous dose; 120 doses were included in the final analysis. Of the nine doses that were excluded, six doses would have been included in the non-dose capped group and two in the dose capped group, with one dose unevaluable. There were 57 doses of PEG-ASP in the dose capped group (47.5%) given across 28 patients, and 63 doses (52.5%) in the non-dose capped group given across 30 patients, or an estimated 2.03 and 2.1 doses per patient in each group respectively. Because these data were analyzed on a per-dose basis, four patients had doses that fell into both groups, and each dose was included within their respective groups. Baseline characteristics were analyzed both as per dose and per patient in Table 1a and Table 1b, respectively, and were largely similar between groups. Of the 120 doses assessed, 37 (39.2%) were given to patients over 39 years. The overall median age was within the adolescent and young adult (AYA) range of 15-39 years—the median age was 34 years in the dose capped group and 32 years in the non-dose capped group; however, when analyzed per patient, the median age in the dose capped group was above the AYA range at 42.5 years. The ages spanned a wide range from 21–70 years in the dose capped group and 18–61 years in the non-dose capped group. The composition of groups differed in terms of doses given to patients of Black race, with 28.1% of such doses in the dose capped group compared to 12.7% in the non-dose capped group (p = 0.060). Doses were administered to relatively fit patients with ECOG 0–1; 87.7% in the dose capped group and 71.4% in the non-dose capped group. The distribution of disease types differed between doses given to each group, with a higher relative percentage of B-ALL patients in the dose capped arm and a higher relative percentage of T-ALL patients in the non-dose capped arm (p = 0.0006). Most doses were part of high intensity regimens, and this was not different between groups. In assessing for potential confounders of the incidence of PEG-ASP-related adverse events, differences between dose capped and non-dose capped groups were identified in baseline serum total bilirubin (0.5 mg/dL, 0.8 mg/dL; p = 0.0057), history of prior VTE (12.3%, 38.1%; p = 0.0013), and baseline prothrombin time (PT) (14.0 s, 14.7 s; p = 0.047).
Baseline characteristics by dose of pegaspargase.
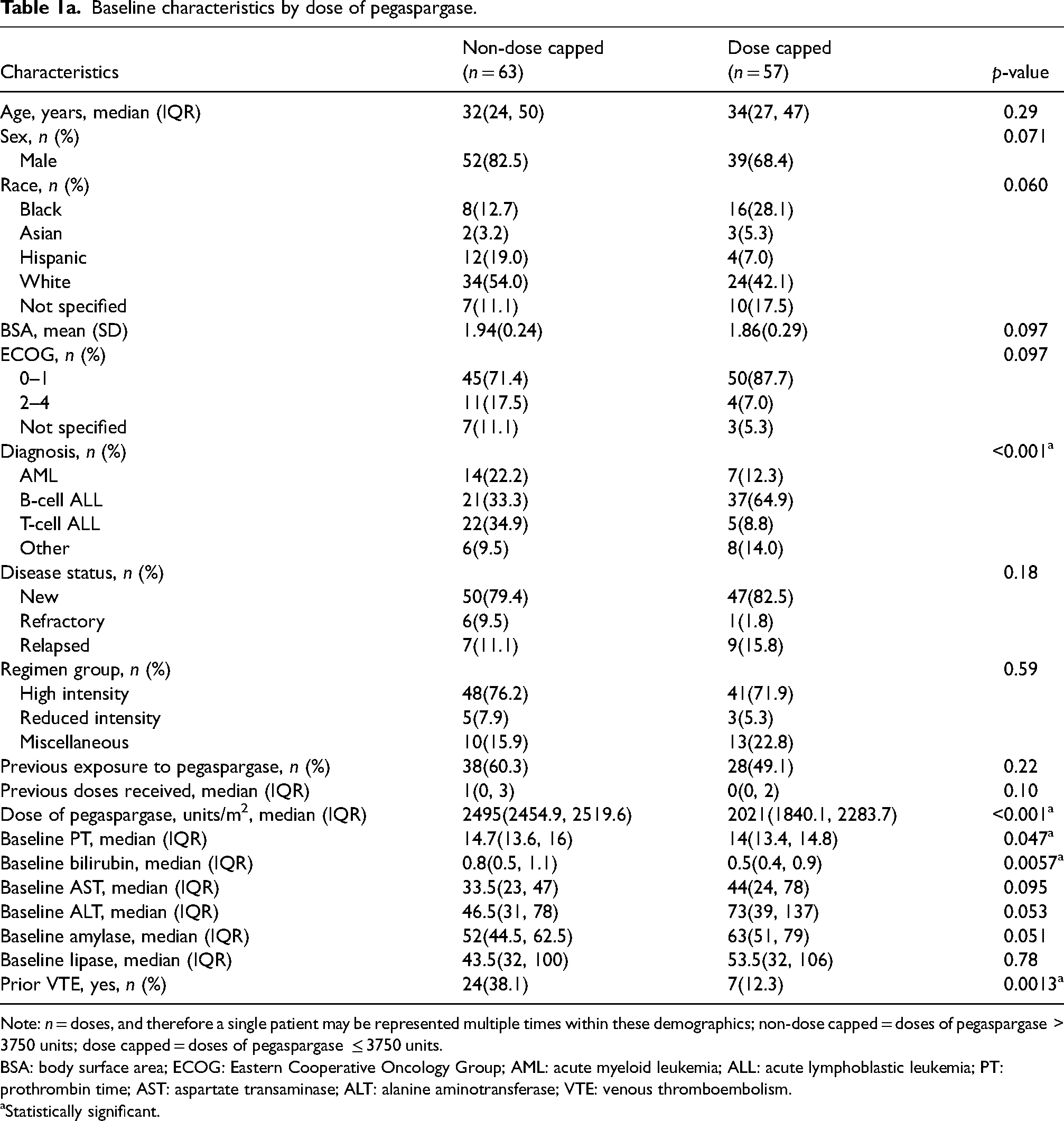
Note: n = doses, and therefore a single patient may be represented multiple times within these demographics; non-dose capped = doses of pegaspargase > 3750 units; dose capped = doses of pegaspargase ≤ 3750 units.
BSA: body surface area; ECOG: Eastern Cooperative Oncology Group; AML: acute myeloid leukemia; ALL: acute lymphoblastic leukemia; PT: prothrombin time; AST: aspartate transaminase; ALT: alanine aminotransferase; VTE: venous thromboembolism.
Statistically significant.
Baseline characteristics by patient.
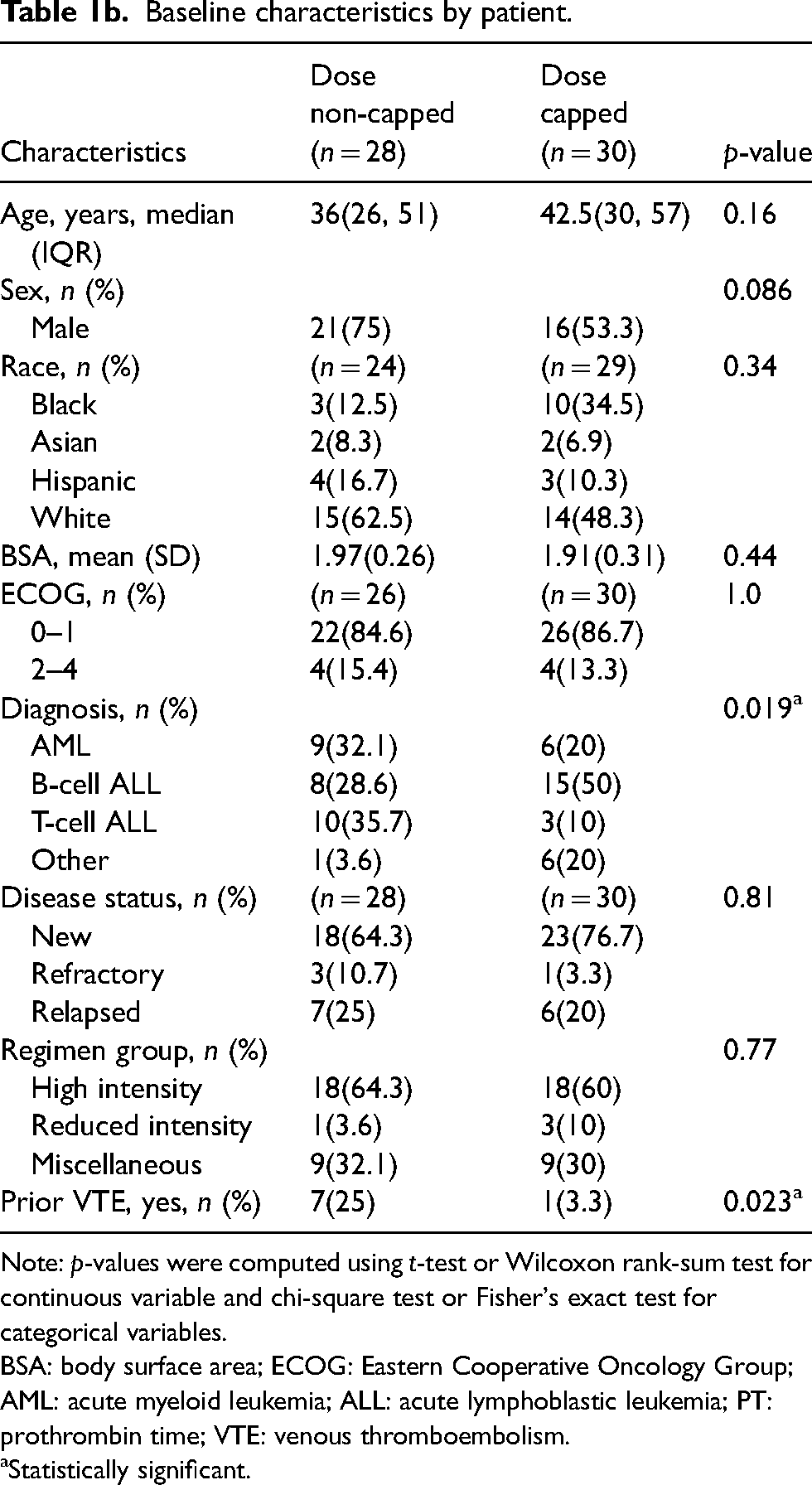
Note: p-values were computed using t-test or Wilcoxon rank-sum test for continuous variable and chi-square test or Fisher's exact test for categorical variables.
BSA: body surface area; ECOG: Eastern Cooperative Oncology Group; AML: acute myeloid leukemia; ALL: acute lymphoblastic leukemia; PT: prothrombin time; VTE: venous thromboembolism.
Statistically significant.
For the primary outcome, there were 26 doses (45.6%) in the dose capped group that resulted in SAEs, and 22 doses (34.9%) in the non-dose capped group (p = 0.23) (Table 2). When a multivariate model was applied to account for confounding variables, there was no significant difference found in the risk of composite incidence of PEG-ASP-related SAEs between capped and non-capped doses (OR 2.56 (0.84, 7.77), p = 0.098).
Primary outcome.
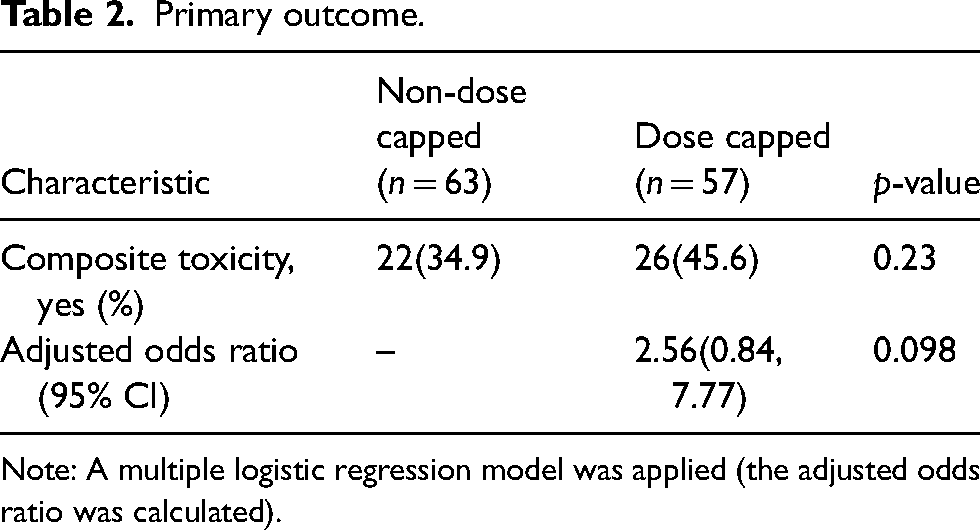
Note: A multiple logistic regression model was applied (the adjusted odds ratio was calculated).
The outcomes relevant to hepatotoxicity, pancreatic toxicity, VTE, and bleeding are listed in Table 3. Of note, all hepatic and pancreatic toxicity events were laboratory abnormalities. There were no statistically significant differences between groups in the incidence of these individual toxicities, although the median peak ALT and peak bilirubin levels were higher in the non-dose capped group. Having B-cell ALL was associated with a lower odds ratio for development of composite toxicity (OR 0.25 (95% CI 0.06, 0.90), p = 0.033), as was having previous exposure to PEG-ASP (OR 0.22 (95% CI 0.07, 0.63), p = 0.0043).
Secondary outcomes.
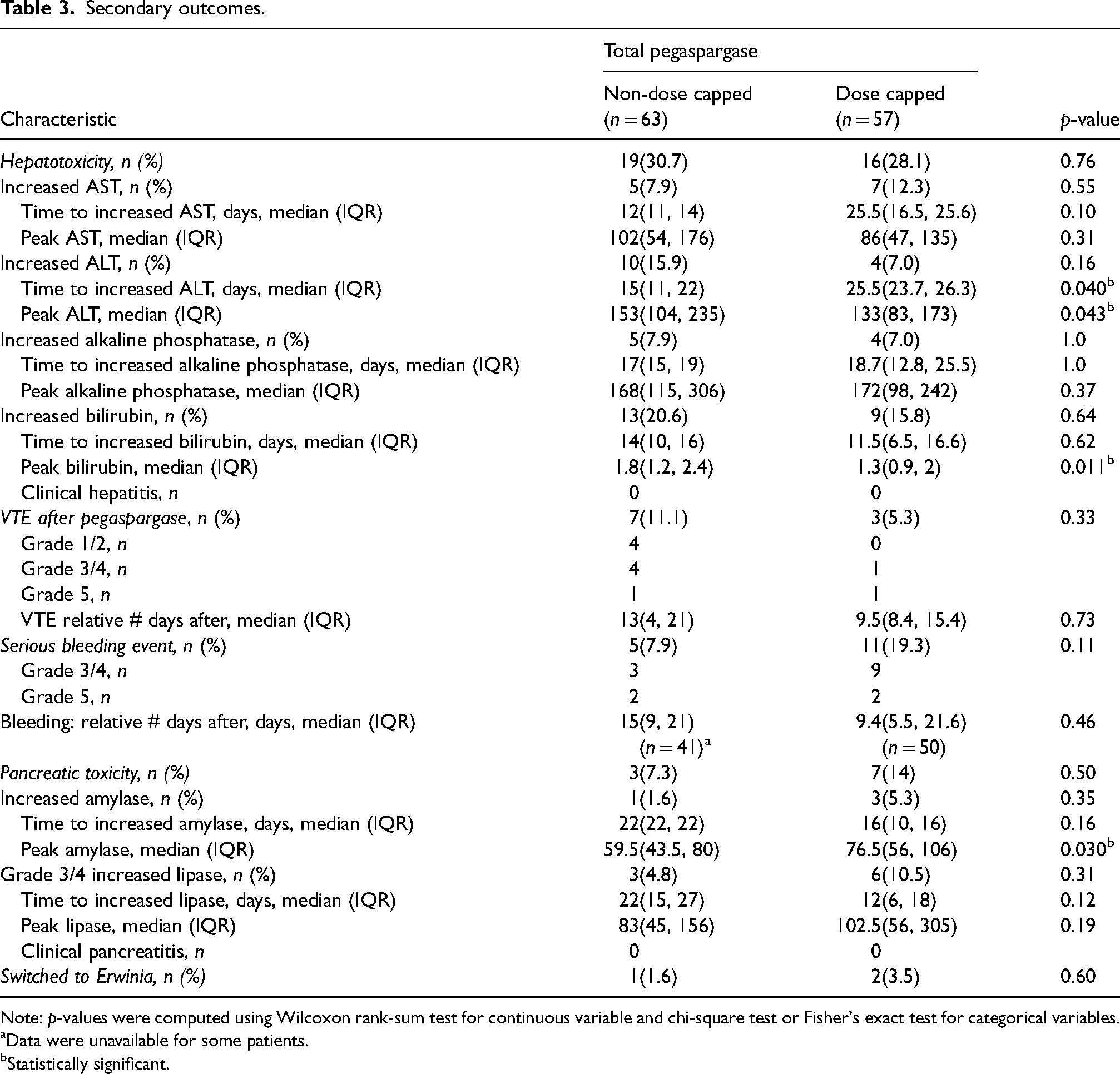
Note: p-values were computed using Wilcoxon rank-sum test for continuous variable and chi-square test or Fisher's exact test for categorical variables.
Data were unavailable for some patients.
Statistically significant.
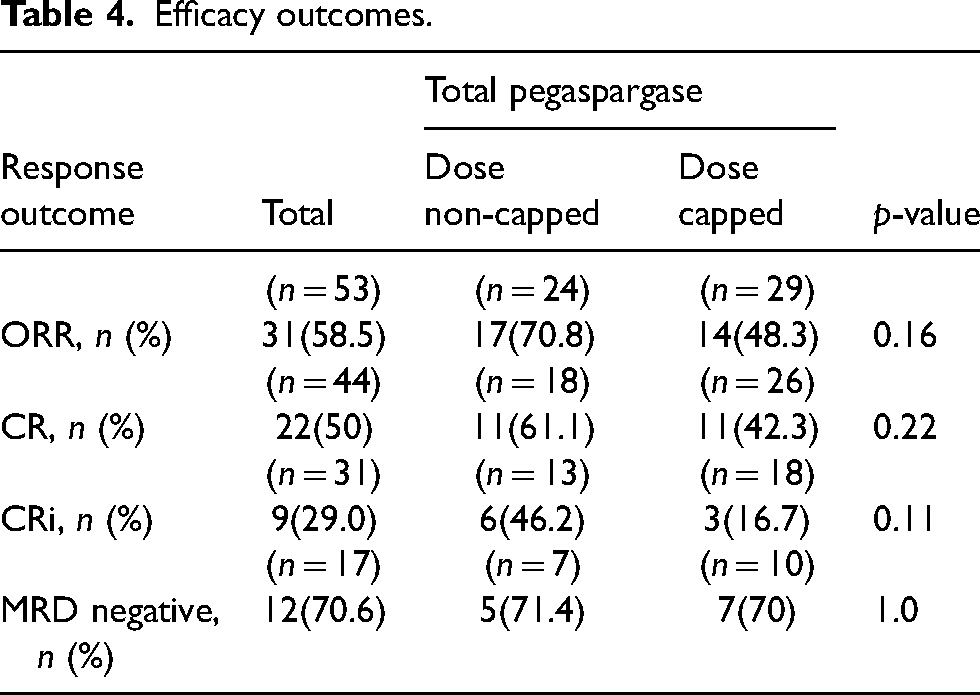
The ORR, rates CR, and CRi did not differ between the two groups (Table 4). Of all doses of PEG-ASP given during the study period, there was no significant difference between groups in the incidence of negative minimal residual disease or incidence of switching therapy to Erwinia asparaginase. A total of 24 deaths occurred during the study period, with no difference in incidence of mortality between groups. Of these, eight deaths were attributable to an adverse event induced by PEG-ASP, with five occurring in the dose capped group and three in the non-dose capped group (Table 5).
Efficacy outcomes.
Causes of deaths attributable to pegaspargase-related adverse events.
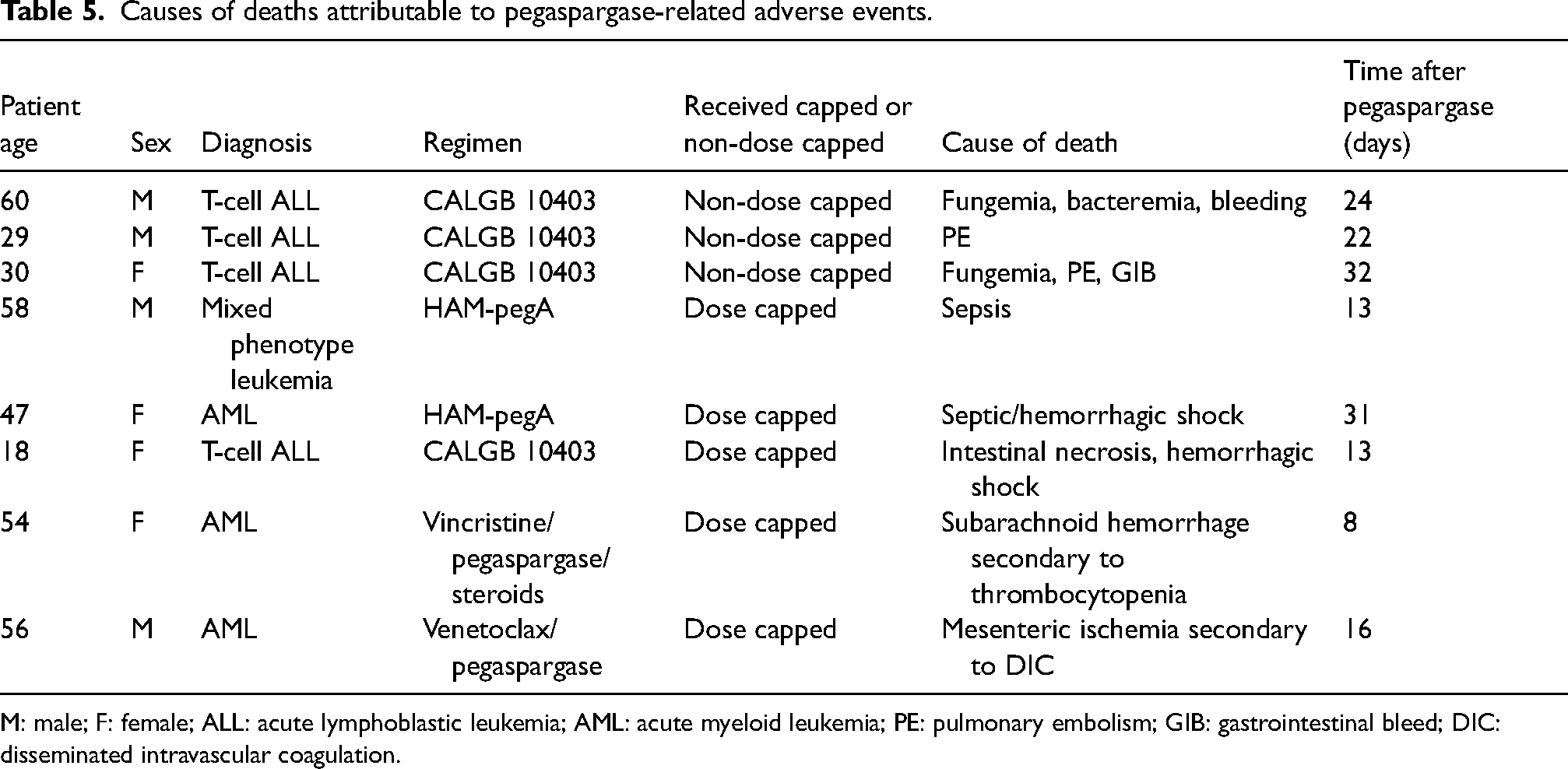
M: male; F: female; ALL: acute lymphoblastic leukemia; AML: acute myeloid leukemia; PE: pulmonary embolism; GIB: gastrointestinal bleed; DIC: disseminated intravascular coagulation.
We conducted a subgroup analysis of first doses of PEG-ASP for the primary outcome to reduce confounding variables introduced by multiple exposures to the drug. This subgroup consisted of 54 doses, 29 of which were capped doses, and 25 of which were non-dose capped. In this subgroup analysis, the primary endpoint of composite incidence of toxicity did not differ significantly between dose capped and non-dose capped groups (57.6% vs 42.4%, p = 0.47). Bivariate analysis showed no significant confounders in this outcome, so a multivariate model was not constructed. In the secondary outcomes, hepatotoxicity and VTE occurred more frequently in the non-dose capped group, while pancreatic toxicity and bleeding events occurred more frequently in the dose capped group, although these findings were not statistically different. For the exploratory outcomes within this subgroup, there were no instances of hypersensitivity causing a switch to Erwinia asparaginase. Mortality also did not differ between dose capped and non-dose capped groups (48.3% vs 36%; p = 0.36). In another subgroup analysis of PEG-ASP doses given to patients less than 40 years versus greater than or equal to 40 years, the primary outcome occurred less frequently in the age group less than 40 years at 45.5% and 29% in the dose capped and non-dose capped groups, respectively, compared to 10 of 19 doses (52.6%) in the dose capped group compared with 13 of 22 (59.1%) doses in the non-dose capped group in the age group greater than or equal to 40 years.
Discussion
Multiple studies have explored using lower doses of PEG-ASP in an effort to minimize the related adverse effects while still achieving depletion of asparagine. Wetzler et al. 4 utilized PEG-ASP at 2000 units/m2 in a prospective study of 102 patients with ALL treated per CALGB 8811 and achieved effective asparagine depletion, which was shown to correlate with improved disease free and overall survival. In another prospective study by Patel et al., 91 patients with newly diagnosed ALL, 66% of which were older than 40 years, were treated with a regimen that included a lower PEG-ASP dose of 1000 units/m2 on days 4 and 18. Measured asparaginase activity was therapeutic in 42 of 49 patients (86%), indicating effectiveness of a lower PEG-ASP dose. Adverse events related to PEG-ASP, which included liver dysfunction, pancreatitis, bleeding, allergic reaction, and vascular events, occurred in 51% of patients, which was attributed to the more advanced age of patients enrolled in this study. 12 Given the growing body of evidence for a lower dose of PEG-ASP for adults, in January 2019, the package insert for PEG-ASP decreased the recommended dose from 2500 units/m2 to 2000 units/m2 for patients age 21 and older. 13 With these supporting data, our institutional guideline likewise amended its recommendation to include the newly reduced dosing recommendation of PEG-ASP 2000 mg/m2 in patients age 21 and older in addition to the existing dose cap of 3750 units in January 2020.
Our study represents a real-world evaluation of the implementation of a dose capping strategy for PEG-ASP as compared to the conventional non-capped dose. Our sample was diverse in terms of age, leukemia subtype, race, and chemotherapy regimen utilized. The two groups, dose capped and non-dose capped, were generally well-balanced, with the exception of diagnosis type and history of prior VTE. The composition of the dose capped group consisted of slightly older adults, as reflected by the median age of 42.5 years when assessed on a per-patient basis. This slight difference in age likely results from some degree of selection bias, with clinicians choosing to cap the dose in older patients as compared to AYA patients prior to the 2018 institutional practice change. Despite the difference in age and dosing strategy, the two groups had similar exposure to PEG-ASP (roughly two doses per patient) with few patients experiencing a hypersensitivity reaction necessitating switching to the Erwinia-derived form of asparaginase.
Overall, the composite incidence of serious PEG-ASP-related adverse events observed in this study was similar between dose capped and non-dose capped groups. In comparing the incidence of SAEs in our study to the published CALGB 10403 data, we observed a lower incidence of hepatotoxicity, but a similar rate of pancreatic toxicity. 2 The majority of SAEs that occurred were strictly laboratory abnormalities, with no reports of clinical hepatitis or pancreatitis. The rate of VTE was higher in the non-dose capped group, but overall was relatively low (8.3%) in our study, while previous literature have reported rates up to 34%. 14 This overall low VTE rate can likely be attributed to our venous thromboembolism prophylaxis practice that includes low-molecular-weight heparin as well as antithrombin III monitoring and repletion for all adult patients. The ORR, CR, and CRi rates did not differ significantly, indicating that the practice of dose capping did not have a significant effect on these outcomes.
Our multivariate analysis revealed some interesting associations between patient characteristics and composite toxicity. Although previous exposure to PEG-ASP did not differ statistically between groups, more patients in the non-dose capped group received previous PEG-ASP. In accounting for potential confounders through the multivariate model, we found that doses that were given to patients who had a previous exposure to PEG-ASP were associated with a lower risk of composite toxicity (OR 0.22 (0.07, 0.63), p = 0.0043). This is likely a product of practice, as patients who experienced toxicity with previous doses are less likely to continue to receive PEG-ASP in future cycles. Another association that was identified was that doses given to patients with B-cell ALL were less associated with the adverse events examined in this study. This may be related to fewer prior therapies received as compared with other hematologic malignancies analyzed, with only 6 of 58 (10.3%) patients having received a previous line of therapy.
Our study had several limitations, some of which are inherent to the retrospective nature of chart review, such as the issue of missing data for several variables of interest. While we elected to divide our groups using the threshold of one vial size, or 3750 units of PEG-ASP to reflect our institutional guideline set forth in 2018, this approach had some advantages and disadvantages. Although this threshold established a clear dividing line, using an absolute value limited our ability to relate the primary outcome to units of PEG-ASP normalized by the body surface area of the patient, which would be a potentially more nuanced approach to examining the data. Another possible confounder was the inclusion of all doses of PEG-ASP irrespective of previous exposure to the drug. The inclusion of all doses of PEG-ASP, with the data being analyzed on a per-dose basis, caused four patients to be represented in the data set multiple times. In particular, one patient in the non-dose capped arm who was 19 years of age received nine doses of PEG-ASP during the study period, which could also have skewed the median of that group. Due to the timeframe selected, doses were included at various phases of treatment, which could introduce additional variance depending on the overall intensity of each phase and make it difficult to discern whether PEG-ASP was discontinued due to toxicity or simply excluded due to the limited study period. To account for this variability, we analyzed the subgroup of first doses, which demonstrated no significant difference in the incidence of the primary outcome. While our study's heterogeneity was a strength in inclusivity, certain variables, particularly the varying intensity levels and schedules of multi-agent, PEG-ASP-containing chemotherapy regimens included, limited the ability to accurately and distinctly compare certain adverse events, such as hepatotoxicity in regimens containing concomitant hepatotoxic medications, between dose capped and non-dose capped PEG-ASP groups. Also, several institutional guideline changes occurred at various points throughout the study period. With these multiple changes, it is difficult to attribute the observed incidence of adverse events solely due to the practice of dose capping as opposed to the additional measures that were implemented for prevention of adverse events. Despite these limitations, this study included a diverse sample of patients that spanned a wide age range and breadth of diagnoses, providing valuable insight into the safety of PEG-ASP utilization in a real-world setting.
Conclusion
In summary, our retrospective single-center study inclusively looked at all doses of PEG-ASP administered to adult patients over a 4-year period. Our study found no difference in the composite incidence of hepatotoxicity, pancreatic toxicity, VTE, and hemorrhage between the group that received capped doses of PEG-ASP as compared with the non-dose capped group. Furthermore, given the low overall incidence of PEG-ASP-related SAEs, and the similar clinical efficacy in terms of ORR, CR, and CRi between the two dosing strategies, our study findings suggest that PEG-ASP may be given using this dose cap even in older adults, coupled with vigilant monitoring and proactive pharmacologic mitigation of adverse effects, to achieve comparable outcomes.
Footnotes
Author contributions
ET, Conceptualization, data curation, investigation, methodology, writing – original draft; CB, Conceptualization, data curation, methodology, project administration, supervision, validation, writing – review and editing; JAT, Conceptualization, methodology, project administration, supervision, writing – review and editing; JL, Conceptualization, methodology, writing – review and editing; HS, Formal analysis, software, writing – review and editing; AE, Conceptualization, methodology, writing – review and editing; AD, Conceptualization, methodology, project administration, supervision, writing – review and editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.